
Abstract
Introduction
Children with mobility difficulties are thought to share similar participation repertoires due to the impact of their physical impairments. However, with these children, as with all others, individual differences and contexts should mediate occupational repertoires and experiences, resulting in participation differences, at least in part. This study aimed to explore the occupational repertoires of children with mobility difficulties and their view of their occupational participation.
Methods
Five children with mobility difficulties were assessed using the paediatric activity card sort, to establish their occupational repertoires. Semi-structured interviews were used to understand the children’s occupational participation.
Findings
Our findings suggest that children with mobility issues are more likely to participate in quiet occupations, but not exclusively. The children defined participation in their own way.
Conclusion
The knowledge about how children with mobility difficulties understand participation in occupation can help occupational therapists to establish goals with their clients and personalise interventions.
Introduction
Children have a continuous, innate tendency toward doing or being occupied (Davis and Polatajko, 2010). Through participation in the occupations of daily life, children develop personal autonomy, become competent and participate in occupational activities building their own personal occupational repertoire (Zilberbrant and Mandich, 2005). An occupational repertoire is the sum total, or constellation, of occupations – meaningful and purposeful activities – in which an individual has the capacity to participate at a given point in time (Davis and Polatajko, 2010). Occupational repertoires change across the lifespan often in concert with an individual’s age, stage of development, skill acquisition, and context. According to Wiseman et al. (2005), the occupations in which children participate are shaped by opportunities, resources, motivations and parental views and values as well as by the interaction among person, occupation and context. In the absence of adequate opportunities to participate in occupations, children are unable to achieve their potential and are less able to grow as individuals (King et al., 2003). This situation is likely to occur among children with disabilities, especially those children with mobility difficulties. This article reports on a study that explored the occupational repertoires of children with mobility difficulties and their view of occupational participation.
Literature review
Occupational participation has been shown to be lower in children with physical disabilities than in their typically developing peers (King et al., 2010; Law et al., 2006). It has also been shown to differ in terms of the type of occupations and intensity of participation relative to typically developing peers (Aitchison, 2003; Law et al., 2006). Children with mobility difficulties emerge as a distinct population among children with disabilities as these limitations present distinct participation issues, in large part as a result of the barriers created by inaccessible environments (Imms, 2008; Lawlor et al., 2006; Lepage et al., 1998; Majnemer et al., 2010).
The study reported here focused broadly on physical disabilities resulting in mobility difficulties in an attempt to address two overriding methodological issues apparent in the current literature on participation in occupations of children with physical disabilities. First, many studies have grouped children with physical disabilities with children with other disabilities, such as cognitive or psychological disabilities. These other disability groups have been shown to have different occupational patterns than children with physical disabilities (Voorman et al., 2006); therefore, grouping all children with disabilities together confounds findings regarding physical disabilities and occupational participation. Second, much of the literature on the participation of children with physical disabilities in occupations has been diagnosis specific. Law and colleagues (2004) suggest that the focus on diagnosis in studies of child participation is misplaced because when controlled for other variables such as age, sex, or physical function, diagnosis alone does not significantly predict a child’s participation in occupation.
This study also set out to understand the perspective of children regarding their participation. While some studies have done this in the past, most of them attempted to understand the participation barriers faced by children (e.g. Law et al., 2007; Schenker et al., 2005; Tonkin et al., 2014), and many have not specifically sought the children’s perspectives. Zwicker et al. (2018) carried out a qualitative study with 13 children with developmental coordination disorder designed to understand better the implications of the disorder on their daily life and to deepen the understanding of their quality of life. The study showed some predictable results regarding the children’s challenges to perform everyday self-care and school occupations; however, the comments from the children also highlighted the extensive impact of developmental coordination disorder on their quality of life and affirmed that developmental coordination disorder is more than a motor impairment. Further, the children’s comments made clear the emotional toll of attempting to perform daily activities without success.
Another study giving voice to children was conducted by Timler et al. (2018). Working with 133 parent–adolescent dyads to investigate the congruency between parent and self-reported motor competence, the authors found that parents identified fewer motor difficulties in their adolescence, especially for girls, than the teens themselves (Timler et al., 2018).
Understanding children’s perspectives on their occupational repertoire can provide occupational therapists and researchers with a more nuanced understanding of how children experience their participation in occupations. This new understanding can reveal gaps in children’s occupational repertoires that can be used as targets for intervention, areas of strength that can be capitalised on, and areas to explore further and understand through research. The study reported here aimed to describe the occupational participation repertoire of children with mobility difficulties, including their perspectives on their participation in occupation.
Methods
A mixed-method design was chosen to address the aims of the study. The Paediatric Activity Card Sort (PACS; Mandich et al., 2004) was administered to collect quantitative data on the occupational repertoire of children with mobility difficulties, and semi-structured interviews were used to gather data to understand the children’s perspectives on their occupational participation.
Participant recruitment and selection
Five children participated in the study. Participants and their families were recruited through community organisations that serve children with physical disabilities and typically developing children such as hospitals, community organisations and schools. Advertising for the study and contact information for the researchers were disseminated to community organisations for distribution to specific families or for posting in a public space. Contact between the families and the researchers was initiated as per the process approved by the University of Toronto health science research ethics board. During this initial contact, the researchers discussed inclusion criteria and outlined study details with potential participants. As this study did not take a diagnosis-specific approach, a variety of diagnoses were considered for inclusion including cerebral palsy (CP), spina bifida, muscular disorder, injury resulting in loss of function of lower extremities, or other impairments resulting in mobility difficulties. All children were identified as having mobility difficulties by their parent/guardian.
Participants were selected if they met the inclusion criteria for the study. Participants were required to be between 5 and 14 years old, to be enrolled in the age-appropriate school grade (as a proxy to identify any children with a cognitive or psychological disability that may impact their occupational participation and thus confound the results), and have the ability to understand and respond to simple verbal commands in English. Participants were excluded from the study if they were severely limited in language comprehension or expression based on parent report.
The PACS administration and semi-structured interview were conducted at the participants’ homes or in a location agreed upon by the participant and researcher. Written parent/guardian consent and written child assent were obtained prior to administration of the PACS and the interview. Child verbal assent was considered sufficient if written assent was not possible; this information was recorded on the assent form.
Data collection
The researchers collected both quantitative and qualitative data to address the research question. The outcome of the PACS, an occupational repertoire, lends itself well to quantitative data collection and analysis. However, it was anticipated that children would provide additional information spontaneously regarding participation that would not be reflected in the quantitative data. To capture these additional data, and to allow the researchers the opportunity to pose questions regarding participation, qualitative data in the form of an interview were collected and analysed.
The PACS
The PACS was administered to children to generate their occupational repertoires. The PACS is an occupation-based, self-report assessment containing 75 photographs of children participating in a broad range of occupations in the four categories of personal care, school and productivity, hobbies and social activities and sports. In completing the PACS, children indicate if they currently participate in the occupation pictured and the frequency of their participation (daily, weekly, monthly, or yearly). If they do not participate in the occupation pictured, they are asked if they would like to participate in the occupation. Participation data are recorded on PACS score sheets. Results from the PACS yielded individual participation percentages for each of the four categories: personal care, school and productivity, hobbies and social activities, and sports and a total percentage score for all categories together.
Semi-structured interview
Interviews were completed to understand the children’s participation. Occupations that were expected to yield different participation responses due to the high mobility demands of the occupation, such as vacuuming and riding a bike, were flagged by researchers a priori and discussed with the children both during and as part of an interview following the PACS administration. If children indicated that they did participate in flagged occupations, such as bathing, researchers probed for further information regarding their participation with a specific question such as ‘How do you (get into the bathtub)?’ If the participants indicated that they did not participate in occupations of interest to them, they would be asked ‘Why don’t you (ride a bike)?’ Children were also asked to indicate which of the activities of their repertoire were most important and which activities they did not perform but wanted to. At times, parents were present during the interviews, interjecting into the child’s interview on some occasions. Interviews were audio recorded and transcribed verbatim.
Data analysis
The PACS
Descriptive statistics were used to analyse demographic and socioeconomic data. The PACS scores were computed as per manual instructions, and data were analysed through the statistical package for social science (SPSS – version 20.0). Descriptive statistics were used to describe participation in individual occupations and occupational patterns. The percentages of occupational participation were calculated for all participants in each of the four PACS categories as well as for the overall result.
Semi-structured interviews
A qualitative descriptive approach (Sandelowski, 2000) to data analysis was used with the transcripts to inform the quantitative study findings. A qualitative descriptive approach aims to provide a comprehensive synthesis of the data using words from (in vivo) or as close to the original transcripts as possible, providing a straight description of the data (Sandelowski, 2000). This descriptive type of qualitative analysis fits well within a mixed-methods design and practice-oriented research as it limits inference and abstraction of the participants’ perspectives to ensure that the analysis is driven by the data, as is consistent with quantitative analysis.
Two of the authors familiarised themselves with the data by transcribing the interviews, reading and re-reading the transcripts. They engaged in the familiarisation process independent of each other to maintain flexibility of thought. The researchers then generated initial codes from the transcripts independently, remaining close to the units of data, before coming together to discuss the generated codes and build consensus for the codes that would be used across all transcripts. The codes were then grouped into categories and each category was named and defined. The final categories were chosen based on their occurrence across the entire dataset, as well as the relevance to the research question.
Findings
Demographics
Five children with a mean age of 10.2 years (±1.6) participated in this study (see Table 1 for complete demographics). No children who were interested in participating were excluded from the study. All participants had at least one sibling and used some type of mobility support (wheelchair, walker, or orthoses).
Participant profiles.
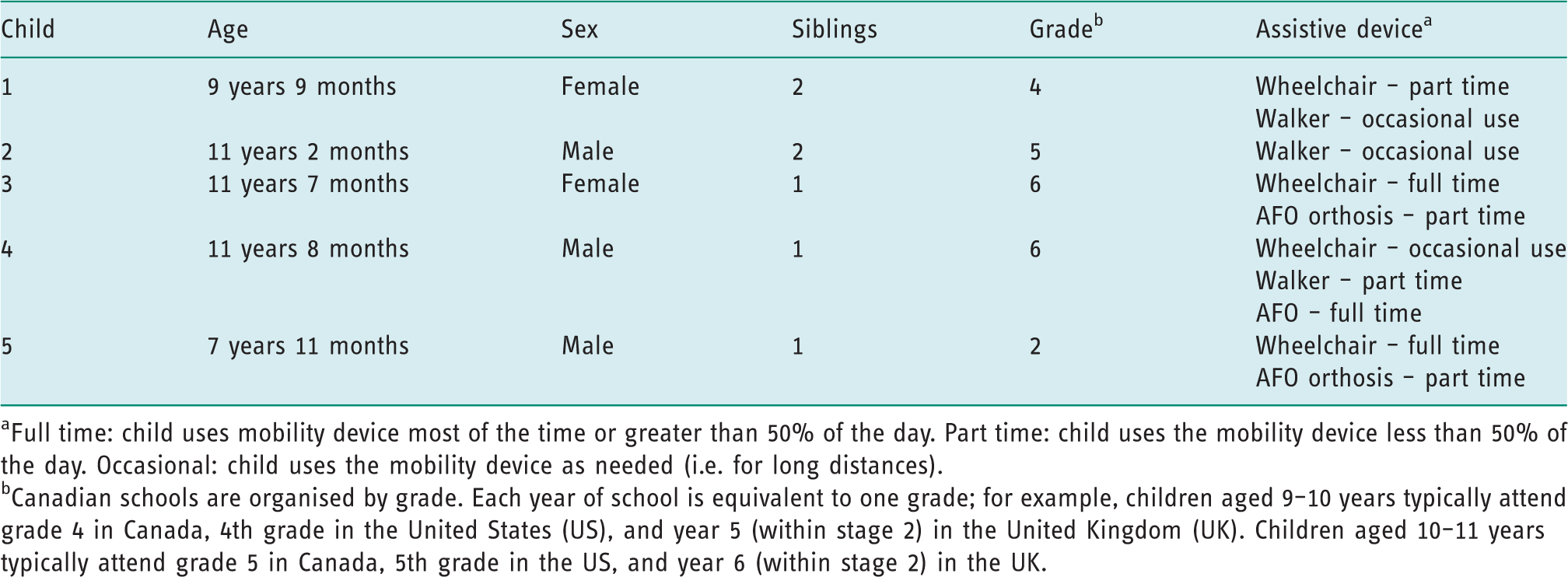
Full time: child uses mobility device most of the time or greater than 50% of the day. Part time: child uses the mobility device less than 50% of the day. Occasional: child uses the mobility device as needed (i.e. for long distances).
Canadian schools are organised by grade. Each year of school is equivalent to one grade; for example, children aged 9–10 years typically attend grade 4 in Canada, 4th grade in the United States (US), and year 5 (within stage 2) in the United Kingdom (UK). Children aged 10–11 years typically attend grade 5 in Canada, 5th grade in the US, and year 6 (within stage 2) in the UK.
Occupational participation repertoires
The PACS results showed that each child’s repertoire comprised numerous occupations (ranging from n = 32 (42.3%) to n = 53 (70.6%) occupations out of 75 total) in each of the four PACS categories: personal care (n = 9 (81.85%) to n = 11 (100%)), school and productivity (n = 5 (29.4%) to n = 13 (76.5%)), hobbies and social activities (n = 15 (42.8%) to n = 27 (77.1%)) and sports (n = 3 (25.0%) to n = 9 (75.0%)) (see Table 2). The occupational repertoires of the children varied child to child; no pattern was discernible (see Figure 1). However, for all children, the percentage of their personal care repertoire was larger than of the productivity, hobbies, or sports categories.
PACS activities, by category, with the three a highest and three lowest reported participation rates.
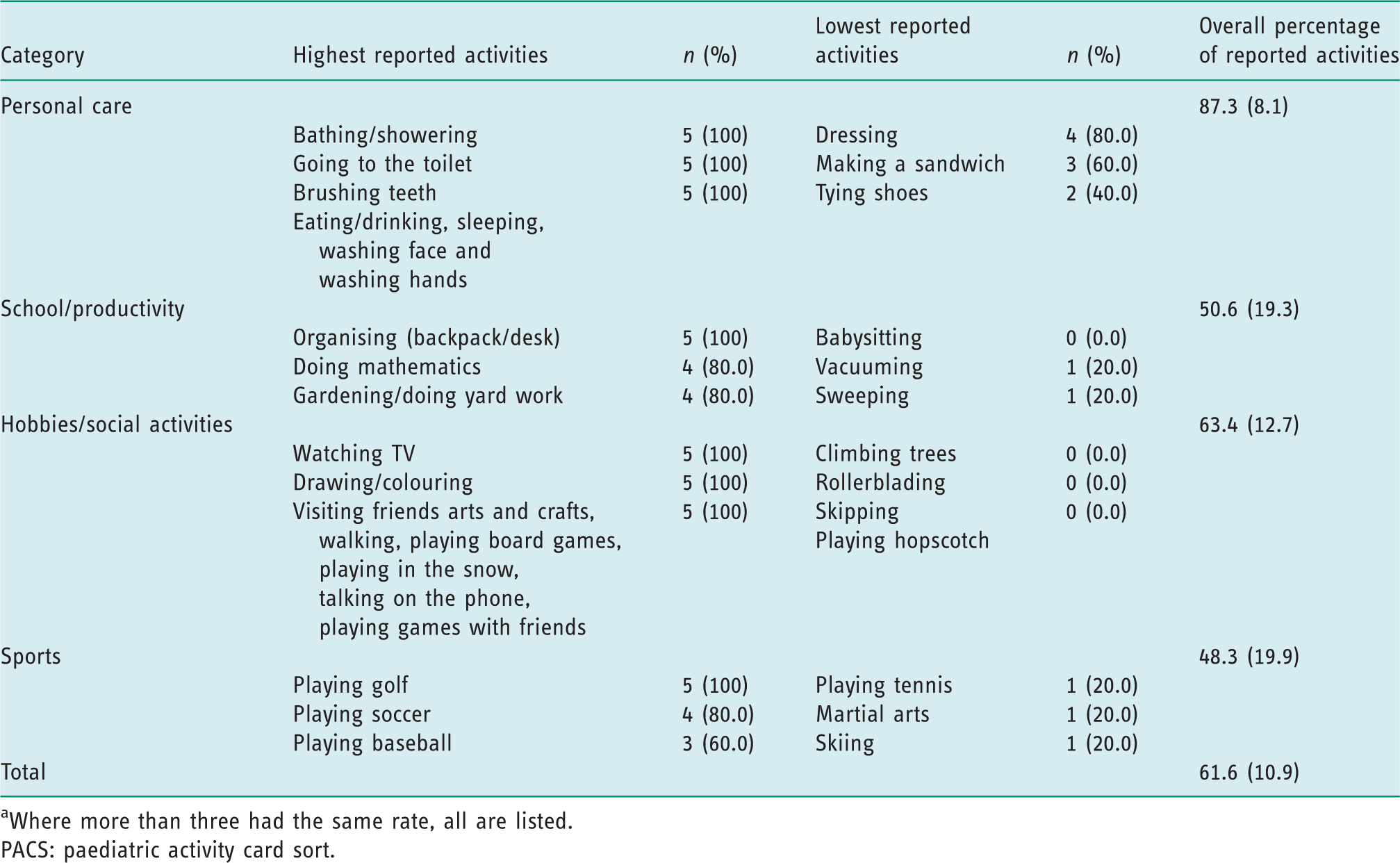
Where more than three had the same rate, all are listed.
PACS: paediatric activity card sort.
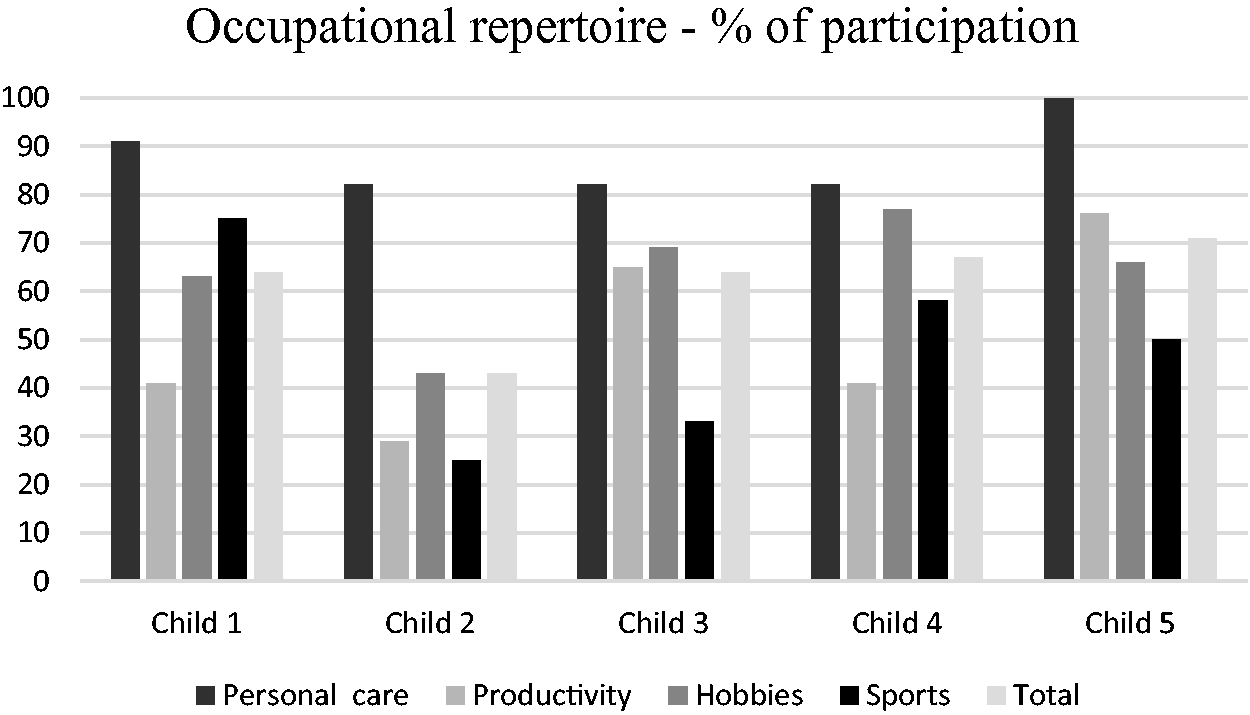
Occupational repertoire by child by category.
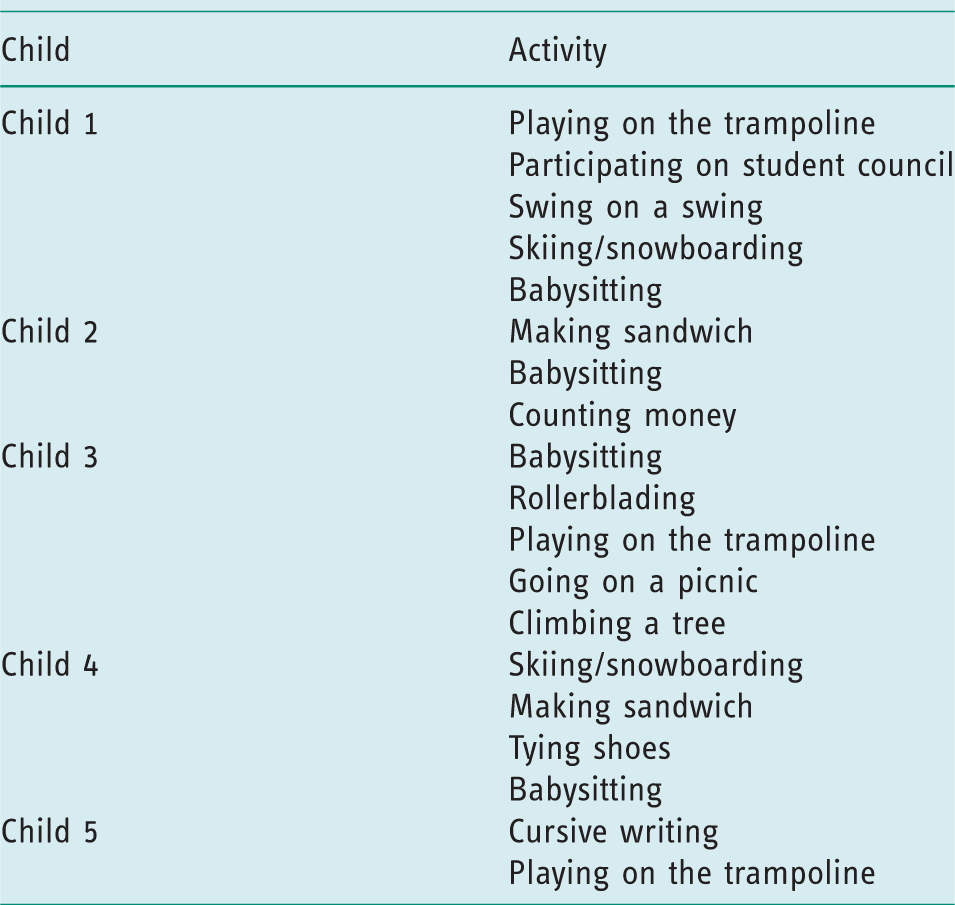
All children participated in personal care such as bathing, eating, or washing hands; however, only one child did shoe tying. No child in the study babysat, and only one child reported vacuuming or sweeping, but all children organised their backpack. All children participated in hobbies, in most cases these were quiet activities such as drawing or talking on the phone, or social occupations such as visiting friends. After completing the PACS, children were asked about which of the occupations they do not do but would like to do. They reported occupations such as babysitting, making a sandwich, tying shoes and swinging on a swing (see Table 3).
Activities in which children would like to participate.
Children’s perspectives of their participation in occupation
Three categories emerged from the transcripts of the semi-structured interviews with the children with mobility difficulties. Together these three categories provide a more nuanced understanding of these children’s occupational repertoires and initial insights into the children’s perspectives.
I do it in my own way
Children with mobility difficulties defined participation in certain occupations in relation to the level of their abilities. This category encompassed much of the dialogue surrounding participation in personal care and hobbies. Children with mobility difficulties participated in personal care with some support from others, ‘I do my zippers and buttons but sometimes I do get a bit of help … . But, yes I do. I do it every day’ (child 4), and/or with help with some tasks of the occupation, ‘Yes. My mom helps me. I can do my buttons and zippers and stuff. I get my shirt on but she needs to help me with my pants’ (child 1).
The children discussed how their participation in sport occupations often involved the assistance of another individual, by modifying the occupation. Child 3 spoke about her involvement in the most popular Canadian winter sport, ice hockey, which has been adapted for people with disabilities using a sledge: ‘I do this (sports) a lot at camp. Yeah, there’s sledge hockey, but I can’t go in a sledge, so I just stay in my wheelchair (to play),’ or with the use of adapted aids or equipment, regarding riding a bike, child 4 said ‘Well, yes I do. Well, not on a real bike, but on an exercise bike I do.’
When parents were present during the interview, there was an often apparent difference in the perception of what ‘participation’ meant. Some parents questioned their child about the level of their participation; for example, when one child was asked if she tied her shoes, the mother exclaimed, ‘Does that mean independently? So you don’t!’ (mother of child 2), while another mother interjected, ‘You have to tell the truth, remember?’ (mother of child 5). Although most of the children stated that they participated in some occupations regardless of potential barriers by doing the occupation in their own way, through help from others, or by using adapted equipment, all the children identified occupations that they would like to do but perceived the barriers as too great to attempt it.
I want to but I can’t
Often, the children perceived their own mobility impairment as a barrier to participating in occupations of interest: ‘Rollerblading, I can’t stand up … . Picnic, or going on a picnic, I can’t really sit down on the ground; I’ve had spine fusion so I can’t cross my legs’ (child 3). Bending, standing, sitting and walking were perceived as barriers to participation: ‘Well, I have cerebral palsy so it’s hard for me to bend down (to tie my shoes)’ (child 4), and ‘I can’t really play on the trampoline because I can’t walk’ (child 5).
Only one child discussed how an accessible environment facilitated his/her participation in the occupation: ‘Visiting friends, it hardly ever happens. But my friend … has a ramp though cuz her mom’s friend is in a wheelchair so I get to go over there sometimes’ (child 3).
I don’t want to do it
One reason that children provided for not doing an occupation is that they were not interested in doing it. This finding was most noticeable in relation to productive occupations. For example, regarding washing and drying the dishes (i.e. crockery), child 2 said, ‘No. Not really. I can sort of, but I don’t really want to (wash and dry the dishes)’; while child 1, regarding certain hobbies noted, ‘Not really. I used to do stuff, something like that, like building with blocks, but that’s when I was really young’ (child 1), and ‘No way. I probably wouldn’t want to climb trees even if I could’ (child 1).
Discussion and implications
This study explored the occupational participation repertoires of children with mobility difficulties to provide a more nuanced understanding of these children’s participation and perspectives. It is well known that children with physical disabilities (see Chiarello et al., 2014; King et al., 2010; Majnemer et al., 2010; Woodmansee et al., 2016) have different occupational repertoires than their typically developing peers. However, information regarding in which occupations children have difficulties participating and their perspective about their participation is still relatively scarce (Timler et al., 2018; Zwicker et al., 2018).
The study reported that children with mobility difficulties participated in at least 81.85% (ranging from 81.85% to 100%) of personal care activities. This finding contrasts with those from a cross-sectional study that compared patterns of household task participation of 75 children (mean age 9.3 years) with CP, Down’s syndrome and typical development (do Amaral et al., 2014). Through parent report, do Amaral et al. found that children with CP and Down’s syndrome scored significantly lower in self-care tasks and total assistance when compared to those with typical development. Another parent report study conducted with 539 children (mean age 38 months; SD 11.3; Chiarello et al., 2014) found decreased participation in personal care activities for children with CP with different levels of severity, when compared to children with typical development. These latter two studies differ from the current study, in that they used parent report to ascertain children’s participation in self-care. The contrast in findings may be due to how participation is perceived differently by parents than by children. Also, the constructs of focus for each of these studies, specified as participation, were actually conceptualised very differently. Whereas the current study aimed to understand how children conceptualised their participation, which may or may not have included assistance, both do Amaral et al. and Chiarello et al. seemed to be assessing competence of performance using a scale as they factored in requiring assistance to their understanding of participation, resulting in lower parent report scores. Regardless of these differences, all studies found that children with motor and/or mobility differences do actively engage in daily personal care activities. In our study, personal care was the category with the highest participation; all children participated in seven of these items. A possible explanation is that children with mobility difficulties redefine participation in occupations to be inclusive of their participation abilities, as we saw in the category, I do it in my own way. During the interviews, the children with mobility difficulties were able to articulate to the researchers how their participation is different from that of their typically developing peers. The qualitative results indicate that differences in what participation looks like do exist, but that children’s perception of their participation allows for their abilities and thus did not result in significantly different mean participation frequencies. In this theme, children with mobility difficulties recognise how their participation differs from their typically developing peers and spontaneously expand on their responses to share how they believe their participation differs in its form. However, they still perceived that they were participating in the occupation, albeit differently. The implications of the findings of this study, in relation to parent versus child report and the inclusion of assistance in the conceptualisation of participation, or performance, speak to the need for reconceptualising what participation means and examining the ableist attitudes contained within our measures.
Our findings suggest that children with mobility difficulties performed more sedentary occupations rather than active occupations. This result was consistent with those presented by Carlon et al. (2013) who showed that young people with CP participated in physical activities at a rate that was 13% to 53% lower than those children with typical development. Woodmansee and colleagues (2016), who evaluated 326 Australian children, also found that children with disabilities were less likely to participate in athletics, team sports, snow sports, non-team sports and play games when compared to children with typical development. The same study also observed that children with disabilities tended to participate less in their preferred activities (Woodmansee et al., 2016). The consistent findings in these studies indicate the need for examining the barriers to participation for children with mobility and/or motor difficulties to support inclusion and engagement.
Our results showed that the school and productivity category had the lowest participation score for three of the five children. A cross-sectional study undertaken with 66 children, 33 children with disabilities, showed that children with disabilities had lower participation both in structured and unstructured school activities. They also had fewer friends and rated their autonomy as lower (Eriksson et al., 2007). Schenker et al. (2005) evaluated 248 children and found that children with CP had decreased participation in occupations related to the classroom, playground, transportation and transitions, bathroom and mealtime in school when compared to children of the same age. However, another study examined household task participation patterns of 46 children and youth with and without physical disability. The authors found that children with a physical disability did not differ significantly from those without disabilities in the number of household tasks they performed; however, they did require more assistance than those without physical disability (Dunn and Gardner, 2013). These studies again point to the need to understand how our perceptions of participation influence findings as well as how the environmental barriers limit children’s participation. As noted above, one study found household tasks as equivalent across groups, which may indicate that the organisation of environments outside the home limit participation.
One possible explanation for the children’s lower levels of participation in occupations related to productivity was presented during the interviews. Most of the occupations that children did not want to do were chores and household tasks. This finding is rarely discussed in the current literature. Some children affirmed that the reason they did not participate in a specific occupation was that they were not interested in doing it. According to Wiseman and colleagues (2005), children have a variety of motivations for participating or not participating in occupations. Pure enjoyment, fit between abilities and the demands of the occupation, and competition are some reasons identified by the children as motivations to participate in occupations (Davis, 2000; Wiseman et al., 2005). As the children were not motivated to participate in these types of occupations (as revealed by our interviews), they did not attempt to perform them even within their capabilities, unlike other occupations that they wanted or needed to do. For these occupations, they would often say they do perform them even if they required assistance. However, when asked about occupations they would like to perform, most of the children did indicate that they would like to do some specific chores, such as babysitting or making a sandwich, ones that may be viewed as providing greater personal incentive. Thus, it may be that their parents did not require them to participate in productive occupations, did not view them as necessary for them to do, or did not offer assistance or teach them how to perform these occupations.
In the theme I want to but I can’t, children usually perceived themselves or their impairment and not the environment as the principal barrier to participate in occupations. Similar results were found by Furtado et al. (2015), who investigated the effect of environmental factors in the relationship between mobility impairment on the gross motor function classification system and school participation of 102 children and adolescents with CP. Their results showed that while mobility impairment was a strong predictor of participation, environmental factors demonstrated a weak predictive effect. In contrast, a systematic review about the meaning of leisure for children and young people with physical disabilities reported that the participants mentioned more often that the restrictions in participation in occupations were the result of other people due to the overprotectiveness from gatekeeping adults or the behaviour of theirs peers (Powrie et al., 2015). In our study during the interviews, some parents questioned the child about his/her ability to perform the occupation – equating independent performance to participation or doing. The parents’ views and values may, with some occupations, influence the way the child perceived his or her capacity to participate in certain occupations, creating a belief that they cannot do the occupation and thus they do not ask to try (Wiseman et al., 2005).
Study limitations and future research
The presence of the parents during the interview and their interjections may have influenced the children’s responses as the parents often perceived children’s participation in occupation differently than did the children themselves. Interviewing parents and children separately may allow the children to offer information about their perspectives of their participation in occupation without the influence of parents; however, the discursive interactions between the parent–child dyad may be important to consider for future research.
Conclusion
Measuring occupational repertoires of children provides practitioners and researchers with valuable insight into children’s occupational participation. Our findings, from the perspective of the children, suggest that children with mobility difficulties participate in fewer occupations related to school, hobbies and sports when compared to typically developing peers. Our findings also indicate that the children define participation in their own way, often including their adaptation of the occupation to fit with their abilities. Children indicated that the reasons they do not participate in particular occupations were that they do not want to or they consider their personal factors (related to the physical impairment) as barriers to participation. The understanding conveyed by children with mobility difficulties of the challenges they face in trying to establish a satisfying occupational repertoire can provide therapists with increased understanding when targeting the aim of intervention and can facilitate participation in occupation.
Key findings
Children describe participation in their own way, often explaining performance adaptations they make to fit with their abilities. Children with mobility difficulties, as with all children, have strong occupational preferences.
What the study has added
Children with mobility difficulties perceive their participation as inclusive of their abilities, suggesting that occupational therapists must be open to children’s unique understandings of their participation to enable their occupations.
Footnotes
Acknowledgements
The authors would like to thank the children and parents who participated in this study.
Research ethics
Ethics approval was obtained from the health science research ethics board of the University of Toronto #25828 – 2010 (initial) to 2014 (closure).
Consent
All participants provided written informed assent (child) and consent (parent) to be interviewed for this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no financial support for the research, authorship, and/or publication of this article.
Contributorship
Tatiana Pontes wrote the current manuscript based on her update of the literature and her re-analysis of the original data. Katie Mah and Adrianne Arnold were involved in conceptualising the study and applying for ethics approval, completed the initial literature search, collected the data, completed the initial data analysis and drafted the initial article, with support from their research co-supervisors, Jane Davis and Helene Polatajko. Helene Polatajko and Jane Davis were involved in conceptualising the initial study, applying for ethics approval, developing the plan and interpreting the findings for both the initial and current manuscript. All authors reviewed and edited the manuscript and approved the final version.