
Abstract
Introduction
Anxiety is one of the most commonly diagnosed mental health disorders on post-secondary campuses, often brought on by stressors unique to the college environment. Traditional psychological approaches to manage anxiety might focus on breathing techniques and progressive muscle relaxation. However, additional techniques that use specific sensory input to reduce anxiety have not received the same attention in the literature.
Method
This longitudinal study compared four interventions for state anxiety (deep breathing, progressive muscle relaxation, an adapted dive reflex, and use of a weighted lap object) in a cohort of professional occupational therapy students.
Results
This study found that all four interventions significantly reduced state anxiety. The sensory-based interventions of adapted dive reflex and weighted lap object appeared to have a longer duration of impact than the traditional interventions of deep breathing and PMR.
Conclusion
These results suggest that both traditional and sensory-based approaches may be effective in reducing anxiety before a testing situation.
Keywords
Mental health concerns are a recognized problem on college campuses, with many students having difficulty managing their mental health needs (Mojtabai et al., 2015; Yusofuv et al., 2019). Anxiety is one of the most commonly diagnosed mental health disorders in the college environment, often brought on by unique stressors on the college campus (Beiter et al., 2015). Students who experience increased levels of anxiety in testing situations may be diagnosed with test anxiety. Test anxiety is defined as heightened arousal, worry, negative thoughts, increased tension, and somatic symptoms during exams or similar testing situations, and it is thought that up to 35% of students have test anxiety (Zeidner, 1998). As an impediment to academic performance, test anxiety is seen more commonly in students with anxiety disorders; however, it can manifest in any student at one time or another (Peleg et al., 2016). Regardless of it being a diagnosed condition or a passing event, anxiety can impact academic performance (Chapell et al., 2005). Students who are equipped with the ability to implement anxiety management techniques before and during an exam may experience a positive influence on their academic performance (Brodersen, 2017; Hubbard and Blyler, 2018). Therefore, this study explored the use of four different techniques, two popular interventions from cognitive-behavioral theories and two less-known sensory-based techniques, to determine which technique, if any, had the most impact on student state anxiety prior to a testing situation. The researchers hypothesized that sensory-based techniques may have a similar impact on text anxiety when compared to more traditional and researched techniques.
Literature review
There are a number of techniques beneficial in reducing test anxiety in students (Hubbard and Blyler, 2018; Regehr et al., 2013), with certain anxiety management techniques being studied more than others (Brodersen, 2017). Two widely utilized and studied interventions, with demonstrated effectiveness to address state anxiety, are breathing techniques and progressive muscle relaxation (PMR) (Damer and Melendres, 2011; Yusofuv et al., 2019; Zargarzadeh and Shirazi, 2014). These are standard therapy tools and are frequently used in conjunction with behavioral and cognitive-behavioral therapies (Nair and Meera, 2014). A cognitive-behavioral explanation for their mechanism of action is that they primarily engage “top-down” processing (Taylor et al., 2010). In “top-down” processing, an individual uses mental processing at the level of the cerebral cortex to elicit a therapeutic response (Taylor et al., 2010). A conscious focus on breathing or muscle tension helps the person become more cognizant of their bodily responses when anxious and consciously relax. This awareness also increases the likelihood of the technique being utilized in the future.
Breathing and PMR also engage “bottom-up” processing, involving the stimulation of various sensory receptors that influence central neural processing via ascending pathways from the periphery to the brainstem and cerebral cortex (Taylor et al., 2010). The slowing down of breath sends a quick message to the brain to activate the parasympathetic nervous system, thereby “putting a break” on the stress response. The holding and releasing of strong muscle contractions (as used in PMR) provides proprioceptive input to the cerebellum, impacting on emotional and cognitive processing as well as autonomic nervous system modulation (Strata, 2015).
Interventions that predominantly use a bottom-up mechanism rely on this quick physiologic response to reduce anxiety and therefore can be performed with little to no training. An example of a primarily bottom-up mechanism useful in the reduction and management of anxiety is sensory modulation. Sensory modulation is the ability to organize and respond appropriately to various sensory stimuli (Champagne, 2011) and, in using sensory input this way, is an effective method of changing how an individual feels (O’Sullivan and Fitzgibbon, 2018). It is thought to impact the physiologic response to anxiety/stress through the parasympathetic system as well as engaging bottom-up mechanisms to de-escalate arousal states (Miller et al., 2007).
A specific example of a sensory modulation intervention to calm is the use of weighted objects. Weighted objects provide deep pressure (touch sensation), which can have a calming effect by changing physiological arousal (Ayres, 1972). It is believed that the application of weight influences both parasympathetic activity through increased vagal tone and sympathetic activity through reduced activation of the stress response (Field et al., 2010). Reynolds et al. (2015) support the foundational principle of deep pressure influencing autonomic arousal through reduction of sympathetic and enhancement of parasympathetic nervous system activity.
Eliciting the dive reflex as an anxiety management technique is a component of Marsha Linehan’s dialectical behavior therapy (DBT) distress tolerance module (Linehan, 2015). Dialectical behavior therapy is a gold-standard cognitive-behavioral intervention that helps individuals manage anxiety and regulate emotions (Linehan, 2015). The dive reflex works as a bottom-up mechanism by facilitating a primitive response to submersion in cool water, stimulating energy-saving cardiovascular responses (Brick, 1966). Changes in both the parasympathetic and sympathetic systems result in reduced cardiac and vascular activity (Gooden, 1994; Leuenberger et al., 2001). As a stand-alone intervention, it has been found to relieve anxiety and assist with treating tachycardia (Smith et al., 2012). The dive reflex uses temperature (touch sensory input) to elicit a physiological response, and as such can be considered a sensory modulation technique in the management of anxiety.
Purpose
Anxiety management techniques rooted in cognitive-behavioral theories have been repeatedly studied and thus demonstrate more evidence in the scientific literature. The potential disadvantages of these techniques are that an individual must learn and practice the technique outside of a stressful situation in order to receive the most benefit. Other techniques that are less reliant on cognitive behavioral strategies, while demonstrating effectiveness across other conditions, are less studied for their application with test anxiety. These techniques, specifically the dive reflex and other sensory modulation techniques, may prove more appealing to students in a test anxiety situation because they can be implemented quickly and require little training. Given the paucity of literature on sensory modulation interventions for state anxiety, this study explored the impact of two sensory modulation techniques (specifically an adapted dive reflex and use of a weighted object) and compared them to more commonly studied techniques (breathing and PMR). It was hypothesized that using sensory modulation techniques may prove just as effective when compared to the cognitive-behavioral focused interventions.
Methods
Design
A longitudinal study design was used to assess the impact of four different interventions for state anxiety pre- and post-intervention and immediately following a testing situation. Baseline trait anxiety and test anxiety were used as control variables. Institutional Review Board approval was granted by Cleveland State University – IRB #FY2020-125. Student data from this course was collected retrospectively from the students. They were asked for permission to use the data for research purposes by providing written consent. After students consented to participate, their data was collected for the research and analysis.
Participants
A convenience sample (N = 45) of Master of Occupational Therapy (MOT) students was used as part of a course in an MOT professional program to assess the impact of four different techniques on state anxiety, specifically a testing situation.
Procedures
One of the courses within the MOT program at the university requires students to undertake four individual quizzes, worth 30% of their grade. Prior to taking the four quizzes in this term, the students were instructed to use a different anxiety-reducing technique. They used the same technique as a group at the same time and were not instructed on the technique prior to the intervention applied directly before a quiz. Prior to the first quiz, students participated in an adapted dive reflex technique. Before the second quiz, the students used a weighted lap object. Before quizzes three and four they used a breathing technique and PMR respectively.
Interventions
Adapted dive reflex
The instructor prepared plastic sandwich bags of water that were cooled in the department refrigerator until class began. The instructor read an explanation of the dive reflex, provided the students with a demonstration, and then cued the students regarding when to begin and end the technique (Linehan, 2015). In total, they were asked to apply the cold item to their face (specifically over bilateral inferior orbital bones) for approximately 1 minute while holding their breath for as much of the duration of the exercise as possible. Students with BMI < 16 were instructed not to use this technique; however, none of the students indicated that this was a concern. Once the exercise was completed, students were provided with their quiz to complete.
Weighted item on lap
Students were instructed to fill a bag or use books that equaled approximately 10–15% of their body weight (Stephenson and Carter, 2008) for the class session that day. After weighing their items to ensure that they were within the 10–15% range, the students were instructed in the technique and then were asked to place the weighted object on their lap. The instructor timed the exercise for 5 minutes and then provided the students with their quiz. Students had the opportunity to keep the weighted object on their lap during the quiz if this was their preference, but uptake of this preference was not recorded.
Breathing technique
Students were instructed in a breathing technique after brief psychoeducation of the benefits of controlled breathing. The Centre for Clinical Interventions (2018) resource on breathing was used as a guide. The students did the breathing exercise for 5 minutes then completed their quiz.
Progressive muscle relaxation
Prior to completing the last quiz, students were guided through a PMR that was played via audio in the classroom. The audio can be found at www.youtube.com/watch?v = ihO02wUzgkc.
Outcomes measures
Trait anxiety and test anxiety were measured at the beginning of the term and again at the end of the term. State anxiety was measured prior to each intervention, following the intervention and after the quiz.
Beck Anxiety Inventory (BAI)
Generalized trait anxiety was measured through the BAI. The BAI was developed by Beck (Beck et al., 1988) and it provides an objective way to measure anxiety. The BAI is a 21-item inventory of common responses to anxiety (for example, “unsteady,” “scared,” and “faint/lightheaded”). Respondents are asked to report symptoms over the last 30 days. Each item is ranked from “0 = not at all” to “3 = severely – it bothered me a lot.” The items are summed. A score of 36 or above is considered cause for concern. Test–retest reliability (r = 0.75) and internal consistency (α = .92) are good (Beck et al., 1988). There is moderate correlation with the revised Hamilton Anxiety Rating Scale (.51) and mild correlation with the Hamilton Depression Rating Scale (.25) (Beck et al., 1988).
Westfield Test Anxiety Scale
Generalized test anxiety was measured through the Westfield Test Anxiety Scale. It was developed by Driscoll (2007) for individuals to self-assess the impact of anxiety on testing situations. The Westfield Test Anxiety Scale is a 10-item scale that asks respondents to rank statements about test anxiety on a Likert scale from “1 = not at all or never” to “5 =extremely or always true.” The scores are summed then divided by 10. Scores above 3.0 signify at least a moderate level of test anxiety. It was found to have good reliability (r = .44) and high validity (r = 0.44) (Driscoll, 2007).
State Trait Anxiety Inventory (STAI)
The STAI was developed by Spielberger et al. (1983) to distinguish between state anxiety, trait anxiety, and feelings of anxiety and depression. The version used in this study was the six-item version. Respondents are asked how they feel at the moment (for example, “I feel calm” “I feel relaxed” “I am tense”). The respondent ranks the items from “1 = not at all” to “4 = very much.” A score of 34–36 is considered normal. The reliability coefficient for the six-item STAI is α = .83. It was reduced from an original 20-item scale with good validity (Pearson’s r = 0.89) (Perpiñá-Galvañ et al., 2011). The researchers chose this measure since they believed it captured more body-based symptoms of anxiety.
Subjective Unit of Distress Scale (SUDS)
The SUDS was developed by Wolpe in 1969 (Molin, 2015). It is a self-assessment tool that measures the subjective intensity of the disturbance/distress that an individual experiences (Molin, 2015). The SUDS has been correlated with the Beck Depression Inventory (Spearman’s rho = .28, p < .05) and the State Anxiety Inventory (Spearman’s rho = .31, p < .05) (Kim et al., 2008). We used a 100-point scale with markers of “100 = highest distress,” “50 = moderate anxiety/distress,” and “0 = no distress.” The researchers chose this measure since they believed it captured more of a global cognitive component of anxiety or distress. By choosing the STAI and SUDS and using them together, the researchers were able to look at both body-based symptoms and more global cognitive symptoms of distress.
Analysis
All analyses were done with SPSS version 25. Paired t-tests compared pre-intervention to post-intervention and pre-intervention to post-quiz for all four interventions. A repeated measure ANOVA was used to analyze the impact of the four interventions over time. All p-values were adjusted for multiple comparisons (p < 0.025).
Results
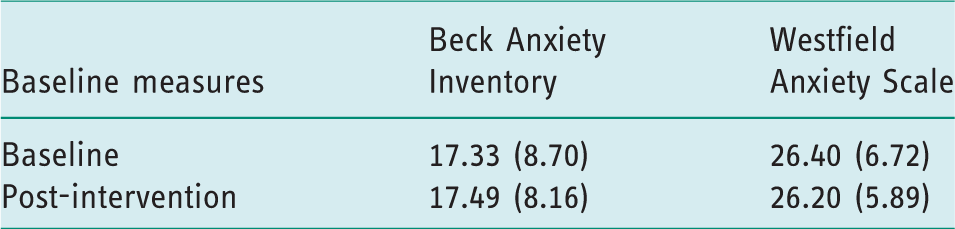
The sample was a convenience sample of 45 MOT students from one university. Student baseline trait anxiety (as measured by the Beck Anxiety Inventory) and test anxiety (as measured by the Westfield Test Anxiety Scale) are displayed in Table 1. There were no outliers for baseline anxiety or test anxiety, and measures of anxiety did not significantly decrease from baseline to the end of the intervention period.
Baseline and post-intervention scores on measures of overall anxiety (Beck Anxiety Inventory) and test anxiety (Westfield Anxiety Scale).
Impact of interventions
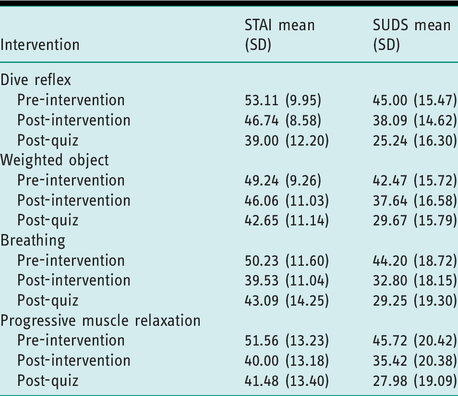
All four anxiety-reducing techniques demonstrated a statistically significant change in anxiety from pre-intervention to post-intervention when measured by both the SUDS [dive reflex, t(44) = 3.052, p = 0.0038; weighted object, t(44) = 3.723, p = 0.0006; breathing, t(43) = 9.133, p < 0.0000; PMR, t(42) = 7.552, p < 0.0000] and the STAI [dive reflex, t(43)=4.467, p < 0.000; weighted object, t(43) = 2.951, p = 0.005; breathing, t(42) = 11.095, p < 0.000; PMR, t(44) = 9.508, p < 0.000]. This reduction in anxiety was also maintained from post-intervention to post-quiz as measured by both the SUDS [dive reflex, t(41) = 7.198, p < 0.0000; weighted object, t(44) = 6.927, p < 0.0000; breathing, t(43) =6.946, p < 0.0000; PMR, t(42) = 3.400, p = 0.0015] and the STAI [dive reflex, t(39) = 8.483, p < 0.000; weighted object, t(38) = 5.569, p < 0.000; breathing, t(41) = 4.303, p < 0.000; PMR, t(44) = 5.560, p < 0.000] as well. Means and standard deviations are reported in Table 2.
Means and standard deviations of each measure (State Trait Anxiety Inventory (STAI) and Subjective Units of Distress Scale (SUDS)) at each time point (pre-intervention, post-intervention, and post-quiz).
When measuring global distress/anxiety with the SUDS, there was insufficient evidence of an interaction effect between the different anxiety-reducing techniques used and time, F(4.099, 155.766) = 2.161, p < .074, partial η2 = .054. There was a statistically significant main effect of time with a trend of improved global anxiety from pre-intervention to post-quiz, F(2.546, 63.425) = 72.181, p < 0.000, that demonstrated a large effect size (partial η2 = .655) (Cohen, 1988), but no statistically significant differences among the interventions on anxiety as measured by the SUDS F(2.546, 96.744) = 0.114, p = 0.931, partial η2 = .003.
However, for the STAI, which measured symptoms associated with state anxiety, there was a statistically significant two-way interaction between intervention and time, F(6,198) = 18.671, p < 0.000; therefore, the researchers looked at simple main effects of intervention and time. Anxiety levels when measured before the intervention were not statistically significantly different from each other, F(2.826,118.694) = 1.492, p = 0.222; but at the post-intervention measure there was a statistically significant difference in anxiety levels, F(2.920,119.720) = 12.297, p < 0.000, with the deep breathing and PMR showing a bigger reduction in anxiety. At the post-quiz measures, there again was not a statistically significant difference in STAI scores, F(2.339, 77.194) = 1.257, p = 0.293, but the trend was for the STAI scores to continue to decrease after the dive reflex and weighted object interventions post-quiz, while the scores on anxiety via the STAI increased between post-intervention and post-quiz for the breathing and PMR interventions (See Figure 1 and Figure 2).
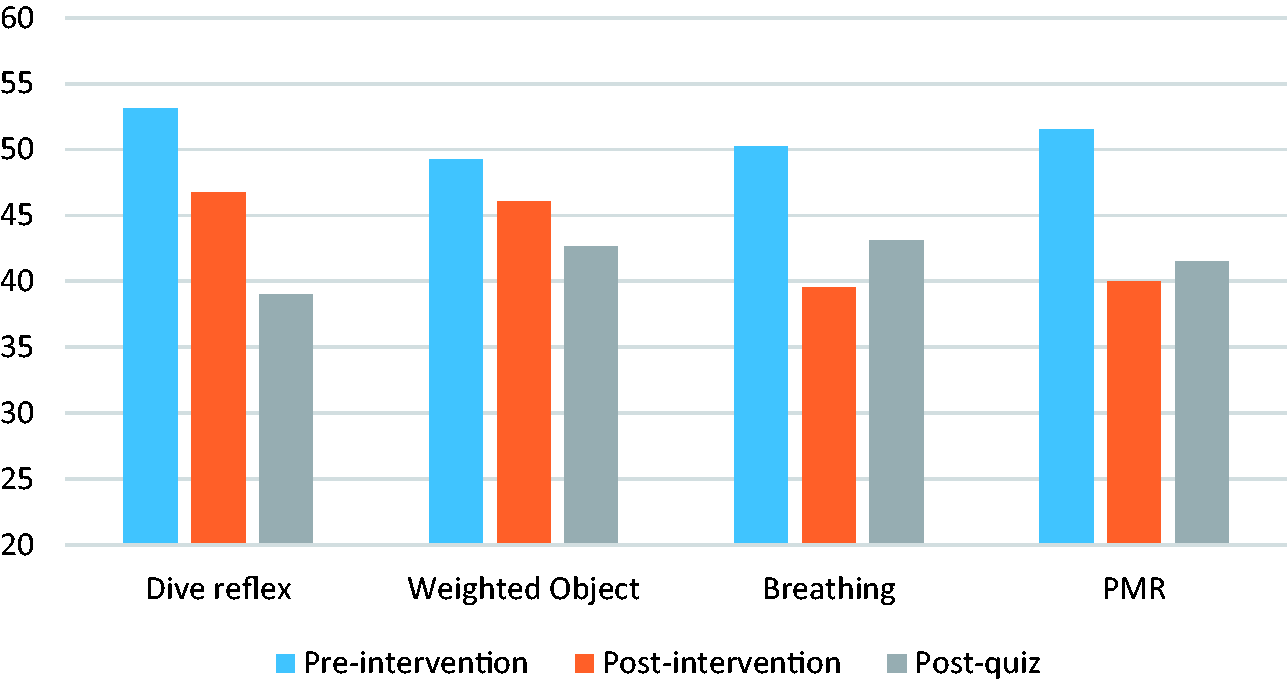
Average State Trait Anxiety Inventory scores over time (pre-intervention, post-intervention, and post-quiz) for the four techniques (dive reflex, weighted object, breathing, and PMR).

Average Subjective Units of Distress Scale scores over time (pre-intervention, post-intervention, post-quiz) for the four techniques (dive reflex, weighted object, breathing, and PMR).
Discussion
It is common for university students to have some stress or anxiety over testing situations, with some students experiencing more distress than others. Stress and anxiety impact on the occupation of education and can have consequences on academic success (Chapell et al., 2005). A testing environment has unique characteristics (for example a need to be quiet, testing with others in close proximity, feeling like one is being watched by the instructor) that can impact on performance. Personal factors need to be managed within this particular context in order to support success. The results of this study suggest that a range of anxiety-reducing techniques that include sensory modulation may help with state anxiety such as that experienced by the students in this study.
Tools that capture global anxiety and symptomology may struggle to take into account an individual’s interoceptive ability (the ability to detect internal bodily cues), which seems to have been highlighted in this study as there were discrepancies between the outcomes of anxiety when looking at the SUDS measure versus the STAI measure. The SUDS was chosen since it captured global distress/anxiety, while the STAI was chosen since it captures more body-based symptoms associated with anxiety. In this study, use of PMR and breathing exercises demonstrated a more significant drop in global anxiety levels (in the SUDS) compared to the adapted dive reflex or using a weighted object in the short term (from pre-intervention to post-intervention) and this reduction continued in all groups based on the SUDS scores. However, a reduction in body-based symptoms (STAI) in the longer term (after the quiz) with the dive reflex and weighted object was present that was not present in the STAI after the PMR or breathing interventions. Global anxiety (as measured by the STAI) actually increased in participants after the quiz when participants had used PMR and breathing. This discrepancy in measurement may be important to note as other research may be impacted by the ability of current anxiety measures to take into account multi-modal representations of anxiety or interoception as it relates to the use of sensory modulation interventions.
However, there can be other explanations for these discrepancies. First, since PMR and breathing techniques are a recognized intervention, especially among a group of professional healthcare students, the reduction in anxiety may be indicative of a placebo effect. In other words, the reduction in the SUDS could have been a learned response: “evidence says these work, so they must work.” Since the SUDS is a global measure of distress/anxiety and the score easier to recall, it may be that the students were quicker to report a lower anxiety score with PMR or breathing without actually feeling lower anxiety levels. The dive reflex and weighted object are lesser known techniques and therefore may not result in an anticipatory response. Consequently, the initial reduction in anxiety levels would be less. Second, since the dive reflex and weighted object use “bottom-up” mechanisms, it may take longer for a person to be consciously aware of their change in anxiety. This may be further influenced by an individual’s interoceptive sense and explains why there might be a discrepancy in the body-based versus more global measure of anxiety. In addition, the overall effect following the PMR and breathing interventions appeared to last for a shorter period of time compared to the dive reflex and weighted lap item interventions. It is possible that these primarily sensory-based approaches may have a longer action time in addressing anxiety and therefore could be an even more effective intervention when a reduction in anxiety requires a longer duration of effect. Finally, the body-based anxiety measures increasing after the quiz with regard to PMR and breathing may also be reflective of the timing of the intervention, as these interventions were used later in the semester. It is possible that grades and other stressors associated with the end of term may have increased student internal state anxiety.
Occupational therapy involves tailoring interventions to the individual needs and strengths of the person. Being able to offer a variety of anxiety management tools increases the likely match between the person, the task, and the environment, thus enhancing occupational performance and functioning and better supporting individual choice. This is further reinforced through the fundamental tenets of the recovery model, which actively support individuals to build expertise in self-management (Glover, 2012). Person-centered approaches support individuals to access a variety of options and interventions that best support their goals and functioning. An approach that capitalizes on personal strengths and individual choice may enhance skills in self-management and improve occupational functioning and quality of life.
The person–environment–occupation (PEO) model recognizes the impact of personal, environmental, and occupational factors on functional performance (Law et al., 1996). When a person experiences anxiety in a particular environment or when engaged in a specific occupation, options allowing the individual to change their internal condition within the constraints of the environment are necessary. A “suite of tools” to manage any anxiety-producing situation may be helpful for those with or without a high level of baseline anxiety. While cognitive-behavioral approaches continue to receive the most attention in the literature, they may not be effective for all people, environments, or occupations. For example, in certain environments or during specific activities it may not be practical to utilize cognitive-behavioral approaches due to the time, effort, and preparation they require to successfully implement. Supporting clients to explore a range of anxiety management strategies suited to their individual preferences and applicable in different scenarios is an important component of person-centered care. Sensory modulation techniques may be a viable alternative for some individuals since they require little training and can be modified to suit a diverse range of environments (Wallis et al., 2018) and for some may offer an easier, longer-lasting alternative (Appukuttan, 2016).
In ensuring the best fit between potential sensory modulation interventions and the individual, O’Sullivan and Fitzgibbon (2018) propose that interventions need to be safe, appropriate, individualized, and meaningful. This concept is presented using the acronym “SAIM” and can be applied to all anxiety-reducing techniques. The sensory modulation items that were selected for this study were a weighted item and a bag of cold water, and both were adapted to take into consideration the student’s current environment and available resources. The backpack was chosen as it was a discreet option for students to place on their lap and heavy objects were a cheap alternative to purchasing a commercial weighted product such as a weighted blanket. The researchers suggested an adapted dive reflex, since students could bring a small bag of water with them in their book bag, instead of submerging their head into a container of water. They can discreetly use the adapted strategy as an alternate and affordable option. While the researchers chose these specific techniques considering the environment, there are other sensory modulation techniques that might be important to consider due to their ease of use and potential to demonstrate similar clinically effective results. Additional techniques could include vestibular input (for example bouncing up and down for a minute or two or head movements), proprioceptive input (for example chewing on gum or candy), or other olfactory, auditory, or gustatory sensory input as alternatives.
Limitations
There are a few limitations worth considering for their impact on the study results: small sample size, lack of a control group, and diversity of the sample. Lack of a control group made it difficult to determine if the outcomes were a result of the intervention or something else. First, it is unclear if there was an anticipatory effect of reduced anxiety following the last two interventions, based on their previous two experiences in reducing anxiety. For example, the students might have experienced reduced anxiety after the last two techniques as a placebo effect as a result of the effectiveness of the first two techniques. However, this would not explain the trend of an increase in anxiety levels after the breathing and PMR techniques (the last two interventions used). The increase in anxiety levels after the last two quizzes might indicate stress over the term (for example, more generalized anxiety related to final grades). On the contrary, as discussed above, this may be a clue to the shorter duration of the effects of these cognitive-behavioral techniques compared to sensory modulation techniques. Using a control group would provide better assumptions about the changes noted in this study and if changes were a result of the intervention. Despite the small sample size, it is worth noting that the effect sizes for the significant ANOVA results were large. However, a larger sample size would have allowed the researchers to determine if anxiety and the anxiety-reducing techniques were impacted by other variables not considered by the researchers, for example grade performance, gender, or age.
The study was conducted with a convenience sample enrolled in a United States-based Master of Occupational Therapy program, who were an inherently homogenous group (occupational therapy majors, the majority of whom were white and female). When considering whether the study was impacted by a “learned” response, it is important to consider the impact of previous learning. The MOT students are taught PMR and breathing techniques in an earlier course within the program (albeit one year prior). They also learn to use the literature to plan evidence-based interventions. Since cognitive-behavioral strategies are more prevalent in the research literature, this might have biased their impression of the impact of the techniques. The students may have also been practicing these techniques since they learned them.
In a future study, the researchers had intended to recruit a control group of MOT students to address the time by intervention interaction, in addition to recruiting another university sample without previous training to use these techniques. Unfortunately, the COVID-19 pandemic has delayed this opportunity into the foreseeable future. The researchers believe that future studies could also include measurements of physiologic response to interventions (for example heart rate, blood pressure, skin temperature) to obtain more information about whether the actual versus perceived impact of the interventions can be observed. This could help explain the impact of these techniques on the physiology of the human system – any decrease in heart rate, skin temperature or blood pressure could be explored both over the long and short term.
Conclusion
Despite ongoing evidence that supports top-down cognitive-behavioral anxiety reduction techniques as a first-line treatment of state anxiety, this study uncovered a significant reduction in anxiety in students in a testing situation with the application of bottom-up approaches that rely on the theories of sensory modulation. This supports the conclusion that sensory modulation techniques and/or those that involve a bottom-up approach to anxiety reduction may be just as effective for students when facing an anxiety-inducing situation. The results of this study are promising in that by knowing that sensory modulation techniques may be effective for students in a testing situation, occupational therapy may be able to expand their reach within student populations. Further research should confirm these results, with more diverse samples and in different state anxiety situations, in order to determine the effectiveness of sensory modulation in addressing anxiety for other populations as well.
Key findings
Sensory modulation decreased state anxiety for students in a testing situation. Sensory modulation interventions had longer-lasting impacts than more traditional cognitive-behavioral strategies in this population.
What the study has added
This study supports the evidence base for anxiety-reducing techniques using sensory modulation. Occupational therapists who can introduce a range of evidence-based intervention options to individuals are actively promoting person-centered care.
Footnotes
Research ethics
Research ethics approved by Cleveland State University IRB #FY2020-125.
Declaration of conflicting interests
The authors confirm that there is no conflict of interest.
Funding
This research did not receive funding for its inception, implementation, or dissemination.
Contributorship
All authors contributed to the research process from inception to submission of this manuscript.
Consent
All research participants provided written consent prior to using their data for research purposes.