
Abstract
Introduction
Intervention studies to date have shown limited evidence of falls reduction in community-dwelling stroke survivors. This study tests the acceptability and feasibility of the Stepping On after Stroke programme in Singapore.
Method
A pre–post-intervention study design was used over a 6-month period. Falls incidence was the main outcome measure, with the recruitment process and attendance rate recorded to test feasibility. Data analysis from evaluation questionnaires (descriptive statistics) and interviews (content analysis) were applied to determine acceptability.
Results
Eight stroke participants and seven caregivers completed the programme at two community sites facilitated by two programme leaders. Stroke participants achieved full attendance over the 7-week programme but family caregivers did not (38%). All participants highlighted their acceptability of the group-based falls-prevention programme. Both programme leaders achieved 92% fidelity in session delivery. Four stroke participants fell during the study period. Stroke participants demonstrated clinically meaningful improvements in community participation at 1 month post-intervention. Family caregivers reported no changes in pre–post evaluations.
Conclusion
The Stepping On after Stroke programme appears feasible and acceptable to therapists and service users in Singapore; however, caregivers’ participation was limited. Findings can be used to further improve the programme and its methodology before testing its effectiveness in a larger-scale trial.
Introduction
Stroke survivors are at a higher risk of falls in comparison to the general ageing population. Our recent systematic review showed that reduced balance and mobility, use of sedative or psychotropic medications, disability in self-care, depression, cognitive impairment, and history of falls are associated with a high risk of falls in community stroke survivors (Xu et al., 2018). Secondary complications after a fall in stroke survivors can be critical as they not only affect stroke survivors in mobility and self-care (Weerdesteyn et al., 2008) but also increase the care burden on their caregivers (Greenwood et al., 2009). As a majority of stroke survivors are discharged home with follow-up services in the community, an effective falls-prevention programme for community-living stroke survivors is needed.
A recent Cochrane review concluded that no falls-prevention programme for the stroke population has been found effective, except using a vitamin D supplement in the institutionalized setting to reduce falls among women after stroke (Verheyden et al., 2013). The review further concluded that single exercise-based interventions have no effect on falls-risk reduction in people with stroke and suggested that falls prevention after stroke should be multi-component (Verheyden et al., 2013). One randomized controlled trial study was conducted to investigate the effectiveness of using a 12-week simplified tai chi programme in reducing falls in community stroke survivors (Taylor-Piliae et al., 2014). The results from this study were not promising as only number of falls were provided but no falls risk analysis (for example risk ratio) and the follow-up period was only 12 weeks.
The Stepping On programme (Clemson et al., 2004) is a multifaceted falls-prevention programme proven to be effective in reducing falls by 31% (relative risk = 0.69) in community-dwelling older adults. The programme covers a 7-week, group-based intervention followed by a home visit and a 3-month booster session facilitated by a trained programme leader. It uses adult learning principles to help older adults in a small group to learn different falls-prevention strategies and encourage behavioural change in everyday life (Clemson et al., 2004). Stepping On was originally developed in Australia and has now been implemented in the United States of America (USA) in the well elderly (Mahoney, 2015). Recent studies confirmed the key elements of Stepping On and areas for further improvement when translating and implementing Stepping On into the USA context (Mahoney et al., 2017; Schlotthauer et al., 2017). However, Stepping On has not been tested specifically for falls prevention in the post-stroke population.
In adapting the Stepping On programme for stroke survivors in Singapore as an intervention to reduce their risk of falls and increase community participation, the Stepping On after Stroke (SOAS) programme for community-dwelling stroke survivors was developed following a systematic review (Xu et al., 2018), interviews with stakeholders (Xu et al., 2019b), focus groups with programme leaders (Xu et al., 2019c), and a Delphi expert review (Xu et al., 2019a).
This paper reports on the acceptability and feasibility study carried out to assess whether (a) the SOAS programme meets the health, social, and care needs of community-dwelling stroke survivors and also their caregivers through participation in an education and support programme; (b) the outcome measures are relevant and applicable; and (c) the programme is culturally relevant within the Singapore context. These findings will be used to design a larger-scale study.
Methods
Design
To design, evaluate and implement a newly developed healthcare intervention in a multicultural society (Singapore), it is highly recommended that a small-scale study is conducted to test its acceptability and feasibility (Eldridge et al., 2016; Sekhon et al., 2017). As part of the process in developing the SOAS programme, a pre–post-intervention study design was used during the intervention phase followed by 6 months observational follow-up. All participants received written information about the study and gave informed consent. Ethics approval was obtained from the Independent Review Board in the National University of Singapore in 2016.
Participants
A recruitment flyer was sent to six community rehabilitation centres, one stroke support centre, and a community hospital 2 months before the study. The inclusion criteria for stroke participants were: aged 50 years and above, diagnosed with stroke within 5 years, medically stable, able to walk for a minimum of 10 metres unsupported (with or without aid), has concerns about falling or had a post-stroke fall in the past 6 months, able to communicate verbally in conversational English or Mandarin, cognitively intact (score of ≥8) (according to the Abbreviated Mental Test (AMT)), and lives with at least one caregiver (either family member or foreign domestic helper). The following exclusion criteria were applied: unable to express verbally or understand verbal instructions, cognitively impaired (AMT<8), wheelchair-bound or bed-bound, or medically unstable (for example unstable angina, untreated fits).
Stroke survivors who met the inclusion criteria were referred to the researchers by the centre therapist(s). The first author explained the study details to the stroke clients face-to-face and obtained written consent prior to the initial screening for eligibility. The stroke client’s family members and/or foreign domestic helpers (also called ‘maids’) were invited to take part in the study if they could speak conversational English or Mandarin.
Five occupational therapists from the two participating organizations who completed the Stepping On leader training were invited to lead the SOAS programme in their workplace. Prior to the commencement of this study, they received an additional half-day training session on the SOAS programme, including changes to the original Stepping On programme and additional key elements (Table 1) identified in our previous studies (Xu et al., 2019a; Xu et al., 2019c).
Key features of the Stepping On after Stroke programme
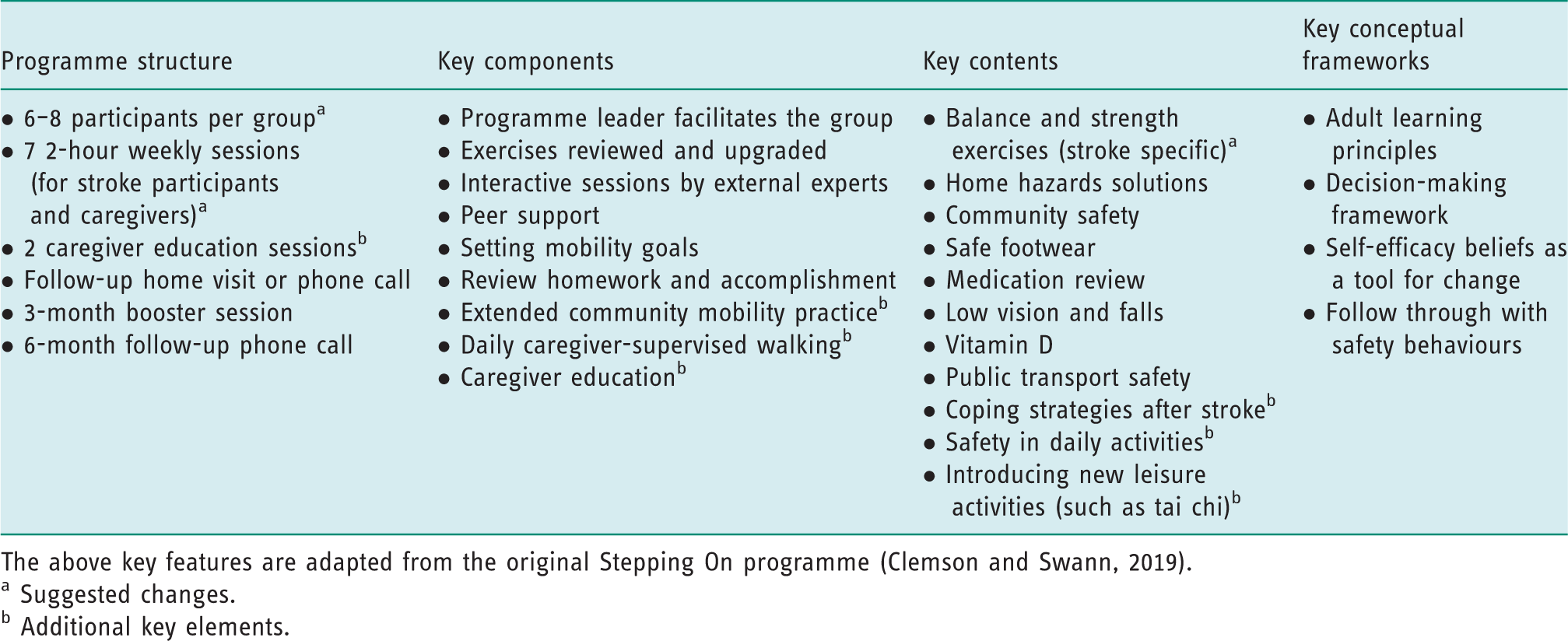
The above key features are adapted from the original Stepping On programme (Clemson and Swann, 2019).
a Suggested changes.
b Additional key elements.
Programme intervention
The programme incorporates the principles of self-efficacy and adult learning, use of the preventive framework in decision-making to facilitate positive behavioural changes, and development of falls-prevention strategies for a long-lasting effect (Clemson et al., 2004). These components were confirmed as key elements in Stepping On by international expert panel members in a Delphi study (Mahoney et al., 2017).
The SOAS programme for stroke participants included seven weekly group sessions focusing on different falls-prevention topics (Table 1) delivered by experts from different fields and facilitated by a trained programme leader. These were followed by a home visit 4 weeks post-intervention, a booster session 3 months post-intervention, and a follow-up phone call 6 months post-intervention. The family caregivers and/or maids were invited to the weekly sessions. In addition, caregivers were invited to participate in two education sessions (Week 1, Week 7).
Data collection
Feasibility
The recruitment process was recorded and evaluated by the number of referrals and eligible participants, reasons for rejections or withdrawals, and acceptance rate in each centre. Feasibility of the group intervention was assessed by weekly attendance rate, where achieving 75% would be considered as feasible (Smeulders et al., 2009).
Acceptability and applicability
Programme evaluation
The programme evaluation questionnaire was designed by drawing on the key features for implementation in the Stepping On manual (Clemson and Swann, 2019). It consists of six categories with 23 items each scored on a 5-point Likert scale, and open-text response options under each category (see online appendix for sample questionnaire). The questionnaire was translated into Chinese using a back-translation method for Mandarin-speaking participants. All stroke participants and caregivers were invited to self-complete relevant sections of the questionnaire at three timepoints: following the 7-week intervention, following the home visit, and following the booster session. For example, the ‘home visit’ section was completed after the home visit occurred. General feedback was collected on the programme structure, outline, content, cultural relevancy, duration, timing, quality of programme leaders, programme location, and challenges. A follow-up phone call was made if any participant did not return the completed survey form.
Weekly field notes
Programme leaders recorded field notes after each weekly session; any feedback/comments by the participants were then discussed with the first author.
Interviews with the programme leaders
A semi-structured interview to gather feedback from programme leaders was conducted by the first author upon completion of the 3-month booster session. Feedback was sought on: implementing the SOAS programme in the workplace; what went well with the programme; what areas could be improved; personal views on the use of pre–post outcome measures; and potential issues the programme leader or their organization might face when implementing the SOAS programme in the future. Interviews were audio-recorded with permission.
Fidelity check
The fidelity checklist used was developed by Mahoney and colleagues through a root cause analysis (Mahoney et al., 2016) and a Delphi expert review (Mahoney et al., 2017), which lists the key elements of the original Stepping On programme. The checklist includes 42 items on the input and quality of the programme leader and level of participant engagement. This was assessed by the first author in sessions 4 and 5 of the 7-week programme. The checklist assessed whether an event ‘occurred/did not occur’ and rated the knowledge and skills applied in facilitating the programme (for example ‘not done at all – 0’, ‘not satisfactory – 1’, ‘satisfactory – 2’, or ‘excellent – 3’). Comments on the areas that went well and recommendations for further improvement were recorded. Comments and recommendations were shared with the programme leader after sessions in weeks 4 and 5.
Primary outcome
All stroke participants were asked to complete the monthly falls calendar throughout the study period. Post-7-week intervention, the first author telephoned stroke participants every month to find out if they had had any fall(s) and reminded them to complete the falls calendar; further verification was carried out with the caregivers. In the event of a fall(s) being recorded in the falls calendar, details of the fall incident(s), including number, fall pattern, location, and time of fall(s), were obtained and recorded separately by the first author. All monthly falls calendars were collected by the first author every month in the first 3 months and at 6-month follow-up.
Secondary outcomes
The pre–post evaluations were conducted by the first author and programme leaders at two time points: a 2-week period before commencement of the intervention and within 1 month following the intervention. Outcome measures used for stroke participants include the Falls Efficacy Scale – International (FES-I) to assess any improvements in falls-related self-efficacy; the Falls Behavioural Scale to detect any changes in the use of safety strategies in self-care among the stroke participants; the Life-Space Assessment (LSA) and the modified Reintegration to Normal Living Index (mRNLI) to detect any improvements in community participation; and the Goal Attainment Scale (GAS) to find out their personal achievements at the end of the programme. As suggested by a GAS practical guide (Turner-Stokes, 2009), three goals per participant were reviewed to calculate the extent of personal goal achievements. The Short Physical Performace Battery (SPPB) was also used to evaluate balance and mobility since it is a reliable tool in detecting physical performance and mobility (Freire et al., 2012). The outcome measures used for caregivers included the SF-12 Health Survey (SF-12) and the modified Caregiver Strain Index (mCSI) to assess their changes in health-related quality of life and level of stress.
The validated Chinese version of all self-rated questionnaires was used for participants who only speak Mandarin, with the exception of the Falls Behavioural (FaB) Scale, which does not have a validated Chinese version. The FaB Scale was translated into Chinese with back-translation by the first author and another clinical staff member fluent in both English and Mandarin. The translated version was further checked for accuracy by an official translator.
Data analysis
To determine the acceptability and feasibility of implementing the SOAS programme with community stroke survivors and their caregivers, graphs and descriptive statistics were generated to show trends. Data gathered from interviews, weekly field notes, and programme evaluation questionnaires (open-text responses) were analysed by two research team members (TX, KOL) independently using content analysis to identify and code recurrent themes. A conventional content analysis approach (Hsieh and Shannon, 2005) was used since the main categories drew on the guided interview responses and open-text evaluation questionnaire responses.
Clinical data from the pre–post evaluations were analysed using IBM® SPSS® for Windows, Version 22 (IBM Corp). Given the small sample size in this study, a non-parametric Wilcoxon signed-rank test was used to compare the means of all pre–post measurement outcomes (Woolson, 2008). The level of statistical significance was set at p<0.05 for all analyses. The effect size was calculated based on the recommendation of Cohen’s power analysis (Cohen, 1992).
Results
Feasibility
As shown in Figure 1, a total of 22 stroke participants, 12 family caregivers, and four maids were referred from four rehabilitation centres and one stroke support centre for eligibility screening between October and November 2016. Eleven stroke participants met the inclusion criteria and participated in the Stepping On programme across the two study sites. Three stroke participants declined to participate following screening due to inaccessibility/lack of transport to the study location and/or personal reasons (for example not interested).
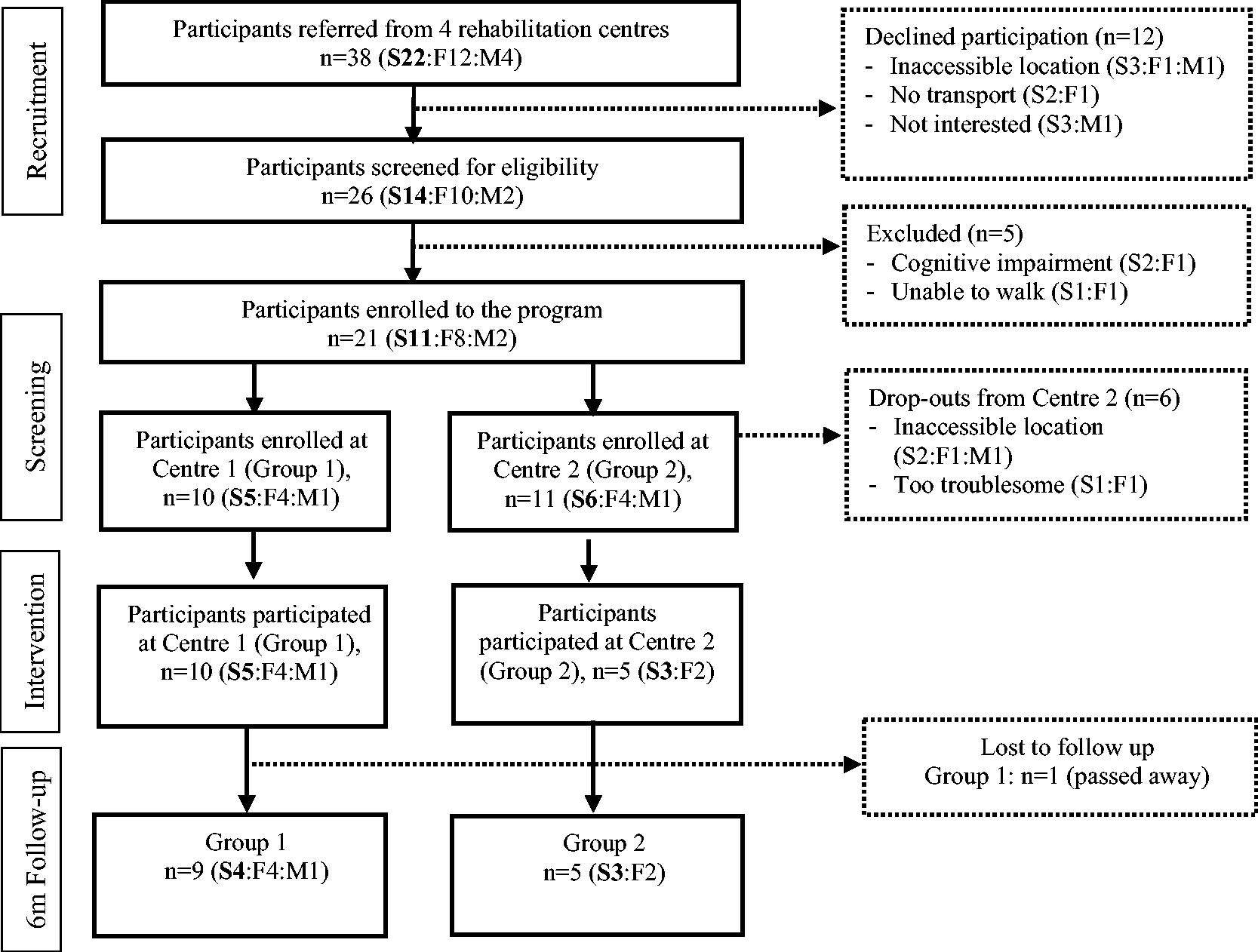
Recruitment/flow of participants through the study.
A total of eight stroke clients, six family caregivers and one maid from two groups completed the programme: Group 1/Centre 1 consisted of five stroke participants, four family members and one maid; Group 2/Centre 2 consisted of three stroke participants and two family members. All participants who commenced the Stepping On programme were retained at 3-month follow-up; one stroke participant from Group 1 was deceased at 6-month follow-up due to a road traffic accident. The summary of baseline demographics and characteristics of the stroke participants are shown in Table 2 (see Table S1 for more details).
Baseline demographics and characteristics of stroke participants (n = 8).
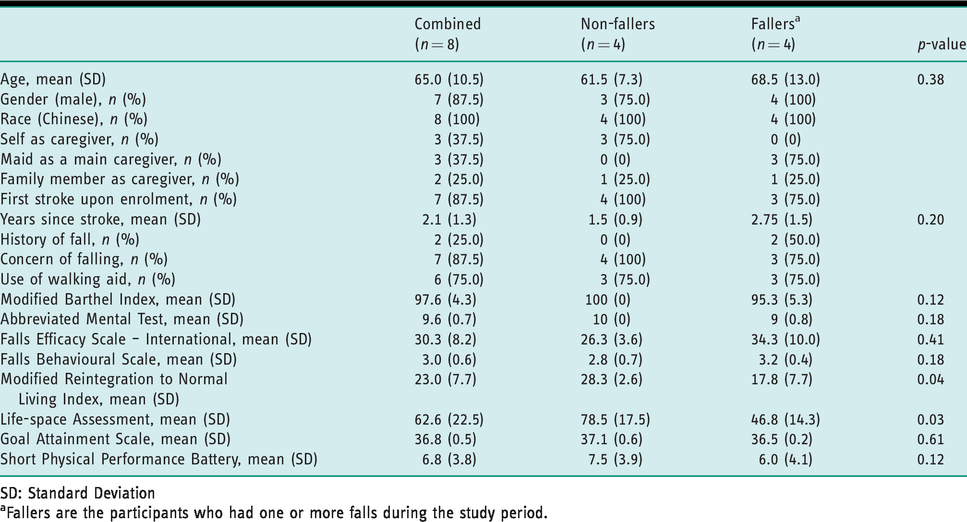
SD: Standard Deviation
aFallers are the participants who had one or more falls during the study period.
The two programme leaders had between 3 and 4 years of clinical experience working with both older adults and stroke clients; however, neither had any experience in running a structured falls-prevention programme prior to the study. The main duty in their current position was to provide community-based rehabilitation therapy services to the clients.
Attendance
All stroke participants in both groups had full attendance during the 7-week intervention. In Group 1, attendance for family members and the maid was 25% and 100% respectively; Group 2 was 64% and 100% respectively (see Table S1). For the caregiver education sessions, two family caregivers and the maid from Group 1 attended in week 1, with none attending in week 7. For Group 2, none of the participants attended either of the sessions. Home visits were conducted with seven of the stroke participants; one participant from Group 2 declined a home visit and therefore was followed up at the rehabilitation centre. Four stroke participants with two family caregivers and the maid from Group 1 attended the booster session. Participants who did not attend were followed up with a telephone call.
Acceptability and applicability
Five major themes emerged from the content analysis of programme leader interviews, weekly field notes and open-text questionnaire responses. These were: acceptance of the group-based falls-prevention programme; relevance and applicability of the outcome measures; importance of programme leaders in group facilitation; challenges in running the programme; and recommendations for future implementation.
Acceptance of the group-based falls-prevention programme
A total of 10 completed programme evaluation questionnaires were collected from four stroke participants and three caregivers who attended the booster session and another stroke participant and two family members who did not attend the booster session. The majority of stroke participants agreed that the duration, timing, structure, and outline of the SOAS programme were adequate and resources provided, such as participant handouts and reading materials, were very useful. All participants agreed that programme leaders and invited experts were knowledgeable and able to facilitate their discussion and learning in falls-prevention. All stroke participants did balance and strength exercises at home regularly; most stroke participants practised daily walking with their caregivers in the outdoor environment; another stroke participant practised daily walking by using his wheelchair as a walking aid for better balance; two stroke participants had grab bars installed in the shower room and toilet; one stroke participant had an eye check-up; and one stroke participant had his medications reviewed by his family physician. All stroke participants commented that the balance and strength exercises and simplified tai chi were useful in making them more steady.
During the interview after the booster session, both programme leaders highlighted the applicability of conducting group-based falls-prevention programmes in the local context. They were satisfied with the group performance throughout the 7-week intervention period, as most participants in both groups benefited from peer learning and group discussion. Leader B shared: ‘I think it was because of the social group. “If you can, I also can do it”. It’s the group dynamics that make it work.’
Relevance and applicability of the outcome measures
The outcome measures for stroke participants were relevant and applicable in detecting the changes in their level of self-efficacy, behaviours in performing self-care activities, level of community integration, goal achievement, and physical functions. However, programme leaders commented that the FaB Scale and FES-I were too long to administer routinely in a clinical setting and some questions in the mRNLI were difficult to understand. In addition, programme leader B highlighted that ‘some questions in the modified Caregiver Strain Index are not so applicable’ for maids, for example, ‘Caregiving is confining’ and ‘Caregiving is a financial strain’.
Importance of programme leaders in group facilitation
Both programme leaders acknowledged the importance of having clinical experience in stroke rehabilitation and good facilitation skills in their role as programme leader. Leader A shared: As a facilitator, I guess I did learn about facilitating, such as how to get participants to reflect and to ask more appropriate questions; how to include the quieter ones and share stories of their own experiences to help them understand things that they learned…
Challenges in running the programme
Despite the successful completion of the programme, both programme leaders encountered some challenges during the intervention.
Firstly, there may have been excessive falls-prevention content delivered by the invited experts that made it difficult for stroke participants to absorb. Leader B expressed: ‘Sometimes I am not sure if our information in the educational sessions is too much as compared to the well elderly group… we don’t know how much they absorbed’. Secondly, the stroke-specific balance and strength exercises were quite overwhelming and challenging, and it took longer to review these exercises than the allocated time within each session. Thirdly, the community mobility practice session was time-consuming and staff-intensive, as raised by Leader B: ‘I think community mobility practice will need more staff’. Lastly, the family caregivers were not fully engaged during the weekly sessions and only two caregivers attended the caregiver education session. Leader A commented: I also [find it] hard to coordinate the caregivers. Most of them, because of the working hours, a bit hard to be present throughout [the programme]. For those who were there, I am sure they benefitted, I feel I didn’t have enough time to talk to them.
Recommendations for future implementation
Based on their experience in running the SOAS programme, both programme leaders recommended having longer sessions or additional sessions given extensive information about stroke covered in 7 weeks. Leader A shared: ‘I wonder if there’s a block of time to talk about neurotherapy, maybe allocate one session on [that] would make them think even more or answer some of their questions’.
Both leaders also highlighted the importance of engaging the caregivers in motivating the stroke participants at home. For instance, Leader B highlighted: ‘I think it’s about how to motivate the caregivers to motivate the patients at home’. In addition, community resources, such as therapy equipment, sufficient staff, and space are essential in running such a group-based programme in the community. As stated by Leader B: Resources might be an issue, especially therapy equipment, as these are shared by different programmes. We might need to have our own equipment. Maybe another staff, like therapy assistant will be good to help us run the group. Another thing is space. We need room to run this group.
Fidelity of the programme
An average of 92% fidelity was achieved from the fidelity checks conducted in sessions 4 and 5 for the programme leader at each site. The only event which was rated as ‘did not occur’ was ‘demonstrated and passed around inappropriate shoes’ from both leaders. Items in relation to the leader’s quality rating of ‘excellent’ included: carrying out the balance and strength exercises; discussing the frequency of exercises; engaging the class in group discussion; assigning homework; pace; and demonstrating good knowledge in the relevant falls-prevention topics. Items in relation to the leader’s quality rating of ‘not done at all – 0’ and ‘not satisfactory – 1’ included: upgrading the exercises using ankle weights; facilitating stories on how to fit exercises into one’s daily routine; prompting for questions during the expert session; reviewing key messages from the experts; and demonstrating skills in storytelling.
Primary outcome
Baseline characteristics of the fallers and non-fallers are shown in Table 2. Fall data were collected for a total of 8 months from baseline. There were four (50%) recurrent fallers and four (50%) non-fallers during the study period. The people who fell were also those with lower mRNLI and LSA scores. Three (75%) of the four who fell twice during the study period had an injurious fall each. For instance, one stroke participant’s fall resulted in a forehead laceration while getting up from the bed 2 months after the 7-week intervention; another two participants had injurious falls resulting in ankle sprain and clavicle fracture when walking unsupervised at home during the 3–6 months follow-up period. All fallers were sent by their family members to the neighbourhood clinic for immediate medical attention. The breakdown of fall locations can be found in Table S2.
Secondary outcomes
Table 3 shows the mean scores of the different outcome measures at the baseline and at 1-month post-intervention follow-up in stroke participants and family caregivers.
Participants’ status at baseline and 1-month post-intervention follow-up, mean (SD).
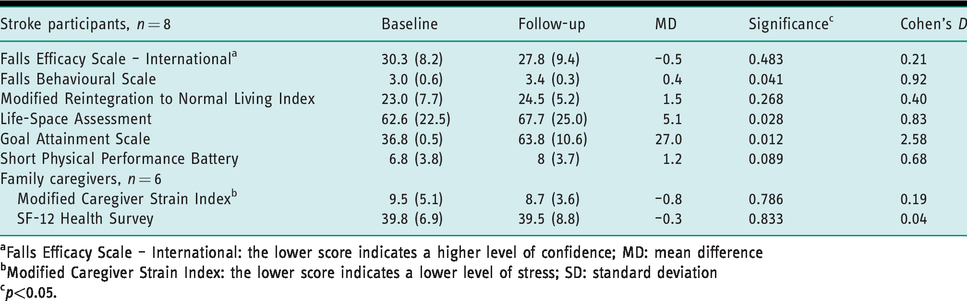
aFalls Efficacy Scale – International: the lower score indicates a higher level of confidence; MD: mean difference
bModified Caregiver Strain Index: the lower score indicates a lower level of stress; SD: standard deviation
cp<0.05.
At 1-month follow-up, stroke participants demonstrated positive changes with large effect sizes (Cohen, 1992) in the FaB Scale (p = .041; d = 0.92), LSA (p = .028; d = 0.83) and GAS (p = .012; d = 2.58) when compared to the baseline. Examples of goals that the stroke participants achieved towards the end of the study period are shown in Figure S1. There were no differences at 1-month follow-up for FES-I, mRNLI, and SPPB.
The results showed no changes among the family caregivers in both the SF-12 (p = .833) and mCSI (p = .786). The maid who participated was the main caregiver of one stroke participant (G1-P05, a recurrent faller). Her stress level had increased at the post-evaluation (mCSI = 4) compared to the baseline (mCSI = 7); however, her general health status was scored higher (SF-12 = 41) at the post-evaluation than the baseline (SF-12 = 32).
Discussion
This was the first small-scale study associated with implementing the newly developed SOAS programme. Our data suggest that the group-based falls-prevention programme for stroke survivors is feasible and acceptable in the local community setting, as evidenced by full attendance from the stroke participants in the 7-week programme. While men traditionally report difficulty engaging in chronic disease management programmes (Marsden et al., 2010), our male stroke participants had full attendance. This may be partially attributed to the group set-up and the active learning environment that the participants experienced. Group-based community programmes are well supported by several established evidence-based falls-prevention programmes, such as Stepping On (Clemson et al., 2004), Otago Exercise Programme (Campbell and Robertson, 2003), and Tai Chi – Moving for Better Balance (Li et al., 2008), and have been shown to be cost-effective in fall reduction in community-dwelling older adults (Carande-Kulis et al., 2015). However, the effectiveness of the group-based falls-prevention programme specifically for community-dwelling stroke survivors is yet to be tested.
A unique feature in the SOAS programme was the involvement of family caregivers and maids during the weekly sessions. As our findings suggest, the acceptability of the SOAS programme was established with the caregivers; however, feasibility in relation to caregivers was not well achieved given their low attendance rate. An explanation for this could be that, since the mean time from stroke onset among stroke participants was 2.1 years, most caregivers had already developed some coping strategies. Their low attendance rate during the weekly sessions and caregiver education sessions most likely affected their learning outcomes, resulting in no significant changes in their health status and stress level between pre–post measures.
To boost caregivers’ attendance in future studies, the biopsychosocial needs of caregivers at different phases should be considered. For instance, the majority of stroke survivors in Singapore were accompanied by either a family caregiver or a maid as they required supervision or assistance in travelling from their home to the rehabilitation centre. As highlighted in our previous study, family caregivers and maids often demonstrate over-protective behaviours to keep stroke survivors safe (Xu et al., 2019b). This could result in activity restriction and further functional deterioration to the stroke survivors. Though our data did not show any positive outcomes among the family caregivers, it suggests that caregiver education could start earlier in the stroke recovery phase as the risk of falling among the stroke survivors is high in the first few months post discharge (Mackintosh et al., 2006). This could potentially reach out to more caregivers who need the necessary information to provide care for their loved ones post stroke.
In this study, participant recruitment was mainly affected by the location of the implementation sites and the difficulty of accessing them by public transport. Future studies should consider the accessibility of the study sites and the availability of transportation services. Also, future recruitment should reach out to more community rehabilitation centres where most stroke survivors in Singapore are followed up for continuous rehabilitation 4 to 6 weeks post stroke. We also suggest the use of other communication channels, including social media, during recruitment to reach out to more stroke survivors and caregivers.
Our qualitative data suggest that most outcome measure tools are applicable and culturally relevant. In recent years, SPPB has been recommended by Singapore’s Ministry of Health and Health Promotion Board in assessing older adults with disabilities for health-related services and programmes in community settings (Lee et al., 2016). However, mRNLI needs to be reviewed. Difficulties may be due to the language used in the validated Chinese version of mRNLI, which was developed in Hong Kong (Pang et al., 2011). Future studies should look into the cross-cultural validation of the mRNLI to meet the various language requirements in the Singapore context and the adaptation of the mCSI to be more relevant for maids as caregivers.
Data from the interview findings suggest that the programme should have an additional session to cover more content (for example coping strategies after stroke) and provide more intensive and stroke-specific exercises, as suggested by the experts in our Delphi review (Xu et al., 2019a). The number of sessions in other community-based stroke programmes differ; for instance, one self-management programme after stroke consists of six weekly group sessions (Marigold et al., 2005), whereas other stroke programmes focusing on exercises consist of eight sessions (Eng et al., 2003). While the SOAS programme aims to reduce fall risk and increase community participation in community-dwelling stroke survivors, stroke survivors should be given sufficient time to process new information and develop coping strategies to regain self-efficacy in self-management (Jones and Riazi, 2011).
The findings from the fidelity checks indicated a need for further improvement in programme leaders’ facilitation skills, since an experienced programme leader is essential to facilitate group discussion and promote peer learning within a small group. Well-trained programme leaders have been reported as one of the key elements in the Delphi expert review (Mahoney et al., 2017). In consideration of the challenges in implementing the SOAS programme, we recommend programme leaders should be healthcare professionals who have worked with the stroke population. Additional training for programme leaders, including workshops focusing on evidence-based falls-prevention strategies, group facilitation skills, and exercise upgrading methods, would improve the programme fidelity (Mahoney et al., 2016). Further, hands-on training sessions with older adults in real community settings supervised by an experienced programme leader/master trainer would allow new programme leaders to receive instant feedback before programme implementation.
It is difficult to interpret the results of our feasibility study given the lack of a control group and small sample size. However, 50% of participants fell during the follow-up, which is similar to other cohort and case-control studies (Persson et al., 2011; Simpson et al., 2011; Yates et al., 2002). Of those participants who did fall, all experienced more than one fall. In comparison to those who did not fall (Table 2), the four participants who fell were older, were a longer period from stroke onset, and had lower levels of community participation. Furthermore, they had poorer physical function and required a caregiver because of a higher level of need for assistance in self-care, all of which increases their risk of falling post stroke (Xu et al., 2018). Nevertheless, our stroke participants, including those with falls, were able to achieve the majority of their goals (see Figure S1), as reported by positive changes in their GAS scores. In addition, most stroke participants reported clinically important improvements in implementing safety strategies (FaB Scale) as well as increased community participation (LSA). As reported in our previous interview study (Xu et al., 2019b), community stroke survivors in Singapore rate highly the importance of being socially connected and living independently in the community. Individualized safety strategies should be developed and reinforced as part of the goal-setting process in a community-based programme as it encourages the participants to be more active learners and better self-managers in reducing their risk of falling. Perhaps in future studies researchers should consider focusing on increasing the level of community participation as well as falls efficacy, rather than purely focusing on the reduction of fall risks.
The results should be interpreted with caution as there were several limitations in this study. First, the relatively small sample size limits the generalizability of the results and the statistical power in calculating the effect size. Small group size also affects the dynamics of group discussion and peer learning. Second, all stroke participants were Chinese and the majority (88%) of them were males. The results may not be representative of the whole stroke population since Singapore is a multicultural society. Third, there was no control group in this study, which also limits the isolation of the effects of SOAS from normal rehabilitation. Fourth, lacking independent assessors in this study may increase the risk of intervention bias. More rigorous research methodology should be used when designing larger-scale trials.
Conclusion
The Stepping On after Stroke programme appears to be feasible for future implementation in Singapore and acceptable to therapists, stroke survivors and their caregivers. While the inclusion of caregivers is essential, their participation was limited in this study; recommendations have been made for future implementation. The study findings can be used to further improve the programme and its methodology prior to testing its effectiveness in a larger-scale study. Further, the results suggest that future studies with post-stroke clients focus on both falls and community participation as the major outcomes.
Key findings
The adapted Stepping On programme for community stroke survivors is feasible and acceptable in the Singapore context. The newly developed Stepping On after Stroke programme has potential to increase community participation in community stroke survivors.
What the study has added
Consideration should be given to community participation as a major outcome measure in any falls-prevention programmes.
Supplemental Material
sj-pdf-1-bjo-10.1177_0308022620946640 - Supplemental material for Stepping On after Stroke falls-prevention programme for community stroke survivors in Singapore: A feasibility study
Supplemental material, sj-pdf-1-bjo-10.1177_0308022620946640 for Stepping On after Stroke falls-prevention programme for community stroke survivors in Singapore: A feasibility study by Tianma Xu, Lindy Clemson, Kate O’Loughlin, Natasha Lannin, Catherine M Dean and Gerald Koh in British Journal of Occupational Therapy
Supplemental Material
sj-xlsx-2-bjo-10.1177_0308022620946640 - Supplemental material for Stepping On after Stroke falls-prevention programme for community stroke survivors in Singapore: A feasibility study
Supplemental material, sj-xlsx-2-bjo-10.1177_0308022620946640 for Stepping On after Stroke falls-prevention programme for community stroke survivors in Singapore: A feasibility study by Tianma Xu, Lindy Clemson, Kate O’Loughlin, Natasha Lannin, Catherine M Dean and Gerald Koh in British Journal of Occupational Therapy
Supplemental Material
sj-jpg-3-bjo-10.1177_0308022620946640 - Supplemental material for Stepping On after Stroke falls-prevention programme for community stroke survivors in Singapore: A feasibility study
Supplemental material, sj-jpg-3-bjo-10.1177_0308022620946640 for Stepping On after Stroke falls-prevention programme for community stroke survivors in Singapore: A feasibility study by Tianma Xu, Lindy Clemson, Kate O’Loughlin, Natasha Lannin, Catherine M Dean and Gerald Koh in British Journal of Occupational Therapy
Footnotes
Acknowledgements
The authors would like to acknowledge the following voluntary welfare organizations who assisted with the subject recruitment and implementation of this project: SPD, St Luke’s Eldercare Ltd, Wellness Kampung @ 765 (Nee Soon Central), and Stroke Support Station.
Research ethics
Ethics approval was obtained from the Independent Review Board of the National University of Singapore (Reference code: B-16-163) in 2016. The study protocol was registered with the Australian New Zealand Clinical Trials Registry (ACTRN12616001195448).
Consent
All participants provided written informed consent.
Declaration of conflicting interests
The authors confirm that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this work was supported by the Singapore Association of Occupational Therapists. Professor Lannin is supported by a Future Leader Fellowship (Award ID 102055) from the National Heart Foundation of Australia.
Contributorship
All authors contributed to the study design including protocol development and data analysis plan. Data was collected by TX, quantitative analysis was conducted by TX and LC and qualitative analysis by TX and KOL with further interpretation involving NL, CMD and GK. TX wrote the first draft of the manuscript, all authors commented on and/or amended this and all authors read and approved the final manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.