
Abstract
Introduction
Reablement services support people to regain skills and increase their independence. This aim resonates with occupational therapy philosophy. This article presents results of a study of the role of occupational therapists in reablement services that involve two organisations.
Method
Theories on the role of occupational therapists in reablement were identified using a realist synthesis approach and were tested and expanded using a qualitative case study design. Each of the three case studies consisted of one reablement service in England. Methods of the study included observations and interviews with occupational therapists, interviews with managers in both organisations and focus groups and interviews with reablement support workers.
Findings
Findings conclude that occupational therapists’ education and experience underpin their ability to undertake assessments and person-centred goal setting. They utilise a range of intervention techniques selecting from their toolbox of interventions to support people. Occupational therapists have a role in training reablement support workers to work in an enabling way. Regular communication and co-location support levels of trust and shared purpose between members of the reablement team.
Conclusion
The conceptual framework developed from the study can be used by organisations when commissioning and developing reablement services to consider the different contextual layers of reablement.
Introduction
Reablement is a time limited service, working with people in their own home to regain skills with an aim of increasing independence and reducing the need for ongoing support (National institute for Health and Care Excellence, 2017; Skills for Care, 2019). Reablement services are developing internationally. In the United States, Australia and New Zealand, services are called restorative care, with a definition in line with reablement, as a restoration of ability and promoting independence (King et al., 2012).
In the United Kingdom the Care Act 2014 in England, the Social Services and Wellbeing (Wales) Act 2014 and the Public Bodies (joint working) (Scotland) Act 2014 place a duty on Local Authorities to provide services to prevent or delay the need for care and support, and cite reablement as a service to meet this duty. With the exception of Northern Ireland, who published a Regional Reablement Pathway for use by Health and Social Care Trusts (Health and Social Care, 2016), there is no blueprint for the delivery of reablement. In the United Kingdom, Local Authorities may provide reablement ‘in-house.’ In the last decade, approximately one quarter of Local Authorities have provided reablement with another organisation, typically a domiciliary care agency (Beresford et al., 2019; Care Services Efficiency Delivery, 2012). Occupational therapists in reablement have been identified primarily as providers of equipment and adaptations and also professionals who can provide guidance and training to reablement support workers to work in a reabling way (Littlechild et al., 2010; McLeod and Mair, 2009).
A need for qualitative studies to explore the views of practitioners in reablement has been identified (Beresford et al., 2019; National institute for Health and Care Excellence, 2017). This study explored the role of occupational therapists working in reablement services in England that commissioned an independent organisation alongside the Local Authority.
The study aimed to answer the following research questions: •How can we critically understand the role and impact of occupational therapists working in reablement services? •What is the experience of occupational therapists working in reablement services, and what contexts and mechanisms affect the outcomes of their practice for people using reablement services, their carers and members of the reablement team?
The study used a realist approach. Realist evaluation seeks to build theories around what works, for whom and in what circumstances (Pawson, 2006). It considers the influence of legislative, institutional and physical contexts and seeks to analyse the causal mechanisms (the unseen reactions, choices and capacities of people) that lead to positive or less positive outcomes of an intervention.
Literature review
Employing a realist approach, a review of the literature was undertaken, using the five stages of realist synthesis. The intended product of a realist review of the literature is a set of programme theories which seek to identify the intended outcome of the intervention and the contexts and mechanisms that affect the success, or otherwise, of meeting that outcome. (Pawson, 2006).
The first stage, identifying the review question for the literature search, was achieved by contacting experts in the field. Telephone conversations were held with five occupational therapists working in reablement to identify initial theories concerning the role of occupational therapists in reablement services. The second stage, the literature search, (Figure 1) included articles that referenced occupational therapists and terms for social care and worldwide terms for reablement including restorative care. Fourteen databases were searched covering health, social care, sociology and humanities to locate relevant literature from a broad range of sources. Process of screening articles.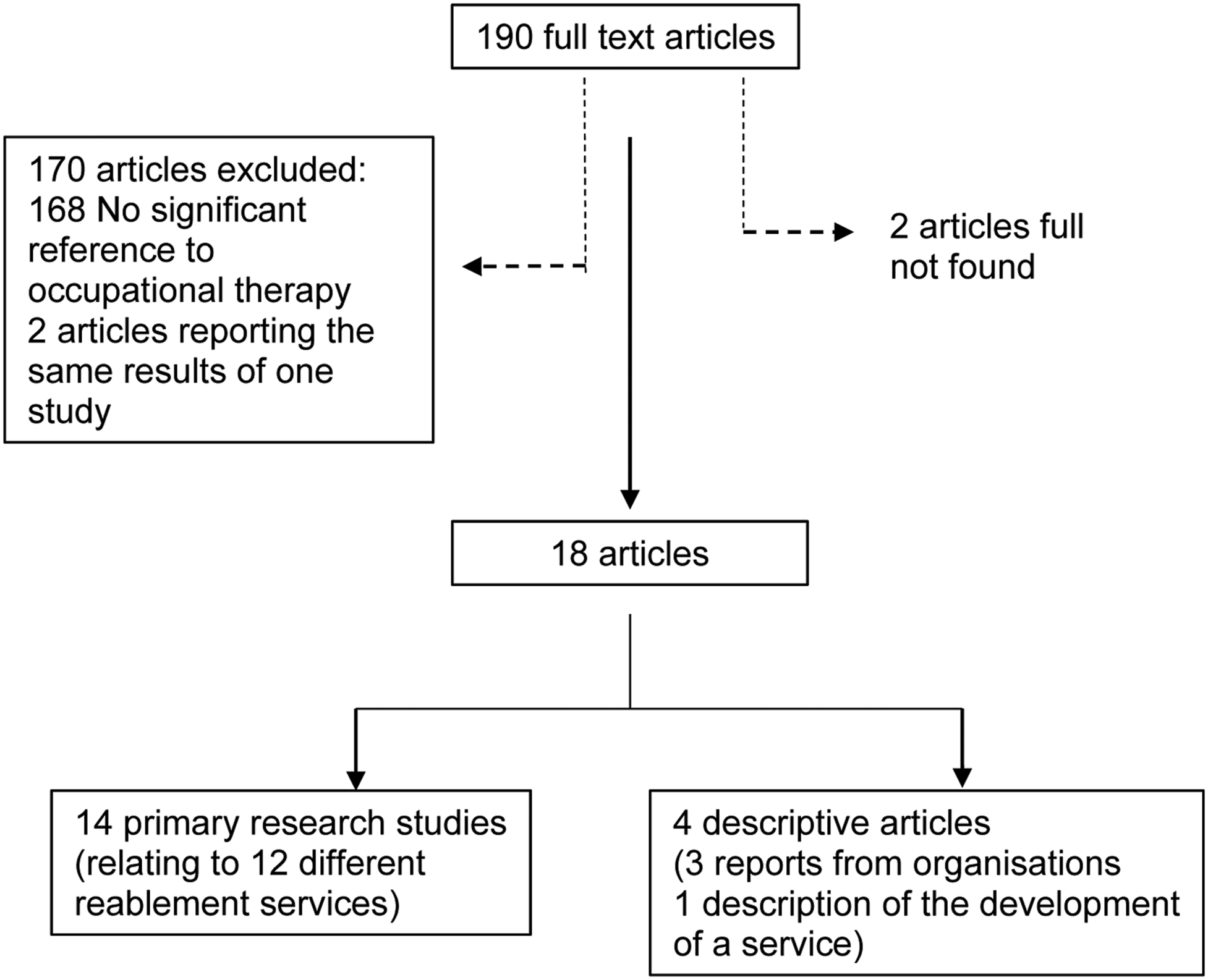
Eighteen articles included the role of occupational therapists in reablement services to any degree. In the third stage, the shortlisted literature was appraised focussing on relevance and rigour. Relevance is the decision on whether any elements of the study are relevant to identifying or developing theories. The assessment of rigour was concerned with the trustworthiness of the relevant aspect of the study. An evaluation form was created for each article including the aspect of relevance from the study and an appraisal of whether specific conclusions of the research related to the theory were supported by the results obtained.
During stage four, data from the literature was extracted into configurations of contexts, mechanisms and outcomes. The context triggers the mechanism. This in turn leads to a particular outcome. These configurations were developed in the final stage of synthesising the data into programme theories.
Programme theory 1 - The skills and knowledge of occupational therapists can be utilised in assessment, goal setting and the development of plans in a holistic way for reablement to support a person’s occupational engagement in all areas of daily life
The role of occupational therapists varies between different reablement services. Occupational therapists have been requested to work primarily with people with complex needs (McLeod and Mair, 2009; Rabiee et al., 2009). Occupational therapists complete assessments and set goals with people with the majority of goals limited to working with the person in their own home (Glendinning et al., 2010). Occupational therapists in reablement services support independence and provide advice and guidance to people using the reablement service in dressing techniques, food preparation, stress management, sensory and cognitive impairments, energy conservation, fatigue management and moving and handling (King et al., 2012; Social Care Institute For Excellence, 2011).
Programme theory 2 - The timely provision of equipment increases a person’s independence and supports carers in their caring role
The provision of equipment and adaptations is a primary role for occupational therapists working in social care settings that can increase a person’s independence, reduce falls and prevent accidents (Boniface et al., 2013). Provision of equipment by occupational therapists has aided the confidence and independence of people using the reablement service (Littlechild et al., 2010; McLeod and Mair, 2009). Timeliness of the provision of equipment has been considered as the primary factor for reablement services; rather than occupational therapists being members of the reablement team (Rabiee and Glendinning, 2011; Tessier et al., 2016). Conversely difficulties accessing occupational therapists results in delays in the provision of equipment, with the outcome of people remaining dependent on the reablement service (Rabiee et al., 2009).
Programme theory 3 - Occupational therapists’ contact with reablement support workers, including involvement in training, increases the skills and confidence of reablement support workers and assists them to work in a reabling way
Training for all members of the team have been identified as key components to an effective reablement service (National institute for Health and Care Excellence, 2017). Some reablement support workers have found working in a more reabling way challenging as a traditional ‘doing for’ approach is asserted as being easier and quicker for staff (Hjelle et al., 2016; Rabiee and Glendinning, 2011).
Training prepares reablement support workers for their role resulting in increased confidence and a consistent approach (McLeod and Mair, 2009; Social Care Institute For Excellence, 2011). Occupational therapists have skills essential for the training of reablement workers (College of Occupational Therapists, 2010; Rabiee and Glendinning, 2011).
Method
Details of case studies.
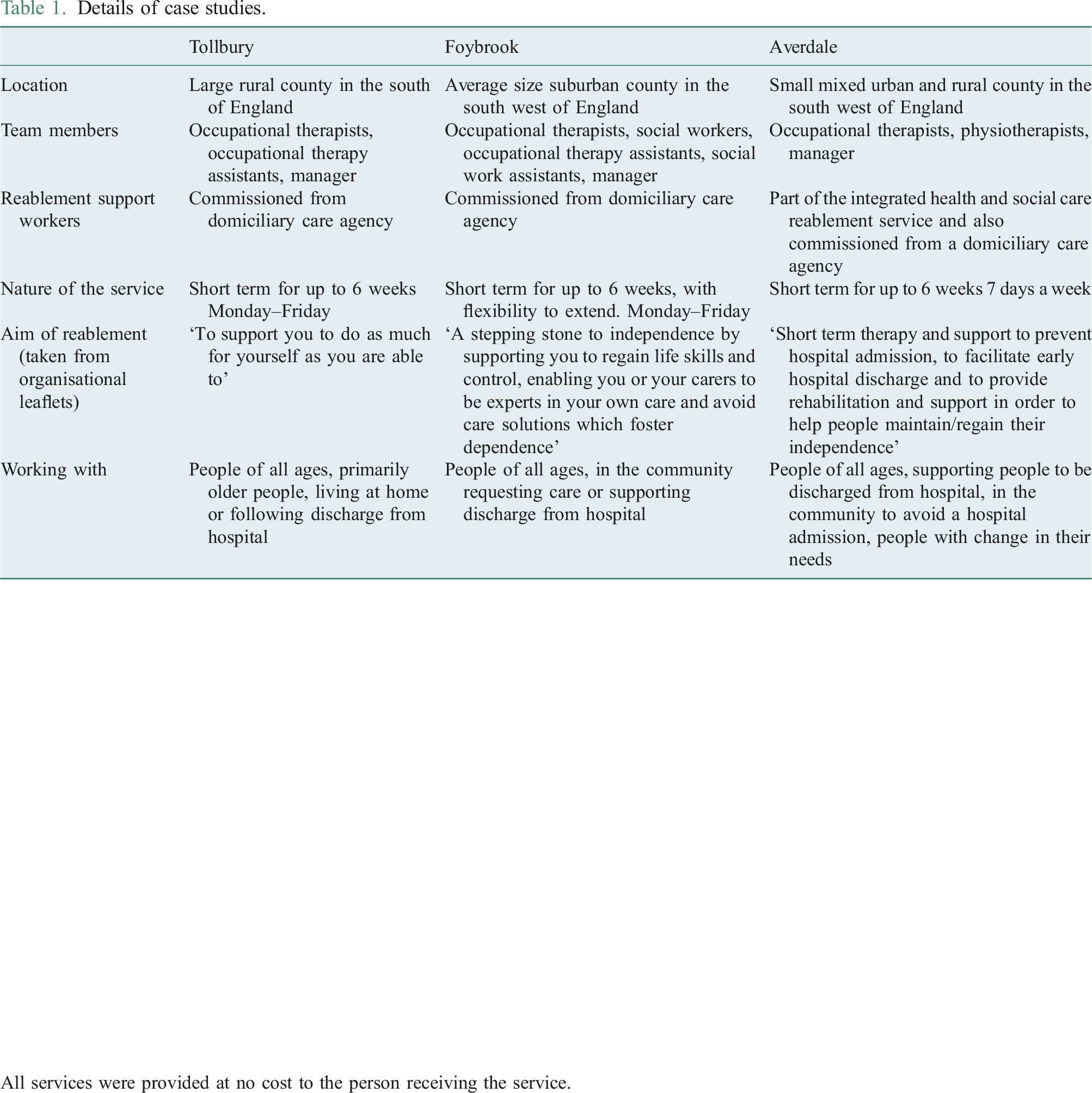
All services were provided at no cost to the person receiving the service.
Study participants.
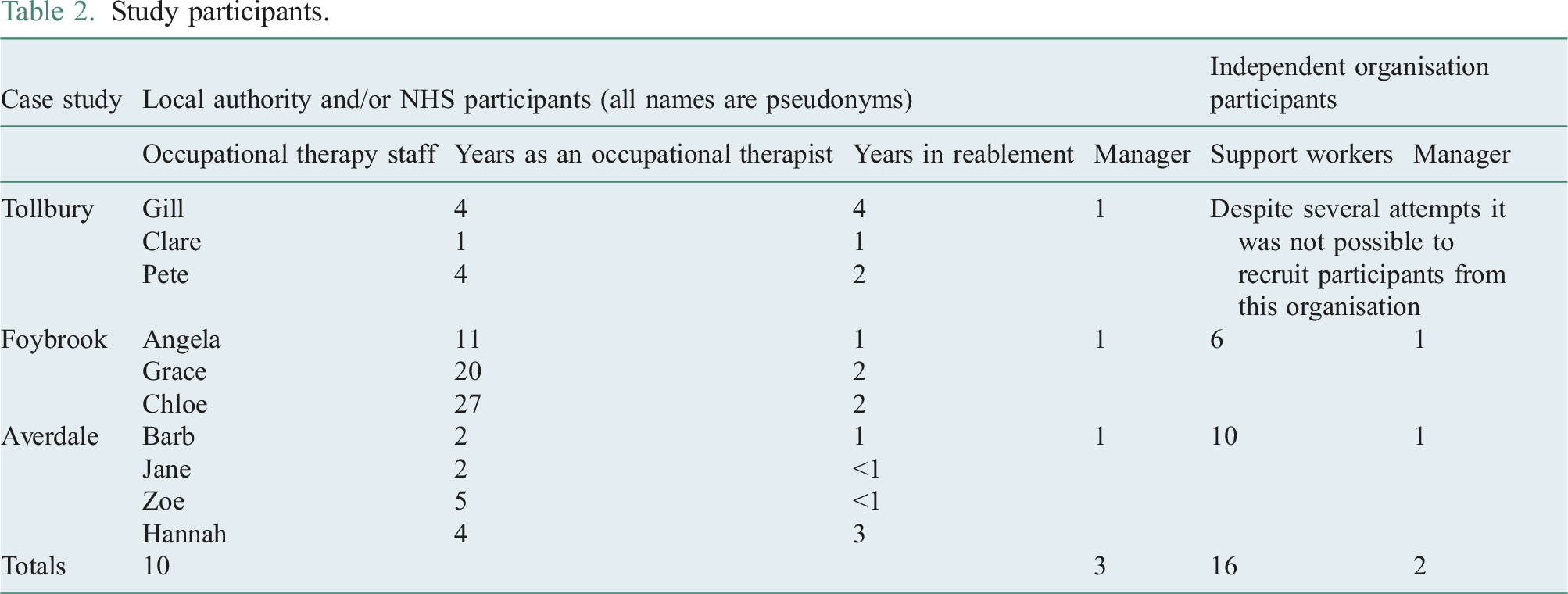
Occupational therapists were observed for a median average duration of 1½ days each, in office settings, a hospital and visits to 20 people being supported by reablement in their own home. The aim of this observation period was to gain an understanding of the reablement setting, the wider team and the occupational therapists’ role within the team. The author assumed a non-participatory approach observing each occupational therapist during all their activities. Notes were taken that related both to the programme theories identified and to potential new theories. Semi structured interviews were completed with occupational therapists and managers to discuss details observed, introduce topics to confirm or refute the theories identified and identify any additional theories on the occupational therapists’ role. Interview and focus group transcripts were sent to participants for checking prior to analysis, no changes were made by participants.
All data collection was undertaken by the author who kept a reflective diary for transparency to explore the impact of her role as an occupational therapist on the research. The researcher’s role was included on information leaflets.
Data analysis
Data were analysed using the strategy of explanation building to explain the how and why of the phenomenon under study (Yin, 2009). During analysis the author continuously reviewed whether initial thoughts during data analysis were based on the data or were influenced by her role as an occupational therapist. The data were analysed using a thematic analysis approach (Braun and Clarke, 2006). Themes from the data were identified as potential contexts (C), mechanisms (M) and outcomes (O). A spreadsheet was used to maintain configurations of the CMOs to compare the configurations against the programme theory in a deductive way. The data analysis revealed CMO configurations that identified new aspects of programme theory in an inductive way.
Ethics
The study was approved by the University Faculty Research Ethics Committee and the Social Care Research Ethics Committee. Each Local Authority also gave ethical approval under their Research Governance Framework. Written informed consent to participate was obtained from each participant including people using the service who were present during observations.
Findings
Each theory is presented as a configuration of contexts, mechanisms and outcomes as labelled in the key in Figure 2. Verbatim quotations use pseudonyms and identify the case study area of the participants. All quotes are from occupational therapists unless otherwise stated. Programme theory 1 – Holistic and Person-centred practice.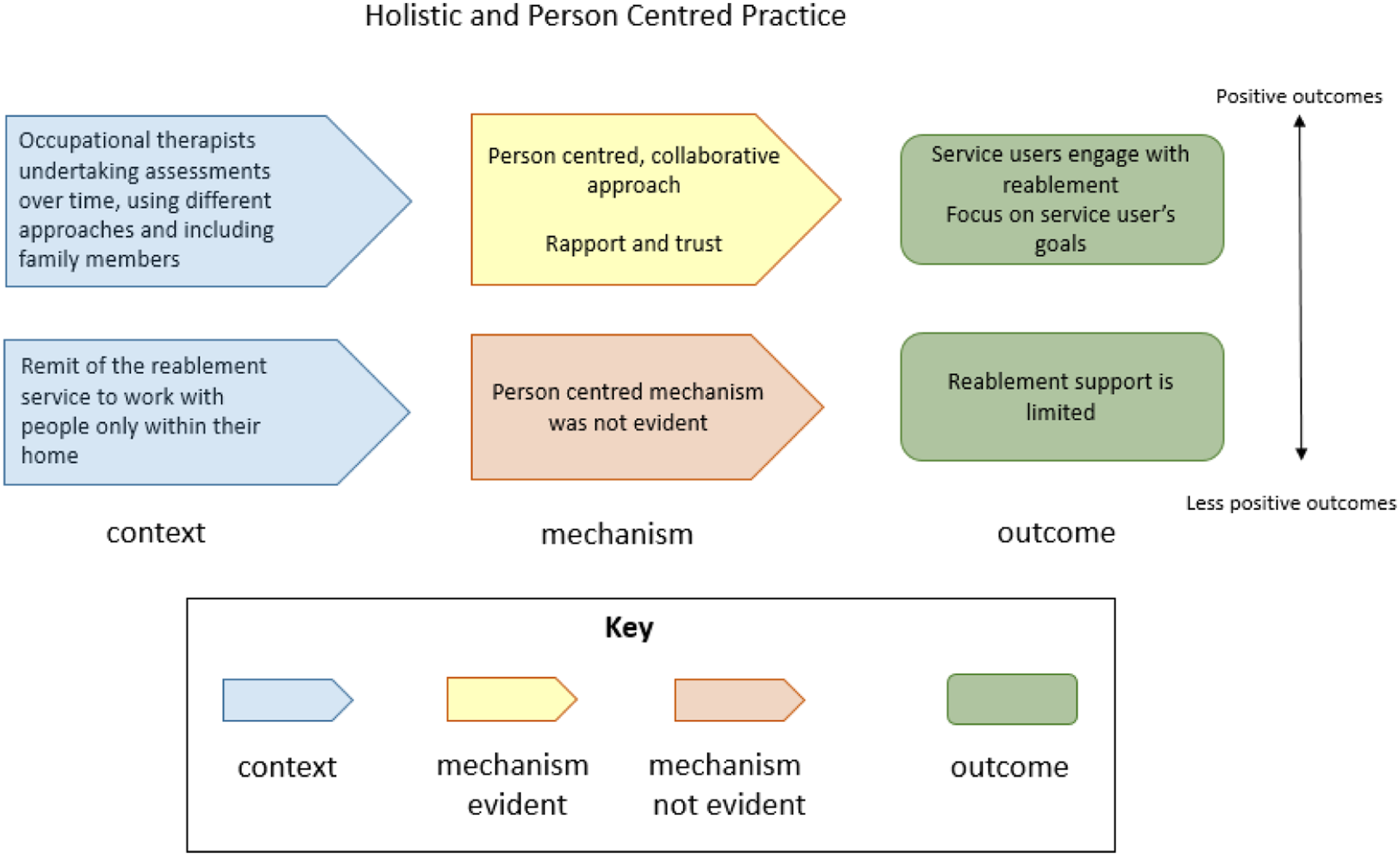
Programme theory 1 - Holistic and person-centred practice
Occupational therapists described their role as person-centred during their assessments and goal setting: ‘the way OTs1 see things is very different. We are very person-centred….we are looking at the individual’ (Clare, Tollbury). ‘ … not just looking at one particular task … but being able to look at it as a whole …. well placed to try and reintegrate someone into the community as opposed to just doing an assessment of function. Trying to enable them to access their lunch club or walking down to their garden... I think OTs are quite well placed to do that perhaps more than any other discipline’ (Zoe, Averdale).
During observed visits occupational therapists demonstrated a person-centred approach inviting people to share their story of what had changed for them to lead them to a referral to the reablement service. Open questions were asked concerning daily occupations and to ascertain what occupations the person needed or wanted to do.
Occupational therapists described assessment as a continual approach guided by the person rather than a one-off activity. Visiting people on a number of occasions enabled the development of rapport and trust and supported the assessment of needs, and development of goals based on conversation and observation.
There was a recognition that a person’s identified goals and the goals that occupational therapists identify as important, may be different: ‘keep asking the person what their priorities are…what they think is important is not what you think is important …it’s definitely our role to make sure that we’re listening to them and we’re not just imparting our thoughts on them and it might not be what they want to focus on’. (Jane, Averdale)
Occupational therapists identified organisational contexts that reduced their ability to be person-centred and work on all the goals a person identified. One occupational therapist described the service as only being able to work with people on ‘the absolute basics’ (Pete, Tollbury) of personal care, mobilising around the home and kitchen skills. This was confirmed in an interview with a reablement manager who said: ‘we can only fix the basics and then we need to let them move on’ (Emily, Manager, Averdale).
Each visit observed by the author involved either setting goals or reviewing goals. These goals were noted down during the visit, the majority of goals were related to personal care. Occupational therapists expressed views that they had both the skills and willingness to work with people on wider goals such as enabling someone to go shopping or accompanying people to clubs in the community to build confidence. They felt that they were constrained by the remit of the service and were only able to provide information to support the person.
Programme theory 2 - A tool box of interventions
Analysis of tasks and problem solving skills were seen as core skills of occupational therapists working in reablement settings and different from traditional models of home care. Occupational therapists used their clinical reasoning skills to analyse the situation: ‘Rather than just saying somebody’s having difficulty getting washed and dressed, actually…breaking that down to then work out “it’s because your standing tolerance is reduced”…It’s really taking that deeper analysis and I think as OTs we are able to really break that down into the …lowest denominator to then say “well actually now we know what the difficulty is, what are the options that we’ve got?”’ (Angela, Foybrook)
Occupational therapists described their training and experience working with people with different medical conditions and their life experience as their ‘knowledge bank’. They described using this knowledge bank alongside a ‘tool box’ of options to decide on the intervention that would support a person to meet their goals (Figure 3 Programme theory 2 – A toolbox of interventions.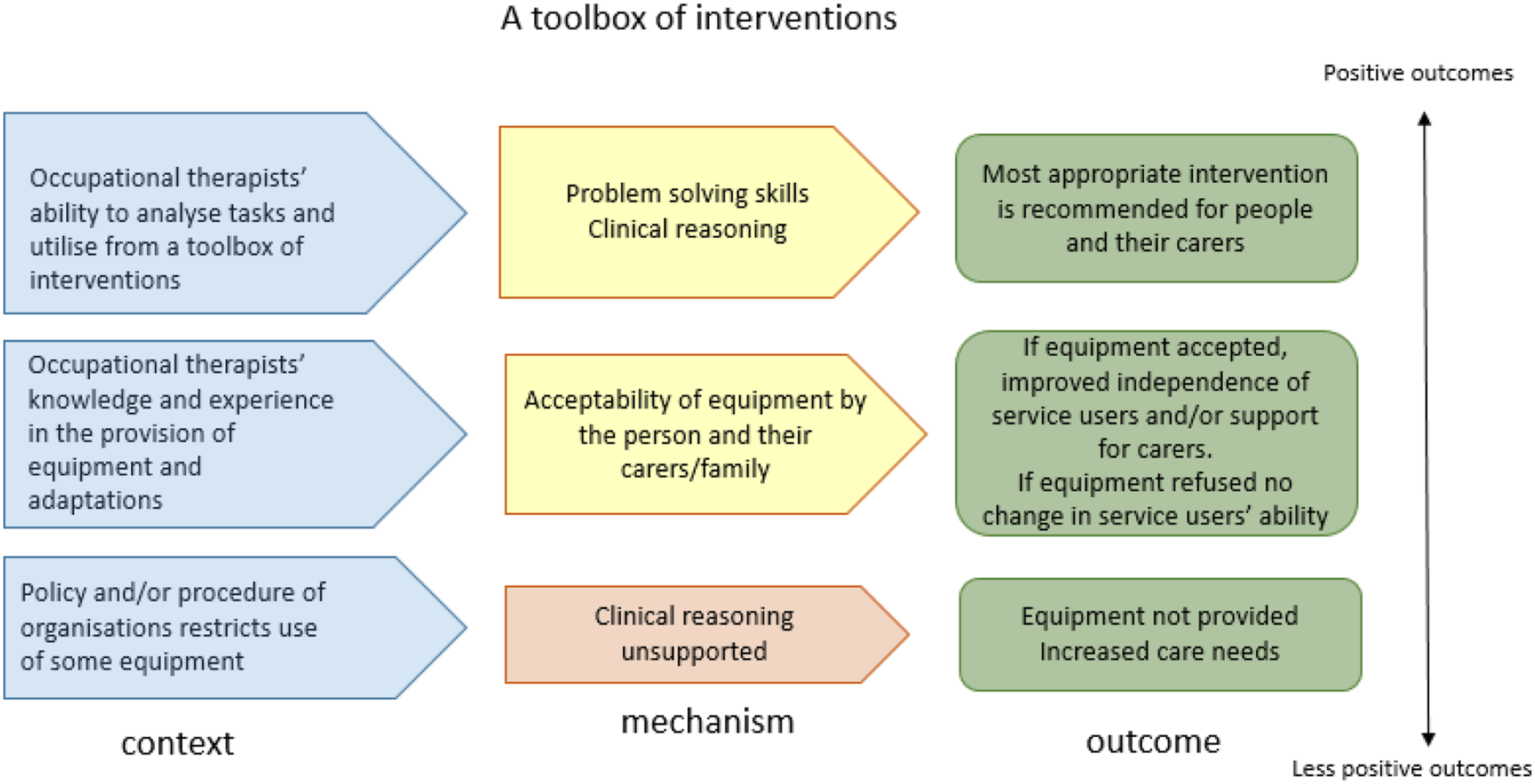
Occupational therapists in all case studies recognised the role of assessing for and providing equipment and adaptations. Both occupational therapists and reablement support workers affirmed the positive effect that equipment had on a person’s physical and emotional wellbeing and ability to carry out tasks. Reablement support workers reported that some people did not readily accept equipment due to embarrassment at having to use the equipment or because family members would not like the equipment. ‘I had someone once “my husband would hate that so I am not having it”, but the fact is the lady could not get off the toilet’ (Matt, reablement support worker, Averdale)
Advising that the provision of equipment was on loan to them at no cost supported acceptance of equipment with some considering the return of equipment as a marker of their improvement.
Occupational therapists had access to a different range of equipment and adaptations in each of the case studies. Small items of equipment were provided in Averdale as they were seen as cost effective: ‘… providing those small aids when you look at the cost of them having a morning visit… Actually it’s much more beneficial …. (Barb, Averdale)
However, obtaining specialist equipment that was outside of the standard stock involved a long process of preparing a case to apply for funding for the equipment, which led to a delay in the reablement process.
Programme theory 3 - Occupational therapists as members of the team
Occupational therapists in each of the case studies were observed to work closely with reablement support workers. They were described by Hannah (Averdale) as ‘our extra eyes and ears.
Occupational therapists were involved in training for reablement support workers that included dressing techniques, preservation of stamina and pacing techniques. In Foybrook, occupational therapists trained reablement support workers during the development of the service to develop skills in enabling people rather than ‘doing for’ people: ‘My biggest transition from doing core care to reablement was learning to stand back a little bit. Because when you are in care you are very hands on and it is all about doing’. (Suzy, reablement support worker, Averdale) Programme theory – Occupational therapists as members of the team.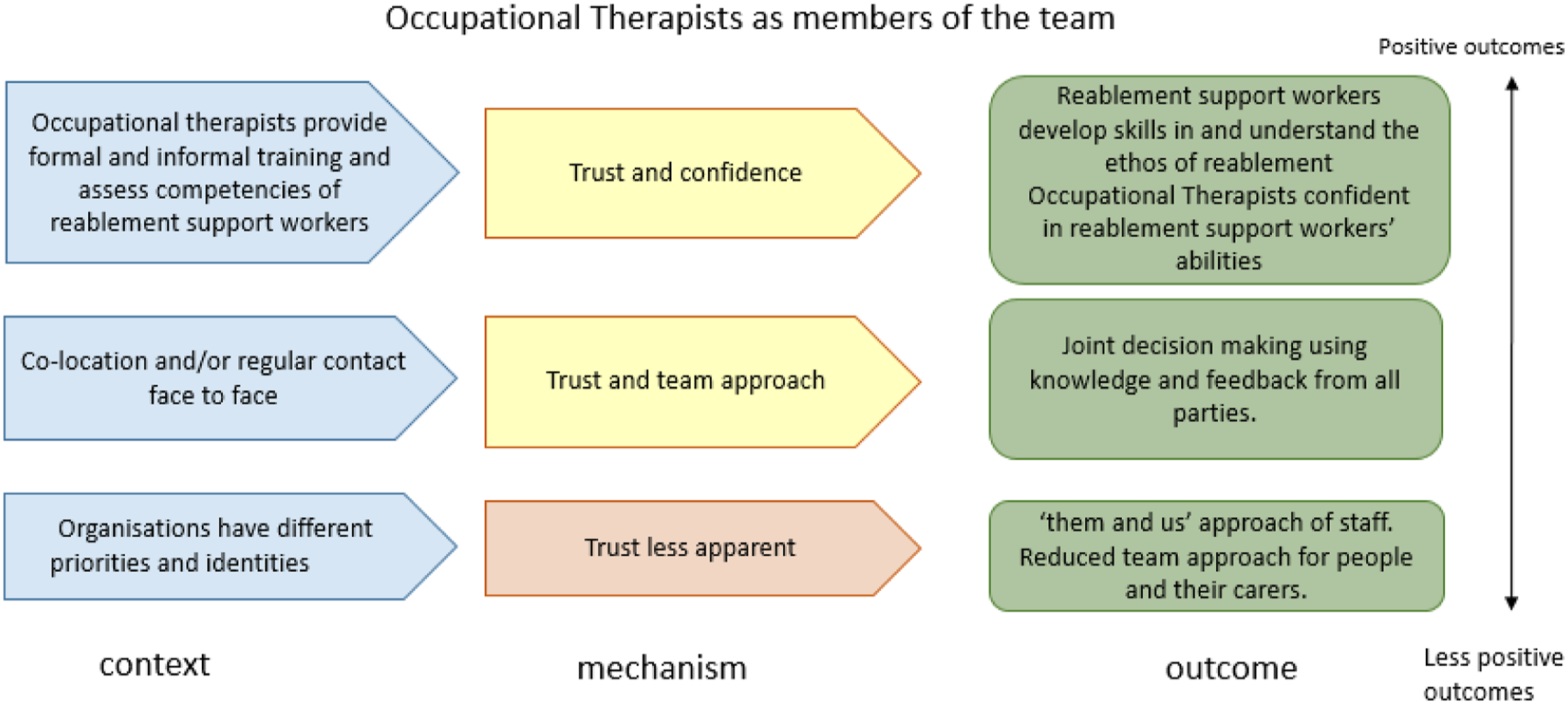
As well as formal training, regular communication supported the mechanism of trust and a team approach between the two organisations that constituted the reablement service. Co-location was identified as being key to understanding and respect between different members of the team. During observations in the office environment in Tollbury, the manager of the independent organisation visited the occupational therapist several times. Visits were typically less than 5 minutes and included discussion about a person and actions were agreed. Reablement support workers also regularly came into the office to feed back about people they were working with and occupational therapists said that this supported good relationships between them.
In Foybrook and Averdale timeliness of response from occupational therapists was highlighted. Reablement support workers reported that delay significantly affected their ability to reable a person. ‘We are back to square one because we have to go right through the whole process of trying to reable that person’. (Joy, Reablement support worker, Foybrook)
Limited contact and poor communication between organisations did not support a team approach. Occupational therapists in one case study used the term ‘them and us’, explaining the concept of the two different organisations having different agendas. Occupational therapists perceived that the focus of the independent organisation was to finish reablement with one person to meet the target within their contract of how many people they support.
In Tollbury and Averdale weekly meetings were held to discuss all the people the team were working with. During observations of three of these meetings in Averdale, there was sense of a team approach. The meetings served to review a person’s progress and decide whether additional support, less support or equipment was required. While each person was allocated a lead professional, team members had an awareness of all the people being supported by reablement through these regular meetings.
Programme theory 4 – Shared purpose
The additional programme theory identified in the case study phase builds on the team approach to include all stakeholders having a shared purpose of reablement (Figure 5). Programme theory – Shared purpose.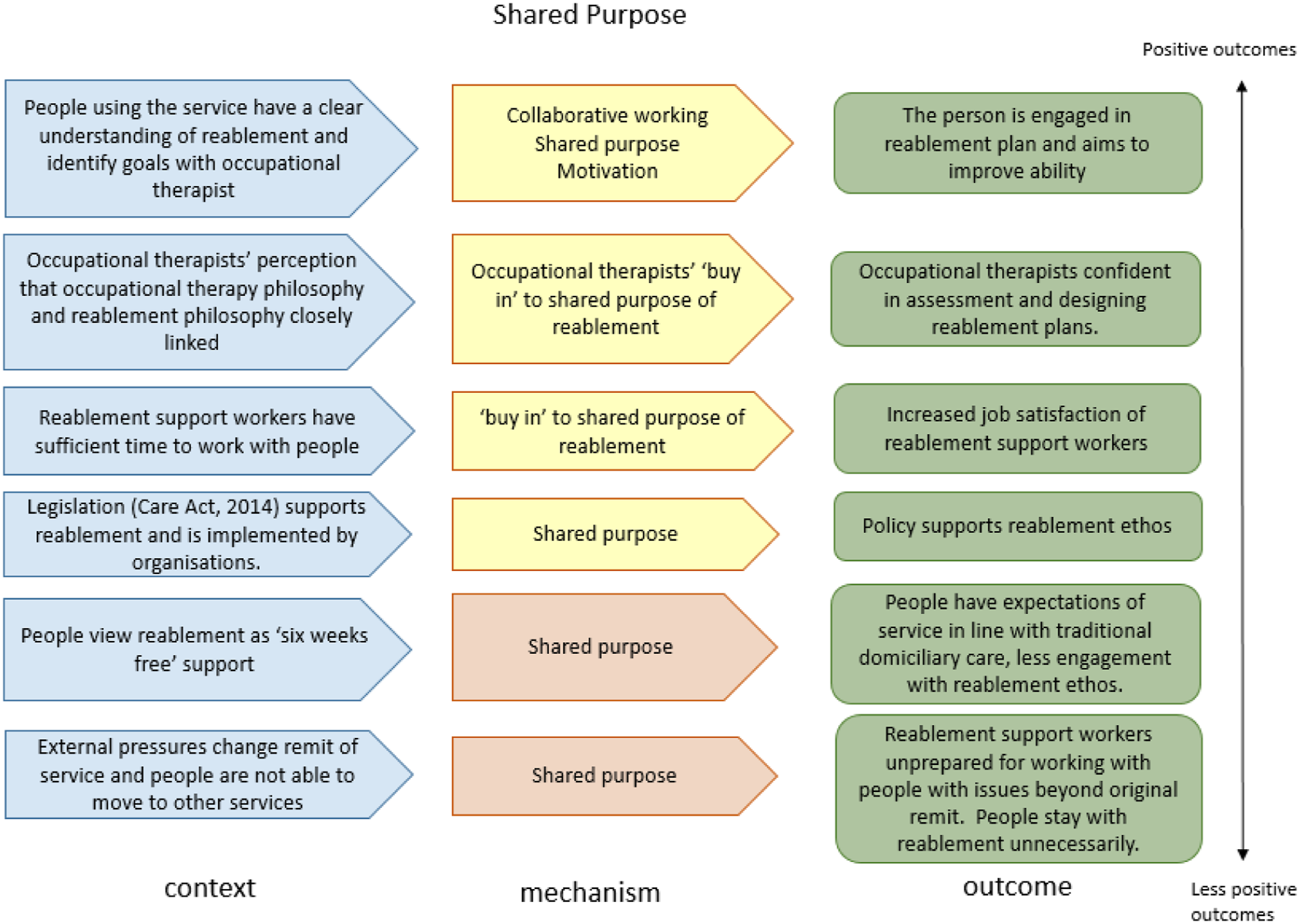
Reablement services in all case studies were designed as short term support for up to 6 weeks, at no cost to the person receiving the support. Some people did not share the purpose of reablement, during an observed visit one person said ‘well I never asked for reablement, I just want care’. Similarly, Gill (Tollbury) recalled attempting to end reablement support as the person was independent in her daily occupations. Family members did not accept this stating that they were ‘promised 6 weeks free care’.
People who understood the purpose of reablement were motivated to work with occupational therapists to set goals. ‘She was really motivated to be independent so goal setting was really easy with her because she knew exactly what she wanted’ (Zoe, Averdale)
All occupational therapists in the study commented that they were committed to the ethos of reablement perceiving that reablement and occupational therapy are closely linked: ‘I think that OT is the core profession for reablement… we have those skills to look at the whole picture, and to look at their environment, and to make small changes which make a big difference on their package of care and their ability to manage things independently (Barb, Averdale)
Assessing function, teaching techniques and adapting the environment were all elements of the reablement service, asserted as within the domain of occupational therapy and a shift from the traditional approach of occupational therapy in social care of providing equipment to compensate for difficulties.
All independent organisations in the case studies recruited reablement support workers who had previous experience in caring. Reablement support workers advised that they were used to working to a tight timescale, describing working in traditional care as ‘tick the boxes and run.’ The reablement support workers all appreciated having adequate time to spend with people and highlighted that supporting people to do more for themselves was very rewarding.
Having a shared purpose to reablement was important at the level of the organisations involved in the service. External pressures affected this approach. The context of pressure to discharge people from hospital was highlighted as a particular concern: ‘I think the hospital social workers are so under pressure to get people out of those beds. [Name of reablement service] is just another service that might pick it up’. (Clare, Tollbury)
In all of the case studies the reduced capacity of mainstream domiciliary care to support people with longer term needs was the main context that led to people being supported by reablement rather than another organisation. In one area, this led to reablement supporting people with a higher level of need and working with people for longer than 6 weeks while alternative support was found. This further blocked other people from utilising reablement. Reablement support workers expressed concern that they were working with people who they were not sufficiently trained to support.
Discussion
A conceptual framework was developed from all the findings of this study (Figure 6). Shared purpose is the title of the first phase of the conceptual framework. It has been highlighted as an essential element of team working and managing change in the NHS (Adair, 1983). Conceptual framework of occupational therapists in reablement services.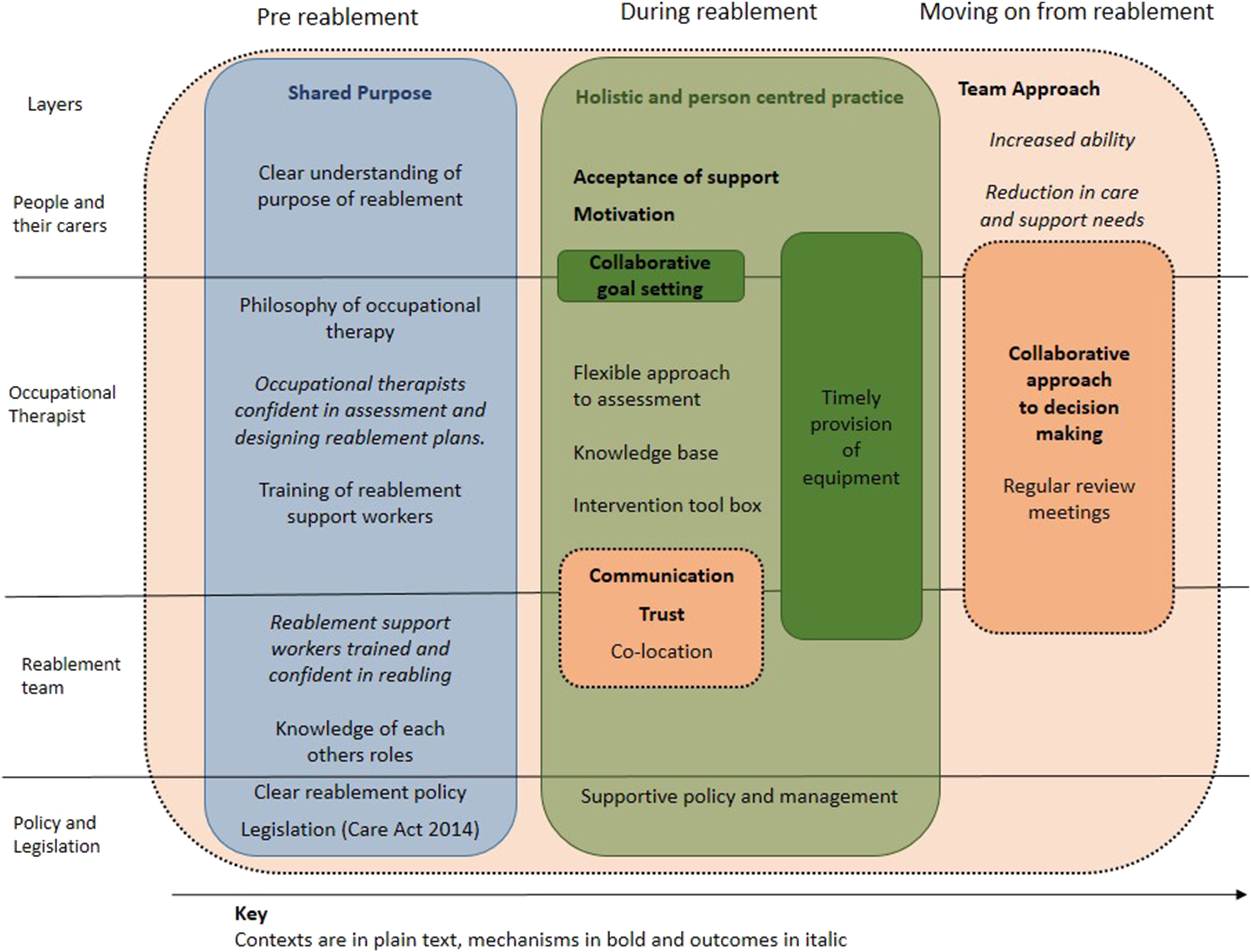
Shared purpose is important in each contextual layer. Occupational therapists in this study aligned the ethos of reablement with the philosophy of occupational therapy to assess, set goals and support people to be independent and engage in occupations important to them. Ensuring reablement intervention is focused on the goals of the person has been recognised as important in other studies (Birkeland et al., 2017; Hjelle et al., 2016) and identified as a core principle of reablement (National institute for Health and Care Excellence, 2017).
Reablement goals
The occupational therapists in this study worked with people living in their own homes, with a variety of physical and/or cognitive difficulties, interests, values and roles. As such, one might expect a variety of goals based on what was important to the person. Goals were limited by the remit of the reablement service to working on goals within the home rather that supporting people in the community if that was important to them. This finding is congruent with other reablement studies that found that goals for reablement were largely confined to occupations within a person’s home (Glendinning et al., 2010; Whitehead et al., 2016).
Current legislation in the four nations of the UK all have a focus on the wellbeing of people in the community including access to recreation and other settings outside the home. Aspinal et al. (2016) argue that a reablement service with a goal of reducing support to people may lead to increased experiences of isolation and loneliness. Designing reablement services to be able to support people with all occupations important to them is a challenge for Local Authorities working within finite resources. Person-centred reablement services supporting people to meet their goals in social and leisure pursuits may have a positive impact on loneliness. The topic of loneliness warrants further investigation within reablement services.
Toolbox of interventions
The interventions described by occupational therapists in their reablement toolbox in this study: providing advice, demonstrating techniques, re-establishing routines and provision of equipment and environmental adaptations to accommodate a difficulty have been identified as within the domain of occupational therapy in reablement settings in other studies (Lewin et al., 2008; Zingmark et al., 2019). Roberts (1996) studied the reasoning of occupational therapists and identified two reasoning strategies. In this study, the experience and knowledge of occupational therapists was key to selecting the most appropriate intervention from the toolbox. Occupational therapists in this study demonstrated the reasoning strategy of pattern recognition in that their decisions were guided by their previous experiences.
In this study, reablement support workers identified that the opinion of families affected whether people accepted equipment. This is in contrast to others studies that have identified family carers as benefitting from the provision of equipment (Dibsdall and Rugg, 2008; Littlechild et al., 2010) and warrants further research.
Reablement support workers
Training, regular contact and co-location were identified as contexts that supported members of the reablement team to move away from ‘doing for’ people, understand each other’s roles and build trust that have been confirmed as essential to successful reablement in other studies (Rooijackers et al., 2021; Tessier et al., 2016). In this study, higher levels of job satisfaction by reablement support workers, compared to working in a traditional domiciliary carer role was attributed to having time to work with people in a reabling way. This finding is unsurprising as traditional domiciliary care has been described as commissioned on a ‘time and task’ basis that provides insufficient time to build a relationship with the person (Lewis and West, 2014).
Legislation and policy
At the policy and legislation layer reablement services provided by health and social care organisations’ services are largely dictated by Acts of Law and guidance. Reablement policy needs to support the shared purpose of reablement as a short term service promoting independence, and the broadness of the goals and provision of equipment as previously described. External pressures, for example, to discharge people from hospital, were identified as factors that pushed the boundaries of reablement, and the shared purpose. During the duration of the study domiciliary care to support people with ongoing needs was frequently not available due to local and national shortages of domiciliary care. Reablement was sometimes referred to as a ‘holding area’ for people waiting for the availability of domiciliary care, a practice described as a ‘coping policy’ in a climate of increased demand (Wolstenholme et al., 2007).
A pressure to discharge people from hospital, in this study, led to people being referred to reablement with higher levels of need. Reablement support workers expressed concern about working with people that they did not have the skills to support that has been identified in other reablement services (Harris, 2010). Occupational therapists did not mirror these concerns. This could be attributed to their higher level of background knowledge, experience and clinical reasoning skills. In times of high demand for services, the professional training of staff has been identified as a resilience tool by health and social care professionals (McGray et al., 2016). This may explain the absence of comments by occupational therapists in this study as they may have been using their underpinning knowledge and experience when working with people with increased difficulties.
Conclusion
Shared purpose was identified as a mechanism that was important across all contextual layers to ensure that all stakeholders were committed to a reablement ethos. Occupational therapists’ education, experience and skills were identified as contexts that supported occupational therapists to work collaboratively with people to identify goals and choose from a toolbox of interventions to support people to engage in occupations important to them within the contextual limitations of the service.
The shared purpose of reablement was flexed due to external pressures to discharge people from hospital. This study suggests that occupational therapists may be resilient to this flexing and organisations should consider any additional training required to support reablement support workers.
The qualitative nature of this research provided rich data to answer the study’s aims. The case studies were limited to the south of England and readers should assess whether the contexts are similar to their own setting to assess the transferability of the findings. The research was undertaken by a sole researcher, use of a reflective diary ensured themes were grounded in the data. Despite this, other researchers may have identified different theories from the literature. A limitation of this study is the omission of people using the reablement service as direct participants. While some of the findings were evidenced during observation of home visits, including the views of people using reablement services would have provided essential data to confirm or refute the theories explored.
Key Findings
Commitment to a shared purpose builds trust between reablement team members. Occupational therapists use a person-centred approach, selecting from their toolbox of interventions to meet the person’s goals.
What the study added
Exploration of the role of occupational therapists in reablement services identified a person-centred approach with people and the importance of regular communication to support a shared purpose of all members of the team.
Footnotes
Acknowledgements
I would like to acknowledge my PhD supervisors Dr Ailie Turton and Dr Stuart McClean for their support during my study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Patient and public involvement data
During the development, progress, and reporting of the submitted research, Patient and Public Involvement in the research was: Not included at any stage of the research.
Ethical approval
2014 Social Care Research Ethics Committee 13/IEC08/0042.
Note
The term OT as a shortened form of occupational therapy or occupational therapist is used only when directly quoted by participants.