
Abstract
Introduction
Occupational therapists work with clients with impaired communication to re-engage in valued occupations. This systematic review seeks to answer the question: What are effective interventions within the scope of occupational therapy practice to address participation for adults with aphasia?
Method
A systematic review of the literature was completed using PubMed, PsychInfo, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Embase, Cochrane Database of Systematic Reviews, and OT Seeker databases. Intervention studies within the scope of occupational therapy practice with a participation outcome, and published in peer reviewed journals from 2000 to 2019, were included. The quality of each study was assessed using the Mixed Methods Appraisal Tool.
Findings
Thirteen articles fit the inclusion criteria. Categories of interventions that emerged from the data include community-based groups, individually tailored programs, adaptation/presentation of materials, interprofessional interventions, and psychoeducation.
Conclusion
There is evidence to support the use of interventions within the scope of occupational therapy practice to increase participation for people with aphasia. Specifically, the use of community-based groups and adaptation of materials are effective to facilitate participation. Most of the studies were pre-post one group design; however, they demonstrated positive results for participation outcomes. More research is needed on people with aphasia that focuses on participation in meaningful occupations.
Keywords
Introduction
Aphasia is a communication disorder that impairs an individual’s ability to express and interpret communication due to an inability to process language (National Aphasia Association, 2020). The ability to comprehend language and communicate effectively is vital to participation in many occupations including reading recipes or measurements in order to cook, interpreting public transportation schedules or maps, working on a computer, communicating virtually via phone, video chat or email, and engaging socially in person. People with aphasia may have significant difficulties engaging in these and many other valued activities.
Most commonly occurring post-stroke, aphasia affects millions of individuals worldwide. Approximately 30% of people with stroke have aphasia (Flowers et al., 2016). As compared to people post-stroke without aphasia, people post-stroke with aphasia have greater disability, longer hospital stays, higher hospital costs, and increased use of rehabilitation services (Flowers et al., 2016). Quality of life and participation outcomes for adults post-stroke with aphasia are often worse than for people post-stroke without aphasia (Hilari, 2011; Wray and Clarke, 2017).
In addition to aphasia, some people may have sequelae such as motor or cognitive impairments that persist months after stroke or traumatic brain injury and may further exacerbate struggles to participate in everyday life activities. A recent synthesis of research related to the perspectives of adults with aphasia recognized the multiple barriers to participation that exist for people with aphasia including other impacts of stroke, the inability to navigate the environment, and avoidance of social situations that would require speaking (Manning et al., 2019). Despite these barriers, people with aphasia want to make contributions to society (Manning et al., 2019).
Management of aphasia varies across the rehabilitation continuum. Early in the rehabilitation process, people with aphasia are likely to receive referrals for occupational therapy, physical therapy, and speech-language pathology. Once clients transition from an acute rehabilitation setting to the community or long-term care, their communication challenges may transition from an acute to a chronic issue. Best practices to improve communication for people with chronic aphasia (greater than 6 months post-stroke) include intensive speech and language therapy (Breitenstein et al., 2017). Clients with aphasia, however, often have goals beyond increasing their speech and language skills. They benefit from working toward increased participation in daily activities through access to a range of services over the course of their aphasia trajectory including years post-stroke (Manning et al., 2019).
The Occupational Therapy Practice Framework (OTPF) (American Occupational Therapy Association, 2020), the guiding document that delineates the domain and process of OT in the United States of America, describes outcomes of OT practice as those that focus on increasing occupational performance including areas of instrumental activities of daily living (IADL), leisure, and social participation. Interventions within the scope of OT practice include, but are not limited to, occupation and activity-based interventions, assistive technology and environmental modifications, and education and training (American Occupational Therapy Association, 2020). It is well established that occupational therapy interventions are effective to increase participation for people post-stroke (Nilsen and Wolf, 2015). We suggest that occupational therapy is uniquely suited to assist clients with aphasia to re-engage in valued occupations impacted by their communication impairment and possible additional motor or cognitive impairment. Understandably, most of the research around intervention effectiveness for people with aphasia focuses on interventions within the scope of speech and language therapy (e.g., Brady et al., 2016) as increasing communication and language skills is a clear and prioritized goal. Increasingly, speech-language pathologists (SLPs) are focusing on participation outcomes as evidenced by their embrace of the Life Participation Approach to Aphasia (Chapey et al., 2000). Several recent systematic reviews which were completed by SLPs look at aspects of participation for adults with aphasia: social participation and working aged adults with aphasia (Pike et al., 2017), the efficacy of aphasia group interventions (Lanyon et al., 2013), and living successfully with aphasia (Manning et al., 2019). However, the outcomes for these reviews were focused on linguistic skills (Lanyon et al., 2013), or qualitative or descriptive experiences of people with aphasia (Manning et al., 2019; Pike et al., 2017). With their professional focus on supporting individuals to increase their participation in meaningful activities, occupational therapy practitioners clearly have a role in rehabilitation with adults with aphasia. However, until now there has not been a systematic review published regarding effective interventions within the scope of occupational therapy practice addressing participation outcomes for this population. This review seeks to answer the question: What are effective interventions within the scope of occupational therapy practice to address participation for adults with aphasia?
Method
Literature search
In order to identify effective interventions within the scope of occupational therapy to address participation outcomes for adults with aphasia, we conducted this review using recommendations from the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (PRISMA; Moher et al., 2009). Search terms were determined based on the authors’ experience, the literature, and consultation with speech-language pathology colleagues. The terms were further elucidated with the assistance of a reference librarian at the first authors’ home institution (see Appendix 1). The databases searched were PubMed, PsychInfo, CINAHL, Embase, Cochrane Database of Systematic Reviews/Cochrane Library, and OT Seeker.
Inclusion and exclusion criteria
The review was limited to articles in English, published in peer reviewed journals from 2000 to 2019. This timeframe was chosen to ensure a wide scope of literature that is current enough to be pertinent considering rapid advancements in technology and health care over the past 20 years. Studies of adults (18 years old and older) with any acquired communication disorder, including disorders resulting from stroke, traumatic brain injury, or Parkinson’s disease, for example, were included. Although the original search focused on identifying interventions for participation outcomes for adults with any acquired communication impairment, all articles that fit the inclusion criteria reported on studies completed with adults with aphasia. Studies on other populations with acquired language disorder, such as people with dysarthria or Parkinson’s disease, focused on interventions or measured outcomes that were not within the scope of OT practice, such as speech intelligibility. Therefore, our final review focuses on intervention effectiveness for people with aphasia. Studies could include participants in the acute or chronic stage of recovery and living in either a facility or the community, with any comorbidities. Only studies that reported on occupation and activity-based interventions, assistive technology and environmental modifications, or education and training with an outcome to increase participation in occupations (rather than solely to remediate language impairments) were included. We used occupation categories from the OTPF to determine studies that included outcomes within the scope of OT practice. Peer reviewed Level I (systematic reviews, meta-analyses, randomized control trials), Level II (two group, non-randomized), and Level III (one group, non-randomized) studies were included (Sackett, 1989).
Level IV (descriptive studies such as single-subject design and case series) or Level V (case reports and expert opinion) studies were excluded from this systematic review as were studies where the intervention was outside the scope of occupational therapy (e.g., constraint induced language therapy) or where the outcome measures focused solely on increasing speech (e.g., increased number of verbs spoken). We also excluded studies that focused on social communication, for example, literature that looked at adults with autism or traumatic brain injury who struggled to interpret social cues. Finally, presentations, conference proceedings, dissertations, and non-peer reviewed literature were not included in the review.
Review process
Two authors reviewed each title and abstract to determine relevance. Articles were rejected if it was clear by the title and/or abstract that the article would not be within the scope of the review inclusion criteria and if both authors agreed (via blind review) on exclusion. If there was any question regarding relevance, the article was included for full text review. During full text review, two authors independently determined if the article was appropriate to include in the review. If disagreement occurred, the third author reviewed the full study and the three authors discussed the study to determine if it met the inclusion criteria. Once articles for inclusion were determined, one author completed the evidence table and a second author reviewed and added to the table, as appropriate.
Study Appraisal
The quality of each study was assessed using the Mixed Methods Appraisal Tool (MMAT) Version 2018 (Hong et al., 2018). Two reviewers independently reviewed each study for quality based on the methodological quality criteria described in the MMAT.
Findings
A total of 2828 titles and/or abstracts were retrieved from the electronic search with an additional seven articles considered based on a review of reference lists. After this initial screen, 147 articles were retrieved for full text review. In total, 13 articles fit the inclusion criteria and were included in this review (see Figure 1). The single randomized control study (RCT) met all the MMAT quality criteria (Thomas et al., 2013). Separate from the one RCT, two studies provided Level II evidence (two groups, non-randomized; Vickers, 2010; Worrall and Yiu, 2010) while the remaining 10 articles provided Level III evidence (one group design). All studies provided a clear research question, collected data that addressed the research question, used outcome measures appropriate to the intervention, provided complete outcome data, and administered the intervention as intended. There were some concerns, however, related to the quality of a few of the studies. Specifically, four studies had no stated inclusion criteria (Brennan et al., 2005; Cherney et al., 2011; Egan et al., 2004; Wilson and Read, 2016) leading one to question how representative the sample was of the target population. Also, potential confounding factors were not addressed in three studies (Cherney et al., 2011; Egan et al., 2004; Vickers, 2010). Worth noting, 11 of the 13 studies in the final review specifically excluded people with dementia or cognitive impairment. PRISMA flowchart of articles identified. Note. *Some studies excluded for multiple reasons; Figure format from “Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement,” by D. Moher, A. Liberati, J. Tetzlaff, and D. G. Altman; The PRISMA Group, 2009, PLoS Medicine, 6(7), e1000097. https://doi.org/10.1371/journal.pmed.1000097.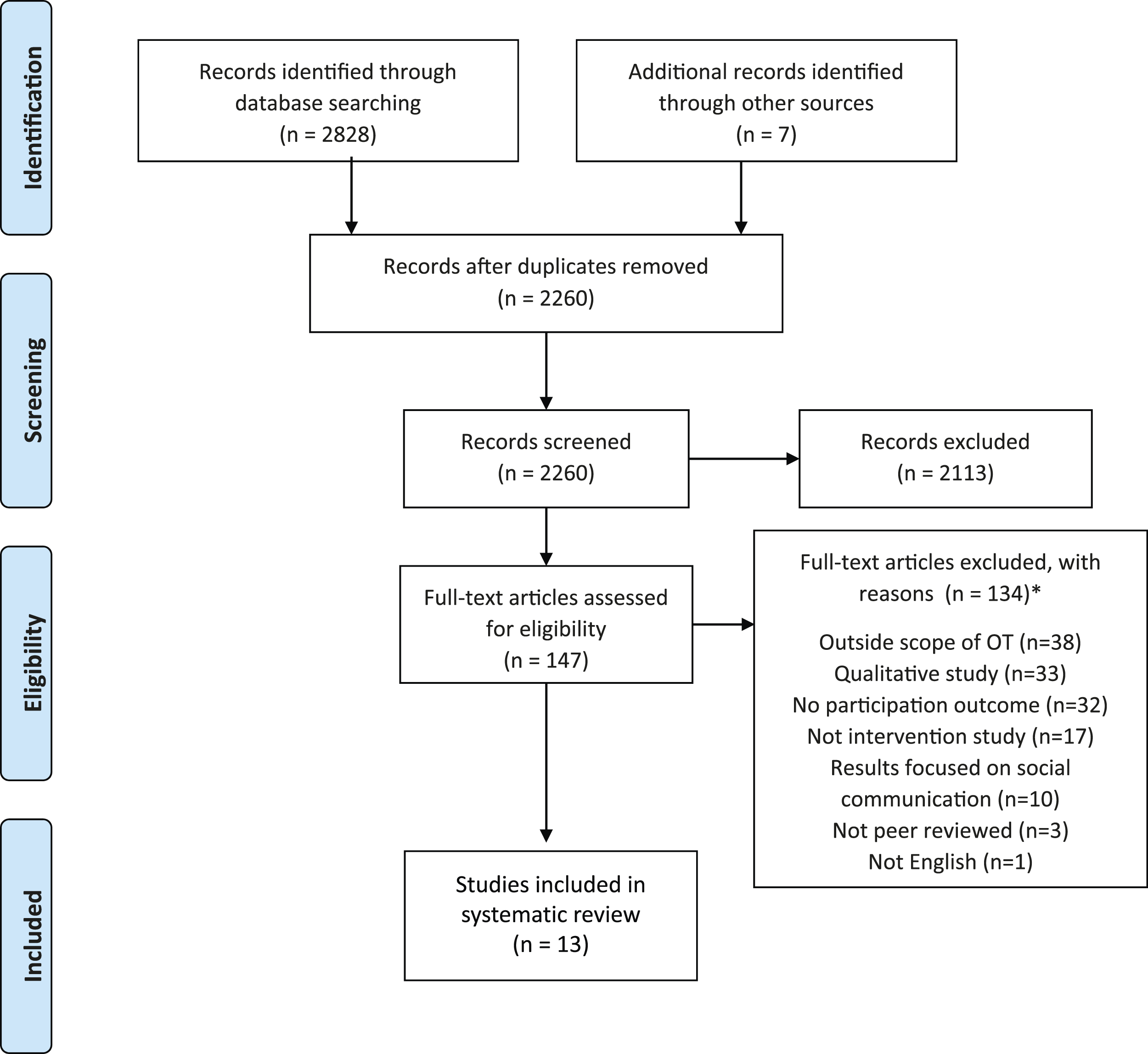
Study characteristic of the included papers.
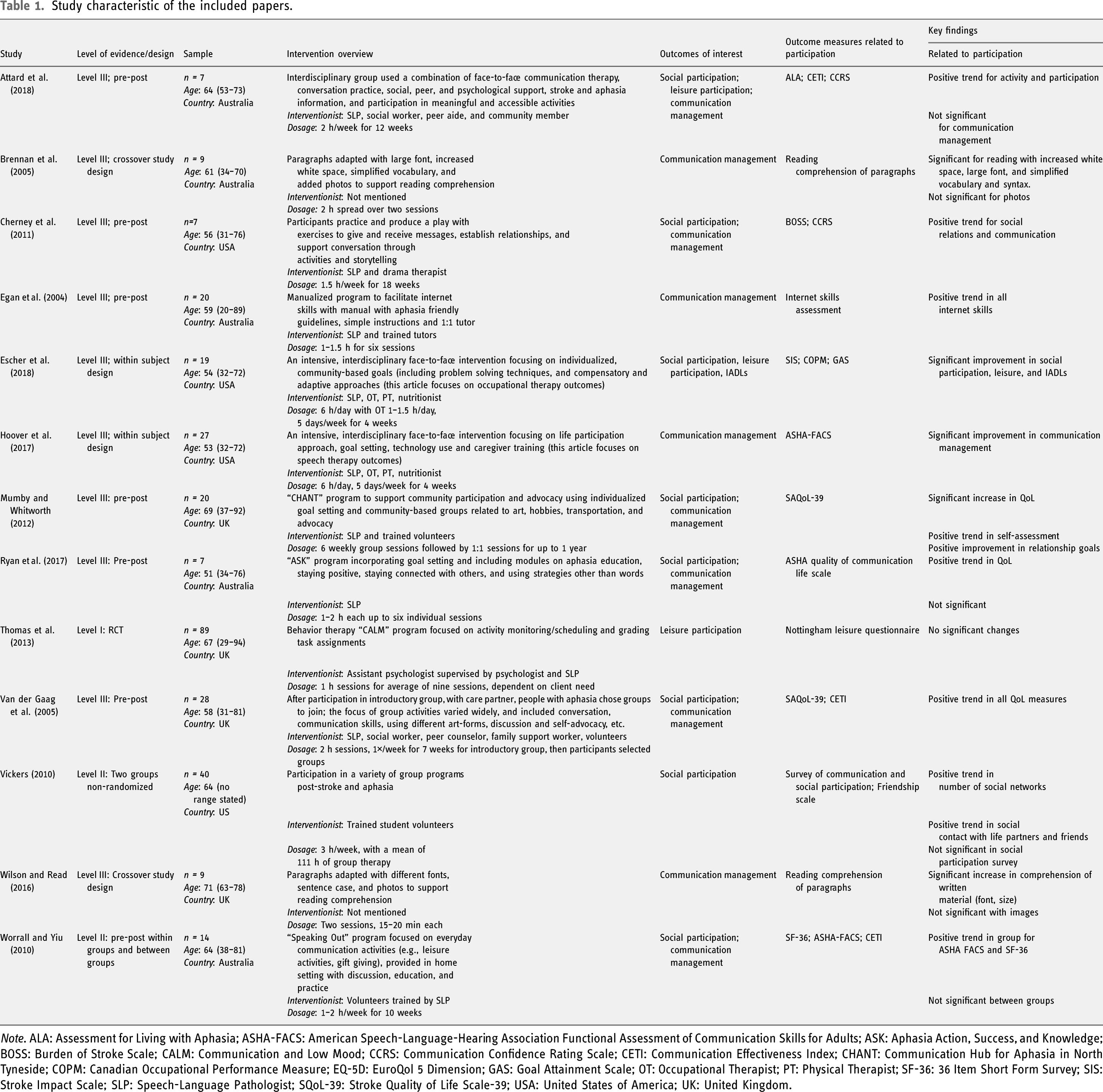
Note. ALA: Assessment for Living with Aphasia; ASHA-FACS: American Speech-Language-Hearing Association Functional Assessment of Communication Skills for Adults; ASK: Aphasia Action, Success, and Knowledge; BOSS: Burden of Stroke Scale; CALM: Communication and Low Mood; CCRS: Communication Confidence Rating Scale; CETI: Communication Effectiveness Index; CHANT: Communication Hub for Aphasia in North Tyneside; COPM: Canadian Occupational Performance Measure; EQ-5D: EuroQol 5 Dimension; GAS: Goal Attainment Scale; OT: Occupational Therapist; PT: Physical Therapist; SF-36: 36 Item Short Form Survey; SIS: Stroke Impact Scale; SLP: Speech-Language Pathologist; SQoL-39: Stroke Quality of Life Scale-39; USA: United States of America; UK: United Kingdom.
A variety of outcome measures were used to measure social and/or leisure participation, most commonly quality of life measures (e.g., Stroke and Aphasia Quality of Life Scale-39 [SAQoL-39]), social network measures (e.g., Social Networks Communication Inventory), and functional measures (e.g., American Speech-Language-Hearing Association Functional Assessment of Communication Skills (ASHA FACS)). Outcome measures used to determine change in IADL, including communication management, varied as well. One study used the Canadian Occupational Performance Measure (COPM) and Goal Attainment Scaling (Escher et al., 2018) to measure progress in reaching individualized goals which included some IADL goals. A few studies used reading comprehension or internet skills and usage as their outcome measures (Brennan et al., 2005; Egan et al., 2004; Wilson and Read, 2016), while others used standardized self-report measures to assess communication management, such as the Communicative Effectiveness Index (Attard et al., 2018; Van der Gaag et al., 2005; Worrall and Yiu, 2010), the SQoL-39 - communication domain (Mumby and Whitworth, 2012; Van der Gaag et al., 2005; Worrall and Yiu, 2010), the Communication Confidence Rating Scale (Attard et al., 2018; Cherney et al., 2011), and the ASHA FACS (Hoover et al., 2017; Worrall and Yiu, 2010).
Additional findings are presented below, categorized by intervention features. The key interventions addressed to support participation for people with aphasia within the scope of occupational therapy included community-based groups, individually tailored programs, adaptation/presentation of materials, interprofessional interventions, and psychoeducation. Several articles used more than one of the above interventions and therefore are addressed in more than one category below.
Community-based groups
Seven articles evaluated the effectiveness of community-based group interventions (Attard et al., 2018; Cherney et al., 2011; Escher et al., 2018; Hoover et al., 2017; Mumby and Whitworth, 2012; Van der Gaag et al., 2005; Vickers, 2010). All of these studies provide Level III evidence except Vickers (2010), which provides Level II evidence. Most group interventions focused on improving social and leisure participation. This is unsurprising as groups provide a natural environment in which to practice social participation and engage in leisure activities. The types of community-based groups that were used as the mode of therapy varied and included a drama class (Cherney et al., 2011), art and advocacy groups (Mumby and Whitworth, 2012), inter-disciplinary aphasia groups (Attard et al., 2018; Escher et al., 2018; Hoover et al., 2017), and more generally, any aphasia group within an aphasia center (Van der Gaag et al., 2005; Vickers, 2010).
Cherney et al. (2011) described the results of a drama class with seven adults with chronic aphasia using multi-modal techniques to support the group member’s ability to engage in the drama activities and the theater performance. Significant improvement was reported by participants on self-report measures related to communication management and confidence in communicating with others while positive trends were noted on social participation scales (Cherney et al., 2011).
Mumby and Whitworth (2012) described the Communication Hub for Aphasia in North Tyneside program which measured results of 20 people with aphasia and their care partners who participated in a variety of community-based groups, many of which focused on the arts and advocacy. Outcomes from this study demonstrated a positive trend in relationship goals and significant improvement in communication management.
Escher et al. (2018) and Hoover et al. (2017) describe the same interprofessional intensive comprehensive aphasia program although Escher et al. included 3 years of participants (n = 19) while Hoover et al. included 4 years (n = 27). This program included both individual and group therapy sessions provided by SLPs, occupational therapists, physical therapists, and nutritionists. Significant improvement in performance and satisfaction, of goals related to IADLs (e.g., home management and communication management), leisure participation, and social participation, were noted (Escher et al., 2018; Hoover et al., 2017). Attard et al. (2018) also reported on the effects of an interdisciplinary community aphasia group program. For the seven people with aphasia who participated in at least 11 of the 12 weeks, no change in activity or participation levels was noted based on self-report. However, three participants showed gains in communication management as noted by proxy report (Attard et al., 2018).
Vickers (2010) studied the effect of a weekly aphasia group on participants’ social networks, social participation, and social isolation (n = 40). Group participants demonstrated increased contact with friends and acquaintances and significantly less perceived isolation. Results also demonstrated increased attendance at events, increased socializing with friends, and increased ability at making new friends for those who attended the weekly aphasia group compared to the control group (Vickers, 2010). Similarly, Van der Gaag et al. (2005) measured the impact of attending an aphasia center with various group offerings for people with aphasia and their family members (n = 28). They found significant improvements in social participation and communication management (Van der Gaag et al., 2005).
Adapting/presentation of materials
Two studies explored layout and design to support reading comprehension (Brennan et al., 2005; Wilson and Read, 2016) and one study used adapted materials and instructions to improve computer use (Egan et al., 2004). Each of these studies provided Level III evidence. Although all three of these studies provided one on one therapy, it is worth noting that Egan et al. (2004) initially piloted their intervention in a group setting, but quickly realized that people with aphasia needed one on one guidance to learn computer skills and revised their study methodology to pair individual volunteer tutors with each study participant.
Brennan et al. (2005) and Wilson and Read (2016) modified paragraphs to support reading comprehension. Both studies included nine participants. Brennan et al. (2005) studied changes to four different written features (i.e., vocabulary and syntax, print size, white space, and photos) while Wilson and Read (2016) modified three features including font (serif vs sans serif), sentence case (vs all capitals), and photos. Significant improvement in reading comprehension was found with adapted vocabulary and syntax, increased print size, increased white space, use of sans serif font, and sentence case print (Brennan et al., 2005; Wilson and Read, 2016). Neither study found significant improvement in use of photos though a trend toward improved comprehension was noted.
Egan et al. (2004), in their study of 20 participants, demonstrated that people with aphasia can learn computer skills with one-to-one tutoring and aphasia friendly written instructions, such as the strategies described above. Positive significant results were noted on specific internet skills, such as surfing the net, sending email, and turning off the computer.
Interprofessional and multiprofessional interventions
While many of the interventions within the studies included in this review were administered by one discipline, four articles, all providing Level III evidence, described interventions that were delivered by multiple professionals (Attard et al., 2018; Cherney et al., 2011; Escher et al., 2018; Hoover et al., 2017). Cherney et al. (2011) used two distinct professionals (a drama therapist and an SLP) who collaborated to provide the drama group intervention. Two other studies had a larger interprofessional team. Occupational therapists, SLPs, physical therapists and nutritionists collaborated to provide an intensive, 1-month, full-day program (Escher et al., 2018; Hoover et al., 2017) while Attard et al. (2018) used a team that included an SLP, a social worker, a peer aide (person post-stroke with aphasia), and a general member of the community. Van der Gaag et al. (2005) studied the impact of a multiprofessional rehabilitation service for people post-stroke with aphasia where participants received intervention from more than one discipline (SLPs, counselors, and others) but not necessarily in a collaborative manner.
While it is difficult to determine the impact of the interprofessional or multiprofessional nature of these interventions, all the studies emphasize the extensive and varied knowledge and skills provided by the varied team members and all studies demonstrated at least positive trends in participation outcomes.
Individually tailored programs
Three studies tailored the intervention to the individual (Escher et al., 2018; Mumby and Whitworth, 2012; Thomas et al., 2013) beyond goal setting. Thomas et al. (2013) provides Level I evidence while the other two provide Level III evidence. As part of the interprofessional intensive program, Escher et al. (2018) provided individualized occupational therapy using a problem-solving approach while working toward individualized goals and demonstrated significant improvement in both perceived performance and perceived satisfaction in a variety of tasks, including leisure activities and many IADLs such as cooking and grocery shopping.
Thomas et al. (2013) compared behavioral therapy and usual care with usual care alone (n = 89). The behavioral therapy consisted of a tailored program for each individual through monitoring, scheduling, and adapting participant activities to support participation and improve mood. No significant change was noted in comparison to the control (usual therapy only) group on the outcome of interest, leisure participation, as measured by the Nottingham Leisure Questionnaire. It is possible this measure was not sensitive enough to assess change as it is a self-report of frequency of leisure with options that include regularly, occasionally, and never. Also, this measure was not administered at baseline but only at 3 and 6 months. Therefore, some improvement may have been made but not accounted for.
After the introductory group sessions focusing on goal setting, participants in the study by Mumby and Whitworth (2012) were encouraged to participate in different community groups, based on their interests, abilities, and goals. Volunteers supported participation as needed, by accompanying them to the first session or providing transportation. Improvement was noted in both relationship goals and communication.
Psychoeducational
Psychoeducational approaches involve using structured, didactic teaching methods to convey information about an illness and its treatment and incorporates emotional and motivational strategies to support individuals (Ekhtiari et al., 2017). It is a common intervention approach used with people with mental illness and their care partners but is also seen in interventions with people with a broad range of health conditions. Five studies in this systematic review included a psychoeducational component to the intervention (Attard et al., 2018; Mumby and Whitworth, 2012; Ryan et al., 2017; Van der Gaag et al., 2005; Worrall and Yiu, 2010). All of these studies provide Level III evidence, except Worrall and Yiu (2010) which provides Level II evidence.
Worrall and Yiu (2010) studied the effectiveness of the Speaking Out Program, an intervention provided by trained volunteers and included both psychoeducational components and interactive activities focused around topics such as aphasia, managing finances, and using the telephone (n = 14). Although improvement in communication management was noted within groups, no significant differences were present when compared to a control group (recreational activities only). The authors suggest that changes might have been noted if the interventionist was a SLP who could individualize the program toward the participant’s goals as opposed to using a trained volunteer who needed to follow the scripted modules.
Ryan et al. (2017) evaluated the effectiveness of Aphasia Action, Success, Knowledge (Aphasia ASK) program, an intervention that provided choice of individual modules that focused on aphasia education and staying connected with others. There were only seven participants in the final analysis, but the authors found positive improvement in confidence with communication management and non-significant positive trends in quality-of-life measures that included social participation (Ryan et al., 2017).
Attard et al. (2018) provided psychoeducational groups on topics such as stroke and aphasia education, psychological and social support, conversation, and participation. As mentioned earlier, change for some participants by proxy report was noted in communication management but not in other areas of occupation.
Two studies (Mumby and Whitworth, 2012; Van der Gaag et al., 2005) provided a series of introductory educational group sessions, followed by additional group intervention. Van der Gaag et al. (2005) found significant improvements in social participation and communication management while Mumby and Whitworth (2012) found a positive trend in these same areas.
Discussion and implications
This systematic review aimed to identify effective interventions within the scope of occupational therapy practice that address participation for adults with aphasia. Across the 13 articles that were included in this review, several different approaches to intervention were studied with varying results.
Overall community-based group interventions were successful in increasing social participation, leisure participation, and communication management for adults with post-stroke aphasia. Although the majority of studies that demonstrated increased participation were Level III evidence, six of the seven studies found positive results and this is consistent with previous research which also supports the importance of group intervention for people with aphasia, including those with chronic and severe aphasia (Lanyon et al., 2018). It appears that practicing social interactions in a natural context, that of a group, can potentially increase skills in this area. The findings of this review also suggest that modifications to written materials, specifically using large print size and sans serif font, modifying syntax, and increasing white space can increase reading comprehension for adults with aphasia. This has important implications for occupational therapy related to written home programs, modifying materials such as recipes, and possibly adaptations to written assessment measures.
Additionally, two studies that used individually tailored programs found positive improvement in leisure and relationship goals, but these results must be considered with caution as the one RCT that was included in this review and focused on individually tailored programs (Thomas et al., 2013) did not find significant change on the outcome of interest, leisure participation. Psychoeducational approaches were used in several of the studies, with some significant positive results for communication management and social participation, and may be considered as a component of a successful intervention for people with aphasia. These findings are consistent with evidence-based stroke guidelines from Australia that indicate interprofessional, individually tailored interventions along with training on understanding aphasia (for patient and caregivers) are recommended components of rehabilitation for people with aphasia post stroke (Stroke Foundation 2021).
Many of the interventions included multiple components which may have impacted the results. Therefore, we were unable to determine if one approach was the effective strategy or if the combination of approaches explained why the overall results were effective. Ultimately, a multi-pronged and multidisciplinary approach may be best for people with aphasia, both owing to the uniqueness of each individual and the multiple challenges that they may experience due to aphasia often post-stroke (Clarke and Forster, 2015).
Although addressing participation is one of the core elements of occupational therapy practice, there was minimal inclusion of an occupational therapy practitioner on the intervention team of the studies in this review. Despite all 13 studies including interventions within the scope of occupational therapy, only two articles (Escher et al., 2018; Hoover et al., 2017), both addressing the same study, included an occupational therapy practitioner as part of the intervention team. Results from a systematic review of qualitative studies about the experience of adults post-stroke with communication impairments also identified areas to support participants that were within the scope of occupational therapy practice (Wray and Clarke, 2017). For example, themes that emerged from this study included “creating a meaningful role” and “creating or maintaining a support network.” The authors further suggest, “the impact of communication difficulties goes beyond symptoms of the medical impairment; influencing social relationships, mood and activities of daily living” (Wray and Clarke, 2017: 14). Future study design should consider use of occupational therapy practitioners to address participation in daily, social, and leisure activities as part of an interprofessional intervention team.
In addition to including occupational therapy as part of the intervention team, there is a need for future studies to measure and address participation more clearly. This is not a new challenge as there is extensive literature regarding the difficulties in measuring participation (e.g., Mirza et al., 2016). Participation was not necessarily the primary outcome of the studies reviewed, but rather each study was included in this review as they used at least one assessment tool that had a participation outcome component. At our initial search, there were hundreds of articles that focused on building communication skills, but only 13 focused on participation as an outcome, as defined by the OTPF (American Occupational Therapy Association, 2020), despite social and leisure participation often requiring communication. Outcome measures used in many of the studies were self-report, not observational in nature. Understanding the subjective experiences of people with aphasia is very important; however, these measures can hold bias. For instance, participants may rate their performance as worse after intervention because their insight into their abilities has improved in spite of an observer noting better performance. Using outcome measures that are based on observation and rated by professionals would provide another aspect of understanding how interventions impact participation (Nielsen et al., 2016). The Evaluation of Social Interactions During Occupational Engagement (Simmons et al., 2010) is one such outcome measure worth considering. Also, some of the studies used self-report measures not specific to people with aphasia. For example, the COPM is a semi-structured interview that can be challenging to administer reliably with people with aphasia. Adapting measures, such as the COPM, to support comprehension and access should be considered (Escher et al., 2021; Tucker et al., 2012).
As the inclusion criteria for this systematic review included participants with any communication impairment, we had hoped to capture intervention effectiveness evidence related to people with dysarthria, communication struggles due to Parkinson’s disease, and other communication challenges. The only studies that met all the inclusion criteria focused on people with aphasia post-stroke. The other articles not included either used interventions outside the scope of occupational therapy or the outcomes measured only focused on speech skills.
Lastly, aphasia presents challenges for data collection, intervention development and access to intervention. Studies have shown that it is difficult for people with aphasia to engage in research (Brady et al., 2013) and many studies use aphasia as an exclusion criterion, especially those that focus on participation outcomes and not language skills. Clinically, there are different priorities for key stages of recovery post-stroke, and participation in occupations such as social and leisure activities may not be regarded as the top priority immediately after onset. While SLPs are often the key professionals to work with people with aphasia, occupational therapy practitioners have an important role to play, as well. Due to communication challenges, people with aphasia may struggle to engage in some IADL, social activities, leisure activities, work or volunteer activities even years after onset. In addition, people with aphasia post-stroke may also be dealing with physical and/or cognitive challenges that limit their ability to participate even further. Unfortunately, people with chronic aphasia may not be able to access occupational therapy services to address their occupational participation goals. However, it is important to remember that people with communication challenges due to stroke can and do make improvements in participation, even years post injury.
This systematic review used the AOTA OTPF to define participation. Future research may benefit from using a different framework, specifically one that is more widely accepted at an international level, such as the International Classification of Function (ICF; World Health Organization, 2002), for classifying participation. Within the Activities and Participation section of the ICF the areas on communication, interpersonal interactions and relationships, and community, social, and civic life directly relate to people with aphasia participating more fully in valued life activities. Future studies should consider using the ICF framework to better identify intervention effectiveness to support participation in occupations for persons with aphasia.
Strengths and limitations
Strengths of this review lie in the rigorous design and use of PRISMA guidelines. Blind reviews occurred by two authors to determine inclusion of each study and a third reviewer participated whenever any disagreement in inclusion occurred. Additionally, results yielded an international presence, which included five articles from Australia (Attard et al., 2018; Brennan et al., 2005; Egan et al., 2004; Ryan et al., 2017; Worrall and Yiu, 2010), four articles from the United Kingdom (Mumby and Whitworth, 2012; Thomas et al., 2013; Van der Gaag et al., 2005; Wilson and Read, 2016), and four articles from the United States (Cherney et al., 2011; Escher et al., 2018; Hoover et al., 2017; Vickers, 2010). The representation of studies from multiple countries contributes to the potential applicability for the international occupational therapy community; however, we acknowledge that the countries represented are all categorized as high-income countries by The World Bank (n.d.).
This review found a lack of high-level evidence that measured participation for people with aphasia. Except for the one RCT (Thomas et al., 2013) and two Level II studies (Vickers, 2010), the other studies were Level III evidence. The majority of the Level III studies were one group pre/post-test design, and many had small sample size (nine studies had less than 30 participants, five of which had less than 15). This dearth of high levels of evidence adds to the challenge of making strong recommendations based on the 13 articles that fit the inclusion criteria. Additionally, we excluded studies that did not have outcomes related to participation, yet interventions might have been within scope of occupational therapy. Despite these limitations, there is evidence that people with aphasia can benefit from therapy within the scope of occupational therapy to improve participation outcomes.
Conclusion
This systematic review, the first one addressing occupational therapy interventions for adults with aphasia, is an initial step towards understanding how occupational therapy can effectively support adults with aphasia to increase their participation. The primary findings demonstrate concrete suggestions for ways occupational therapy practitioners can support participation for this population. Community-based group intervention is recommended for improving IADL, leisure, and social participation. Modifications to written materials are effective for increasing participation in communication management. Although not always possible, intervention in multidisciplinary or interdisciplinary teams seems to be an effective approach to address the various needs of people with chronic aphasia. As SLPs work on increasing linguistic skills, occupational therapists should address clients’ participation in meaningful occupations.
We hope that the findings of this systematic review provide OT practitioners with beginning evidence to support their role with adults with aphasia. Although SLPs have the primary role of working on language and communication with people with aphasia, return to valued roles, routines, and participation in meaningful activity are goals of people post-stroke with aphasia and the focus of occupational therapy practice.
Key findings
• Interventions within scope of occupational therapy are effective for increasing participation in activities for people with aphasia. • Effective interventions include modifications to written materials and community-based groups.
What the study has added
This systematic review highlights effective interventions that focus on increasing participation in meaningful activities for people with aphasia and provides beginning evidence demonstrating the value of occupational therapy for people with aphasia.
Footnotes
Acknowledgments
The authors wish to acknowledge Kate Silfen, Boston University Health Sciences Librarian, for lending her expertise to the search terms and search strategy. We also wish to thank Magdalen Balz, our SLP colleague, for consulting on search terms.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Research ethics
Ethics approval was not required for this study.
Search terms PubMed
#1 adults [MeSH] OR adult [TIAB] OR “middle aged” [MeSH] OR “middle aged” [TIAB] OR aged [MeSH] OR aged [TIAB] OR “young adult”[MeSH] OR “young adult” [TIAB] #2 “nervous system diseases”[MeSH] OR “nervous system disease”[TIAB] OR “neurological disorder”[TIAB] OR “neurological impairment” [TIAB] “Parkinson disease”[MeSH] OR “Parkinson disease”[TIAB] OR stroke[TIAB] OR stroke[MeSH] OR “Amyotrophic Lateral Sclerosis”[Mesh] OR “amyotrophic lateral sclerosis”[TIAB] OR “Brain Injuries, Traumatic”[Mesh] OR “brain injuries”[tiab] OR “Multiple Sclerosis” [Mesh] OR “Alzheimer disease” [Mesh] OR “aphasia, primary progressive” [Mesh] OR “frontotemporal dementia” [Mesh] #3 aphasia [MeSH] OR aphasia [TIAB] OR “communication disorders” [MeSH] OR “communication disorder”[TIAB] OR “acquired communication disorder”[TIAB] #4 “occupational therapy”[MeSH] OR “occupational therapy”[TIAB] OR “Rehabilitation of Speech and Language Disorders”[MeSH] OR “Rehabilitation”[MeSH] OR rehabilitation[TIAB] OR “Therapeutics”[MeSH] OR therapy[TIAB] OR intervention[TIAB] OR “Communication Aids for Disabled”[Mesh] OR “communication aid”[TIAB] OR “Patient Education as Topic”[Mesh] OR “patient education”[TIAB] OR “social participation” [MeSH] OR “social participation”[TIAB] OR “Leisure Activities”[Mesh] OR “leisure participation”[TIAB] OR “community participation”[MeSH] OR “community participation”[TIAB] OR “quality of life”[MeSH] OR “quality of life”[TIAB] OR “mental health”[MeSH] OR “mental health”[TIAB] OR “well being”[TIAB] OR volunteer[TIAB] OR “human activities”[MeSH] OR “augmentative and alternative communication”[TIAB] OR “script training”[TIAB] OR “psychosocial adjustment”[TIAB] OR “Adaptation, Psychological”[Mesh] OR “Activities of Daily Living”[Mesh] OR “activities of daily living”[TIAB] OR “Reading”[Mesh] OR “Health Promotion”[Mesh] OR “Health Behavior"[Mesh] OR “Self-Management”[Mesh] OR “self-management”[TIAB] OR “Problem Solving”[Mesh] OR “problem solving”[TIAB] OR “partner training”[TIAB] #4 ”Practice Guideline”[Publication Type] OR “Randomized Controlled Trial”[Publication Type] OR “Systematic Review”[Publication Type] OR “Controlled Clinical Trial” [Publication Type] OR “Cohort Studies”[Mesh] OR “Meta-Analysis”[Publication Type] OR “Comparative Study”[Publication Type] OR “Evidence-Based Practice”[Mesh] OR “Epidemiologic Studies”[Mesh] OR “Double-Blind Method”[Mesh] OR “Case Reports” [Publication Type] OR “practice guideline”[TIAB] OR “randomized controlled trial”[TIAB] OR “systematic review”[TIAB] OR “controlled clinical trial”[TIAB] OR “cohort study”[TIAB] OR “meta-analysis”[TIAB] OR “comparative study”[TIAB] OR “evidence based”[TIAB] OR “epidemiologic studies”[TIAB] OR “double blind”[TIAB] OR “case report”[TIAB] OR “case study”[TIAB] Note: “AND” was used between lines; All words searched in title, abstract, and MESH terms.