
Abstract
Introduction:
Deficits in visual scanning can result from various neurological or sensory conditions, disrupting the ability to gather and interpret visual information. The Bioness Integrated Therapy System offers a promising tool for screening and improving functional vision. The study aimed to provide preliminary reference data for visual scanning performance using user-paced and time-paced Bioness Integrated Therapy System programs.
Method:
Descriptive study conducted at the University of Alabama at Birmingham, Center for Low Vision Rehabilitation. Eighty healthy adults aged 19–29 and 50–59 years were included. Participants were randomly assigned to one of two age categories and completed four sets of both programs. Each session included four sets of visual scanning tasks, with familiarization and actual trials for each program. Accuracy, reaction time, and number of hits were collected following each actual trial.
Results:
Preliminary reference data were established for each program and dependent variables. Reaction time showed significant main effects for central fixation in young adults (F = 213.671, α < 0.001, η² = 0.846) and middle-aged adults (F = 225.853, α < 0.001, η² = 0.853), respectively.
Conclusions:
This study offers preliminary reference benchmarks for visual scanning using Bioness Integrated Therapy System, supporting its utility in occupational therapy for assessing and addressing scanning deficits.
Introduction
Visual scanning requires coordinated movement of the eyes, head, and body to systematically locate and interpret environmental stimuli. This function integrates perceptual-motor and cognitive processes and is influenced by interest, expectations, and task demands (Circelli et al., 2013; Warren, 2017). Neurological injuries, aging, or sensory deficits can cause visual scanning impairments, which disrupt focal inspection, making it difficult to form an accurate internal representation of the environment and complete daily functioning (Senger et al., 2017).
Visual scanning strategies may be influenced by modifications to environmental context, lighting, and task familiarity. Structured training can improve visual scanning through neuroplasticity, as visual scanning training is a promising intervention that aims to enhance the efficiency, precision, and coordination of visual exploration (Kolb and Gibb, 2014; Stone et al., 2019). Additionally, vision rehabilitation leverages residual vision and teaches compensatory strategies to enhance function (van Nispen et al., 2020). Specifically, the Bioness Integrated Therapy System (BITS) is a computerized training tool that offers targeted interventions to address deficits. BITS includes programs focusing on visual scanning, pursuit, visual motor coordination, cognition, and assessment. These programs can be modified based on the user’s needs and clinical goals, with built-in metrics for measuring progress. In contrast, Dynavision D2, a well-established visual training tool, has normative data and reliability metrics (Wells et al., 2014). The current study serves as a precursor to expanded normative data collection on BITS and comparisons between BITS and Dynavision, focusing on two BITS programs, user- paced and time-paced, which correspond to Dynavision’s modes A and B, respectively.
In the user-paced mode, stimuli appear randomly but continuously on the screen so participants can locate them and respond at their own speed. In time-paced mode, stimuli disappear after a brief interval, requiring quicker responses. Familiarization trials are recommended before testing to mitigate learning effects and ensure participant readiness, such as maintaining posture and proper distance from the screen and understanding task demands (Wells et al., 2014). For both programs, participants are encouraged to use eye, head, and trunk movements as needed.
To our knowledge, normative data for the BITS visual scanning programs have not been published. Therefore, this study aims to provide preliminary reference data for young and middle-aged adults across outcomes, modes, and fixation. These benchmarks can help occupational therapists integrate BITS programs into structured scanning protocols, tailor intervention intensity based on baseline performance, and align treatment plans with functional goals such as improving reading, mobility, and activities of daily living safety. By linking performance metrics with everyday occupational outcomes, this study provides practical guidance for both clinical decision-making and interdisciplinary rehabilitation planning. In addition, we hypothesize that differences in reaction time will exist between age groups and between program types.
Method
Study design
This descriptive study aimed to generate preliminary reference data for the BITS visual scanning programs in two age groups: young adults (19–29 years) and middle-aged adults (50–59 years). Participant age groups were selected based on prior literature and partly for pragmatic recruitment reasons. A 2 × 2 within-subjects design was used, examining the effects of pacing conditions (user-paced and time-paced) and fixation conditions (with and without central fixation) on accuracy, reaction time, and number of hits. The study was conducted at the University of Alabama at Birmingham (UAB) Center for Low Vision Rehabilitation. Institutional Review Board approval was obtained from UAB.
Participants
Eighty healthy participants were recruited through convenience and snowball sampling. Each age group included 40 individuals. A G*Power analysis indicated that this sample size would yield a power of 0.87 with α = 0.05 and two repeated measures. Additionally, we used an effect size of .25 to detect a moderate effect size difference. Recruitment occurred via campus flyers, emails, and social media.
Inclusion criteria required participants to be English-speaking adults without physical, visual, balance, or cognitive impairments. Individuals with corrected visual acuity (e.g., wearing prescription lenses) were eligible. Exclusion criteria included neurological impairments, seizure history, upper extremity range-of-motion limitations, hand numbness, and inability to stand or walk without assistive devices.
Participants’ inclusion criteria were ensured through a two-step self-report screening process. First, all participants filled out a Qualtrics survey, requiring a mandatory response to health status items. Participants who self-reported having a disability were automatically excluded from completing the survey. Second, the first author reviewed participants’ responses and clarified unclear ones through phone calls to ensure eligibility.
Procedures
Each participant completed a single testing session. Height, arm span, and viewing distance were recorded to ensure consistent positioning. Participants were randomly assigned to one of four groups (A–D), stratified by age and task order (see Table 1). Groups A and B (young and middle-aged adults, respectively) began with user-paced tasks, while Groups C and D began with time-paced tasks.
Study protocol.
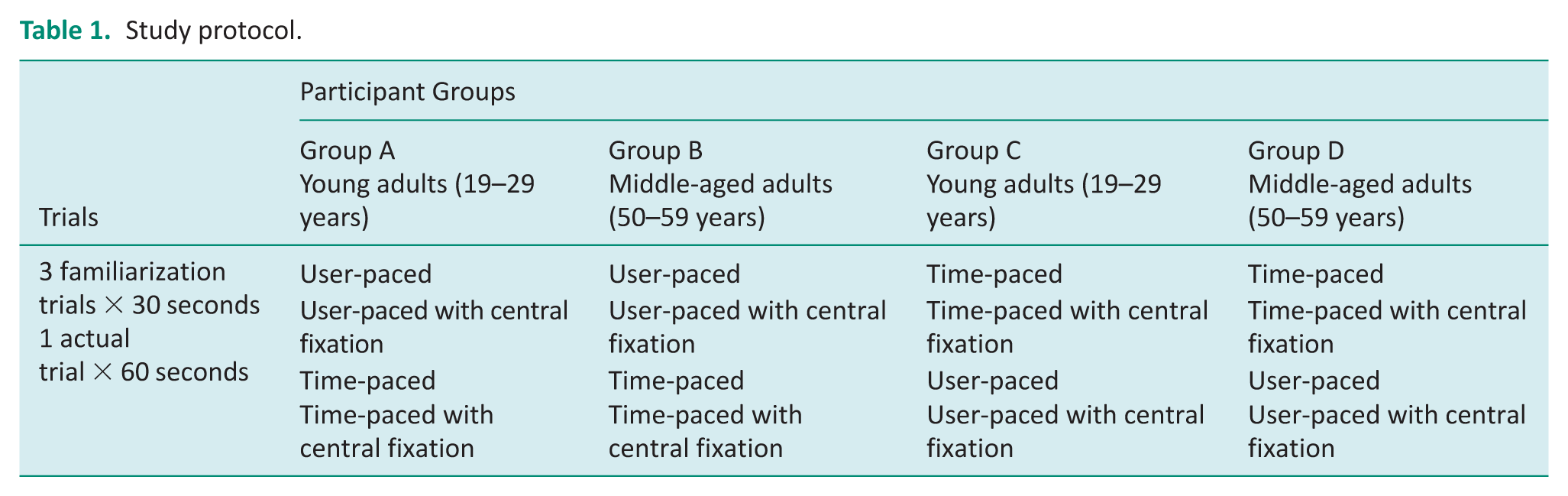
Each session included four programs exposing the subject to each pacing mode with and without central fixation. For each condition, participants completed three 30-second familiarization trials and one 60-second actual trial. The familiarization trials, which included verbal feedback to ensure comprehension, helped standardize positioning (e.g., eye fixation, slightly bent knees, elevated arms) and reduced learning effects.
Before each program, participants received standardized verbal instructions. Testing occurred in a quiet, private room with overhead lighting turned off to reduce glare and enhance contrast. BITS protocols allowed participants to use both hands, a stylus, and turn their heads.
In all tests, central fixation was maintained by instructing participants to focus on the “Start” button in the screen’s center prior to task initiation. Default BITS settings were used (stimulus size, 5; duration, 60 seconds; circle stimuli; and blue-and-white background). Stimuli in time-paced programs disappeared after 3 seconds if not activated by tapping.
Data collection
Demographic and vision history data included age, gender, date of birth, dominant hand, use of corrective lenses, history of neurological or physical impairments, race, and contact information. These demographics reflect participants from diverse ethnicities within a single urban region, which may limit the generalizability of our findings to populations in less diverse or rural regions. Additionally, the prevalence of eye diseases is known to vary across ethnicities and different regions. Therefore, interpreting our findings for other demographic groups should be done with caution. Upon arrival, participants’ dates of birth were verified using a valid ID.
BITS software automatically recorded the outcome measures:
Metrics were collected during each of the four conditions. For each age group, quartile performance on each outcome was reported for each condition to yield preliminary reference results. Bootstrap analyses were conducted to determine standard errors within each quartile and estimate confidence intervals for comparisons within and between age groups. Within-subjects ANOVAs (2 pacing × 2 fixation) were used to analyze main and interaction effects within age-group.
Results
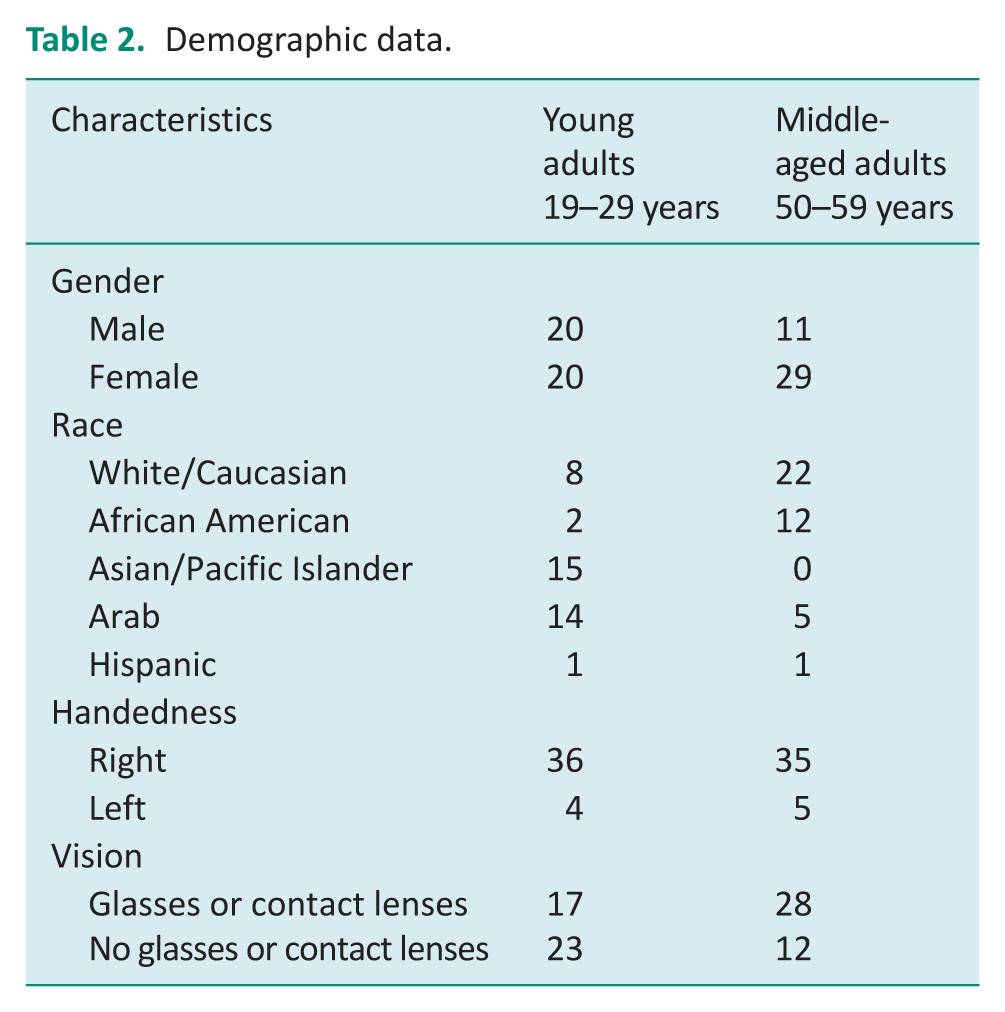
Eighty participants enrolled in this study from October 2024 to March 2025, with 40 participants in each age cohort. Most participants in the young adult group were Arab and Asian/Pacific Islander, right-handed, and did not wear corrective lenses; those in the middle-aged group were mostly White/Caucasian and African American (see Table 2 for further demographic information).
Demographic data.
Preliminary reference data
Table 3 presents reference visual scanning data for 40 healthy young adults, with a graphical representation provided in Figure 1. Due in part to the small sample size, an overlap of 95% confidence intervals of quartile values occurred between the first, second, and third quartiles. However, we found differences in confidence intervals between the first and second quartiles for reaction time in all programs and conditions, which supported our hypothesis. For example, the reaction time for user-paced without central fixation, we are 95% confident that the 25th percentile for the population is between 0.74 and 0.78 and that the 50th percentile for the population is between 0.80 and 0.84. There were also gaps for confidence intervals between the second and third quartiles for reaction time in user-paced tasks without central fixation, as well as for accuracy and reaction time in time-paced tasks with central fixation. All other confidence intervals for sequential quartiles overlapped.
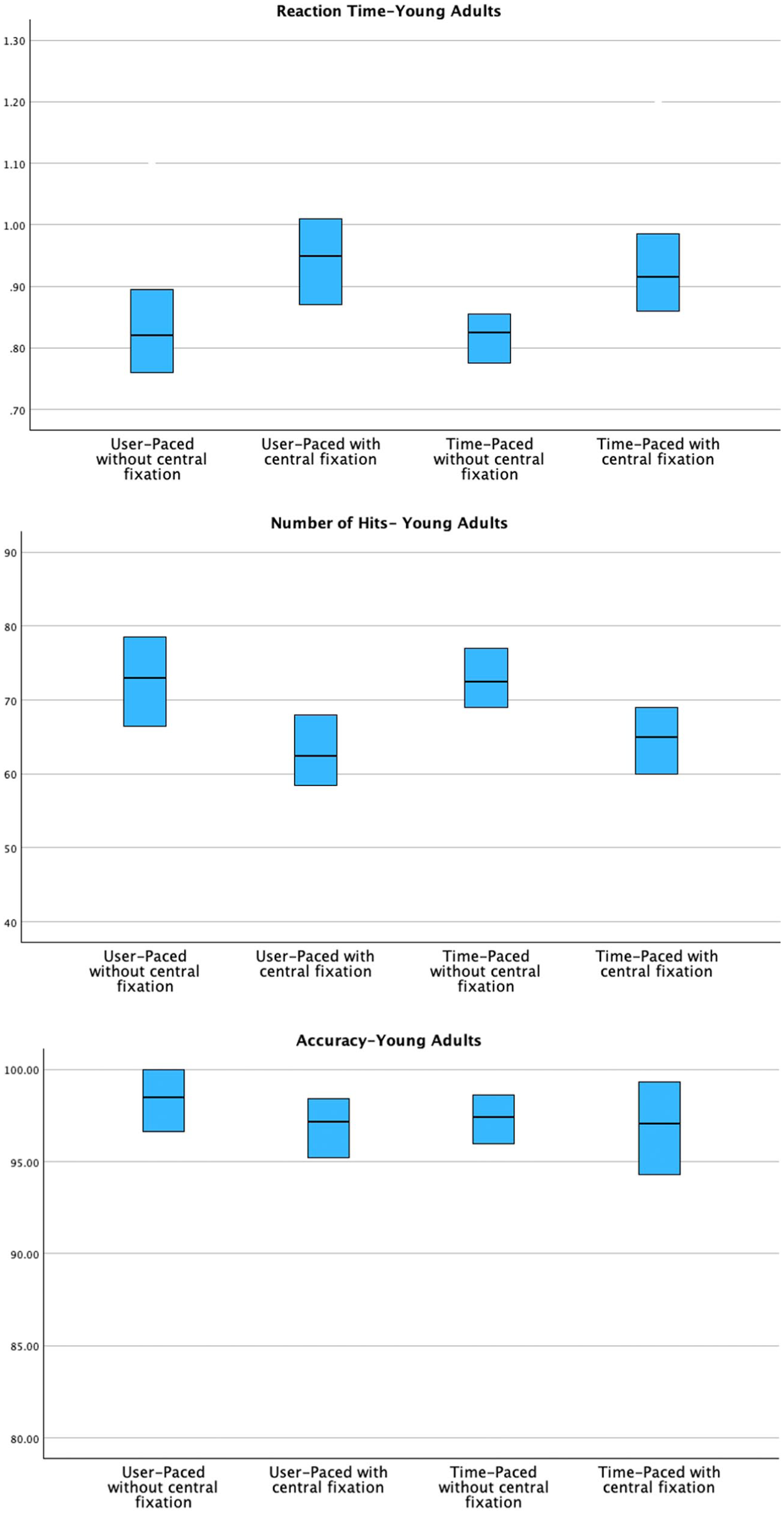
Graphical representation of preliminary reference visual scanning data among young adults.
Reference visual scanning data for healthy young adults.
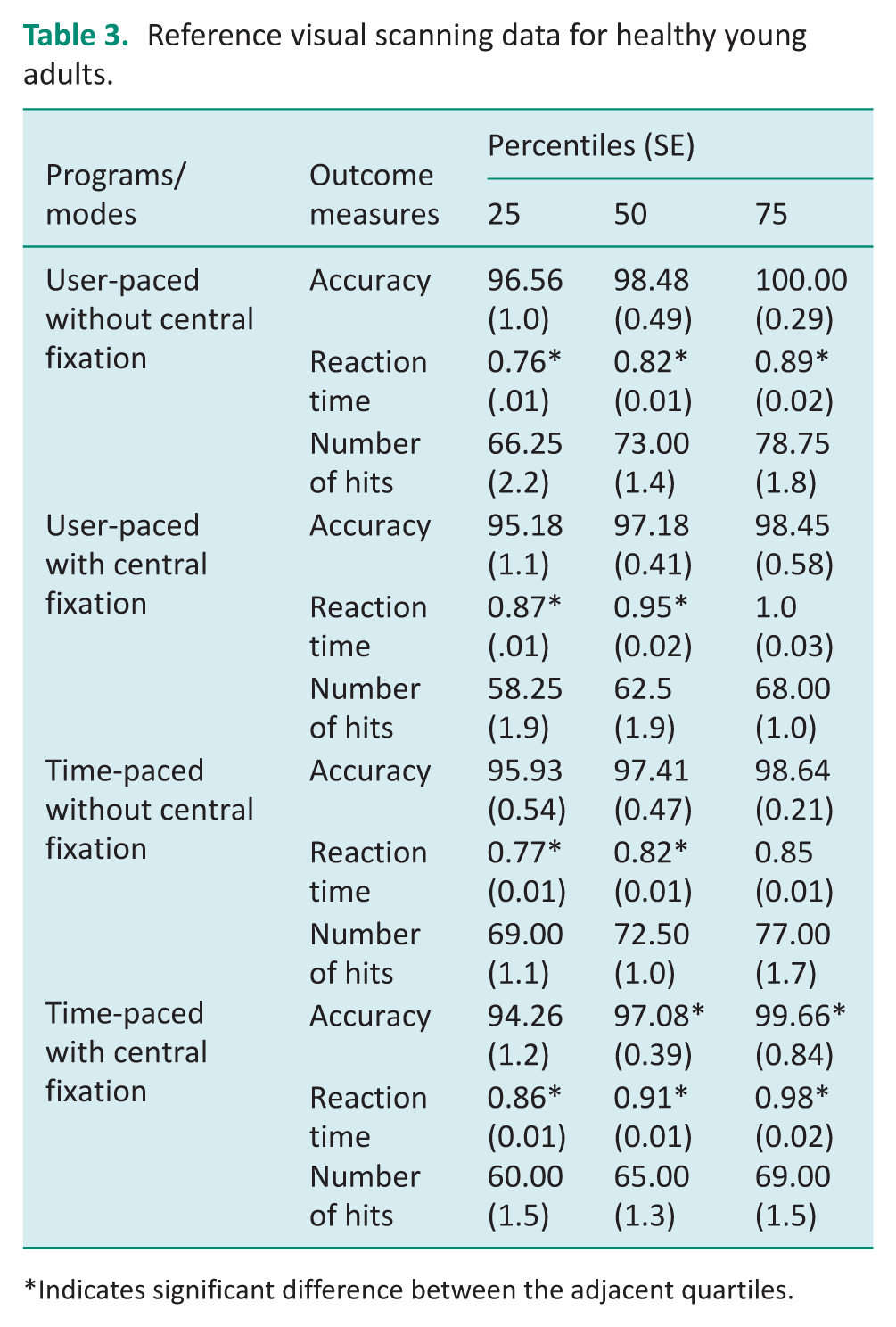
Indicates significant difference between the adjacent quartiles.
Based on Kruskal–Wallis analysis, the only differences between races across dependent variables (accuracy, reaction time, number of hits) were for user-paced number of hits (α = 0.03), user-paced with central fixation number of hits (α = 0.04), time-paced number of hits (α = .02), and time-paced with central fixation accuracy (α = 0.02). There was no difference between gender and the dependent variables for any condition.
Table 4 provides reference visual scanning data for 40 healthy middle-aged adults, with a graphical representation provided in Figure 2. With two standard error confidence intervals, we found differences between the first and second quartiles for the number of hits in user-paced tasks without central fixation and reaction time in time-paced tasks without central fixation. There were also differences between the second and third quartiles for reaction time in user-paced tasks with central fixation and the number of hits in time-paced tasks with central fixation.
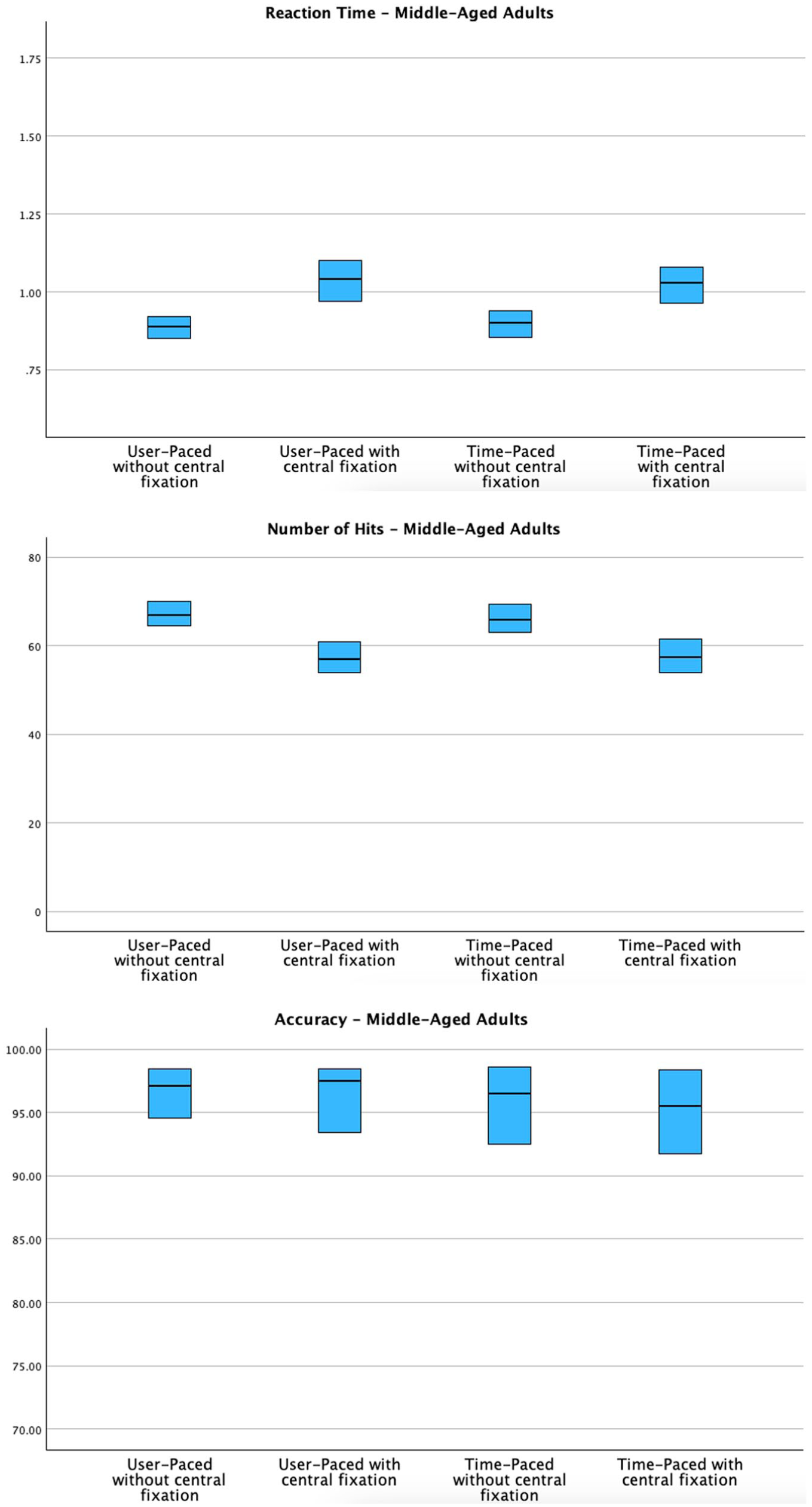
Graphical representation of preliminary reference visual scanning data among middle-aged adults.
Reference visual scanning data for healthy middle-aged adults.
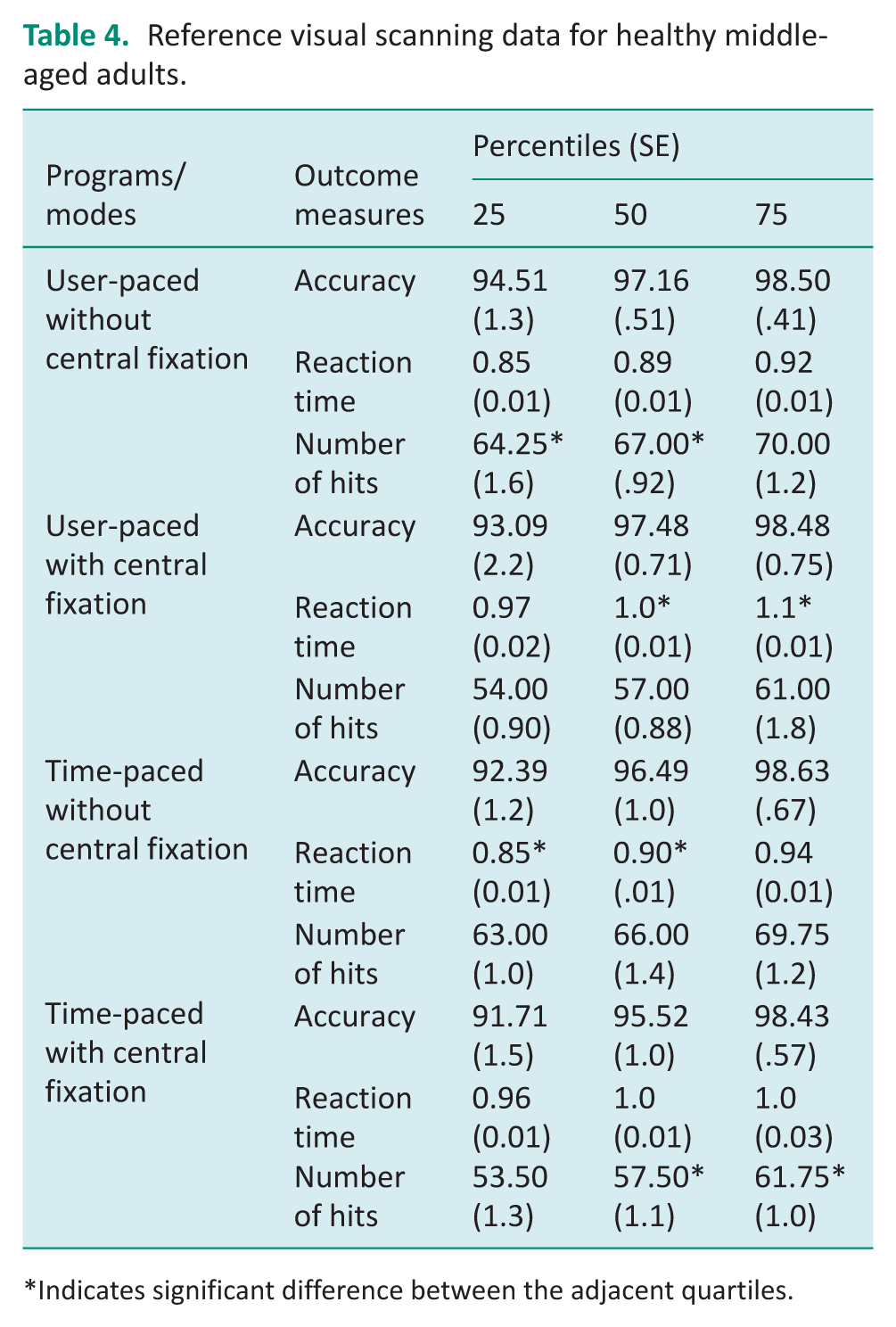
Indicates significant difference between the adjacent quartiles.
Based on Kruskal–Wallis analysis, there were no significant differences between race and gender for our dependent variables (accuracy, reaction time, number of hits) for any condition.
Effects of condition on outcomes
Young adults
Reaction time: Repeated measure ANOVA was performed to analyze the reaction time of 40 young adult participants. Results showed a significant main effect for program/mode (F = 7 .55, α = 0.009, η² = 0.162), central fixation (F = 213.671, α < 0.001, η² = 0.846), and the interaction between these factors (F = 4.377, α = .043, η² = .101), all of which supported our hypothesis. The interaction effect was due to a greater decrease in reaction time for central fixation between user-paced and time-paced tasks. There was no interaction between the modes, central fixation, and device order (α = 0.225). Additionally, our findings showed that young adults performed faster on time-paced programs and programs without central fixation than on user-paced programs. Improvements in reaction time in user-paced versus time-paced tasks were greatest for the condition without central fixation.
Number of hits: There was a significant main effect for number of hits for program/mode (F = 5.339, α = 0.026) and for central fixation (F = 273.219, α < 0.001); however, the interaction between these factors was not significant (F = 3.604, α = 0.065). The number of hits was significantly higher for the time-paced program and tasks without central fixation.
Accuracy: The main effect for accuracy of young adults’ performance was not significant for programs/modes (F = 0.410, α = 0.526, η² = 0.010), central fixation (F = 2.707, α = 0.108, η² = 0.065), or the interaction between these factors (F = 0.012, α = 0.915, η² = 0.000).
Middle-aged adults
Reaction time: A repeated measure ANOVA was performed to analyze the reaction time of 40 middle-aged participants. Results showed a significant main effect for central fixation (F = 225.853, α < 0.001, η² = 0.853) but not for program/mode (F = 0.084, α = 0.774, η² = 0.002) or interaction between factors (F = 1.672, α = 0.204, η² = 0.041). Reaction times were slower for user-paced and time-paced tasks with central fixation.
Number of hits: There was a significant main effect for number of hits for central fixation (F = 70.149, α < 0.001, η² = 0.643) but not for program/mode (F = 0.437, α = 512, η² = 0.011) or interaction between factors (F = 0.131, α = .720, η² = 0.003). We also found that middle-aged adults could identify more targets with both time-paced and user-paced programs without central fixation.
Accuracy: The main effect for accuracy of middle-aged adults’ performance was not significant for programs/modes (F = 0.3.131, α = 0.085, η² = 0.074), central fixation (F = 0.542, α = 0.466, η² = 0.014), or the interaction between these factors (F = 0.263, α = 0.611, η² = 0.007).
Discussion
This descriptive study aimed to obtain preliminary reference data and analyze visual scanning performance using BITS user-paced and time-paced programs in adults aged 19–29 years and 50–59 years.
Comparison within the age group
Tables 3 and 4 provide preliminary reference data for young and middle-aged adults across all four conditions. Although some quartile confidence intervals overlapped, perhaps due to the modest sample size, reaction time showed small standard errors of quartiles, suggesting BITS may be a sensitive and stable measure for screening and training visual scanning skills. Observed reaction times ranged from 0.74 to 1.12 seconds. Clinicians may consider performance above the 75th percentile for reaction time and below the 25th percentile for number of hits and accuracy as potential indicators of reduced visual scanning efficiency and potentially reflective of delayed processing, which may warrant further assessment.
Participants frequently reported that time-paced programs with central fixation were more challenging. In these conditions, participants had only 3 seconds to locate and activate a stimulus following a centrally focused start, which increased task complexity. These findings align with clinical observations that combining timing constraints with attentional control can elevate task demands, particularly in middle-aged or neurologically vulnerable individuals.
Using three familiarization trials reduced the learning effect and allowed participants to practice and adjust their posture (e.g., maintaining upright stance, engaging head and trunk movement, and positioning arms for activation). This strategy may be especially valuable when using BITS with patients who require additional time to adapt to unfamiliar technology or tasks.
The first quartile for accuracy and number of hits, and the third quartile for reaction time reflect points that may be of clinical importance to clinicians identifying patients that may benefit from training. Subjects that fall outside such quartiles (or the confidence intervals for such quartiles) are within the lowest performing 25% of the sample on those outcomes within different program/mode combinations.
Comparison between age groups
Analysis of interquartile ranges (Table 5) demonstrated that young adults generally outperformed middle-aged adults on reaction time and number of hits, especially in time-paced conditions. For example, in time-paced tasks without central fixation, the 25th percentile reaction time for young adults was 0.77 seconds (CI 0.75–0.79), compared to 0.85 seconds (CI 0.83–0.87) for middle-aged adults. Similarly, young adults consistently recorded higher hit counts across all conditions. These differences suggest age-related decline occurs in visual-motor response speed and target acquisition, even in healthy adults without identified impairments (Li et al., 2021; Markowitz, 2006).
Analysis of interquartile ranges for reference visual scanning data for both groups.
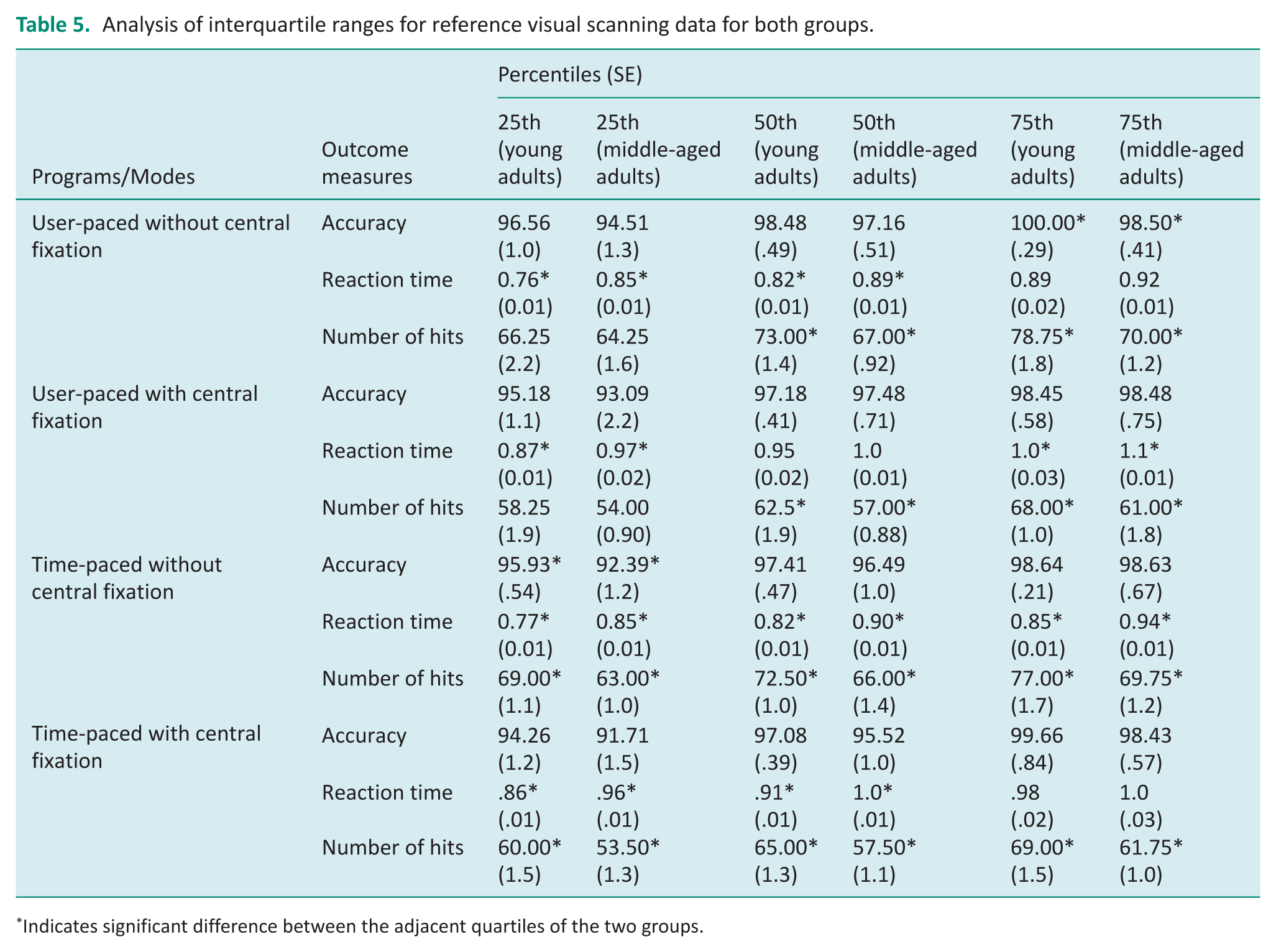
Indicates significant difference between the adjacent quartiles of the two groups.
As accuracy was high across both groups, it was less effective at detecting subtle performance differences. This supports prior findings that accuracy, when near ceiling, may not be an ideal standalone metric in normative or screening contexts (Larner, 2019). Clinicians may prefer to prioritize reaction time and hit count when using BITS as a performance measure.
For both age groups, reaction time showed significant main effects for central fixation, supporting our hypothesis that visual scanning performance would be influenced by fixation demands. All participants performed faster in both programs without central fixation. Similarly, number of hits was significantly affected by central fixation, indicating that both age groups performed better without central fixation. In contrast, accuracy remained consistently high in all conditions, likely due to a ceiling effect, as most participants exceeded 90% accuracy regardless of program mode.
We also found an interaction effect in reaction time between age group and central fixation (F = 5.43, α = 0.022, η² = 0.065), indicating that middle-aged adults were more affected by central fixation demands than younger adults. This suggests that older adults may require more processing time to transition from central fixation to peripheral target response, possibly due to age-related slowing in attentional shifting or motor planning (Stöckel et al., 2017).
The Kruskal–Wallis analysis revealed no significant group differences by gender or race across most conditions. However, in the young adult group, significant differences were observed in the number of hits for user-paced and time-paced programs (α = 0.03 and α = 0.02, respectively) and in accuracy for time-paced tasks with central fixation (α = 0.02). While interesting, these findings should be interpreted with caution, given the small subgroup sizes and homogeneity within certain demographic categories.
Significance and future research
To our knowledge, this is the first study to report preliminary reference data for visual scanning programs using BITS. These findings offer a benchmark for therapists using BITS in clinical practice and may support its use as both a screening and training tool for clients with visual scanning deficits. Previous work by Fagan et al. (2022) highlighted the utility of BITS in addressing visual field awareness; our study extends this evidence by identifying age-specific baseline performance across pacing and fixation conditions.
The results also align with literature on neuroplasticity and the potential for structured visual scanning training to improve visual attention and motor response (Kolb and Gibb, 2014; Stone et al., 2019) and quality of life (van Nispen et al., 2020). Future studies should explore BITS-based interventions in clinical populations, such as individuals with stroke, traumatic brain injury, or age-related visual decline, to examine generalizability and treatment responsiveness. Specifically, we recommend that researchers explore the minimal clinically important difference for BITS metrics in clinical populations, such as stroke. Additionally, we recommend incorporating more challenging tasks to examine the ceiling effect of accuracy in either healthy individuals or clinical populations with vision impairments.
Limitations
Several limitations should be noted. First, participants were recruited from a single urban region, limiting external validity. Despite this, we tried to minimize bias by randomly assigning participants to different groups for each age category. Second, while the sample size was adequate for preliminary analysis, it may not provide robust population norms. Third, inclusion was based on self-report, which may have introduced bias or underreported mild impairments. However, the first author reviewed participants’ responses and clarified unclear ones through phone calls to ensure eligibility. Finally, motivation and fatigue likely influenced performance, particularly in longer sessions. Some participants, especially those in the middle-aged group, reported fatigue and visual discomfort due to screen brightness and sustained attention requirements. These factors underscore the need to monitor engagement and offer breaks during clinical or research use of BITS. To address this limitation, fatigue and visual discomfort were controlled throughout the procedure by changing the room lighting and offering breaks when needed.
Implications for occupational therapy practice and research
This study provides the following implications for occupational therapy practice and research:
BITS offers a standardized, practical tool for assessing and treating visual scanning deficits in clinical settings, supporting participation in ADLs and IADLs.
Age-based reference data (Tables 3 and 4) allow therapists to identify reduced scanning performance and track client progress.
Reaction time and number of hits are the most sensitive metrics for differentiating performance and guiding intervention.
Central fixation tasks increase difficulty, supporting graded training for clients needing higher-level visual attention demands.
Familiarization trials improve consistency, helping clients adjust to the task and interface.
Further research should validate BITS across diverse populations and explore links between BITS performance and functional outcomes.
Conclusion
BITS is a promising tool for assessing and addressing visual scanning performance in adults. This study provides preliminary reference data for user-paced and time-paced programs, offering age-based benchmarks that support occupational therapy assessment and intervention. Findings suggest that reaction time and number of hits are sensitive indicators of scanning performance and may be useful in identifying deficits. Future research should validate these results in clinical populations and explore the broader applicability of BITS across age ranges and practice settings.
Key findings
BITS offers a practical tool for assessing and treating visual scanning deficits.
Reaction time and number of hits are the most sensitive metrics for guiding intervention.
What the study has added
This is the first study to present reference data for BITS visual scanning programs, supporting their clinical use for addressing scanning deficits in occupational therapy settings and highlighting the need for validation with broader populations.
These reference data can help occupational therapists integrate BITS programs into structured scanning protocols, tailor intervention intensity based on baseline performance, and align treatment plans with functional goals such as improving reading, mobility, and activities of daily living safety.
By linking performance metrics with everyday occupational outcomes, this study provides practical guidance for both clinical decision-making and interdisciplinary rehabilitation planning.
Footnotes
Acknowledgements
We thank Sarah Beth Spraberry, MSOT, OTR/L, faculty members, PhD candidates, and students at UAB, particularly those from Saudi Arabia, who helped recruit participants and showed their support throughout the data collection phase. We also thank Emily Delzell, UAB grant writer at UAB, for reviewing this manuscript.
Research ethics
The study was conducted at the University of Alabama at Birmingham (UAB) Center for Low Vision Rehabilitation. Institutional Review Board approval was obtained from UAB. The UAB IRB Protocol#: IRB-300012642.
Consent
A written informed consent was obtained from participants as part of the Qualtrics survey.
Patient and public involvement data
During the development, progress, and reporting of the submitted research, Patient and Public Involvement in the research was not included at any stage of the research.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors declared no financial support for the research, authorship, and/or publication of this article.
Contributorship
• All authors contributed to the development of the study protocol and reviewed the manuscript.
• LA was involved in gaining ethical approval, recruiting participants, data collection, data analysis, writing, and editing the manuscript.
• SS was involved in data analysis and interpretation of findings.
• JV and EB were involved in conceptualizing the research idea, study design, and reviewing the discussion.