
Abstract
Introduction:
Occupational balance significantly affects healthcare professionals’ health and well-being. However, existing scales for assessing the occupational balance cannot measure multiple aspects. This study aimed to develop and validate the Occupational Balance Assessment Scale (OBAS) to analyze occupational balance of healthcare professionals across multiple aspects.
Method:
Phase 1 involved the development of conceptual framework and item pool through literature review and consensus among five occupational therapists, followed by assessment content validity. Phase 2, psychometric tests were performed to refine the scale using data from 318 healthcare professionals in Japan, assessing internal consistency, structural validity, criterion validity, and construct validity.
Results:
The final OBAS included 15 items across five factors (Resources, Time, Adjustment, Taxonomy, and Meaning). The scale demonstrated excellent internal consistency (Cronbach’s α = 0.903) and good structural validity (comparative fit index = 0.947, root mean square error of approximation = 0.082). Criterion validity showed strong positive correlation with occupational dysfunction (r = 0.81, p < 0.001), moderate positive correlation with stress response (r = .61, p < 0.001), and moderate negative correlation with self-control (r = −0.47, p < 0.001).
Conclusion:
The OBAS has established reliability and validity. This tool is useful for comprehensively assessing occupational balance of healthcare professionals.
Keywords
Introduction
Occupational balance is a foundational concept in occupational therapy (Meyer, 1922). Occupational balance is commonly considered a component of lifestyle balance, describing an individual’s perception of having an appropriate quantity of occupations and an adequate variation between them (Matuska and Christiansen, 2008; Wagman et al., 2012; Yamane and Yoshikawa, 2022). However, occupational balance lacks an agreed-upon definition, reflecting historical variations and the coexistence of multiple aspects on occupational balance in the modern era (Wagman et al., 2012; Yamane and Yoshikawa, 2022). Particularly in today’s complex lives, it is essential not only to allocate the quantity of occupations but also to adjust them in response to changing situations and contexts (Yazdani et al., 2018; Backman, 2013; Barbara et al, 2023). For example, adjustment refers to the individual's ability to reorganize or modify their occupations in the face of contextual demands, while maintaining the perception of occupational balance. However, no existing assessment scales have focused on the adjustment of occupational balance (Yamane and Yoshikawa, 2022).
Modern occupational balance is conceptualized as harmony because it involves multiple aspects (Backman, 2013; Eklund et al., 2017; Lomas, 2021; Liu et al., 2023). Harmonization requires accommodating changes in occupational balance (Eklund et al., 2017). However, failure to adapt to changes in occupational balance, resulting in its disruption, can lead to a decline in health-related quality of life and deterioration in mental health, thereby contributing to the occurrence of stress-related disorders such as depression and burnout (Anaby et al., 2010; Håkansson and Ahlborg, 2017; Wagman et al., 2017). This issue is particularly serious among healthcare professionals, a high-stress group (Wagman et al., 2017). In Japan, evidence indicates that approximately 63% of healthcare professionals experience difficulties in maintaining occupational balance (Miyake et al., 2014). Therefore, achieving harmony requires analyzing multiple aspects of occupational balance and making necessary adjustments (Backman, 2013; Barbara et al., 2023; Yazdani et al., 2018).
Based on these findings, achieving appropriate occupational balance requires analyzing its multiple aspects with a focus on adjustment (Backman, 2013; Barbara et al., 2023; Yazdani et al., 2018). The Occupational Balance Questionnaire 11 (OBQ11; Wagman and Håkansson, 2014; Håkansson et al., 2020), Satisfaction with Daily Occupations and Occupational Balance (SDO-OB; Eklund and Argentzell, 2016), and Occupational Balance-Questionnaire (OB-Quest; Dür et al., 2014) are existing scales for measuring occupational balance. However, none of these scales includes items related to adjustment. Additionally, the SDO-OB targets individuals with mental health disorders (Eklund and Argentzell, 2016), and OBQ11 and OB-Quest have a single-factor structure (Hernandez et al., 2023; Ho et al., 2020), leaving the research gap unaddressed. There is a need to develop and validate a new assessment tool that can measure the multiple aspects of occupational balance with a focus on adjustment.
Therefore, this study aimed to develop the Occupational Balance Assessment Scale (OBAS), a comprehensive scale specifically for healthcare professionals that focuses on adjustment and conducts a multiple aspects analysis of occupational balance. The significance of this study lies in providing occupational therapists with the OBAS, a new assessment scale that enables assessment of occupational balance from multiple aspects. By equipping occupational therapists with the OBAS, this study contributes to interventions aimed at improving healthcare professionals’ health and well-being. Furthermore, the findings provide valuable insight into evaluating the effectiveness of occupational therapy interventions through measurable outcomes.
Methods
Study design
This two-phase methodological study was conducted in accordance with the international standards of scale development, particularly the COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN; Gagnier et al., 2021), to confirm the validity and reliability of the scale, including content validity, item response theory, exploratory factor analysis, confirmatory factor analysis, internal consistency, and hypothesis testing for construct validity. This study was approved by the Ethics Review Board of Kibi International University (Approval Number: 22-33). Approval for data collection was obtained from the representatives of each participating facility. This study was conducted in two phases: Phase 1, in which the conceptual framework of occupational balance was developed, and the item pool was created, and the content validity of the prototype OBAS was evaluated; Phase 2, in which data were collected from healthcare professionals using the prototype OBAS developed in Phase 1. The items included in the final OBAS were selected based on their validity and reliability.
Procedure
Phase 1: Development of the prototype OBAS
Phase 1 aimed to refine the conceptual framework of the occupational balance and scale items, examine item content validity, and develop the prototype OBAS.
Literature review for developing operational definitions of constructs
A literature review was conducted between April and December 2022 to conceptually organize the construct of occupational balance. The review focused on English and Japanese publications published within the past 20 years. Searches were performed using databases such as PubMed, OTDBASE, and Google Scholar, with keywords including “occupational balance,” “occupational imbalance,” and related terms. Additionally, manual searches were conducted based on the reference lists of key publications. The studies found were reviewed to explore theories, concepts, and assessment scales in order to operationally define the constructs of occupational balance. Particular attention was given to literature addressing relevant theoretical models, conceptual frameworks, and assessment scales. Given the exploratory nature of the review, strict inclusion or exclusion criteria were not applied. Instead, studies were selected based on their relevance to the conceptual clarification of occupational balance. Final selection and content validity were confirmed through consensus within the research team.
Creation of item pool
The items were collected through a literature review related to the conceptual constructs. Relevant items associated with the conceptual constructs were developed based on the literature regarding theories, concepts, and assessment scales.
Content validity
A consensus-based Delphi method was used to evaluate the content validity of the item pool.
Participants in Phase 1 were selected based on the following inclusion criteria:
(1) having published scholarly work (e.g., academic papers, books, or conference presentations) related to occupational balance or relevant theoretical models;
(2) being a licensed occupational therapist with experience in research, education, or clinical practice; and (3) holding a master’s or doctoral degree. Participants were recruited through purposive expert sampling via professional networks, including academic societies and training seminars. Individuals who did not meet these criteria—such as those without a relevant publication history, without a professional license in occupational therapy, or without an advanced academic degree—were excluded from participation.
The evaluation was performed using the content validity ratio (CVR), with thresholds based on the number of evaluators: 0.99 for 5–6 evaluators, 0.85 for 7–8 evaluators, and 0.62 for 9–10 evaluators (Lawshe, 1975). The survey form was distributed via email, and participants were asked to assess whether the wording and content of each item were appropriate for the corresponding factor. The degree of agreement was rated using a four-point Likert scale: “strongly agree” (four points), “somewhat agree” (three points), “somewhat disagree” (two points), and “strongly disagree” (one point). Based on participants’ ratings and written feedback, the researchers reviewed and revised item content as needed. Items that did not meet the CVR thresholds were excluded from the assessment scale. This Delphi process was conducted over three rounds to ensure consensus.
Phase 2: Development of the OBAS
Phase 2 aimed to examine the validity and reliability of the OBAS for healthcare professionals.
Participants
Participants in the Phase 2 were eligible for inclusion if they met all of the following criteria: (1) being a healthcare professional working in the medical or long-term care insurance sector in Japan; (2) aged 18 years or older; (3) completion of the entire electronically (Google Forms) or in paper format; (4) provision of informed consent to participate in the study; and (5) ability to read and respond in Japanese. Individuals were excluded if they did not meet the inclusion criteria or if their responses were incomplete or considered invalid.
Participants were recruited using convenience sampling through professional networks, including colleagues met at academic societies and training seminars, who then invited healthcare professionals from their affiliated institutions. The sample size was determined to be seven times the number of items, as recommended (Mokkink et al., 2019). The decision to focus on healthcare professionals as participants was based on evidence that approximately 63% of healthcare workers in Japan experience difficulties in maintaining occupational balance (Miyake et al., 2014). Data were collected from July 10 to October 2, 2023, including responses to the prototype OBAS, a demographic information sheet, and criterion-related scales. The collected data were statistically analyzed, including internal consistency assessment and factor analysis.
Survey form
Demographic information sheet
Basic information was collected from the respondents, including gender, age, occupation, and years of experience.
Classification and assessment of occupational dysfunction
The Classification and Assessment of Occupational Dysfunction (CAOD) is a scale for assessing occupational dysfunction (Teraoka and Kyougoku, 2015). It consists of four factors and 16 items, including occupational imbalance (4 items), occupational deprivation (3 items), occupational alienation (3 items), and occupational marginalization (6 items). Items are scored on a 7-point Likert scale ranging from 1 to 7, with 1 indicating “strongly disagree” and 7 indicating “strongly agree.” Based on the cutoff value for healthy individuals, a score of ⩾52 points indicates occupational dysfunction. Validity was a good estimate of the model fit with root mean square error of approximation (RMSEA) = 0.073 and comparative fit index (CFI) = 0.935. Reliability was internal consistency of Cronbach’s α (α = 0.826–0.902) and displayed strong test-retest (r = 0.516–0.678, p < 0.01). These were all verified in healthy adults. It is hypothesized that disruption of occupational balance is associated with the development of occupational dysfunction.
Stress Response Scale
The Stress Response Scale (SRS-18) is a scale for assessing psychological stress responses (Suzuki et al., 2007). It consists of three factors and 18 items, including depression and anxiety (6 items), irritability and anger (6 items), and apathy (6 items). Items are scored on a 4-point Likert scale ranging from 0 to 3, with 0 indicating “not at all true” and 3 indicating “very true.” Higher scores indicate higher stress response levels. The SRS-18 has been developed only in Japanese. Reliability was internal consistency of Cronbach’s α (α = 0.82–0.88) and displayed strong test-retest (r = 0.83–0.91, p < 0.01), verified in healthy adults. It is hypothesized that disruption of occupational balance increases stress responses.
The Japanese Translation of the Brief Self-Control Scale
The Japanese Translation of the Brief Self-Control Scale (BSCS-J) is a scale for assessing self-control (Ozaki et al., 2016). It consists of 13 items. Items are scored on a 5-point Likert scale ranging from 1 to 5, with 1 indicating “strongly disagree” and 5 indicating “strongly agree.” Higher scores indicate greater self-control. Validity was good estimate of the model fit with RMSEA = 0.058 and Goodness of fit index (GFI) = 0.904. Reliability was internal consistency of Cronbach’s α (α = 0.83) and displayed strong test-retest (r = 0.73, p < 0.001). These were all verified in healthy adults. It is hypothesized that disruption of occupational balance is associated with self-control, as individuals may struggle to adjust effectively to their occupations.
Statistical analysis
Statistical analysis was performed using Jamovi Version 2.3.28.0 for demographic information, criterion validity, internal consistency, and hypothesis testing, RStudio version 2023.06.1+524 for item response theory and confirmatory factor analysis (CFA), and Jeffreys's Amazing Statistics Program (JASP) version 0.18.3 for exploratory factor analysis (EFA).
Demographic information
The mean and standard deviation of the participants’ age and years of experience were calculated to understand their characteristics. Frequencies and percentages were determined for gender and occupation. Additionally, the mean, standard deviation, minimum, maximum, skewness, and kurtosis were calculated for the total scores of the prototype OBAS, CAOD, SRS-18, BSCS-J, and OBAS items.
Criterion validity
Spearman’s rank correlation coefficients were calculated for the CAOD, SRS-18, and BSCS-J to investigate the relationship between the factor structures of the prototype OBAS and the related scales. Correlation coefficients were computed between the total score and subfactors of the OBAS and the total score and subfactors of the CAOD, SRS-18, and BSCS-J. The significance level was set at p < 0.05. The correlation coefficients were interpreted as follows: values between 0.1 and <0.4 indicating weak correlation, values between 0.4 and <0.7 indicating moderate correlation, and values of ⩾0.7 indicating strong correlation (Akoglu, 2018). Items showing no correlation or failing to meet the criteria were considered for revision or deletion. At the time of this study, the validity of the Japanese versions of existing occupational balance assessments, such as the OBQ-11, OB-Quest, and SDO-OB, had not yet been verified. Therefore, we adopted the CAOD, which includes aspects related to occupational balance.
Item response theory
The discrimination and difficulty level of all items in the prototype OBAS were calculated to examine the validity of each item. Discrimination is an index of item acuity, with a criterion value of 0.2–2.0 (Noguchi and Kyougoku 2021). Difficulty is an index of item difficulty, with an absolute value of <4.0 as the criterion (Noguchi and Kyougoku 2021). The discrimination was divided by 1.702 during statistical processing (Camilli, 1994). The estimation method was the maximum likelihood estimation method. Items not meeting the discriminative power and difficulty criteria were considered for revision or deletion.
Exploratory factor analysis
A categorical EFA was performed to check whether the factors assumed in the constructs of the scale were extracted. Items with similar factor loadings for multiple factors were considered for deletion. The estimation method was the robust weighted least squares method, and the rotation method was the geomin rotation. Items were repeatedly revised or deleted while analyzing changes in factor loadings.
Confirmatory factor analysis
A categorical CFA was performed to examine the structural validity of each factor structure. The CFI, Tucker–Lewis Index (TLI), standardized root mean square residual (SRMR), RMSEA, and χ2 values were used. The cutoff values of CFI ⩾ 0.90, TLI ⩾ 0.90, SRMR ⩽ 0.05, RMSEA ⩽ 0.05 (best), 0.08 (good), and 0.10 (acceptable), and Chi-square p-value ⩽ 0.05 were adopted (Nam et al., 2024). The estimation method was the robust weighted least squares method. Items not meeting the criteria for the goodness-of-fit indices were considered for revision or deletion.
Internal consistency
Good reference values for the α and ω coefficients were set at ⩾0.80 (Čunek et al., 2023).
Hypothesis testing for construct validity
Three hypotheses were tested for the total item scores and criterion-related scales employed in the OBAS: (1) Since CAOD reflects aspects of occupational balance, there was a moderate positive correlation between OBAS and CAOD; (2) As occupational balance disruption increases stress levels, OBAS and SRS-18 had a moderate to weak positive correlation; (3) Because disruption of occupational balance can lead to difficulties in adjustment and is associated with self-control, there was a moderate negative correlation between OBAS and BSCS-J. The significance level was set at p < 0.05.
Results
Phase 1: Development of the prototype OBAS
Literature review for developing operational definitions of constructs
These definitions were derived by the authors based on the review conducted in the “Literature Review for Developing Operational Definitions of Constructs—Methods” section. The prototype constructs comprised six constructs: “Time,” “Taxonomy,” “Quantity,” “Resources,” “Meaning,” and “Adjustment.” Time has been discussed in previous studies as reflecting the balance of time use across different periods, such as a day or a week (Matuska and Christiansen, 2008; Meyer, 1922; Yamane and Yoshikawa, 2022). Based on this conceptualization, in the present study, time is defined as the duration allocated to each occupation. Taxonomy captures the multifaceted nature of occupations, which are not limited to a small number of fixed categories and may include activities that individuals want to do, have to do, or feel obligated to do (Eklund et al., 2017; Matuska and Christiansen, 2008; Yamane and Yoshikawa, 2022). Accordingly, taxonomy is defined as the personal and general categories of each occupation. Quantity is based on the notion that there is an appropriate overall amount of occupations, as having too many or too few occupations may affect occupational balance (Eklund et al., 2017; Yamane and Yoshikawa, 2022). Therefore, quantity is defined as the total number of occupations. Resources reflect the various factors that influence engagement in occupations, including individual abilities, characteristics of the occupation, and environmental conditions (Anaby et al., 2010; Eklund et al., 2017; Fisher and Marterella, 2019). In this study, resources are defined as the power sources required for each occupation. Meaning emphasizes the importance of alignment between an individual’s values and the purpose of occupations, as well as the sense of satisfaction derived from engagement (Eklund et al., 2017; Wagman et al., 2012; Yamane and Yoshikawa, 2022). Thus, meaning is defined as the significance, purpose, or value associated with each occupation. Adjustment is grounded in the understanding that occupational balance is dynamic and that maintaining or improving balance requires the coordination and regulation of multiple occupations (Backman, 2013; Barbara et al., 2023; Yazdani et al., 2018). Accordingly, adjustment is defined as the management and coordination of various occupations. In this study, “occupational balance is defined as a state in which multiple occupational performances, experiences, and engagement are harmonized (複数の作業遂行や経験,結びつきが調和している状態).” This definition was established by consensus between the researchers based on a review of the literature. The literature review related to the conceptual constructs resulted in the creation of 42 items. The sources included research and frameworks from occupational science, occupation-based practice 2.0 (Teraoka and Kyougoku, 2014), the Model of Human Occupation (Taylor and Yamada, 2019), the Canadian Model of Occupational Performance and Engagement (Townsend et al., 2011), the Transactional Model of Occupation (Fisher and Marterella, 2019), the Occupational Therapy Practice Framework (American Occupational Therapy Association, 2020), and Occupational Orchestration (Barbara et al., 2023).
Content validity
Valid responses were obtained from five of six occupational therapists for content validity. The respondents included two university faculty members and three clinicians. Their educational backgrounds consisted of two doctoral graduates and three master’s graduates. Additionally, four of the respondents had experience in scale development research and were well-versed in the methods. Based on the comments provided, revisions were discussed among the researchers and were conducted iteratively three times until no further disagreements arose. Consequently, the prototype OBAS, consisting of six constructs and 38 items meeting the CVR threshold, was developed. The results of the content validity analysis can be found in the supplementary materials.
Phase 2: Development of the OBAS
Demographic information
A total of 318 valid responses were obtained from 320 participants. The mean age of the participants was 33.3 (±10.6) years, and the mean years of experience was 8.67 (±7.50) years. Approximately 80% of the participants were rehabilitation professionals. Table 1 shows the results of the other basic attributes, criterion-related scales, and the descriptive analysis of the OBAS.
Demographic information (n = 318).
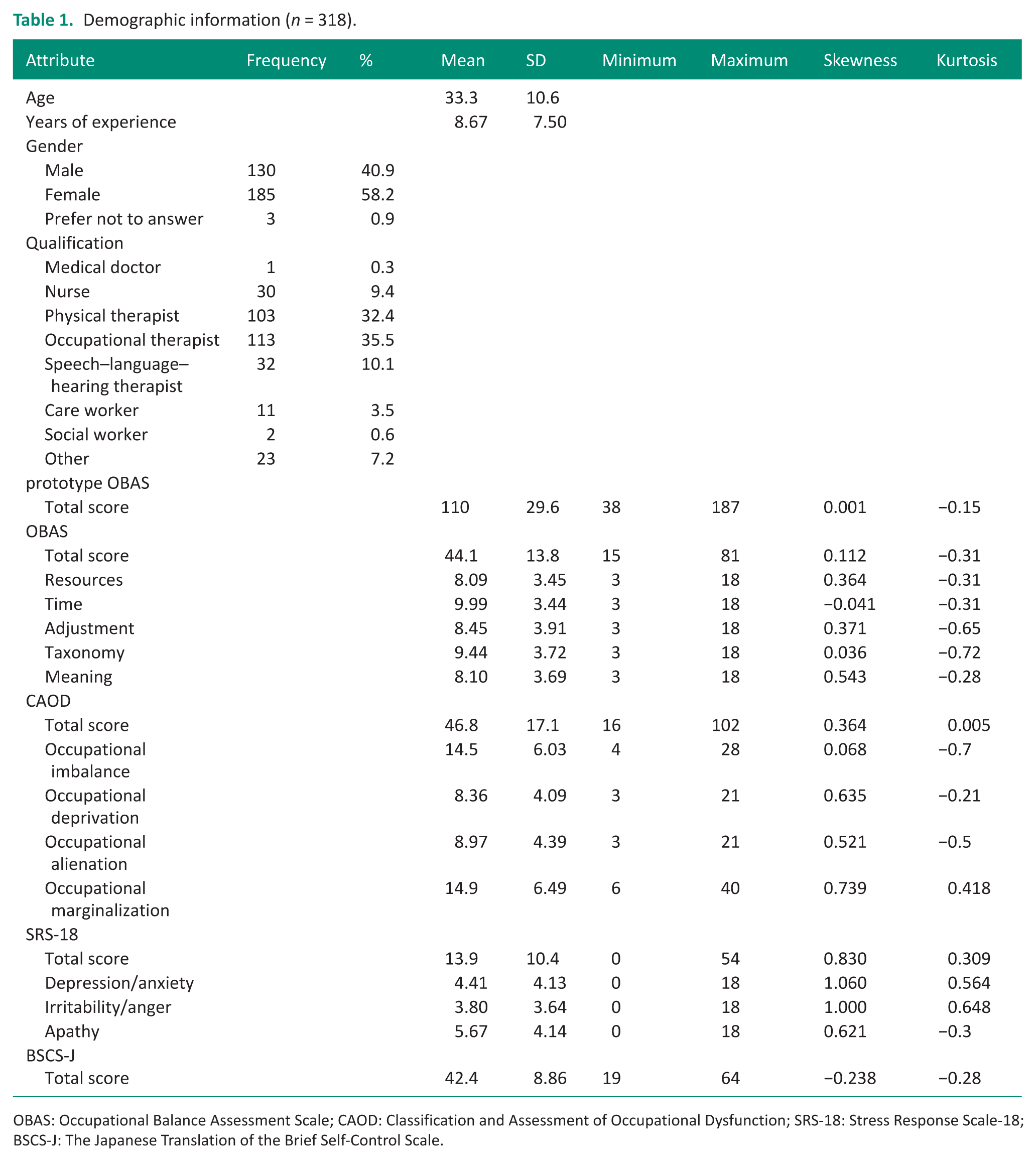
OBAS: Occupational Balance Assessment Scale; CAOD: Classification and Assessment of Occupational Dysfunction; SRS-18: Stress Response Scale-18; BSCS-J: The Japanese Translation of the Brief Self-Control Scale.
Reduction of OBAS items
Statistical analysis was performed to refine the 38 items in the prototype OBAS. Item numbers 1–6 and 8 were deleted as they did not meet the threshold values for discrimination and difficulty in the item response theory. Additionally, Item numbers 1–6 demonstrated no correlation with the related scales CAOD, SRS-18, and BSCS-J, which were hypothesized to be associated with occupational balance (Table 2). The factor “Quantity” was left with only Item number 7, making it unviable as a factor. The remaining items were subjected to repeated EFA, and items that did not align with the intended factors were deleted (Table 3). Ultimately, 23 items from the prototype were removed, resulting in a final OBAS with 15 items. The final OBAS version of the scale can be accessed in the Supplemental Materials.
Reduction of OBAS items.
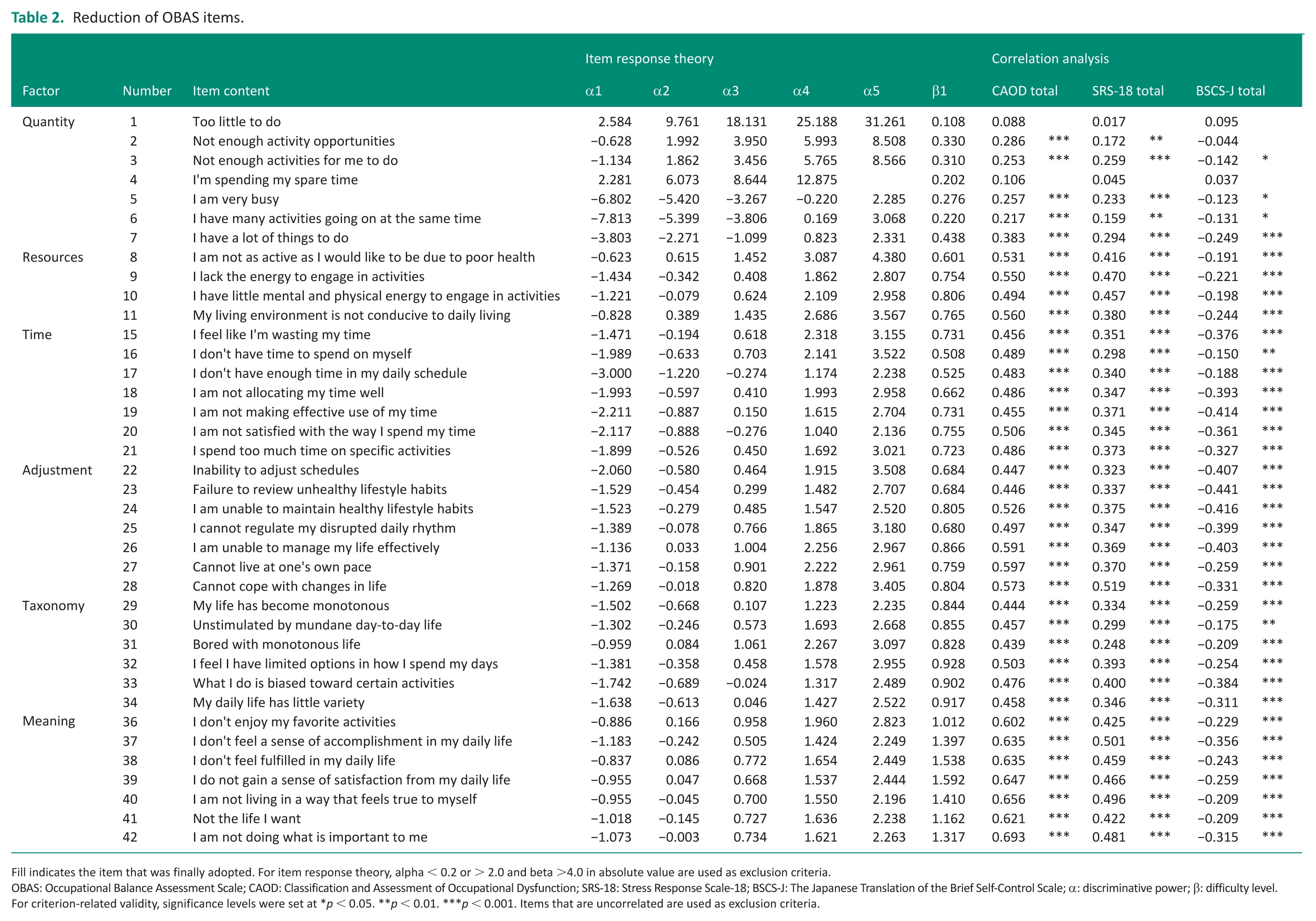
Fill indicates the item that was finally adopted. For item response theory, alpha < 0.2 or > 2.0 and beta >4.0 in absolute value are used as exclusion criteria.
OBAS: Occupational Balance Assessment Scale; CAOD: Classification and Assessment of Occupational Dysfunction; SRS-18: Stress Response Scale-18; BSCS-J: The Japanese Translation of the Brief Self-Control Scale; α: discriminative power; β: difficulty level.
For criterion-related validity, significance levels were set at *p < 0.05. **p < 0.01. ***p < 0.001. Items that are uncorrelated are used as exclusion criteria.
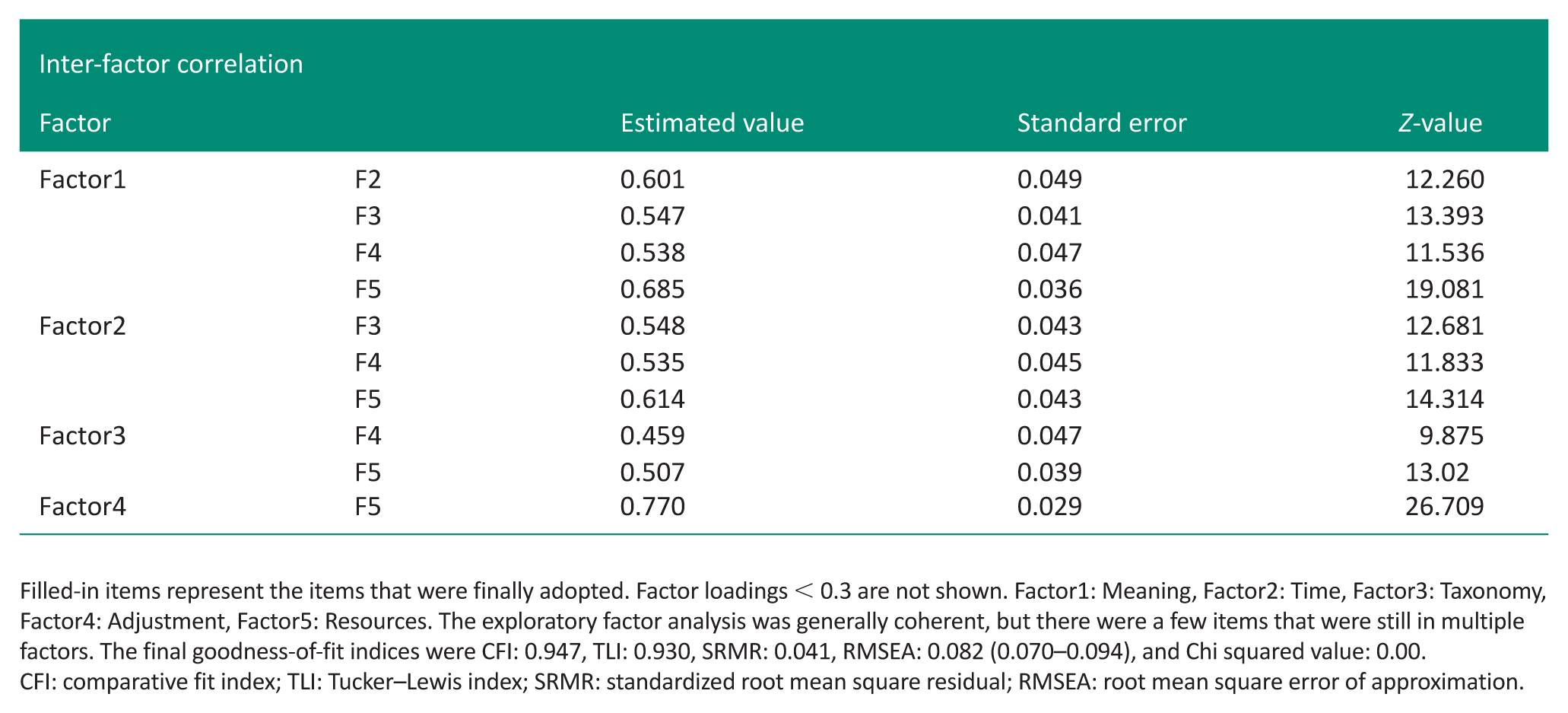
Exploratory factor analysis and confirmatory factor analysis.
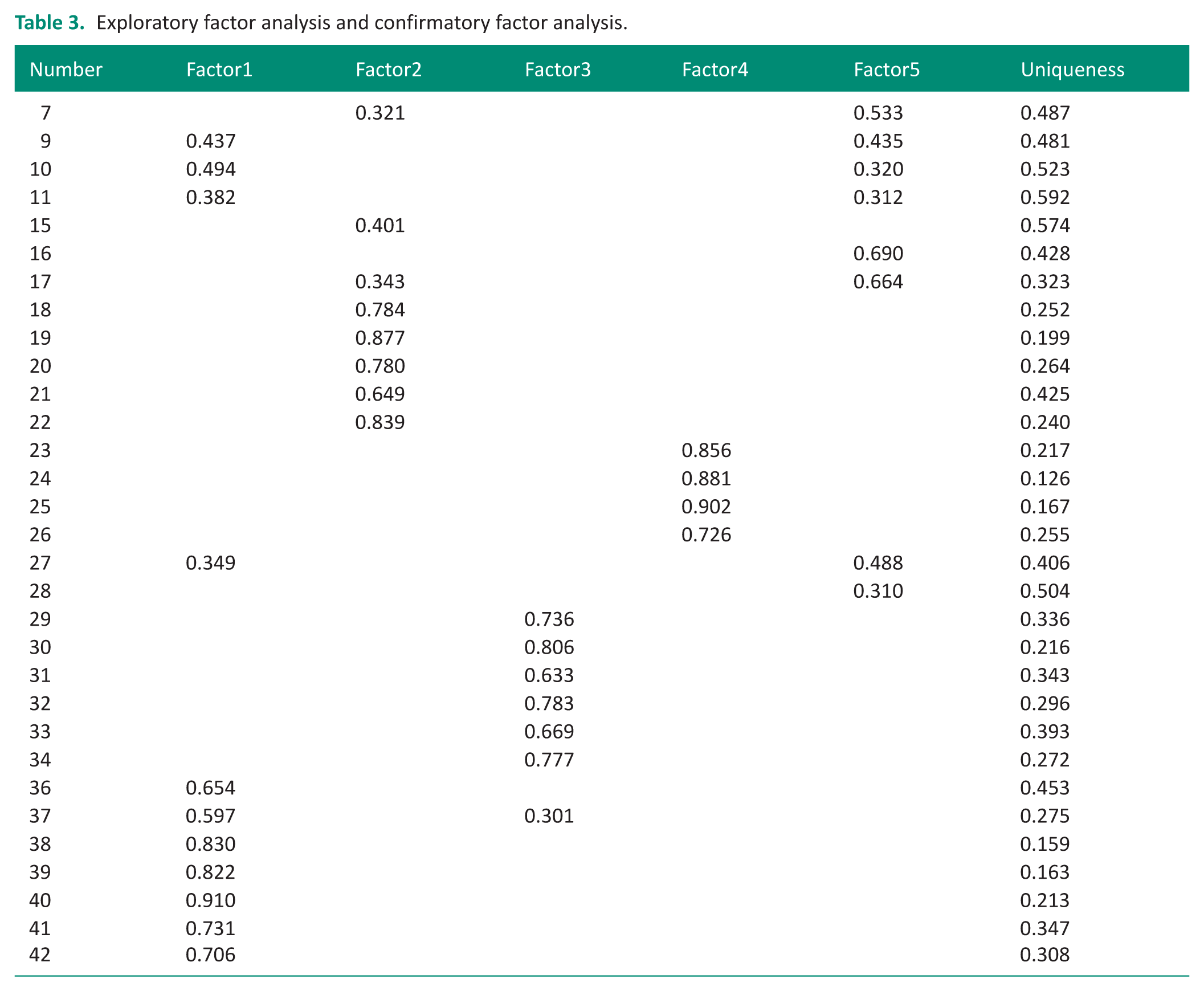
Filled-in items represent the items that were finally adopted. Factor loadings < 0.3 are not shown. Factor1: Meaning, Factor2: Time, Factor3: Taxonomy, Factor4: Adjustment, Factor5: Resources. The exploratory factor analysis was generally coherent, but there were a few items that were still in multiple factors. The final goodness-of-fit indices were CFI: 0.947, TLI: 0.930, SRMR: 0.041, RMSEA: 0.082 (0.070–0.094), and Chi squared value: 0.00.
CFI: comparative fit index; TLI: Tucker–Lewis index; SRMR: standardized root mean square residual; RMSEA: root mean square error of approximation.
Reliability and validity of the OBAS
For the reliability of the OBAS, item response theory was the discrimination values of each item ranged from 0.525 to 1.592, and the difficulty values ranged from −3.00 to 3.567 (Table 2), which fell within the acceptable thresholds. The difficulty values covered a wide range, indicating that the OBAS included a mix of easy and difficult items. The internal consistency of the OBAS was demonstrated by Cronbach’s α (α = 0.903) and McDonald’s ω (ω = 0.905), both exceeding the acceptable threshold (0.80). When each item was individually deleted, Cronbach’s α was 0.892–0.903, and McDonald’s ω was 0.894–0.904. These results indicated that item deletion did not improve reliability.
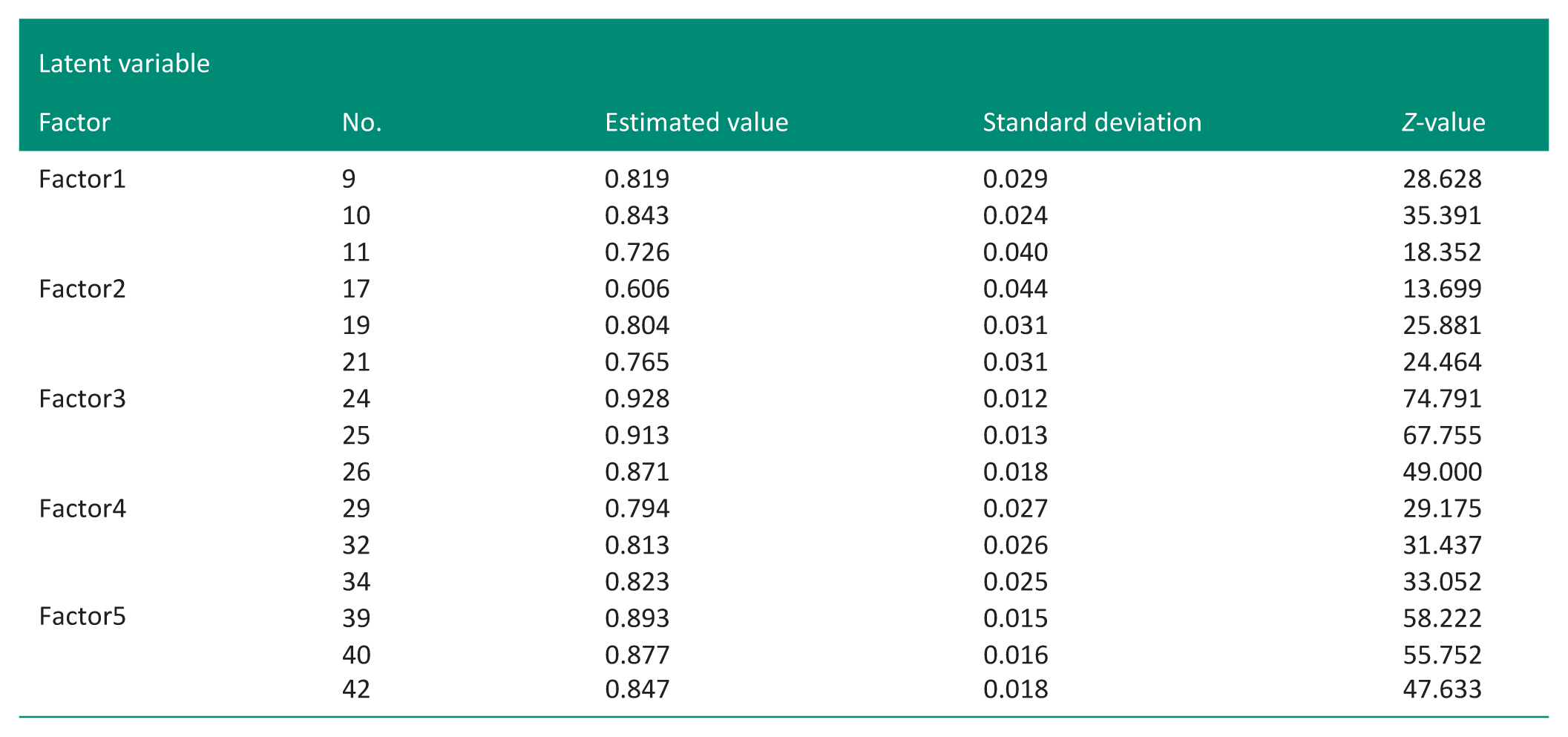
For validity, the CFA fit indices were as follows: CFI = 0.947, TLI = 0.930, SRMR = 0.041, RMSEA = 0.082 (95% CI: 0.070–0.094), and Chi-square = 0.00 (Table 3). The final structure included five factors, namely, “Resources,” “Time,” “Adjustment,” “Taxonomy,” and “Meaning,” with three items each, resulting in 15 items meeting the required standards. The three hypotheses were supported. A strong positive correlation was observed between the OBAS and CAOD (r = 0.81), a moderate positive correlation between the OBAS and SRS-18 (r = 0.610), and a moderate negative correlation between the OBAS and BSCS-J (r = −0.471; Table 4).
Hypothesis testing of construct validity.
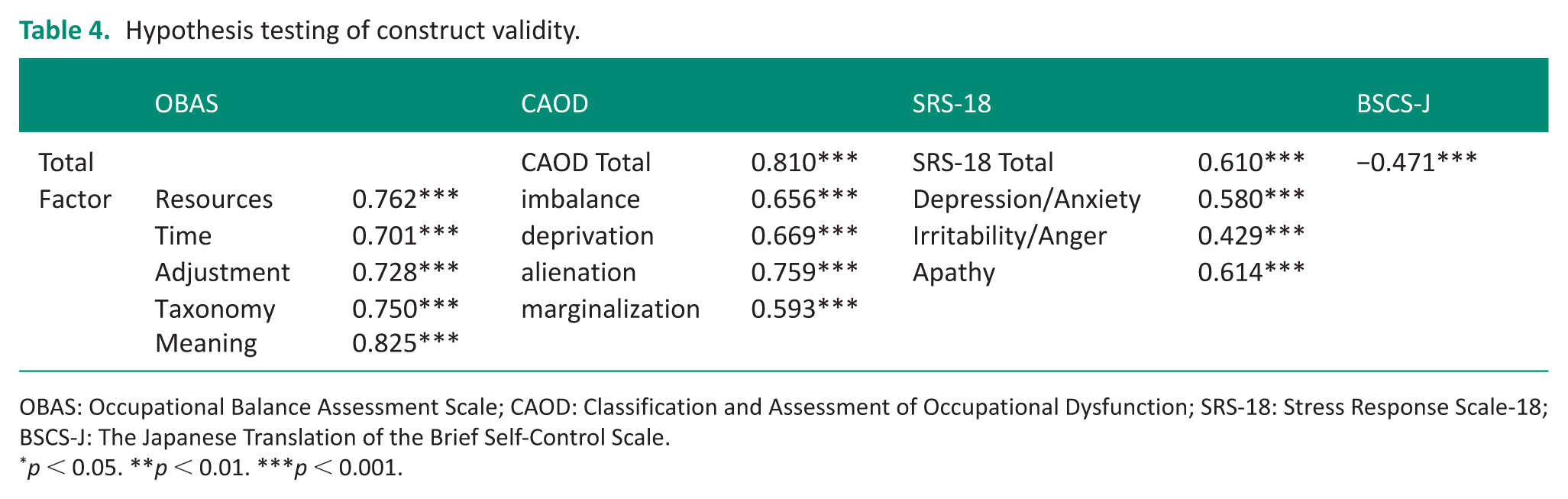
OBAS: Occupational Balance Assessment Scale; CAOD: Classification and Assessment of Occupational Dysfunction; SRS-18: Stress Response Scale-18; BSCS-J: The Japanese Translation of the Brief Self-Control Scale.
p < 0.05. **p < 0.01. ***p < 0.001.
Scoring of the OBAS
The total OBAS score was calculated by summing the raw scores of all 15 items. As each item was rated on a 6-point Likert scale, the minimum possible total score was 15, and the maximum possible total score was 90. Each of the five factors comprised three items, resulting in a minimum possible factor score of 3 and a maximum possible factor score of 18. Higher total and factor scores indicate greater occupational imbalance. All items were scored in the same direction, and no reverse-coded items were included. Factor scores were calculated by summing the raw scores of the corresponding items. No cut-off scores or normative values were established in this study.
Discussion
This study was conducted to develop the OBAS for healthcare professionals. The OBAS is an assessment scale designed to focus on the adjustment of occupational balance and analyze multiple factors. In Phase 1, the conceptual constructs and item pool were established, and the prototype OBAS was developed. Content validation was also carried out using the Delphi method by occupational therapists. In Phase 2, a survey was conducted among healthcare professionals. Statistical analyses were performed to refine the items: Item response theory (IRT), EFA, CFA, internal consistency, and hypothesis testing for construct validity. Finally, a reliable and valid OBAS comprising five factors and 15 items was developed. The five factors were: “Resources,” “Time,” “Adjustment,” “Taxonomy,” and “Meaning.” The OBAS is a valuable tool for developing support strategies to adjust occupational balance among healthcare professionals.
Content validity
The content validity demonstrated in Phase 1 was satisfactory. This was supported by the rigorous content validity evaluation process employed in this phase. Content validity assessment was conducted over three rounds, during which items that did not meet the predefined criteria were revised to improve clarity and relevance, resulting in the construction of the 38-item prototype. Consequently, in Phase 1, all 38 items of the prototype OBAS met the CVR threshold (>0.99) for content validity. Given that the prototype initially included a number of items several times greater than the final version, this was considered an appropriate item pool size. The evaluation involved appropriately qualified occupational therapists who possessed extensive knowledge of occupational balance.
Demographic information
In Step 2, a total of 318 valid responses were obtained from 320 participants. The mean age of the participants was 33.3 (±10.6) years, and their mean years of experience was 8.67 (±7.50). Approximately 80% of the participants were rehabilitation professionals. This may reflect the researchers’ area of expertise, as the collaborating institutions were selected using purposive sampling. Consequently, the findings of this study may primarily reflect perspectives common among rehabilitation professionals. Increasing the diversity of professions among participants should therefore be considered in future research.
Criterion validity
Regarding criterion validity, the OBAS showed significant correlations with all of the comparison scales. In particular, its correlation with the CAOD, which includes aspects of occupational balance, demonstrated that the OBAS is related to occupational balance. At the time of this study, the validity of existing Japanese versions of occupational balance measures—such as the OBQ-11, OB-Quest, and SDO-OB—had not yet been examined, and therefore these instruments could not be used for criterion validation in the present study. However, future studies should assess the criterion validity of the OBAS using these internationally utilized occupational balance–related instruments once their Japanese versions become available.
Item response theory
In the item response theory analysis of the OBAS, the discrimination parameters ranged from .525 to 1.592, and the difficulty parameters ranged from −3.00 to 3.567, all of which fell within acceptable ranges. Previous research has reported discrimination values of 1.091 to 1.307 and difficulty values of −1.935 to 1.533 for items of the CAOD that include aspects of occupational balance (Teraoka and Kyougoku, 2015). This suggests that the OBAS encompasses a broader range of discrimination and difficulty parameters than the CAOD, indicating that it includes both easier and more difficult items. The wide distribution of difficulty values further suggests that the OBAS comprises a mix of items varying in difficulty.
Exploratory factor analysis
The EFA revealed that the factor loadings for “Quantity” overlapped with those of “Resources” and “Time.” Based on previous studies, the “Quantity” factor includes elements of time and count (Yamane and Yoshikawa, 2022). This overlap may be interpreted in light of how quantity is perceived within the concept of occupational balance. In this context, quantity does not simply refer to the number of occupations, but rather to the extent to which occupations fit within available time. Furthermore, the appropriateness of quantity is often evaluated in relation to limited resources, suggesting that quantity is inherently multidimensional. As a result, the “Quantity” factor may not function as an independent construct and was ultimately integrated into the “Time” and “Resources” factors.
Confirmatory factor analysis
The CFA demonstrated acceptable fit indices, with CFI = 0.947, TLI = 0.930, SRMR = 0.041, and RMSEA = 0.082 (95% CI: 0.070–0.094), indicating an acceptable fit of the hypothesized factor model. Although the RMSEA value was slightly above the conventional threshold for good fit, the other fit indices indicated a satisfactory model fit. In addition, all items showed adequate standardized factor loadings on their respective factors, supporting the validity of the proposed factor structure. These results suggest that each factor was appropriately represented by its corresponding items and contributed meaningfully to the measurement of occupational balance. The factor intercorrelations did not include any strong correlations (r ⩾ 0.80), suggesting that the factors are relatively distinct from one another. The identification of “Adjustment” as an independent factor suggests that occupational balance, conceptualized as harmony, is not merely a function of time or resource allocation but reflects a dynamic process of self-management in response to changing contextual demands. Thus, the OBAS enables a multifaceted analysis of occupational balance across five aspects, including “Adjustment.” This represents the first scale structure that is not available in existing occupational balance measures (Dür et al., 2014; Eklund and Argentzell, 2016; Håkansson et al., 2020; Yamane and Yoshikawa, 2022; Wagman and Håkansson, 2014).
Internal consistency
The reliability of the OBAS was satisfactory. The internal consistency of the OBAS was demonstrated by a Cronbach’s α coefficient of 0.903 and a McDonald’s ω coefficient of 0.905. These values indicate superior reliability compared with the α coefficient of 0.80 reported for the OB-Quest (Ho et al., 2020) and are comparable to the α coefficient of 0.936 reported for the OBQ (Wagman and Håkansson, 2014), which exceeds 0.90 and is considered excellent (Dür et al., 2014). Therefore, the OBAS with 15 items developed in this study consistently measures occupational balance.
Hypothesis testing for construct validity
Construct validity was confirmed as hypothesized (CAOD: r = 0.810, SRS-18: r = 0.610, BSCS-J: r = −0.471). These findings indicate that OBAS scores were positively correlated with CAOD and SRS-18 scores and negatively correlated with BSCS-J scores. Therefore, the OBAS developed in this study demonstrated a scale structure capable of analyzing multiple factors and showed satisfactory validity and reliability.
Interpretation of the OBAS
To facilitate the practical interpretation and application of the OBAS, the following explanation is provided. The OBAS assesses occupational balance across five factors—“Resources,” “Time,” “Adjustment,” “Taxonomy,” and “Meaning”—and is intended to support reflective discussions and decision-making in applied settings, such as health management and individualized support planning. Existing measures of occupational balance are primarily based on a single-factor structure and focus on capturing overall occupational balance (Dür et al., 2014; Eklund and Argentzell, 2016; Håkansson et al., 2020; Wagman and Håkansson, 2014). In contrast, the OBAS focuses on multiple aspects of occupational balance and has the advantage of clearly indicating which aspects of occupational balance are problematic by distinguishing five interacting aspects. For example, if the total OBAS score is high and the “Time” score is also high, it can be interpreted that an imbalance in occupational balance arises from disproportionate time allocation across different occupations. After time-use interventions, if the total OBAS score decreases, the OBAS can be used to evaluate the effectiveness of the intervention. Even when the total OBAS score is low, the factor-level results can provide insights for potential intervention targets. For instance, a relatively high “Adjustment” score may indicate difficulties in managing and coordinating various occupations, suggesting the need for some form of support. Thus, the OBAS can assist in identifying individualized intervention strategies. However, the current interpretation of OBAS scores is limited to comparisons based on raw scores, and further investigation into numerical interpretation will be necessary.
Limitations
This study has some limitations. First, approximately 80% of the participants were rehabilitation professionals, and the study did not fully reflect the characteristics of all healthcare professionals. Therefore, this may introduce a sampling bias and limit the transferability of the results to other health professionals. Future studies should include a diverse set of professionals. Second, the SRS-18 used in this validation study is only available in Japanese, which limits its applicability of OBAS in international contexts. In addition, the appendix OBAS was translated by the authors. Therefore, cross-cultural validation will be necessary for future use of OBAS in research. Third, the OBAS was developed specifically for healthcare professionals. Although all participants were recruited as healthcare workers, we did not inquire about the presence of disabilities during recruitment. Therefore, it cannot be ruled out that some participants may have had disabilities. Future studies should examine the psychometric properties of the OBAS, including its applicability across broader and more diverse populations. Finally, further investigation is needed to establish numerical standards for interpreting OBAS scores.
Conclusion
The OBAS is the first occupational balance assessment to include an “adjustment” factor developed for healthcare professionals. Multiple factors within the five factors, 15 items OBAS, were analyzed, a valid and reliable tool for identifying occupational balance among healthcare professionals. Future studies are needed to examine further psychometric properties, including cross-cultural validity.
Key findings
The Occupational Balance Assessment Scale (OBAS) provides indicator for analyzing occupational balance of healthcare professionals.
The OBAS enables the analysis of occupational balance through five factors: “Resources,” “Time,” “Adjustment,” “Taxonomy,” and “Meaning.”
What the study has added
This study provides initial evidence for the reliability and validity of the scale that can be used to analyze the occupational balance of healthcare professionals from multiple factors.
Supplemental Material
sj-docx-2-bjo-10.1177_03080226261454903 – Supplemental material for Development and validation of the occupational balance assessment scale for healthcare professionals
Supplemental material, sj-docx-2-bjo-10.1177_03080226261454903 for Development and validation of the occupational balance assessment scale for healthcare professionals by Shinya Onda, Mutsumi Teraoka and Makoto Kyougoku in British Journal of Occupational Therapy
Supplemental Material
sj-xlsx-1-bjo-10.1177_03080226261454903 – Supplemental material for Development and validation of the occupational balance assessment scale for healthcare professionals
Supplemental material, sj-xlsx-1-bjo-10.1177_03080226261454903 for Development and validation of the occupational balance assessment scale for healthcare professionals by Shinya Onda, Mutsumi Teraoka and Makoto Kyougoku in British Journal of Occupational Therapy
Footnotes
Acknowledgements
The authors would like to express their deepest gratitude to the subjects who cooperated in data collection and to all research collaborators.
Ethical considerations
This study was approved by the Ethics Review Board of Kibi International University (Approval Number: 22-33). Recognition Day (December 21, 2022). Study period: December 21, 2022 to March 31, 2024.
Consent to participate
Approval for data collection was obtained from the representatives of each participating facility. Participants were healthcare professionals working in the medical insurance or long-term care insurance fields who provided consent to participate in the study. Instruments were distributed electronically (Google Forms) or in paper format, and providing responses was considered consent to participate.
Author contributions
SO researched literature and conceived the study. MT and MK were involved in gaining ethical approval and data analysis. SO wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Funding
The authors declared no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Patient and public involvement data
During the development, progress, and reporting of the submitted research, Patient and Public Involvement in the research was: a.Included at all stages of the research.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.