
Abstract
Introduction:
Romantic relationships represent a meaningful domain of occupational participation. Although individuals with serious mental illness (SMI) commonly desire romantic relationships, stigma, sexual dysfunction, economic constraints, and limited social participation may hinder engagement. Quantitative studies integrating these factors remain scarce. This study aimed to clarify how community-living individuals with SMI in Japan perceive the skills, resources, and attitudes required to establish and maintain romantic relationships and to examine their associations with related factors.
Method:
Thirty-nine adults with SMI attending psychiatric day-care services completed a cross-sectional survey including the Romantic Relationship Functioning Scale (RRFS), Perceived Devaluation-Discrimination Scale, Nagoya Sexual Functional Questionnaire, Recovery Assessment Scale, and Temple University Community Participation Measure (Japanese version). Correlation analyses were conducted using RRFS scores as the primary outcome.
Results:
Participants reported comparatively lower perceived interpersonal skills and resources related to romantic relationship functioning. Recovery was the only factor significantly associated with romantic relationship functioning (r = 0.571, p < 0.01).
Conclusion:
Romantic relationship functioning appears to represent a distinct domain of occupational participation requiring explicit consideration within occupational therapy assessment and intervention. These findings provide preliminary quantitative evidence regarding relational skills and resources among individuals with SMI in Japan.
Introduction
Romantic relationships among individuals with mental illness
Romantic relationships have increasingly been recognized as an important aspect of recovery and social participation among individuals with mental illness. Romantic and intimate relationships are commonly desired among individuals with mental illness (Budziszewska et al., 2020; Forrester-Jones et al., 2023; Stein et al., 2024; Volman and Landeen, 2007). Although many individuals with mental illness desire romantic relationships, support for romantic relationships among them is limited. Moreover, a multinational study conducted across 19 countries indicated that having a mental illness is associated with a lower likelihood of marriage and a higher likelihood of divorce (Breslau et al., 2011).
Findings regarding relationships and mental illness have been mixed. Several studies have reported beneficial effects of romantic relationships for individuals with mental illness. For instance, one systematic review found that having a romantic partner was associated with reduced positive and negative symptoms over time (White et al., 2021). A narrative review study on individuals with serious mental illness (SMI) reported that married individuals showed higher quality of life and better social functioning (Lyngdoh et al., 2023).
Conversely, other studies have identified potential adverse effects of romantic relationships on individuals with mental illness. Lyngdoh et al. (2023) noted that relapse was more frequent among married individuals with SMI compared to their unmarried counterparts, although only a few studies have examined this association. The same authors also reported that many individuals with SMI demonstrated poor adherence to medication or discontinued medication after marriage, possibly due to negative symptoms and impaired functioning (Lyngdoh et al., 2023). Azorin et al. (2021) highlighted the burdens experienced by partners of individuals with bipolar disorder, including self-sacrifice, caregiver strain, emotional distress, and health problems.
Moreover, these individuals may encounter difficulties in building and maintaining romantic relationships (Budziszewska et al., 2020; Elkington et al., 2013; Forrester-Jones et al., 2023; Redmond et al., 2010; Stein et al., 2024; Volman and Landeen, 2007). Such difficulties arise from a variety of factors, including low economic status (Budziszewska et al., 2020), stigma (Budziszewska et al., 2020; Elkington et al., 2013; Forrester-Jones et al., 2023; Stein et al., 2024; Volman and Landeen, 2007), sexual dysfunction (Volman and Landeen, 2007), psychiatric symptoms (Budziszewska et al., 2020; Forrester-Jones et al., 2023; Stein et al., 2024), low self-esteem (Forrester-Jones et al., 2023; Stein et al., 2024), and limited social participation (Budziszewska et al., 2020; Forrester-Jones et al., 2023; Volman and Landeen, 2007).
Romantic relationships as occupation
Romantic relationships represent a significant domain of human occupation across the lifespan. Growing literature has begun to recognize romantic relationships as a meaningful form of occupation. Bertrand et al. (2025) highlighted the importance of co-occupation in romantic partnerships. Co-occupation within these relationships involves sharing meaning, time, and space, supporting one’s partner through individual tasks, and adapting occupations in response to changes in a partner’s health. McCarthy and Jackson (2022) reported that dating was perceived as a crucial activity in seeking a partner, and contributed to greater resilience and self-confidence. Walker et al. (2020) emphasized the expertise of occupational therapists in assessing everyday occupations that facilitate intimate activities, including dressing, hugging, kissing, petting, and sexual intercourse.
From the perspective of the Person–Environment–Occupation–Performance (PEOP) model, a core theoretical framework in occupational therapy, they can be understood not as a single act but as a complex occupation composed of multiple activities, including intimate communication, physical contact, and emotional interaction. The performance of these occupations emerges from the dynamic interaction between personal factors, such as interpersonal skills and self-understanding, and environmental factors, including non-discriminatory social attitudes and cultural norms that enable relationship formation.
Particularly for individuals with mental health conditions, participation in romantic relationships may be especially vulnerable to social exclusion and stigma, potentially constraining opportunities for occupational participation itself. Furthermore, engagement in romantic relationships represents an important experience that contributes to the expression of one’s identity and the development of self-concept. Therefore, like other occupations, romantic relationships hold multifaceted meanings and provide occupational therapists with an essential perspective for understanding the client’s life. Additionally, occupational therapists are uniquely positioned to promote romantic relationships because they address participation in meaningful life situations.
Current challenges and research gaps
As noted above, individuals with mental illness can face difficulties forming and maintaining romantic relationships, underscoring a need for appropriate support. However, in previous research, the factors that influence romantic relationships are diverse and interrelated. To advance understanding and improve support for individuals with mental illness, these factors must be examined in an integrated manner. Additionally, a systematic review on support for intimate relationships among individuals with schizophrenia, bipolar disorder, and depression revealed a narrow research focus, with most studies targeting only those with depression or already in relationships (Caiada et al., 2024).
Furthermore, much of the existing research has been conducted primarily in Western countries, raising the possibility that cultural diversity in romantic relationships has not been sufficiently reflected. Therefore, examining the realities of romantic relationships within diverse cultural contexts, including those in Asian societies, is warranted. In this field, qualitative studies, particularly interview-based research focusing on personal experiences, have accumulated considerably. Such approaches are valuable for understanding the highly personal and subjective nature of romantic relationships. However, studies that systematically examine the associations between the factors identified through qualitative research and romantic relationships remain limited. Accordingly, there is a need for quantitative investigations to clarify the relationships among these factors.
Despite growing interest in romantic relationships among individuals with mental illness, limited research has examined these relationships through an occupational lens. Examining these issues from an occupational perspective may provide important insights for occupational therapy practice.
In response to these gaps, the aims of the present study were
1. To clarify how community-living individuals with SMI in Japan perceive the skills, resources, and attitudes required to establish and maintain romantic relationships; and
2. To quantitatively examine the associations between these skills, resources, and attitudes and the factors influencing romantic relationships among community-living individuals with SMI in Japan.
This study aimed to contribute to a deeper understanding of the challenges and underlying factors involved in forming and maintaining romantic relationships among individuals with mental illness. By elucidating these aspects, a foundational basis will be provided for developing future support strategies and evidence-based interventions aimed at promoting healthy and fulfilling romantic relationships within this population. Given that Japan has one of the largest occupational therapy workforces in the world, with approximately 20% practicing in the mental health field, examining the Japanese context is important for generating clinical implications and may also contribute to the expansion of international knowledge.
Method
Design
The present study employed a cross-sectional design to examine correlations between skills, resources, and attitudes related to romantic relationships and factors influencing these relationships.
Participants
The inclusion criteria for participants were as follows: (a) having an SMI; (b) attending a psychiatric day-care service; (c) age 20–59 years; (d) living in the community; and (e) having the ability to understand the study and provide informed consent.
Participants were recruited exclusively from psychiatric day-care services, as these facilities play a central role in the delivery of community-based mental health care in Japan. Psychiatric day-care services represent a structured, facility-based form of psychiatric rehabilitation designed to support community-living among individuals with mental illness. Programs typically include therapeutic group activities, stress-management and daily living skills training, creative and recreational activities, and vocational support. The staff are multidisciplinary, typically comprising psychiatrists, nurses, mental health social workers, clinical psychologists, and occupational therapists.
The exclusion criteria were as follows: (a) individuals with love delusion as deemed by physicians or healthcare providers; (b) individuals who had been hospitalized within the past year; (c) individuals without a psychiatric diagnosis; or (d) individuals who did not identify as cisgender. Participants were limited to cisgender individuals to ensure consistency between anatomical sex (i.e., internal and external genitalia) and gender identity when assessing sexual functioning.
All participants provided written informed consent before participation.
Data collection
Participants were recruited through purposive sampling as users of either of two psychiatric day-care services (Service Institution A or B). After 3 months of data collection at Service Institution A, the sample size remained limited. Data collection was therefore extended to Service Institution B. Participants at Service Institution B received a 500-yen gift card upon completing the questionnaire.
Data collection was between November 25, 2024, and March 10, 2025. Participants answered self-administered online surveys via Microsoft Forms and paper-based questionnaires.
Each participant completed anonymous, self-administered questionnaires. In addition to the assessment measures, we collected demographic variables, including age, sex, sexual orientation, current and past romantic partnership status, highest educational level, employment status, living situation, and the amount of money available for personal use per month (“monthly budget for personal use”). Attending physicians or healthcare providers assessed participant functioning using the global assessment of functioning (GAF). We also extracted medical information from the clinical records, including psychiatric diagnosis, illness duration, number of hospitalizations, and prescribed medications.
Measures
To meet the aims of the present study, the first author (T.I.) and five occupational therapy researchers categorized the factors related to difficulties in romantic relationships identified from qualitative studies involving individuals with mental illness (Budziszewska et al., 2020; Elkington et al., 2013; Forrester-Jones et al., 2023; Redmond et al., 2010; Stein et al., 2024; Volman and Landeen, 2007). Six factors were initially identified: economic status; self-stigma; sexual dysfunction; recovery; social participation; and psychiatric symptoms. However, psychiatric symptoms were not assessed to minimize participant’s burden. As a result, five factors were examined in the present study.
These measures were selected to capture key domains relevant to occupational participation and romantic relationship functioning among individuals with mental illness.
The Romantic Relationship Functioning Scale
The Romantic Relationship Functioning Scale (RRFS) measures the skills, resources, and attitudes toward romantic relationships (romantic relationship functioning) for individuals with mental illness (domain: romantic relationship functioning) (Bonfils et al., 2016). This scale consists of three subscales: a Resources and Interpersonal Skills subscale (13 items), a Risks subscale (six items), and a Stigma subscale (three items). All 22 items were evaluated using a five-point scale (1 = strongly disagree; 5 = strongly agree). Reverse-scored items were recorded, with higher scores indicating higher romantic relationship functioning.
Since a Japanese version of RRFS did not exist, we developed one using a back-translation procedure. The first author (T.I.) conducted the initial translation. Subsequently, five occupational therapy researchers, including individuals with study-abroad experience in English-speaking countries, reviewed the translation. A professional translation company then back-translated the final Japanese version into English. The original author of the RRFS reviewed the back-translated version and evaluated the accuracy of the contents.
The Perceived Devaluation Discrimination Scale
The Perceived Devaluation Discrimination Scale (PDD) uses 12 items to measure stigma for individuals with mental illness (domain: perceived stigma). This is a self-reported questionnaire. Participants answer with a four-point scale (1 = strongly disagree; 4 = strongly agree). The total score is calculated following the adjustment of reverse-scored items, with higher scores indicating higher stigma. The reliability and validity of the Japanese version have been confirmed (Shimotsu et al., 2006).
The Nagoya Sexual Functional Questionnaire
The Nagoya Sexual Functional Questionnaire (NSFQ) is a self-reported questionnaire measuring sexual dysfunction for individuals with schizophrenia or mood disorders (domain: sexual functioning). The five or seven items are evaluated with a six-point scale (1 = not at all; 5 = always; 6 = unsure). Responses 1 through 5 are scored from 1 to 5 points, respectively, while a response of 6 is scored as 1 point. Higher scores indicate more serious sexual dysfunction. The reliability and validity of the NSFQ have been confirmed in Japan (Kikuchi et al., 2011).
The Recovery Assessment Scale
The Recovery Assessment Scale (RAS) is a self-reported questionnaire measuring the process of recovery for individuals with mental illness (domain: recovery). This measure consists of 24 items with five subscales: goal/success orientation and hope (nine items); reliance on others (four items); personal confidence (five items); no domination by symptoms (two items); and willingness to ask for help (four items). Respondents answer each item using a five-point scale (1 = strongly disagree; 5 = strongly agree). Higher scores indicate a higher level of recovery. The reliability and validity of the Japanese version have been confirmed (Chiba et al., 2010).
The Temple University Community Participation measure – Japanese version
The Temple University Community Participation measure – Japanese version (TUCP-J) measures community participation for individuals with mental illness (domain: participation). This scale requires participants to self-report on the following, for each of 27 activities over the past 30 days: (a) the number of days the activity was performed without staff assistance; (b) the level of satisfaction (1 = sufficient, 2 = insufficient, 3 = excessive); and (c) whether the activity is considered important (1 = yes, 2 = no). The TUCP-J has five participation constructs:
Participation amount
The total number of days of participation reported across the 27 activity domains (range: 0–810).
Number of important activities areas
The number of activities identified by the participant as important (range: 0–27).
Breadth of participation
The total number of important domains in which the participant engaged on at least 1 day. This score reflects the diversity of domains in which the individual is at least somewhat involved (range: 0–27).
Breadth ratio
The proportion of important activities in which the participant engaged on at least 1 day (range: 0–1.0).
Participation sufficiency
The proportion of important activities in which the participant reported being “sufficiently able to participate” (range: 0–1.0).
The reliability and validity of TUCP-J have been confirmed (Nagata et al., 2022). The present study examined three constructs: participation amount; breadth ratio; and participation sufficiency.
Data analysis
We used R Studio (version 4.4.0) for all analyses.
Descriptive statistics were first conducted to summarize demographic variables. For each measure, scores were calculated according to established scoring procedures, and normality was assessed using the Shapiro–Wilk test.
To examine associations between assessment scores and demographic characteristics, we conducted univariate analyses, including analysis of variance (ANOVA), Pearson’s correlation coefficients, and Spearman’s rank correlation coefficients. ANOVA was used for nominal variables, Pearson’s correlation for normally distributed variables, and Spearman’s correlation when normality assumptions were not met.
The primary objective was to assess correlations between romantic relationship functioning and factors hypothesized to influence such functioning among individuals with SMI. The RRFS score served as the response variable, with monthly budget for personal use, PDD, NSFQ, RAS, and TUCP-J scores included as explanatory variables.
To clarify these associations, univariate correlation analyses were performed between RRFS total and subscale scores and each explanatory variable. Pearson’s correlations were used for PDD, NSFQ, RAS, and TUCP-J, whereas Spearman’s correlations were used for monthly budget for personal use. Age and highest educational level were included as covariates based on preliminary findings.
Statistical significance was defined as p < 0.05 after Bonferroni correction.
Results
Participant characteristics
A total of 41 participants were recruited. After screening, one participant was excluded because they were not cisgender, and another because they did not report having an SMI. The final data set thus comprised 39 participants.
Table 1 summarizes demographic variables as the frequency or mean ± standard deviation (SD). The mean (±SD) age of participants was 42.3 ± 10.8 years. Participants comprised 12 women (30.8%) and 27 men (69.2%). Five participants (12.8%) were married, 3 (7.7%) were in a relationship, and 31 (79.5%) were single. Mean GAF score was 57.3 ± 13.6. Diagnoses were schizophrenia in 27 participants (69.2%), depression in 9 (23.1%), and bipolar disorder in 7 (17.9%). Overall, the sample was characterized primarily by middle-aged, predominantly male, and largely single individuals, most of whom were diagnosed with schizophrenia.
Characteristics of study participants (n = 39).
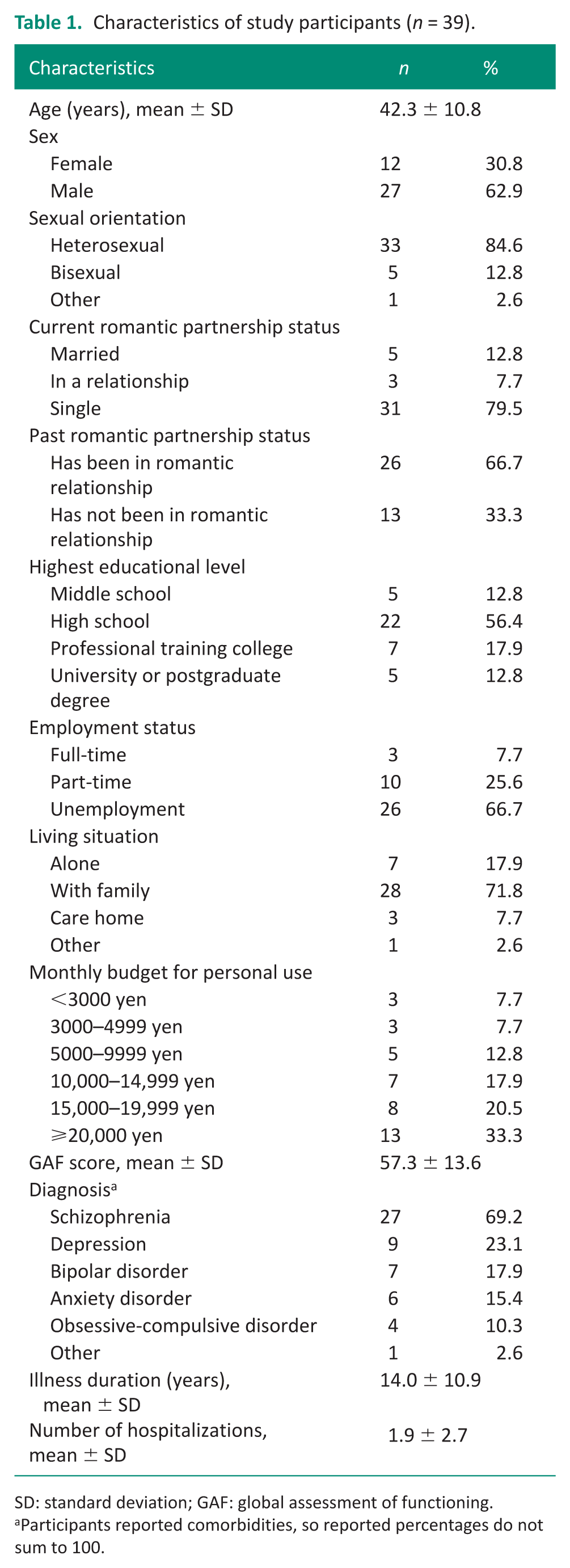
SD: standard deviation; GAF: global assessment of functioning.
Participants reported comorbidities, so reported percentages do not sum to 100.
Results from self-reported questionnaires
Results from the RRFS, PDD, NSFQ, RAS, and TUCP-J are shown in Table 2.
Results of questionnaires.
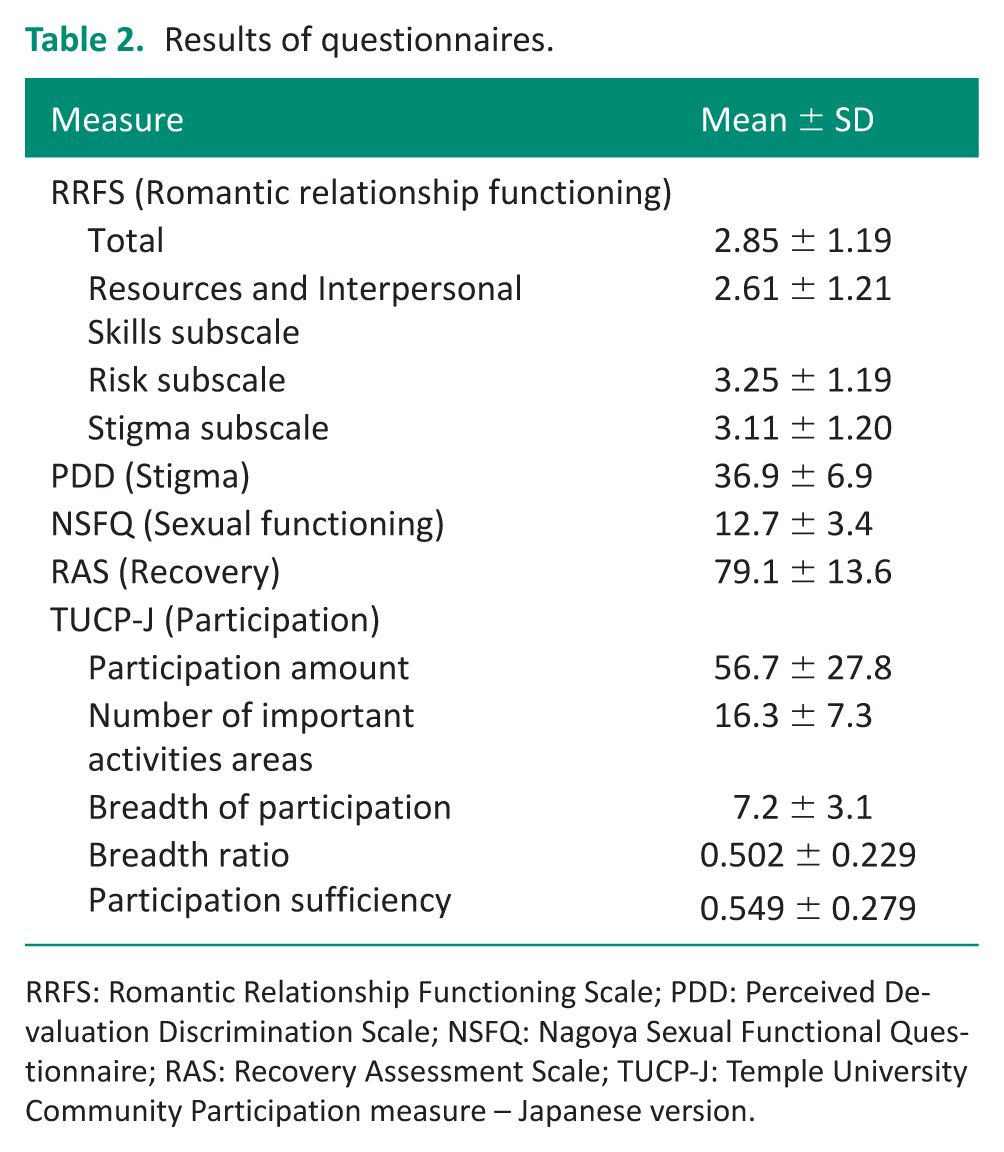
RRFS: Romantic Relationship Functioning Scale; PDD: Perceived Devaluation Discrimination Scale; NSFQ: Nagoya Sexual Functional Questionnaire; RAS: Recovery Assessment Scale; TUCP-J: Temple University Community Participation measure – Japanese version.
The mean total score of the RRFS, which assesses romantic relationship functioning including skills, resources, and attitudes, was 2.85 ± 1.19. Among its subscales, the mean score for Resources and Interpersonal Skills was 2.61 ± 1.21, Risk was 3.25 ± 1.19, and Stigma was 3.11 ± 1.20. These results indicate that participants reported comparatively lower levels of perceived interpersonal skills and resources related to romantic relationships, whereas scores on the Risk and Stigma subscales were comparatively higher, suggesting that difficulties in these domains were less pronounced.
Mean scores for the other measures were 36.9 ± 6.9 for the PDD, 12.7 ± 3.4 for the NSFQ, and 79.1 ± 13.6 for the RAS. For the TUCP-J, mean scores were 56.7 ± 27.8 for Participation Amount, 0.502 ± 0.229 for Breadth Ratio, and 0.549 ± 0.279 for Participation Sufficiency.
To examine associations between participant characteristics and outcome measures, ANOVA, Pearson’s correlation coefficients, or Spearman’s rank correlation coefficients were applied as appropriate based on the level of measurement and distribution of the variables. The results showed a significant association between PDD score and educational attainment. Participants with a university or postgraduate degree scored significantly higher on the PDD than those with a vocational school or middle school education (p < 0.05). In addition, Participation Amount correlated significantly with age, such that younger participants reported greater levels of Participation Amount (r = −0.46, p < 0.05). These findings suggest that educational attainment and age may be associated with perceived stigma and community participation.
Based on these results, further analyses were conducted to examine the associations between romantic relationship functioning and the identified factors.
Associations between RRFS total score and explanatory variables
Partial correlation analyses were conducted to examine factors associated with romantic relationship functioning while controlling potential confounding influences. We conducted partial correlation analysis between RRFS total score and explanatory variables to clarify the correlation between romantic relationship functioning and factors related to difficulties in romantic relationships. RAS score showed a significant positive correlation with the RRFS total score (Table 3). In other words, higher levels of recovery were associated with greater romantic relationship functioning.
Correlation between romantic relationship functioning and economic status, self-stigma, sexual dysfunction, recovery, and social participation.
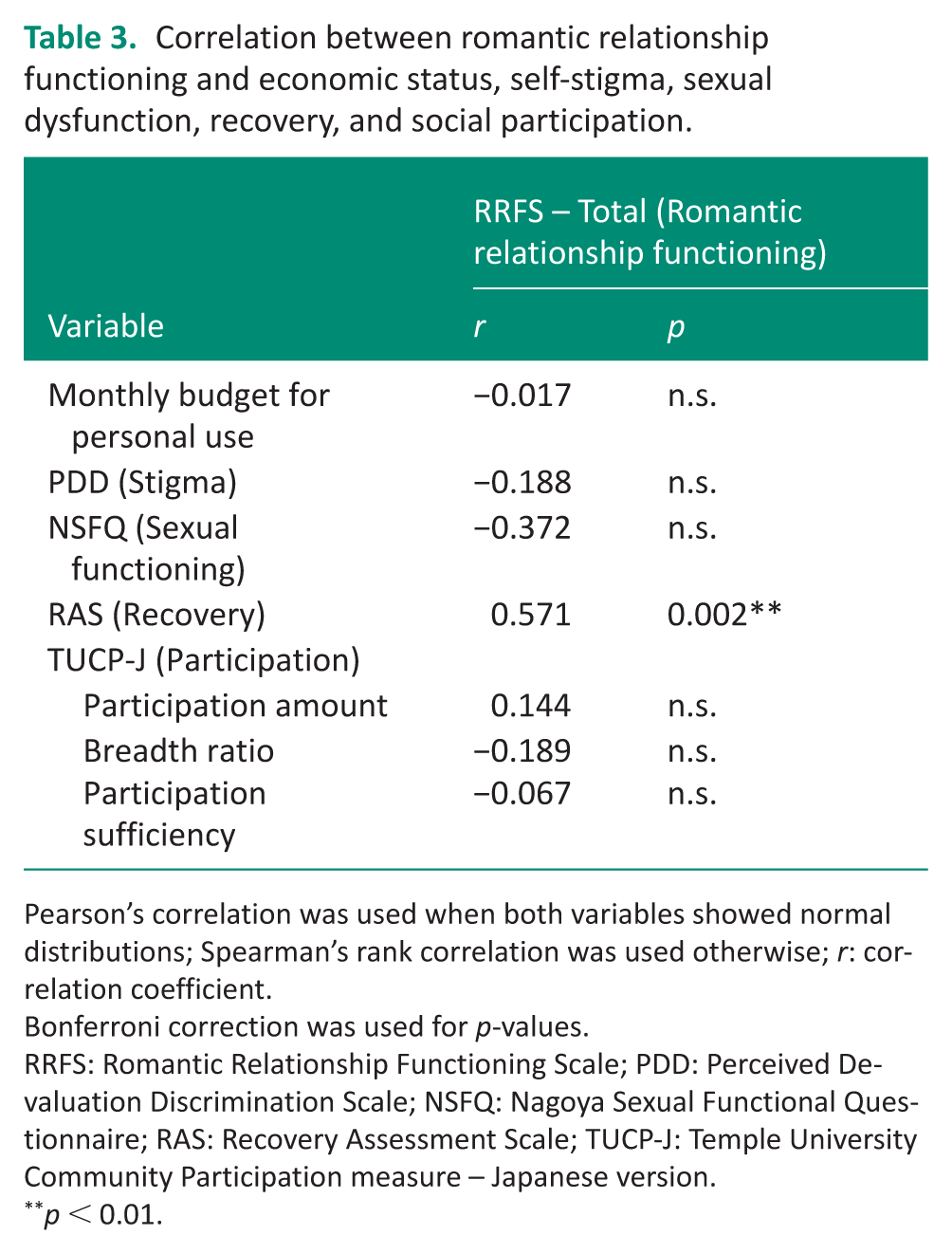
Pearson’s correlation was used when both variables showed normal distributions; Spearman’s rank correlation was used otherwise; r: correlation coefficient.
Bonferroni correction was used for p-values.
RRFS: Romantic Relationship Functioning Scale; PDD: Perceived Devaluation Discrimination Scale; NSFQ: Nagoya Sexual Functional Questionnaire; RAS: Recovery Assessment Scale; TUCP-J: Temple University Community Participation measure – Japanese version.
p < 0.01.
Association between RRFS subscale scores and explanatory variables
To further explore these relationships, partial correlation analyses were performed for each RRFS subscale. We conducted partial correlation analysis between RRFS subscale scores and explanatory variables to understand the correlations in detail. RAS score showed a significant positive correlation with the RRFS Resources and Interpersonal Skills subscale score (Table 4). This indicates that participants with higher recovery scores tended to report stronger interpersonal skills and resources related to romantic relationships.
Correlation between RRFS subscales and economic status, self-stigma, sexual dysfunction, recovery, and social participation.
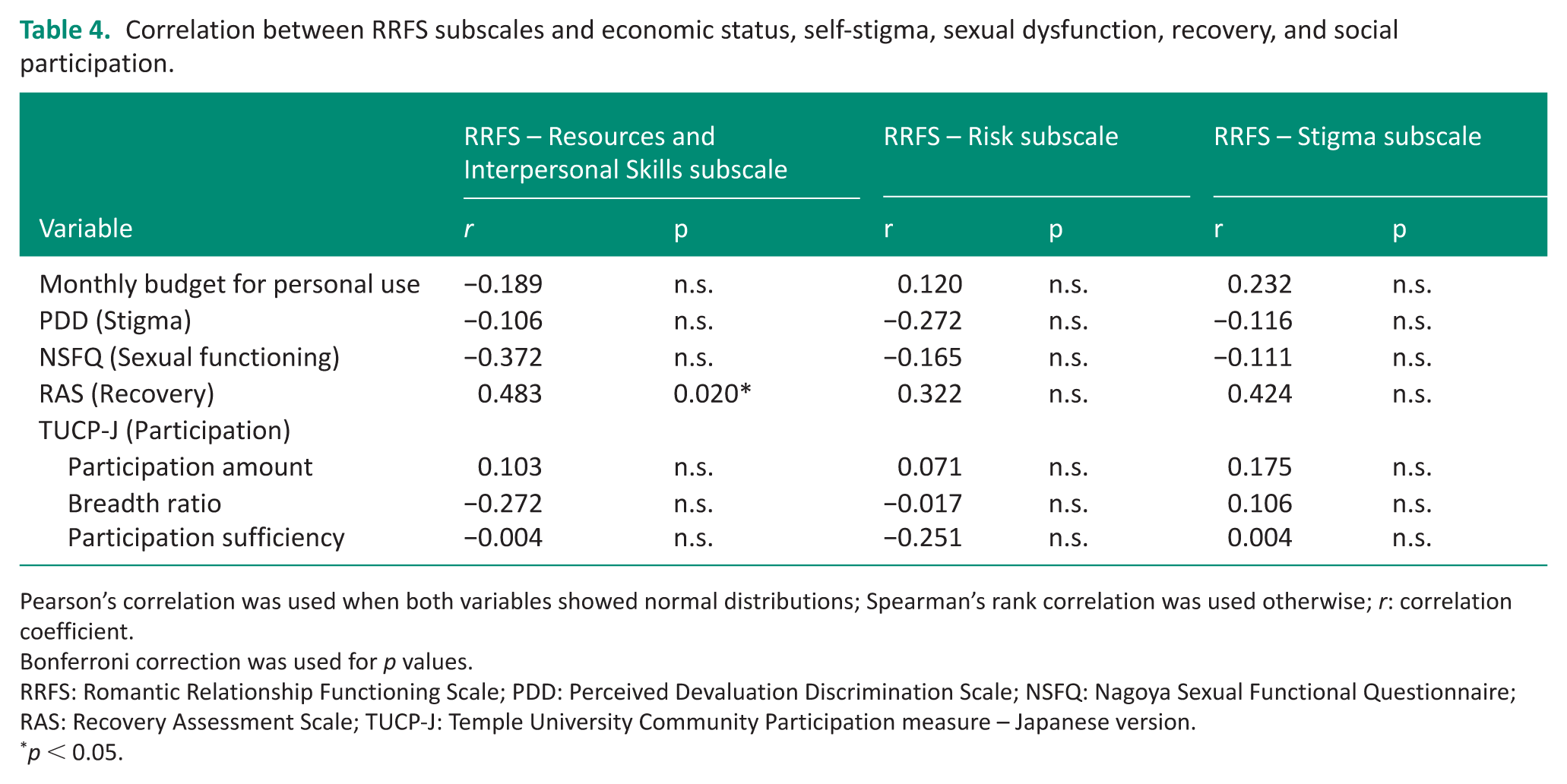
Pearson’s correlation was used when both variables showed normal distributions; Spearman’s rank correlation was used otherwise; r: correlation coefficient.
Bonferroni correction was used for p values.
RRFS: Romantic Relationship Functioning Scale; PDD: Perceived Devaluation Discrimination Scale; NSFQ: Nagoya Sexual Functional Questionnaire; RAS: Recovery Assessment Scale; TUCP-J: Temple University Community Participation measure – Japanese version.
p < 0.05.
Discussion
The present study aimed to clarify how community-living individuals with SMI in Japan perceive the skills, resources, and attitudes required to establish and maintain romantic relationships, and to examine how these perceptions are associated with factors influencing romantic relationships.
Findings related to romantic relationship functioning
The findings indicate that participants reported relatively low levels of perceived resources and interpersonal skills related to romantic relationships, whereas difficulties related to risks and stigma appeared less pronounced. Among the examined factors, recovery was the only variable significantly associated with overall romantic relationship functioning. Importantly, these results suggest that challenges in romantic relationship participation may be particularly linked to perceived competence and contextual barriers rather than to lack of interest.
The relatively lower scores on the Resources and Interpersonal Skills subscale suggest that participants may experience limited confidence in initiating, sustaining, and navigating intimate relationships. Romantic relationships require complex interpersonal communication, emotional regulation, and the coordination of shared activities (Bertrand et al., 2025; Lovis-Schmidt et al., 2024); thus, these capacities represent core components of romantic relationship functioning. In contrast, the comparatively higher scores on the Risk and Stigma subscales suggest that perceived barriers related to negative outcomes or social judgment may have been less pronounced than difficulties in Resources and Interpersonal Skills. Together, these findings highlight that difficulties in romantic relationship participation may be particularly reflected in perceived competence and available resources, while also being situated within a broader sociocultural context.
To contextualize these findings within Japan, the present results were compared with previous studies. RRFS scores were lower than those reported among mental health service users in the United States (Bonfils et al., 2016), suggesting comparatively lower perceived romantic relationship functioning in this Japanese sample. Mean PDD scores were higher than those reported by Okamoto (2020), indicating relatively elevated perceived stigma. In contrast, NSFQ and RAS scores were comparable to prior Japanese studies (Kikuchi et al., 2011; Okamoto, 2020), suggesting that sexual functioning and recovery levels were not substantially different from other Japanese mental health populations. For TUCP score, direct comparisons were limited due to differences in activity items (Nagata et al., 2020). Collectively, these patterns may reflect sociocultural factors specific to Japan, where social expectations regarding romantic relationships and persistent stigma toward mental illness may shape individuals’ perceptions of their relational capacities and opportunities.
Relationships between romantic relationship function and recovery
In this study, recovery was the only factor significantly associated with romantic relationship functioning. This finding aligns with prior studies suggesting that relational intimacy and confidence are positively related to recovery among individuals with SMI (Ecker et al., 2018; Kageyama et al., 2023).
Recovery involves psychological capacities such as hope, self-efficacy, acceptance of illness, and the ability to manage personal resources to achieve goals (Barbic and Krupa, 2018; Dell et al., 2021). These capacities overlap conceptually with the interpersonal and resource-related components required to initiate and maintain romantic relationships. In particular, the significant association between the RRFS Resources and Interpersonal Skills subscale and RAS scores suggests that recognizing and utilizing personal strengths may constitute a shared mechanism underlying both recovery and romantic relationship functioning.
Although the present cross-sectional design does not allow determination of causality, it may not be unexpected that recovery and romantic relationship functioning are related. Individuals who experience greater psychological stability and self-confidence may feel more capable of engaging in intimate relationships, while relational experiences themselves may contribute to strengthening recovery-related processes. Future longitudinal research is warranted to clarify the direction and mechanisms of this association.
Consideration of nonsignificant factors
In contrast to recovery, the other examined factors, including perceived stigma, sexual dysfunction, and community participation, were not significantly associated with romantic relationship functioning in this study. This finding suggests that romantic relationship functioning may not be directly determined by symptom-related or participation-related indicators solely.
One possible interpretation is that global measures of stigma or community participation may not fully capture the interpersonal competencies and subjective relational confidence reflected in romantic relationship functioning. Romantic relationships require context-specific skills, emotional regulation, and dyadic interaction patterns that may not be sufficiently represented in broader measures of social participation (Fávero et al., 2021).
Additionally, the relatively small sample size may have limited the statistical power to detect modest associations. Cultural factors may also influence how individuals perceive stigma and relational capacity, potentially moderating these relationships in ways not captured by the present design.
Taken together, these findings indicate that romantic relationship functioning represents a distinct and multifaceted domain that cannot be reduced to general social participation or symptom-related variables.
Clinical implications
The present findings suggest that romantic relationship functioning should be explicitly addressed within occupational therapy practice, particularly in relation to perceived interpersonal skills and relational confidence. Rather than viewing romantic relationships solely as emotional experiences or as secondary outcomes of recovery, therapists may consider them as meaningful occupations that require specific competencies, including communication skills, emotional regulation, and the ability to manage shared activities.
Given that participants reported comparatively lower perceived resources and interpersonal skills, occupational therapy interventions may benefit from incorporating structured opportunities to develop relational competencies. This may include interventions focused on self-efficacy in social interaction, value clarification regarding intimate relationships, and skill-building approaches that support clients in navigating the practical and emotional demands of partnership.
Although recovery was significantly associated with romantic relationship functioning, the findings indicate that romantic relationship functioning represents a distinct domain that cannot be fully explained by general recovery-oriented interventions alone. Therefore, romantic relationships and sexuality should be more intentionally integrated into occupational therapy assessment and goal-setting processes, rather than addressed indirectly.
Intimate relationships constitute one dimension of sexuality. Despite recognition of sexuality as part of occupational therapy’s professional scope, clinical engagement in this area remains limited due to factors such as insufficient training, lack of practice guidelines, professional discomfort, and privacy concerns (Hwang et al., 2023; Hyland and Mc Grath, 2013). The present study highlights the need to move beyond avoidance and to position romantic relationship participation as a legitimate and ethically relevant area of occupational therapy practice and education.
By acknowledging romantic relationship functioning as a meaningful occupation requiring specific skills and contextual support, occupational therapy may further advance toward a holistic and person-centered model that addresses the full spectrum of human participation.
Limitations
The present study has four main limitations. First, all examined factors were based on Western research, despite substantial cultural differences in romantic and sexual norms between Asian and Western societies. Greater sexual conservatism in Asian populations (Meston and Ahrold, 2010) may have influenced the finding. Second, sex differences were not examined, even though variations in romantic relationships across sexes may exist. Third, psychiatric symptoms were not assessed, limiting interpretation of their potential effects on romantic relationship functioning. Fourth, the small sample size reduced the statistical power, partly because many individuals declined to participate due to discomfort discussing romantic relationships. Future studies should adopt culturally sensitive recruitment strategies. In addition, larger samples and multivariate approaches (such as multiple regression or path analysis) will be necessary to clarify how these factors influence romantic relationship functioning. Despite these limitations, the present study contributes preliminary evidence regarding the skills, resources, and attitudes associated with romantic relationship functioning among community-living individuals with SMI in Japan and provides a foundation for further research in this domain.
Conclusion
This study examined the skills, resources, and attitudes related to romantic relationship functioning among community-living individuals with SMI in Japan. The findings indicated that participants reported relatively lower perceived interpersonal skills and resources, while recovery was significantly associated with romantic relationship functioning. These results suggest that romantic relationship functioning represents an important and distinct domain of occupational participation that warrants explicit attention within occupational therapy assessment and intervention. Further research with larger samples and multivariate approaches is needed to clarify the mechanisms underlying these associations.
Key findings
Romantic relationship functioning was characterized by lower perceived relational skills and resources.
Recovery was the only significant associated factor.
What the study has added
This study provides preliminary quantitative evidence on romantic relationship functioning, including perceived skills and resources, among individuals with SMI in Japan and highlights its relevance for occupational therapy assessment and intervention.
Footnotes
Acknowledgements
We sincerely appreciate all the participants for their valuable contributions to this study. We also extend our gratitude to the staff of the day-care centers and to the members of our laboratory for their support.
Ethical considerations
This study was approved by the Research Ethics Committee of the Graduate School of Medicine, Nagoya University, Japan in 2024 (authorization no. 24-601) and the Research Ethics Committee of Kyowa Hospital, Specified Medical Corporation Kyowakai, Japan in 2024 (authorization no. 2024-010).
Consent to participate
Verbal and written consent was obtained from all participants prior to study enrollment.
Author contributions
All authors made substantial contributions to the study. TI and HI led the development of the Japanese version of the Romantic Relationship Functioning Scale, which served as the primary outcome measure in this study, through a structured translation and back-translation process. TI and AH obtained ethics approval. TI and YI coordinated participant recruitment and collected the data. TI drafted the initial manuscript. All authors contributed to the analysis and interpretation of the data, engaged in critical discussion, revised the manuscript for important intellectual content, and approved the final version of the manuscript.
Funding
The authors declared no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Patient and public involvement data
During the development, progress, and reporting of the submitted research, patient and public involvement in the research was not included at any stage of the research.