
Abstract
Introduction:
Occupational therapists play a crucial role in identifying and addressing residual visual function impairments—such as oculomotor and binocular dysfunctions—as part of comprehensive neurorehabilitation. This study aimed to describe the effects of individualised, vision-focused occupational therapy on patient-reported outcomes among individuals with post-COVID-19 visual dysfunction.
Method:
A retrospective before-and-after design was employed. Thirty-six consecutive patients with confirmed visual impairment following COVID-19 infection participated. Visual function screening was followed by tailored occupational therapy targeting visual deficits. The primary outcome was a domain-specific adaptation of the Canadian Occupational Performance Measure. Secondary outcomes included the Convergence Insufficiency Symptom Survey and the Mental Fatigue Scale.
Results:
Significant improvements were observed in occupational performance (p < 0.001) and satisfaction with performance (p < 0.001). Mental fatigue and self-rated symptoms during near activities were also significantly reduced (both p < 0.001).
Conclusion:
Identifying the daily occupations most affected by visual impairments enables occupational therapists to effectively target interventions. Individualised, vision-focused occupational therapy improved patient-reported occupational performance and alleviated associated symptoms.
Introduction
Vision is fundamental to daily activities and is often considered a primary sense due to its essential role in information processing, communication, mobility, movement guidance, and spatial orientation (Kerkhoff, 2000). Efficient visual function depends, for example, on the seamless visuomotor integration. Acquired brain injury (ABI) caused by trauma, stroke, or infection can disrupt this process, leading to symptoms such as, double or blurred vision, eyestrain, headaches, reduced activity endurance, and dizziness—particularly in visually busy environments (Berthold-Lindstedt et al., 2019; Johansson et al., 2022; Rowe et al., 2019).
Rehabilitation, including occupational therapy, following ABI primarily focuses on identifying the patient’s resources and needs. A comprehensive rehabilitation assessment typically results in a detailed profile of the patient’s physical, cognitive, and emotional strengths and limitations, as well as their specific occupational and participation needs. Within this process, occupational therapists play a crucial role, with information regarding patients’ abilities, needs, and challenges forming the foundation for a personalised rehabilitation programme.
Literature review
Consequences of visual dysfunction, including oculomotor and/or binocular function has been described in several scientific studies. Consequences affecting daily life are, for example, uncertainty in unfamiliar environments, fear of falling, difficulties with fine motor tasks due to impaired eye–hand coordination, challenges in group communication caused by problems with shifting or maintaining visual attention. In addition, difficulties with reading, computer, or phone use and driving, have been described (Ciuffreda et al., 2007; Smaakjaer et al., 2018).
Wagener and Kreiger (2019) conducted a cross-sectional study interviewing 40 individuals with ABI and confirmed visual impairment attending outpatient rehabilitation. Over 85% of participants reported difficulties in leisure activities, work or study, and household management. Common challenges included group communication (82%), attending sports events (83%), cycling (83%), computer use (72%), and driving (68%). Regression analysis indicated that visual impairment accounted for approximately half of the participation difficulties reported.
Identifying vision-related impairments can be challenging, and simply asking the patient may not be sufficient (Berthold-Lindstedt et al., 2021). Standard neurological assessments may not detect diffuse visual symptoms or their impact on daily life. Therefore, a comprehensive approach involving observation of occupational performance, structured anamnestic questions, functional testing, and symptom provocation is often required. Any identified problems can then guide individually tailored interventions. The intervention applied in this study was based on vision therapy principles (American Optometric Association), which have been shown to improve affected functions, alleviate perceived symptoms (Johansson et al., 2021), and enhance overall activity performance (Smaakjaer et al., 2018). Despite the use of holistic frameworks, sensory systems—particularly visual function—are often overlooked in assessment and rehabilitation planning. This is noteworthy, as several studies report a prevalence of visual impairments exceeding 50% among patients with ABI (Ciuffreda et al., 2007; Pula and Yuen, 2017; Thiagarajan et al., 2011). The present study focuses on oculomotor and binocular dysfunctions as a post-COVID-19 symptom and explores their impact on daily life-symptoms commonly described after ABI of any aetiology.
Similar descriptions of visuo-related problems as outlined above, have been reported following COVID-19 (Duan et al., 2024; González-Vides et al., 2024; Johansson et al., 2022, 2024; Trofimov et al., 2023; Vinuela-Navarro et al., 2023). However, we identified no studies of relevance, evaluating vision-specific rehabilitation after COVID-19 that report outcome in terms of occupational performance. Owing to the lack of outcome studies, this study aimed to describe the effects of individualised, vision-focused occupational therapy on patient-reported outcomes among individuals with post-COVID-19 visual dysfunction.
Methods
Study design
A retrospective before-and-after design was employed
Ethics
The study was performed in accordance with the Declaration of Helsinki. An ethical approval was granted in 2022, and informed consent was obtained from all participants.
Setting
Patients with vision-related problems were referred from a temporary post-COVID-19 outpatient clinic to a university rehabilitation department. A structured screening of visual function, based on a model assessing both oculomotor and non-oculomotor function, was conducted by a specialist nurse in collaboration with an occupational therapist, with support from an optometrist. At the appointment, each patient also completed two standard questionnaires addressing visual symptoms and fatigue. Of the first 45 patients who completed rehabilitation, 36 (78%) consented to participate.
Screening of visual function
Screening included several relevant tests (Supplemental Appendix Table 1), complemented by clinical assessments of eye movements (Supplemental Appendix Table 2) and visual motion sensitivity (VMS). VMS was assessed by exposing patients to peripheral motion—initially using hand movement (n = 12), and later using an optokinetic drum (n = 23) (Tannen et al., 2020). Patients rated discomfort on a 0–10 scale for each quadrant of the visual field; scores of ⩾5 were considered clinically important.
Intervention
The aim of the individualised vision-focused occupational therapy (IVFOT) programme was to improve patients’ ability to carry out the activities most important to them. The content was guided by symptoms, screening findings, and individual needs. The International Classification of Functioning, Disability and Health (World Health Organization, 2001) was used to describe the functional and activity-oriented context (Figure 1).
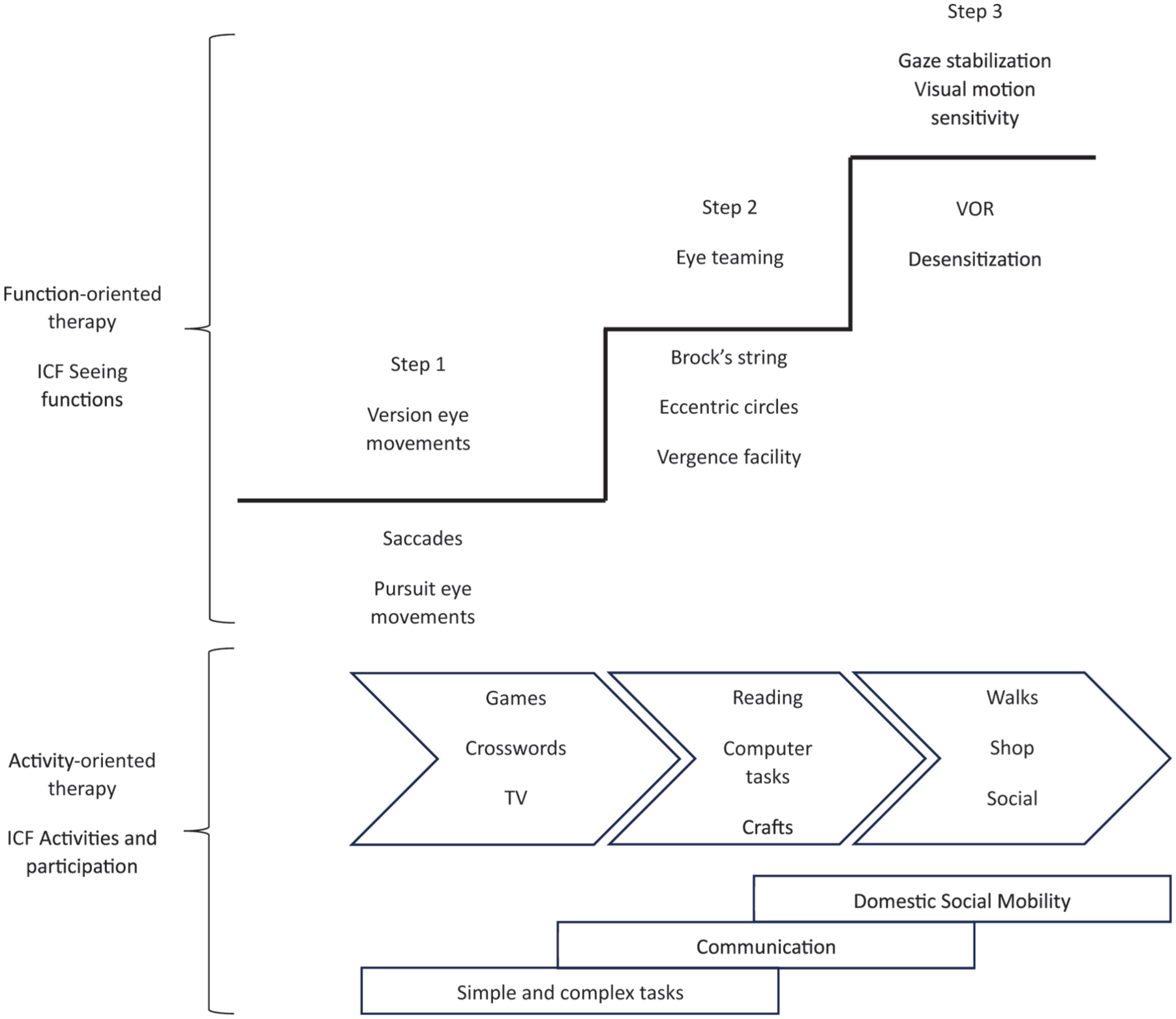
The structure of the individualised vision-focused rehabilitation.
IVFOT was delivered in three progressive steps (Figure 1), each comprising specific training activities with indicative performance targets (Supplemental Appendix Table 3 for details). A specialised occupational therapist tailored home-based exercises for each patient and conducted regular follow-up to adjust the frequency, type, and intensity of training.
The function-oriented rehabilitation targeted seeing functions (ICF b210). The activity-oriented rehabilitation phase was introduced to gradually generalise the function-oriented IVFOT to vision-demanding prioritised activities in daily life. The primary targets included:
General tasks and demands (simple and complex tasks, ICF d210),
Communication (conversation and use of communication devices, ICF d360),
Mobility (moving around and using transportation, ICF d499),
Domestic life (acquisition of goods and services, ICF d620),
Community, social, and civic life (recreation and leisure, ICF d920).
Version eye movements refer to conjugate eye movements where both eyes move in the same direction. Eye teaming involves binocular functions, enabling the eyes to move, focus together, and shift between near and far viewing. Gaze stabilisation compensates for head movements, allowing for steady fixation. VMS refers to increased sensitivity to moving visual stimuli.
Early stages focused on eye movements to help patients recognise symptoms and balance training intensity. Later stages introduced more complex, occupational-based tasks such as reading, computer work, crafts, and walking in natural or urban environments, integrating visual scanning, eye-teaming, and gaze stabilisation within everyday contexts.
Outcome measures
Primary outcome
The Canadian Occupational Performance Measure (COPM) (Law et al., 1990) was adapted for visual symptoms based on prior research and clinical experience (Johansson et al., 2022). The occupational therapist initially discussed three predefined occupational areas with all clients: reading, screen use, and performing activities in visually busy and/or cluttered environments. In addition, patients could identify any other important occupational performance problems affected by vision-related symptoms. Patients identified up to five vision-related problematic occupations and rated performance (COPM-P) and satisfaction (COPM-S) on a 1–10 scale, where 1 = not able to do it at all/not satisfied at all, and 10 = able to do it extremely well/extremely satisfied. During follow-up, patients rescored the same occupations without being shown their initial scores.
Secondary outcomes
The Convergence Insufficiency Symptom Survey (CISS) is a self-rating questionnaire focusing on reading and activities performed at near (Rouse et al., 2004). Results from CISS help to quantify the severity of symptoms such as eye pain, blurred vision, headache, or difficulty concentrating while reading or doing activities at near. CISS includes 15 questions, and the patient is asked to rate how often the symptom occurs on a 5-point scale (0 = never; 4 = always). A cut-off score >21 is considered to be a clinical observandum (Rouse et al., 2004). The CISS was filled in by the patient at three occasions: at the temporary COVID-19 outpatient clinic, and before and after IVFOT.
The Mental Fatigue Scale (MFS) questionnaire is designed to capture the perceived mental fatigue and related symptoms experienced over the past month irrespective of neurological disease or injury (Johansson et al., 2010). The MFS includes 14 questions on affective, cognitive, and sensory symptoms, duration of sleep, and daytime variation in symptom severity. The severity of symptoms are rated: none = 0, slight = 1, fairly serious = 2, and serious = 3 problems. The patient is asked to compare each condition with how it was before the injury/illness. The maximum score is 42 and a score >10.5 is considered to be a clinical observandum. Furthermore, the score has been empirically categorised as mild mental fatigue (10.5–14.5), moderate mental fatigue (15–20), and severe mental fatigue (20.5–42) (personal communication, B. Johansson). The MFS was filled in by the patient before and after IVFOT.
Statistics
Analyses were performed using IBM SPSS Statistics 27 (IBM, Armonk, NY). The Wilcoxon matched-pairs test was used to compare baseline and follow-up data. Friedman’s ANOVA was used for repeated CISS measures with Bonferroni corrections. Effect sizes were calculated from z-scores. Correlations were analysed using Spearman’s rho with bias-corrected and accelerated (BCa) 95% confidence intervals from 1,000 bootstrap samples. Significance was set at p ⩽ 0.05.
Results
The mean age was 50 ± 9.2 years (range 30–70; of the 36 participants, 29 were female/81%). The mean interval from COVID-19 infection to vision assessment was 15.8 ± 6.1 months (range 8–30 months).
Screening of visual function
The most common symptoms reported by the patients were dizziness, nausea, headache, tiredness, eyestrain, blurred vision, and a gritty sensation in the eyes. Two questions from the vision screening were repeated after IVFOT: VMS and headache. After IVFOT, VMS symptoms decreased from 91% (n = 32) to 14% (n = 5). Headache was initially reported by 71% (n = 28) of which all but four patients still experienced headaches at follow-up.
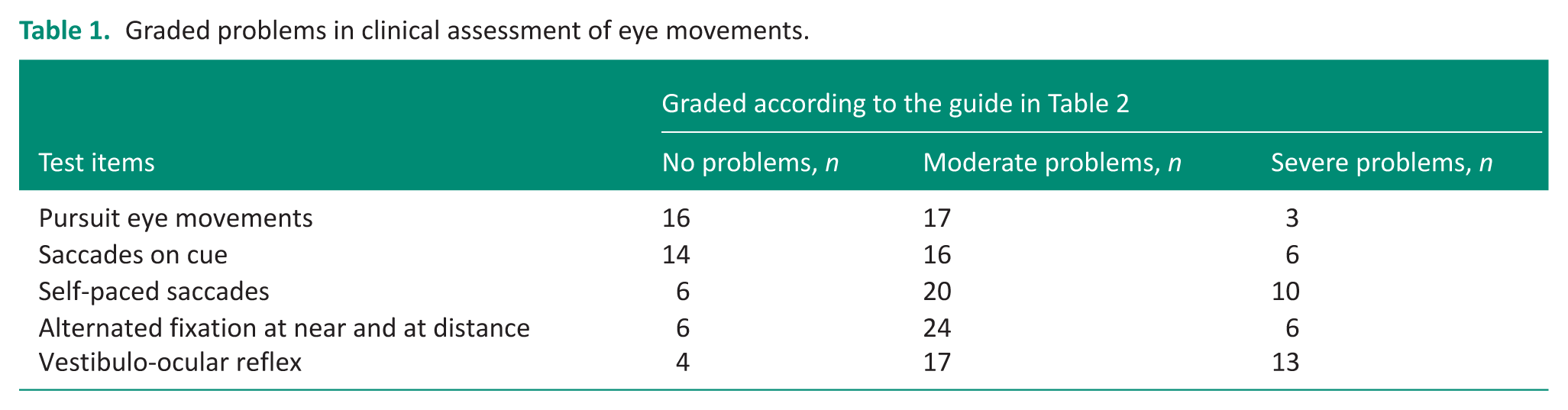
The optometrist was consulted when there was an indication of unstable eye teaming function (n = 5). Based on this, training activities targeting eye teaming were adapted. Overall, 22 (61%) patients reported discomfort during clinical assessment of visual motion. Three patients had suboptimal visual acuity due to inadequate optical correction and were referred to an optician. A receded near point of convergence (>10 cm) was found in 14 patients (40%). Impaired performance in three or more screening items; pursuit, saccades on cue or self-paced, altered fixation, VOR, and convergence, occurred in 86% of the patients. A summary of the eye movement screening is shown in Table 1.
Graded problems in clinical assessment of eye movements.
Occupational performance and satisfaction
As shown in Figure 2, significant improvements were found in COPM-P (p < 0.001; effect size = 0.61) and COPM-S (p < 0.001; effect size = 0.62).
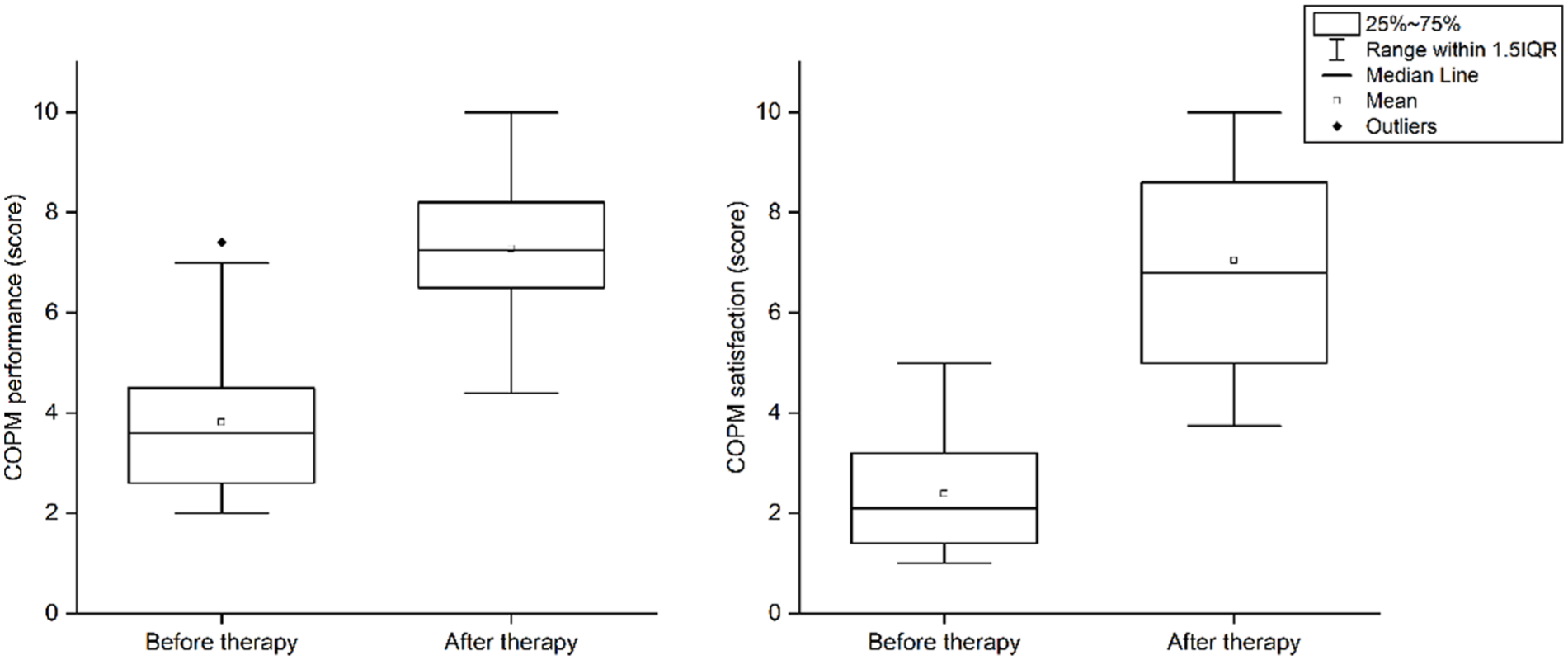
Outcomes of patient-reported data regarding activity performance and satisfaction with performance before and after VFR.
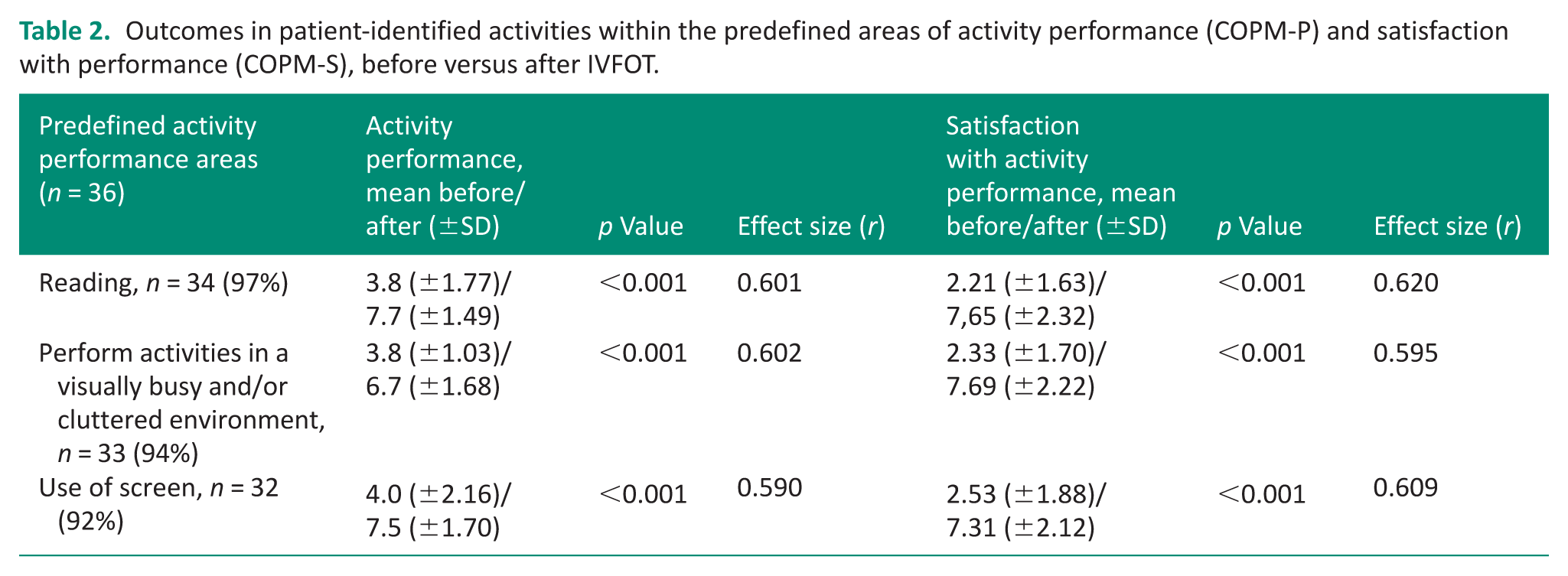
In predefined occupational areas (reading, screen use, visually busy environments), 92%–97% of patients reported problems (Table 2). Ninety-four per cent identified additional affected occupations, most commonly driving or being a passenger (51%), walking, running, social participation, climbing stairs, playing golf, and household tasks.
Outcomes in patient-identified activities within the predefined areas of activity performance (COPM-P) and satisfaction with performance (COPM-S), before versus after IVFOT.
Visual symptoms and mental fatigue
CISS scores did not change significantly between referral (34.2) and vision screening (32.4; p = 0.951) but had decreased at follow-up to 22.5 (p < 0.001; effect size = 0.49). MFS scores also decreased significantly from vision screening to follow-up (p < 0.001; effect size = 0.43). The number of patients with moderate-to-severe mental fatigue decreased at follow-up (Figure 3).
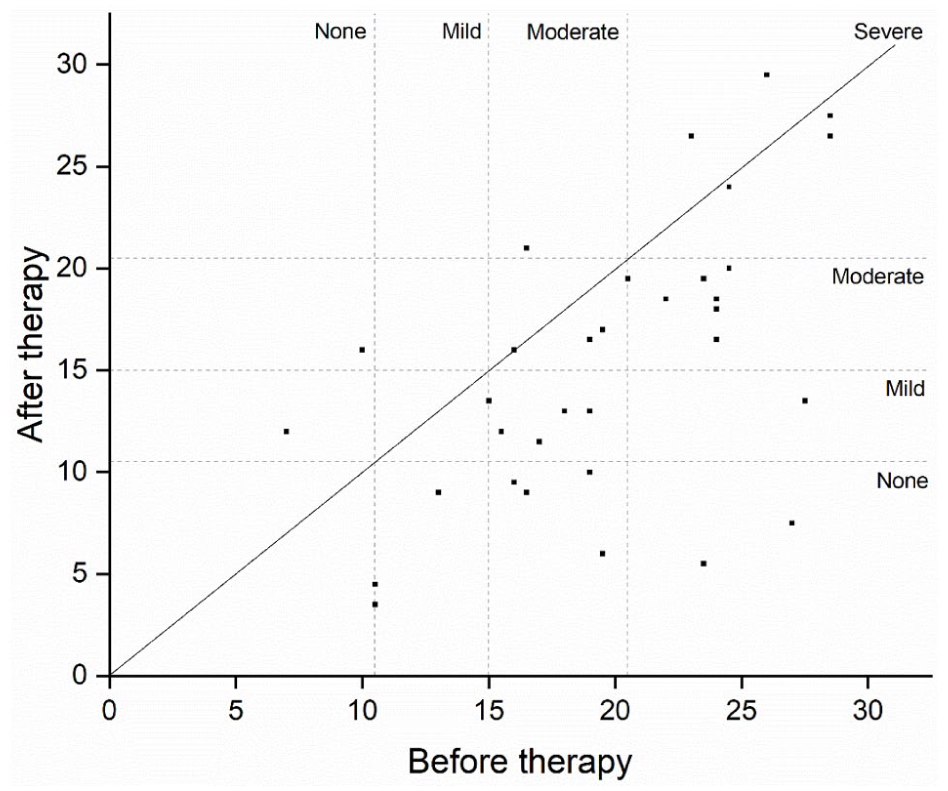
Levels of mental fatigue before and after IVFOT seen in relation to clinical thresholds.
Discussion
This study aimed to describe the effects of individualised, vision-focused occupational therapy (VFOT) on patient-reported outcomes among individuals with post-COVID-19 visual dysfunction. The findings underscore the potential benefits of systematic screening of visual functions, complemented by semi-structured interviews, to identify the impact of patient-reported visual impairments reported by patients following an injury or illness affecting the brain, such as COVID-19. Furthermore, the results support the value of individualised VFOT tailored to specific symptoms and needs, which addresses not only clinical deficits but also occupational limitations identified by the patients themselves.
The use of the COPM as the primary outcome measure aligns with the Canadian Model of Occupational Performance, as it considers the interaction between the person, the environment, and the occupation in intervention planning (Townsend and Polatajko, 2007). The use of the ICF as a structure for describing the type of impairment or disability aspects, as demonstrated in Figure 1, helps in understanding the targets of occupational therapy interventions.
The reliability, validity, and responsiveness of the COPM are well documented (Law et al., 2019), and its clinical utility in enhancing decision-making and patient engagement is well established (Roe et al., 2020). By identifying occupations to the patients but which have become difficult or impossible to perform, the COPM helps motivate patients to engage in training and overcome their avoidance of challenging environments and activities (Nielsen et al., 2015). Furthermore, outcome analyses based on COPM interviews provide professionals with valuable insight into the consequences of visuomotor impairment in daily life, and a foundation for evaluating the effectiveness of VFOT in addressing these challenges. The large effect size and results well above the suggested threshold for a clinically important difference ⩾2 (Law et al., 2019), as well as results presented in Table 2, reinforce the effectiveness of this approach.
Secondary measures, including CISS and MFS, complemented the vision screening by highlighting the impact of symptoms on near-distance activities and mental fatigue, factors critical for tailoring individualised VFOT plans and goal setting. The rationale for using the CISS was based on the premise that insufficient oculomotor functions are more likely to cause symptoms due to higher demands when focusing at near distances. High initial CISS scores, with no pre-rehabilitation improvement, suggest persistent symptoms without intervention. However, the significant reduction in CISS scores post-VFOT indicates its utility in monitoring symptom changes related to near-activity. That said, the measure could be enhanced by incorporating questions on light and motion sensitivity (Johansson et al., 2022, 2024).
Mental fatigue also decreased after VFOT, with some patients reporting a shift to lower clinical fatigue levels at follow-up, as shown in Figure 3. The correlation between reduced fatigue and vision-related symptoms (CISS) aligns with prior research, reinforcing the connection between visual impairment and mental fatigue (Berthold Lindstedt et al., 2019; Kuodi et al., 2023). However residual symptoms related to the multifactorial nature of mental fatigue (Johansson et al., 2014) suggest the need for further investigation into its underlying mechanisms and the role of cognitive functions in CISS assessments (Nunes et al., 2020). Another noteworthy aspect is the mental fatigability reported by most patients, which is difficult to measure and not adequately captured by the MFS. Further studies should explore this issue in more detail, particularly from the perspective of the consequences it has on daily functioning.
The systematic screening procedure proved clinically valuable in identifying patients who could benefit from VFOT. The grading criteria for clinical oculomotor function (Appendix 2) revealed moderate-to-severe deficits in eye movements, fixation, and gaze stabilisation. Additionally, the screening helped increase patients’ awareness and understanding of the underlying mechanisms of their symptoms. These findings are consistent with, and to some instances exceed, findings from previous studies (Johansson et al., 2022, 2024; Kelly et al., 2022), suggesting that impaired eye teaming, eye movements, and sensory integration issues may underpin the symptoms. While the screening procedure cannot replace neurological assessment, it provides a practical tool for confirming elusive symptoms and enhancing patient understanding of their condition. Clinical implications with key learnings from the study highlight the need to perform enough repetitions of each test to provoke symptoms; the patients showed a clear increase in fatigue over time/repetitions and found the assessment surprisingly difficult and bothersome. Fatigability, measured as degrading performance over time, has previously been demonstrated as a factor for assessing brain function (Möller et al., 2017).
The screening procedure as well as the try-out of VFOT triggered symptoms and subsequently contributed to the recognition and awareness of the symptoms. By acknowledging the symptoms and explaining the cause, the patient could be reassured and be part of the process of finding a balanced intensity of the rehabilitation that could be maintained at home. As the rehabilitation progressed, there were often peaks of symptoms, in some cases in direct conjunction with rehabilitation activities, in some cases as a delayed effect as the occupational therapy accumulated, and in some cases, as part of a setback due to a temporary decline in general health and well-being. The occupational therapist played an important role by being available to answer questions, provide reassurance, adjust the intensity when needed and decide when to move on in the rehabilitation programme. The occupational therapist supported training and knowledge-based pep talks were key factors for improvements according to patient feedback. Further, by using the COPM, patients were involved in identifying needs and measures and thereby had an influence on the content of VFOT. As a side effect, outcomes from the COPM measures assisted the clinic in identifying common consequences for activity performance and based on that, appropriate VFOT could be set up.
The study makes a unique contribution to understanding vision-related symptoms and vision-focused rehabilitation following COVID-19, an area in which research remains limited.
Given the similarities in how visual impairments manifest in other conditions requiring neurorehabilitation, the described methods for assessment, intervention, and follow-up are likely applicable across diverse rehabilitation settings. Consequently, the findings from this clinical study hold particular value.
Study limitations and strengths
The retrospective before-and-after design limits the ability to draw causal inference, and the absence of a control group introduces potential confounding factors, such as natural recovery or placebo effects. Post-intervention visual function assessments were not conducted due to clinical routines, preventing direct evaluation of functional changes. Nevertheless, the significant improvements in occupational performance, satisfaction, and symptom reduction suggest meaningful clinical benefits for patients. Future research should include prospective controlled studies incorporating both subjective and objective outcome measures to strengthen the evidence base for VFOT.
Conclusion
Individualised, VFOT effectively reduced symptoms and improved occupational performance among individuals experiencing post-COVID-19 visual impairment. Systematic visual function screening was clinically valuable in identifying visually triggered problems and tailoring occupational therapy interventions accordingly.
Key findings
Support from a professional vision assessment was crucial for enabling a plan for the vision-focused occupational therapy.
Individually identified problems with occupational performance and participation were reduced following vision-focused therapy.
What the study has added
Occupational therapist working in neurorehabilitation need to routinely consider visual impairments into their clinical history-taking and develop the skills required to provide vision-focused occupational therapy as part of their intervention toolbox
Supplemental Material
sj-docx-1-bjo-10.1177_03080226261454913 – Supplemental material for Effects of individualised vision-focused Occupational Therapy on patient-reported outcomes following post-COVID-19 visual impairment
Supplemental material, sj-docx-1-bjo-10.1177_03080226261454913 for Effects of individualised vision-focused Occupational Therapy on patient-reported outcomes following post-COVID-19 visual impairment by Stina Gunnarsson, Kersti Samuelsson, Maria Jacobsson and Jan Johansson in British Journal of Occupational Therapy
Footnotes
Ethical considerations
Ethical approval was granted by the Swedish Ethical Review Authority (Dnr 2022-00618-01).
Consent to participate
Written informed consent was obtained from all participants.
Author contributions
SG, KS and JJ conceptualised the study. All authors contributed to the study design and to protocol development. SG and KS obtained ethical approval and contributed to data analysis together with JJ. SG conducted the formal data analysis and SG, KS and JJ drafted the first version of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Health Care Region of Östergötland, which had no role in study design, data collection, analysis, interpretation, or the decision to submit this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Patient and public involvement data
Patient or Public Involvement in the research was not included at any stage of the research
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.