
Abstract
Introduction:
Patient implementation of breast cancer-related lymphoedema treatment recommendations is often considered suboptimal. This study explored patient implementation of occupational therapy breast cancer-related lymphoedema treatment recommendations and identified barriers and enablers.
Method:
An observational retrospective cohort study was conducted using clinical data from a tertiary hospital’s prospective surveillance model of care for early breast cancer-related lymphoedema detection and intervention. Patients who received occupational therapy were included, and implementation levels were compared above and below a 70% threshold.
Results:
Among 63 patients (median age = 60 years, interquartile range 47.0–70.0), 73% (n = 46) implemented over 70% of recommendations and 29% achieved full implementation. Pain (54%, n = 34) was the main barrier, while strong support networks (63.5%, n = 40) were the leading enabler. Lower implementation was associated with receipt of taxane chemotherapy (p = 0.030), fewer therapy interventions provided (p < 0.001), type of tumour (p = 0.014), lymphoedema management not seen as a patient priority (p = 0.001) and receiving nicotine treatment (p = 0.038). Sentinel node biopsy (p = 0.024) and understanding the risks of poor lymphoedema management (p = 0.019) were associated with increased patient implementation.
Conclusion:
Most patients implemented >70% of breast cancer-related lymphoedema treatment recommendations; however, understanding and addressing clinical and psychosocial factors could optimise implementation and improve outcomes.
Introduction
Approximately 57 Australians are diagnosed with breast cancer each day (Australian Institute of Health and Welfare, 2020), and between 20% and 30% of patients who have received treatment for breast cancer experience breast cancer-related lymphoedema (BCRL) of the upper limb (Zou et al., 2018). Lymphoedema is a chronic, progressive condition that occurs when the volume of lymphatic fluid to be transported exceeds the capacity of the lymphatic system, resulting in accumulation of a protein-rich extracellular fluid in the interstitium (Jung et al., 2020). Left untreated, patients with lymphoedema are twice as likely to develop cellulitis requiring hospitalisation and intravenous antibiotic therapy (Australian Institute of Health and Welfare, 2023).
Lymphoedema has detrimental effects on a person’s physical and psychosocial health and is often associated with pain, discomfort and a loss of function (Loibnegger-Traußnig et al., 2024). All patients undergoing nodal surgeries that is, sentinel node biopsy or axillary clearance have a latent, life-long risk of developing lymphoedema (Westmead Breast Cancer Institute, 2024). However, risk profiles are also influenced by nonsurgical factors, such as radiation to the regional node basin, taxane chemotherapy, high body mass index (BMI) and post-operative wound complications (Koelmeyer et al., 2021).
Living with lymphoedema can have significant functional, psychological and economic impacts on both the individual and the health services, with the severity of the condition directly related to degree of burden (Koelmeyer et al., 2021). As up to 80% of patients with breast cancer will attain full life expectancy, chronic treatment-related morbidity should be minimised (Stout et al., 2012). The pathophysiology of lymphoedema typically progresses through two phases: an early reversible phase with fluid accumulation but no fibrosis, followed by a chronic irreversible phase with intradermal fibrosis (Shaitelman et al., 2015). This progression provides a window of opportunity for intervention in the early phase to prevent chronic lymphoedema.
The Australasian Lymphology Association, National Lymphoedema Network and National Comprehensive Cancer Network all endorse prospective monitoring programmes for patients treated for breast cancer, particularly for those at higher risk of developing BCRL (Dylke, 2019). Evidence suggests that surveillance and early detection through a prospective surveillance model of care (PSM) may be associated with lower incidence and severity of BCRL and lower costs when compared with a traditional referral model of care (Kilgore et al., 2018).
However, despite earlier intervention supported by a PSM, patient implementation of treatment recommendations also significantly impacts BCRL development (DiMatteo et al., 2002). Defined as the extent to which patients follow therapist treatment recommendations, implementation requires collaboration between patients and health professionals (Alcorso et al., 2016; Naumann et al., 2023; Ostby et al., 2018). Treatment for lymphoedema can include skin care, aerobic and resistance exercises, compression therapy, manual lymphatic drainage (MLD), complete decongestive therapy and compression garments (Asfoor and Ghulmi 2021). Studies have indicated suboptimal levels of patient implementation in Australia, with only 19.5% of patients fully implementing prescribed regimens, according to a study completed by Alcorso et al. (2016). This study also identified a correlation between time since diagnosis of BCRL and reduced implementation further emphasising the importance of early intervention in BCRL care (Ostby et al., 2018). Research shows low adherence to lymphoedema care, with only 60% of patients wearing compression garments, 72.5% following skin care regimens and 30% completing bandaging and lymphatic drainage (Alcorso et al., 2016; Rubio et al., 2022).
Some previous studies have examined psychosocial and intervention-related barriers to patient implementation of BCRL treatment recommendations, but relied on self-reported data and lacked objective measures of lymphoedema stage or severity (Alcorso et al., 2016; Brown et al., 2014; Naumann et al., 2023; Rubio et al., 2022). Additionally, previous studies have not explored the combined impact of clinical and sociodemographic factors as implementation barriers (Brown et al., 2014; Rubio et al., 2022). The role of enabling factors in supporting patient implementation in BCRL is also missing in current literature. As such this study aimed to identify the level and type of patient implementation of occupational therapy treatment recommendations for BCRL and determine key barriers and enablers that influence implementation. As this was an observational study, all interventions were considered evenly in importance for implementation. It was anticipated that this research would support service delivery by improving understanding of how interventions can be tailored to patients and how clinicians can address barriers to implementation of treatment recommendations.
Methods
Study design and setting
This study utilised a retrospective cohort design and involved the extraction of data from an existing clinical dataset. The retrospective design was chosen for its efficiency in investigating outcomes associated with BCRL, which often have a longer latency period. In conducting a retrospective design, we were able determine barriers and enablers to implementation, and to potentially guide future prospective interventional studies.
The dataset included 398 patients who had received a PSM including occupational therapy and/or physiotherapy at a tertiary metropolitan hospital cancer clinic. Seventy patients received occupational therapy between January 2021 and April 2024. Reporting adheres to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement for observational studies (von Elm et al., 2007).
Participants and recruitment
Eligible participants were aged 18 years or older, had undergone breast cancer surgery, were referred for occupational therapy as part of the PSM and attended at least one cancer clinic appointment. Exclusion criteria included a metastatic disease diagnosis, chemotherapy history for other cancers, prophylactic breast surgery for BRCA gene not involving node sampling, cognitive impairment, cardiac failure, chronic renal failure and recurrent breast cancer or other cancer requiring node clearance and/or radiation within the same or adjacent lymphatic drainage basin.
Ethical considerations
This project was approved by the Sir Charles Gairdner Osborne Park Health Care Group Safety and Quality Department (QI50656) and reciprocal approval was received by the Curtin University Human Research Ethics Committee (HRE2023-0710). All patient data were de-identified and analysed in aggregate form to maintain confidentiality. As this was a retrospective audit, the need for patient written consent was waived.
Lymphoedema assessment and intervention
Diagnosis of BCRL involved clinical observations of swelling, and bioimpedance spectroscopy (BIS) circumferential arm measurements. (Dietrich et al., 2023). Patients with sub-clinical lymphoedema were involved in the study. Sub-clinical lymphoedema was defined by a (BIS) L-Dex increase of 6.5 points above pre-operative baseline and/or a unilateral volume increase from baseline of >5–10% of the affected upper limb and/or unilateral tape measure circumference increase of >0.5–2 cm (using 7 cm intervals) at two consecutive points (Koelmeyer et al., 2021; Pappalardo et al., 2021; Ridner et al., 2022). Patients were treated by two senior occupational therapists who were Australasian Lymphology Association accredited practitioners.
Occupational therapy intervention consisted of comprehensive subjective and objective assessments, leading to a personalised management plan that included treatments such as risk reduction education, self-massage education, garment schedules and donning/doffing techniques. Patients were provided with two Ready-to-Wear Class 2 garments (arm sleeve and/or hand piece), unless custom garments were needed due to body habitus, skin issues, or difficulty donning. Reassessment occurred every 4–6 weeks to monitor progress with patient discharge as clinically appropriate.
Audit tool and data variables
This study used a piloted audit form in Research Electronic Data Capture (REDCap) (Harris et al., 2019) to support data extraction from medical files in addition to information extracted from the existing clinical dataset. Data were extracted for all eligible patients supported by two research assistants and a supervisor. To ensure consistency in data extraction, 10 files were reviewed together by the research team. Variables extracted consisted of sociodemographic and clinical characteristics such as age, gender, living situation, cancer descriptors, hand dominance, BIS L-Dex measurements, lymphoedema stage and BMI at referral. Lymphoedema was classified as: stage 0 (subclinical, no visible swelling), stage I (swelling that reduces with limb elevation), stage II (persistent swelling with fibrotic changes) and stage III (severe swelling with skin changes) (International Society of Lymphology, 2020). Additional data collected included treatment received, medical history and medications. Level of function was collected and defined as independent with activities of daily living (ADL), requiring minimal assistance or moderate assistance with ADL tasks. The type and number of occupational therapy interventions were collected.
On the audit tool possible barriers to patient implementation of treatment recommendations were considered against the Person Environment Occupation Performance model and known BCRL risk factors (Bass et al., 2024; Koelmeyer et al., 2022; Liu et al., 2023; Thomis et al., 2023) with six barriers pre-identified. These were psychological, psychosocial, physical, treatment burden, education and comorbidities (resulting in 35 different items, Supplemental Appendix 1) supporting identification and categorisation of barriers during the audit. The research assistant reviewed the information in the clinical dataset and a patient’s medical record, noting any possible barriers that is, limited social supports, increased work demands, etc.
As enabling factors for BCRL have not been well described in previous literature, an open text section was included in the audit form for the research assistant to capture any enabling factors for each patient. Enabling factors were defined as anything explicitly documented in the medical records as providing support for the patient. Due to the retrospective design of this study, it was not possible to obtain participants’ direct feedback regarding the interventions or the factors that facilitated or hindered their progress. All information was therefore extracted from the patient’s medical record. Relevant details were identified within the narrative sections of the medical notes, for example, initial occupational therapy assessments that may describe whether an individual had formal supports (such as a package of care), informal supports (such as a friend visiting regularly) or lifestyle factors such as their usual level of physical activity.
Implementation was calculated as a percentage by dividing the number of implemented interventions by the number of prescribed interventions and multiplying the result by 100. Patient implementation of treatment recommendations was explored as a continuous variable and classified as ‘below optimal’ (<70%) or ‘optimal’ (⩾70%), closely aligning with the BCRL literature indicating compliance levels below 75% are associated with an increase in arm volume and progression of BCRL to more advanced stages (Armer et al., 2020). Previous patient implementation research has typically examined individual components of BCRL management that is, bandaging, skin regimes, etc., with varying definitions for implementation used (Ostby and Armer, 2015). No prior studies were identified that measured overall implementation across all therapist recommended treatments. As this study was observational in nature, all interventions were considered of equal importance, without accounting for intensity, frequency or treatment burden.
Data analysis
Descriptive data including patient demographics and clinical characteristics were reported as a mean score with standard deviation, or median and interquartile range (IQR), depending on type and distribution of the data. Categorical data were reported using frequencies and percentages. Additionally, dependent on level of implementation (<70% vs ⩾70%), groups were comparatively analysed using Chi-square tests, Fisher’s exact tests and Mann–Whitney U tests. All variables that were significant in group comparisons were entered into individual logistic regression models.
Percentage of implementation was also analysed as a continuous outcome. Univariate group comparisons were conducted using Mann–Whitney U tests for categorical variables and correlation analyses for continuous variables, with statistical significance set at p < 0.05. Variables demonstrating significant or near-significant associations were entered into individual linear regression models.
Free text enabling factors were analysed using summative content analysis, whereby key words were identified and quantified (Hsieh and Shannon, 2005); and considered in line with the Occupational Therapy Practice Framework (American Occupational Therapy Association, 2020). The qualitative content was transcribed, systematically coded and organised into thematic categories, which were then counted for quantitative analysis. Two researchers independently reviewed the data, identified semantic meaning units and generated codes. Any discrepancies were discussed until a consensus was reached.
Results
Sample characteristics
Sixty-three participants (median age: 60.0 years, IQR 47.0–70.0) were included. Two (3.2%) identified as male and two (3.2%) as Aboriginal or Torres Strait Islander. Seven (11.1%) lived in rural or regional areas and nine (14.3%) lived alone. Clinically, 54 (85.7%) participants had invasive breast cancer and five (7.9%) had triple-negative breast cancer. The most common comorbidities were hypertension (n = 11, 17.5%), hypothyroidism (n = 6, 9.5%), osteoarthritis (n = 6, 9.5%), anxiety (n = 5, 7.9%), depression (n = 4, 6.3%) and asthma (n = 4, 6.3%). Functionally, 79.4% (n = 50) were independent, 14.3% (n = 9) needed minimal assistance and 6.3% (n = 4) required moderate assistance. Five (7.9%) had formal care support, while 18 (28.6%) relied on informal support. Clinical and socio-demographic characteristics and treatment modalities are detailed in Table 1.
Sample descriptives.
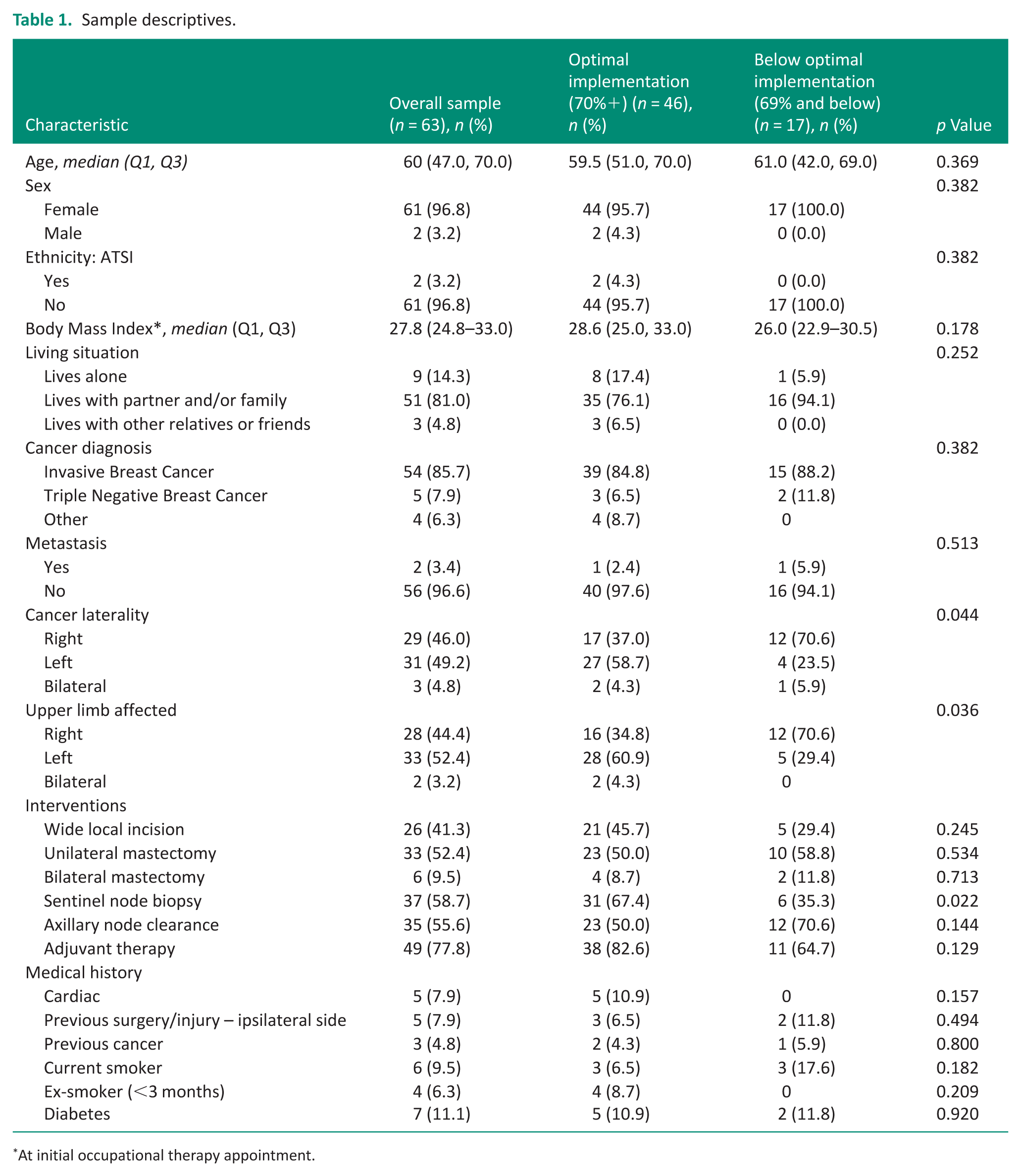
At initial occupational therapy appointment.
Level of implementation
Forty-six patients (73%) demonstrated optimal implementation of treatment recommendations (classified as adhering to 70% or more prescribed treatments), while 17 patients (27%) demonstrated below optimal implementation of treatment recommendations (classified as adhering to 69% or fewer treatments). The total number of interventions implemented was significantly different between groups (p < 0.001), with a median of five (IQR 5–6) in the optimal implementation group compared to three (IQR 2–3) in the below optimal group. Four or more interventions were implemented in 97.8% (n = 45) of the optimal implementation group compared to 23.5% (n = 4) of the below optimal group (p < 0.001).
There were no significant differences between these groups when reviewing demographic characteristics such as age, gender, supports available and living situation (Table 2). Regarding clinical factors, cancer laterality differed between groups, with right-sided cancer more common in the below optimal group (70.6% vs 37.0%, p = 0.044). However, when implementation was examined as a continuous outcome, there was no significant difference in median percentage implementation across right, left, or bilateral involvement (p = 0.422).
Barriers to patient implementation of BCRL occupational therapy treatment recommendations.
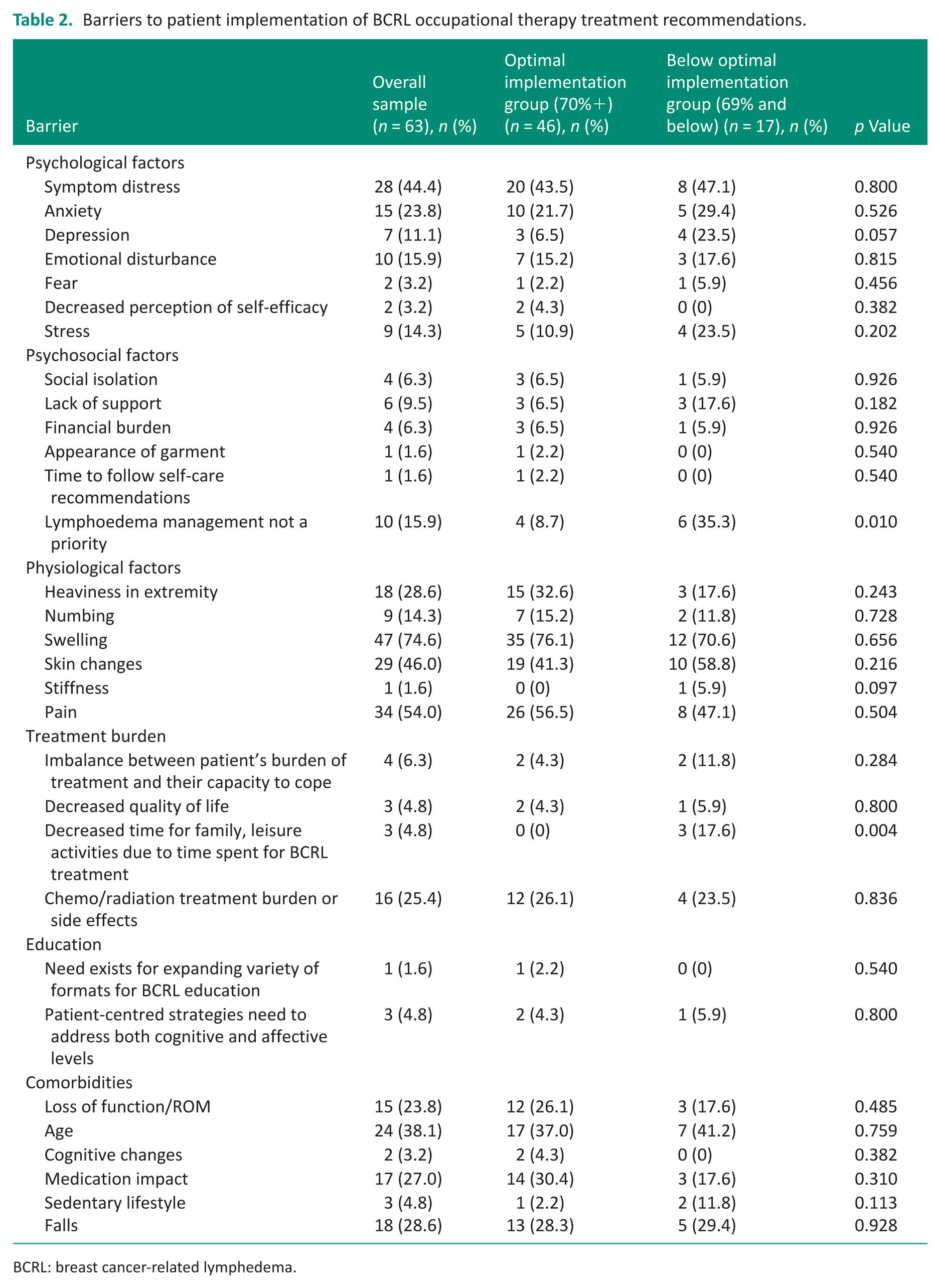
BCRL: breast cancer-related lymphedema.
Medical interventions included wide local incision, mastectomy, sentinel node biopsy and adjuvant therapy. Sentinel node biopsy was more frequent in the optimal implementation group (67.4% vs 35.3%, p = 0.022), while taxane chemotherapy was more common in the below optimal group (35.3% vs 6.5%, p = 0.004). These associations were consistent when implementation was analysed as a continuous variable: participants receiving sentinel node biopsy had higher median implementation (83.3% vs 75.0%, p = 0.024), while those receiving taxanes had lower median implementation (60.0% vs 83.3%, p = 0.030). Nicotine use was also associated with lower median implementation (60.0% vs 81.7%, p = 0.038).
There were no differences between groups regarding the types of occupational therapy lymphoedema interventions provided, the number of interventions prescribed, or the number of therapy appointments attended (Table 2). Among those whose BCRL progressed (n = 13), 76.9% (n = 10) achieved optimal implementation. Fifty patients did not experience BCRL progression with 72.0% (n = 36) demonstrating optimal implementation.
Treatment recommendations
The most common treatment recommendations provided by occupational therapists were education on the cause and nature of lymphoedema (100%, n = 63) and lymphoedema prevention and arm care (98.4%, n = 62). Sixty-one patients (96.8%) were provided with a compression garment and four (6.3%) required intensive bandaging. Other treatment recommendations included self-massage (n = 56, 88.9%), laser treatment (n = 11, 17.5%), night garmenting (n = 19, 30.2%), exercises (n = 59, 93.7%) and use of an intermittent pneumatic pump (n = 2, 3.2%). A median of six (IQR 5–7) treatment recommendations were made per patient.
Barriers to implementation
All participants (100%) encountered at least one barrier to implementing treatment recommendations, with psychological distress, physiological and psychosocial challenges, treatment burden, educational obstacles and comorbidities recognised as risk factors. Psychological factors, such as symptom distress, anxiety, emotional disturbances and stress were most common (Table 2); however, were not significantly different between groups. Three patients (4.8%) in the optimal implementation group had depression compared to four (6.3%) in the below optimal implementation group (p = 0.057). Overall, 74.6% (n = 47) experienced swelling and 54% (n = 34) pain; however, no significant differences were found between groups.
Twenty-five percent (n = 16) were identified as experiencing treatment burden. A significant difference was found between groups for a perceived reduction in family and leisure time, found by 17.6% (n = 3) in the below optimal implementation group compared to none in the optimal implementation group (p = 0.004). Additionally, there was a significant difference regarding patient’s view and prioritisation of lymphoedema management, with 35.3% (n = 6) in the below optimal group not finding this a priority compared to 8.7% (n = 4) in the optimal implementation group (p = 0.010). These factors remained when considering implementation as a continuous variable (Supplemental Appendix 2). Participants who were identified as not seeing lymphoedema management as a priority had a significantly lower median percentage of implementation than those who did not (53.6% vs 83.3%, p = 0.001). Additionally, participants who reported decreased time for family as a treatment‑burden barrier had a lower median percentage of implementation than those who did not, with this difference approaching statistical significance (60.0% vs 81.7%, p = 0.051). Education needs did not differ between groups, and there was no significant impact from confounding factors such as age, level of function and cognitive changes for example.
Enablers to implementation
Free text enabling factors were identified from the medical records and categorised into strong support network, exercise participation, motivated to return to occupation, supportive employer, health literacy and understanding of BCRL risk. Additionally previous knowledge of MLD and ability to attend appointments were also identified as enablers. Strong support network consisted of both formal and informal services. Formal services were considered as any paid services such as cleaning or childcare. Informal support was divided into partner, family, social and workplace support, where support was explicitly stated. Exercise participation encompassed any physical activity, such as gym attendance, yoga or walking. Motivated to return to occupations was noted when records explicitly stated ‘motivated’ to engage in occupation including leisure, employment, self-care and/or occupational roles including caregiver or friend. Health literacy and understanding of risk was noted when records stated that the patient was aware of treatment risks and intervention benefits (Table 3).
Enabling factors to patient implementation of BCRL occupational therapy treatment recommendations.
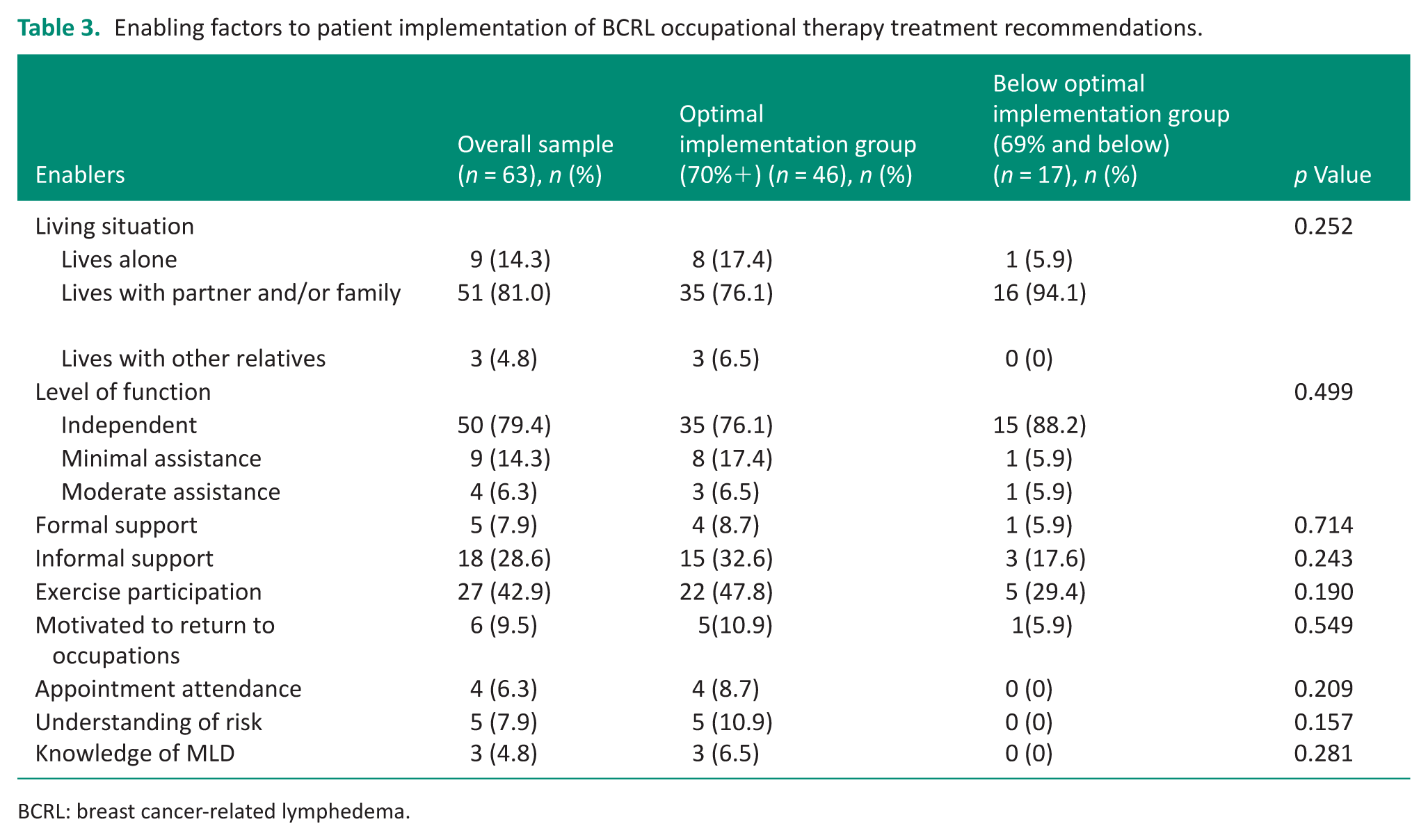
BCRL: breast cancer-related lymphedema.
While enablers did not differ significantly between optimal and below optimal groups, associations emerged when implementation was analysed continuously. Participants receiving four or more interventions had substantially higher implementation (83.3% vs 50.0%, p < 0.001), and those who understood the risks of poor lymphoedema management demonstrated higher implementation (100.0% vs 80.0%, p = 0.019).
Logistic regression modelling between groups
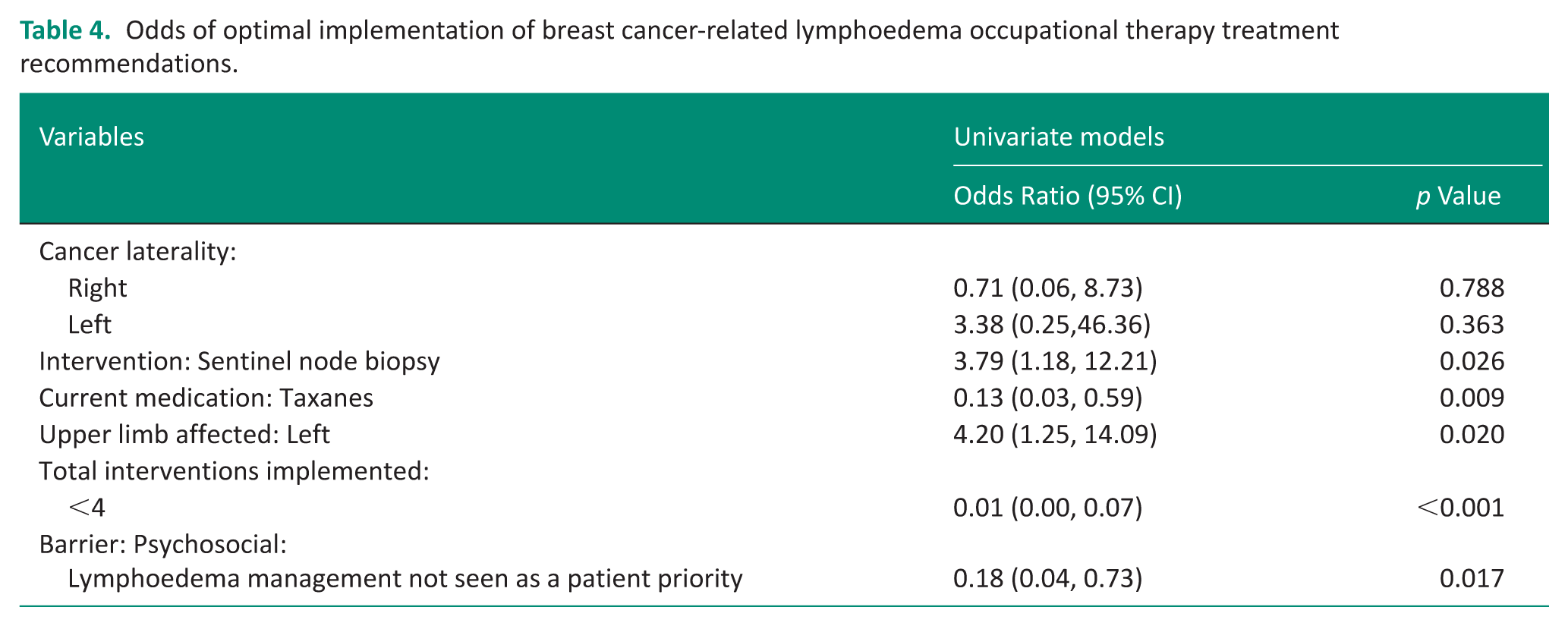
Univariate logistic regression identified several predictors of optimal implementation, including receipt of sentinel node biopsy (OR = 3.79, 95% CI 1.18–12.21, p = 0.026), taxane chemotherapy (OR = 0.13, 95% CI 0.03–0.59, p = 0.009) and left-sided upper limb involvement (OR = 4.20, 95% CI 1.25–14.09, p = 0.020). Not perceiving lymphoedema management as a patient priority was associated with reduced odds of optimal implementation (OR = 0.18, 95% CI 0.04–0.73, p = 0.017; Table 4).
Odds of optimal implementation of breast cancer-related lymphoedema occupational therapy treatment recommendations.
Linear regression treating implementation as a continuous outcome
Univariate linear regression analyses showed similar patterns (Supplemental Appendix 2). Sentinel node biopsy was positively associated with implementation (B = 11.57, 95% CI 1.77–21.36, p = 0.021), while taxane chemotherapy (B = −19.09, p = 0.006), nicotine use (B = −22.94, p = 0.012) and T2 tumour classification (B = −15.89, p = 0.006) were associated with lower implementation. Receiving four or more interventions demonstrated the strongest positive association (B = 36.99, p < 0.001). Understanding treatment risks was also positively associated (B = 18.31, p = 0.047), while decreased time for family showed a non-significant negative trend.
Discussion
This study examined patient implementation of lymphoedema treatment recommendations, focusing on barriers, enablers and the role of clinical and sociodemographic factors on implementation. Results showed that 73% of participants adhered to 70% or more of treatment recommendations, with 28.5% achieving 100% implementation. All participants faced barriers, such as psychological distress, physiological issues and treatment burden.
This study identified several factors significantly associated with optimal implementation to BCRL treatment recommendations. Sentinel node biopsy was strongly associated with implementation, with patients undergoing this procedure showing over four times greater odds of engaging with therapy. This may reflect the less invasive nature of the intervention, its association with a lower risk of lymphoedema (with one study reporting a 65% reduction compared to more invasive surgeries (Mattar et al., 2025)), and its impact on recovery trajectories. Similarly, left-sided upper limb involvement was associated with optimal implementation when examined as a dichotomous outcome. One possible explanation is that given most individuals are right hand dominant (Papadatou-Pastou et al., 2020), having the left limb affected may allow greater use of the dominant hand for self-management tasks, thereby making implementation more feasible that is, wearing a compression garment on the affected left arm. However, this association was not observed when implementation was examined as a continuous outcome and should therefore be interpreted cautiously due to the observational study design and analytic approach.
In contrast, taxane chemotherapy was linked to substantially lower implementation, likely due to its side effects that can hinder participation in rehabilitation. Psychosocial barriers also played a role, with patients who did not view lymphoedema management as a priority significantly less likely to implement treatment recommendations, highlighting the importance of patient-centred education. These findings underscore the need for tailored approaches that consider both clinical and psychosocial dimensions to improve therapy engagement.
Previous studies have reported varied implementation rates, with some finding an average implementation rate of 79% (Armer et al., 2020) and others reporting much lower rates (19.5–31%) (Alcorso et al., 2016; Brown et al., 2014).This variability likely stems from differences in how implementation is defined, measured and the cut-off points used. Some of the studies assessed only individual treatment modalities or used lower or higher thresholds to define implementation. For instance, some studies focus on specific components of self-management, such as skin care, which tends to have higher implementation rates, while others assess more complex modalities like compression garment use, or self-lymphatic drainage, which has shown lower rates of implementation. This study did not find any significant differences between the two groups in regards to wearing compression garments or completing skin care.
Earlier studies by Alcorso et al. (2016) and Brown et al. (2014) reported no significant associations between psychosocial variables, demographics or medical history and the implementation of lymphoedema interventions, with only Alcorso et al. (2016) identifying time since diagnosis as a relevant clinical factor. In contrast, our findings highlight several significant associations with implementation levels, including clinical factors such as treatment and the type of surgical intervention, as well as psychosocial barriers and treatment burden. These results suggest that both clinical and psychosocial factors may play a more substantial role in influencing implementation, underscoring the need for more nuanced and targeted intervention strategies.
Sherman and Koelmeyer (2011) emphasised that increased understanding of lymphoedema and its associated risks predicted greater engagement with treatment recommendations. Education in lymphoedema management is important to highlight how engagement in preventative strategies reduces the risk of chronic lymphoedema development. In our study, all participants received education on the cause and nature of lymphoedema, and only four reported any barriers to accessing this information. The barriers identified were the need for alternative formats of delivery, and the provided education not being tailored to participants’ cognitive abilities, rather than there being a lack of education made available. These findings can support the ongoing refinement of the education, and the process currently used.
Patients included in this study were participating in a PSM to manage BCRL. Although not the primary aim of this study, we can note that out of 398 patients, 17.6% (n = 70) required occupational therapy for treatment of sub-clinical lymphoedema. Additionally, our study found that the level of psychological distress within the participant population was 30.2%, approximately double that of the wider Australian population, which is reported at 15.4% (Australian Bureau of Statistics, 2023). While this did not produce statistical significance in terms of implementation, the high percentage of psychological distress amongst the BCRL population indicates the continued need for holistic healthcare that addresses both physical and psychological barriers.
Clinical implications and future research
Early intervention and preventative care are important to reduce incidence of chronic lymphoedema which has significant impacts on the patient and the health care system. Previous research has found sub-optimal levels of patient implementation of treatment recommendations in lymphoedema management. As such this study had been important to consider a wide range of factors that can impact on patient implementation of treatment recommendations. Therapists can use this information to better tailor and support patient care. However, future prospective studies using more granular implementation metrics would allow for a more nuanced understanding of implementation patterns. Future research could also explore if intensity, time demands or complexity of treatment recommendations impact on patient implementation.
Importantly, the study found that patients experiencing greater treatment burden were less likely to implement recommended strategies, highlighting the necessity of balancing therapeutic demands with quality of life considerations. Occupational therapists play a critical role in this process, particularly in addressing barriers and leveraging enablers within the environmental context and resources domain. By adapting treatment recommendations to align with patient characteristics and capacities, therapists may enhance implementation and potentially reduce healthcare costs through more effective management of BCRL.
Limitations
The interpretation of findings in this study was subject to several limitations. First, the reliance on medical records introduced variability due to differences in documentation and interpretation. To mitigate bias, an audit tool was developed and piloted, data extraction was conducted collaboratively by three co-investigators, and inter-rater reliability was established through joint auditing of ten files with supervisory oversight. Nevertheless, enabling factors were drawn from free text entries, which depended on what therapists recorded at the time and may not fully capture all enablers experienced by patients. The findings are descriptive and a more robust approach would involve collecting data directly from patients during treatment sessions through structured interviews or surveys, which could be considered in future research. Another key limitation of this study is that the implementation outcome does not differentiate between types of recommendations or account for their relative intensity or burden. As such, it provides only a crude approximation of patient engagement. This limits the extent to which clinical inferences can be drawn regarding the comparative difficulty or uptake of specific interventions. A key methodological limitation is that the analysis was restricted to univariable regression due to insufficient predictors for a multivariable model, limiting our ability to adjust for confounding. This study also has a small sample size and was completed at a single site, reducing generalisability.
Conclusion
This observational study has found that receiving sentinel node biopsy surgery and patient understanding of the risks of poor lymphoedema management are associated with higher implementation of lymphoedema treatment recommendations. Taxane chemotherapy, nicotine use, T2 tumour classification and patients not viewing lymphoedema management as a priority were associated with lower implementation. While laterality was associated with optimal implementation in dichotomous analyses, this finding was not consistent across analytic approaches and should be interpreted cautiously. Overall, this study highlights the need for individualised treatment plans addressing patient specific barriers and enablers which may lead to more effective symptom management and limit the progression of BCRL.
Key findings
73% implemented >70% of therapy BCRL recommendations.
Implementation was associated with sentinel node biopsy and understanding risk.
Taxanes, nicotine use, T2 tumours and psychosocial barriers reduced implementation.
What this study has added
This study explores clinical and psychosocial factors influencing patient implementation of occupational therapy treatment recommendations in lymphoedema management, providing evidence to guide tailored care.
Supplemental Material
sj-docx-1-bjo-10.1177_03080226261454919 – Supplemental material for How can occupational therapists support patient implementation of lymphoedema treatment recommendations? A retrospective cohort study
Supplemental material, sj-docx-1-bjo-10.1177_03080226261454919 for How can occupational therapists support patient implementation of lymphoedema treatment recommendations? A retrospective cohort study by Susie Veart, Erryn Siva, Caitlin Beck, Eliza Briggs, Indi Rogers, Simone Priestly, Angela Jacques and Kristie Harper in British Journal of Occupational Therapy
Supplemental Material
sj-docx-2-bjo-10.1177_03080226261454919 – Supplemental material for How can occupational therapists support patient implementation of lymphoedema treatment recommendations? A retrospective cohort study
Supplemental material, sj-docx-2-bjo-10.1177_03080226261454919 for How can occupational therapists support patient implementation of lymphoedema treatment recommendations? A retrospective cohort study by Susie Veart, Erryn Siva, Caitlin Beck, Eliza Briggs, Indi Rogers, Simone Priestly, Angela Jacques and Kristie Harper in British Journal of Occupational Therapy
Footnotes
Ethical considerations
This project was approved by the Sir Charles Gairdner Osborne Park Health Care Group Safety and Quality Department (QI50656) and deemed to be of minimal risk as per the National Statement on Ethical Conduct in Human Research. Reciprocal approval was received by the Curtin University Human Research Ethics Committee (HRE2023-0710). All patient data were de-identified and analysed in aggregate form to maintain confidentiality.
Consent to participate
As this was a retrospective audit, the need for patient written consent was waived.
Author contributions
EB, IR, SP, CB, ES, SV and KH contributed to the design and implementation of this retrospective audit, including gaining research approvals and supporting data extraction. AJ, EB, IR, SP supported data analysis. All authors have contributed to reviewing the findings and write-up.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research was funded by a Charlies Foundation for Research Bright Ideas Grant.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Patient and public involvement data
During the development, progress and reporting of the submitted research, patient and public involvement in the research was not included at any stage of the research as it was a retrospective audit.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.