
Abstract
This study longitudinally examined the associations between paretic upper limb use, upper limb motor function, and Internal Health Locus of Control (IHLC) in hospitalised patients with subacute stroke. Forty patients were assessed using the Motor Activity Log–Amount of Use, the Fugl–Meyer Assessment-Upper Extremity, and IHLC. Hierarchical multiple regression analyses showed that paretic upper limb use was associated with motor function at both 1 and 2 months, whereas no association with IHLC was observed. Secondary (exploratory) analyses suggested that depressive symptoms, self-efficacy, and activities of daily living independence may differ according to the degree of improvement in paretic upper limb use.
Introduction
Stroke is a major global health problem. In 2019, approximately 12.2 million people were estimated to have experienced stroke worldwide (GBD 2019 Stroke Collaborators, 2021). It has been reported that more than 85% of people with post-stroke hemiparesis have residual upper limb impairment (Geddes et al., 1996). Consequently, many patients experience difficulties due to impaired motor function of the paretic upper limb. Such impairments are known to have substantial impacts on Activities of Daily Living (ADL) and Quality Of Life (QOL; Chen et al., 2015; Nichols-Larsen et al., 2005).
The frequency of paretic upper limb use is usually related to motor function. However, in some patients, this relationship is not observed. This has been attributed to learned nonuse, whereby reliance on the non-paretic upper limb becomes habitual and the use of the paretic upper limb remains restricted even after recovery of motor function (Taub et al., 2006).
Constraint-induced movement therapy (CIMT) has been proposed as an effective approach to learned nonuse, and has been reported to increase paretic upper limb use (Van der Lee et al., 1999). CIMT is grounded in behavioural mechanisms, including enhancing motivation to use the paretic upper limb (Taub et al., 2002). Nevertheless, psychological factors that promote paretic upper limb use have not been fully elucidated (Kwakkel et al., 2015).
In this context, health locus of control (HLC) has attracted attention. HLC is a psychological framework describing beliefs about the extent to which health outcomes are controllable through one’s own actions (Wallston et al., 1976). Among HLC dimensions, internal health locus of control (IHLC) reflects a tendency to believe that one’s own behaviour directly affects health outcomes. Individuals with higher IHLC are known to engage more actively in health behaviours (Bonetti and Johnston, 2008). IHLC has been associated with improved medication adherence (Náfrádi et al., 2017) and with continued attendance at physiotherapy among patients with musculoskeletal conditions (Wahl et al., 2018). In stroke populations, IHLC has been suggested to be associated with QOL (Van Mierlo et al., 2014) and ADL (Rapolienė et al., 2018). However, previous research has not clearly demonstrated an association between IHLC and the frequency of paretic upper limb use. Based on this background, we hypothesised that IHLC, reflecting a tendency to take proactive action regarding one’s health, may be associated with the frequency of paretic upper limb use.
The aim of this study was to clarify the associations between the frequency of paretic upper limb use and both upper limb motor function and IHLC in patients with subacute stroke during inpatient rehabilitation. In addition, to further understand background factors related to paretic upper limb use, we secondarily evaluated depressive symptoms using the Self-rating Depression Scale (SDS; Fukuda & Kobayashi, 1973; Zung, 1965), self-efficacy using the General Self-Efficacy Scale (GSES; Bandura, 1977; Sakano and Tohjoh, 1986), and ADL independence using the Functional Independence Measure (FIM; Chino, 1991; Granger et al., 1986; Okawa et al., 1994).
The findings of this study are expected to contribute to occupational therapy practice aimed at preventing learned nonuse and supporting improvements in the frequency of paretic upper limb use.
Methods
Study design
This study employed a longitudinal study design.
Participants
Participants were recruited from nine rehabilitation hospitals located in the metropolitan area of Japan between February 2023 and March 2024.
Inclusion criteria
Participants were eligible if they met all of the following criteria:
(1) adults aged 18 years or older;
(2) receiving 40–60 minutes each of physical therapy and occupational therapy per day;
(3) hemiparesis due to cerebral infarction or intracerebral haemorrhage and within 6 months post-stroke;
(4) permission to use the paretic hand in daily life and no institutional rules restricting upper limb use;
(5) Brunnstrom recovery stage II or higher for the upper limb (Brunnstrom, 1966);
(6) preserved cognitive function, defined as the Mini-Mental State Examination–Japanese version (MMSE-J) ⩾ 24 (Sugishita et al., 2016) or the Revised Hasegawa’s Dementia Scale (HDS-R) ⩾ 20 (Kato et al., 1991);
(7) absence of severe aphasia and ability to complete questionnaires independently.
Exclusion criteria
Participants were excluded if they met any of the following criteria:
(1) Brunnstrom recovery stage I for the upper limb;
(2) MMSE-J ⩽ 23 or HDS-R ⩽ 19;
(3) Severe aphasia and inability to complete questionnaires independently;
(4) Upper limb movement restrictions due to other physical factors, such as orthopaedic conditions.
Data collection
Occupational therapists at each hospital participated as research collaborators. To minimise variability in assessment procedures, the principal investigator provided standardisation training for the evaluation methods either online or in person. Assessments were conducted at three time points: baseline, 1, and 2 months.
Measures included the Motor Activity Log-Amount of Use (MAL-AOU) as an index of paretic upper limb use (Takahashi et al., 2009; Uswatte et al., 2005); IHLC (Horike, 1991; Wallston et al., 1976); upper limb motor function using the Fugl–Meyer Assessment-Upper Extremity (FMA-UE) (Fugl-Meyer et al., 1975); depressive symptoms using the SDS (Fukuda & Kobayashi, 1973; Zung, 1965); self-efficacy using the GSES (Bandura, 1977; Sakano and Tohjoh, 1986); and ADL independence using the FIM (Chino, 1991; Granger et al., 1986; Okawa et al., 1994). Demographic and clinical information (age, sex, premorbid dominant hand, side of paresis, diagnosis, and time since stroke onset) was collected from medical records.
Measures
Motor activity log
The MAL is a self-report measure assessing the frequency and quality of paretic upper limb use in daily life (Uswatte et al., 2005). We used the Japanese version, which has demonstrated reliability and validity (Takahashi et al., 2009). Fourteen daily activities (e.g. eating, grooming, dressing, and moving objects) are rated on a 6-point scale from 0 (“does not use at all”) to 5 (“uses as much as the non-paretic limb”). Higher scores indicate more frequent and higher-quality use. In this study, only the Amount of Use score was used (MAL-AOU). The minimal detectable change (MDC) for MAL-AOU is 0.84 (Chen et al., 2012). The omega coefficient for MAL-AOU in this study was 0.81.
Japan Health Locus of Control scale
HLC is a self-report scale assessing beliefs regarding control over health (Wallston et al., 1976). We used the validated Japanese version, the Japan Health Locus of Control scale (Horike, 1991). The scale comprises 25 items across 5 factors (“Internal,” “Family,” “Professional,” “Chance,” and “Supernatural”), with 5 items per factor. Each item is rated on a 6-point scale from 1 (“strongly disagree”) to 6 (“strongly agree”). Higher scores indicate stronger attribution to that factor. In this study, only the internal factor score was used as IHLC. The omega coefficient for IHLC in this study was 0.81.
Fugl–Meyer assessment
The FMA is a clinician-administered measure that quantifies motor impairment after stroke (Fugl-Meyer et al., 1975) and has established reliability and validity (Gladstone et al., 2002). We assessed 33 upper limb items (FMA-UE). The maximum score is 66 points, comprising shoulder/elbow/forearm (36 points), wrist (10 points), hand (14 points), and coordination/speed (6 points). Higher scores indicate better upper limb motor function. The omega coefficient for FMA-UE in this study was 0.78.
Self-rating depression scale
The SDS is a self-report measure of depressive symptoms (Zung, 1965). We used the validated Japanese version (Fukuda & Kobayashi, 1973). It consists of 20 items covering domains such as depressed mood, diurnal variation, crying spells, sleep disturbance, appetite, and libido. Items are rated on a 4-point scale from “a little of the time” to “most of the time,” with higher scores indicating more severe depressive symptoms. Scores of ⩾40 indicate mild depression and ⩾50 indicate moderate depression. The omega coefficient for the SDS in this study was 0.86.
General self-efficacy scale
The GSES is a self-report measure of general self-efficacy based on Bandura’s theory (Bandura, 1977) and was administered using the validated Japanese version (Sakano and Tohjoh, 1986). It comprises 16 items, answered as “yes” or “no,” and yields a total score; higher scores indicate greater self-efficacy. The omega coefficient for the GSES in this study was 0.79.
Functional independence measure
The FIM is a clinician-rated measure of ADL independence (Granger et al., 1986). The Japanese version has been developed (Chino, 1991) and its reliability and validity have been established (Okawa et al., 1994). The scale comprises 18 items: 13 motor items (e.g. self-care, toileting, transfers, locomotion) and 5 cognitive items (communication and social cognition). Each item is rated from 1 to 7 based on actual performance, with a maximum total of 126. Higher scores indicate greater independence. In this study, we used only the motor items (FIM-M). The omega coefficient for FIM-M in this study was 0.73.
Statistical analysis
MAL-AOU was defined as the primary outcome and IHLC as the primary explanatory variable. SDS, GSES, and FIM-M were analysed as secondary (exploratory) outcomes. Values of MAL-AOU, IHLC, FMA-UE, SDS, GSES, and FIM-M at 1 and 2 months were used for the main analyses.
Participants were divided into a higher MDC group and a lower MDC group based on whether the change in MAL-AOU exceeded the MDC (=0.84). Group comparisons were performed using analysis of covariance (ANCOVA), adjusting for baseline values as covariates. In addition, mediation analyses were conducted using hierarchical multiple regression, with FMA-UE as the independent variable, MAL-AOU as the dependent variable, and IHLC as the mediator. To account for potential non-normality and the small sample size, bias-corrected and accelerated (BCa) bootstrapping with 5000 resamples was performed (Hiraga and Hayashi, 2022). Statistical significance was set at 5%, and effects were considered statistically significant when the 95% confidence interval (CI) did not include 0. IBM SPSS Statistics (version 28.0; IBM Corp., Armonk, NY, USA) was used for all analyses. Effect sizes for ANCOVA were reported as partial η2. For mediation analyses, model explanatory power was reported as R2 and adjusted R2.
Ethical considerations
This study was approved by the Research Ethics Committee of Kanagawa University of Human Services (approval number: 5-22-25; approval date: 30 September 2022). All participants received a full explanation of the study purpose and procedures and provided written informed consent. All study procedures were conducted in accordance with the ethical principles of the Declaration of Helsinki. Data were anonymised to prevent identification of individuals and were stored securely for analysis.
Results
Table 1 presents baseline demographic characteristics and the mean (standard deviation) values of each outcome at 1 and 2 months, stratified by the MDC (=0.84) of MAL-AOU (Takahashi et al., 2009; Uswatte et al., 2005). Forty patients consented to participate and all completed the baseline assessment. At 1 month, all participants remained hospitalized, and no missing data were observed. At 2 months, 14 participants had been discharged; therefore, analyses were conducted on the remaining 26 participants.
Subgroup characteristics at 1 and 2 months based on baseline characteristics and change in MAL-AOU (Minimum detectable change).
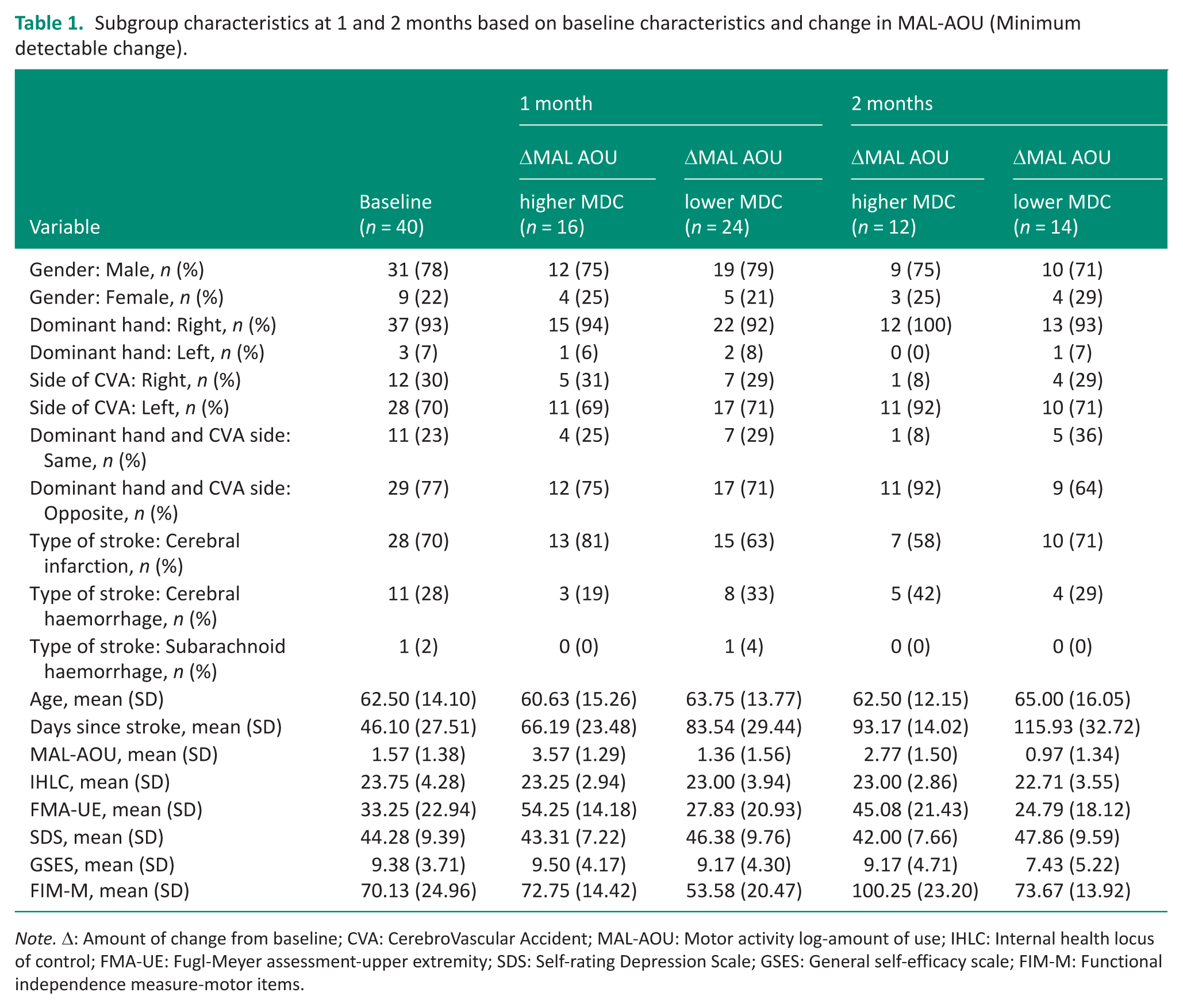
Note. Δ: Amount of change from baseline; CVA: CerebroVascular Accident; MAL-AOU: Motor activity log-amount of use; IHLC: Internal health locus of control; FMA-UE: Fugl-Meyer assessment-upper extremity; SDS: Self-rating Depression Scale; GSES: General self-efficacy scale; FIM-M: Functional independence measure-motor items.
Table 2 shows ANCOVA results comparing the higher MDC and lower MDC groups based on changes in MAL-AOU. MAL-AOU differed significantly between groups at both 1 and 2 months (both p < 0.01), supporting the validity of the group classification. IHLC (Horike, 1991; Wallston et al., 1976) did not significantly differ between groups at either 1 month (F = 2.41, p = 0.13, partial η2 = 0.06, 95% BCa CI −3.34 to 0.04) or 2 months (F = 0.40, p = 0.53, partial η2 = 0.02, 95% BCa CI −3.25 to 1.34).
Results of ANCOVA comparing the improvement and non-improvement groups.
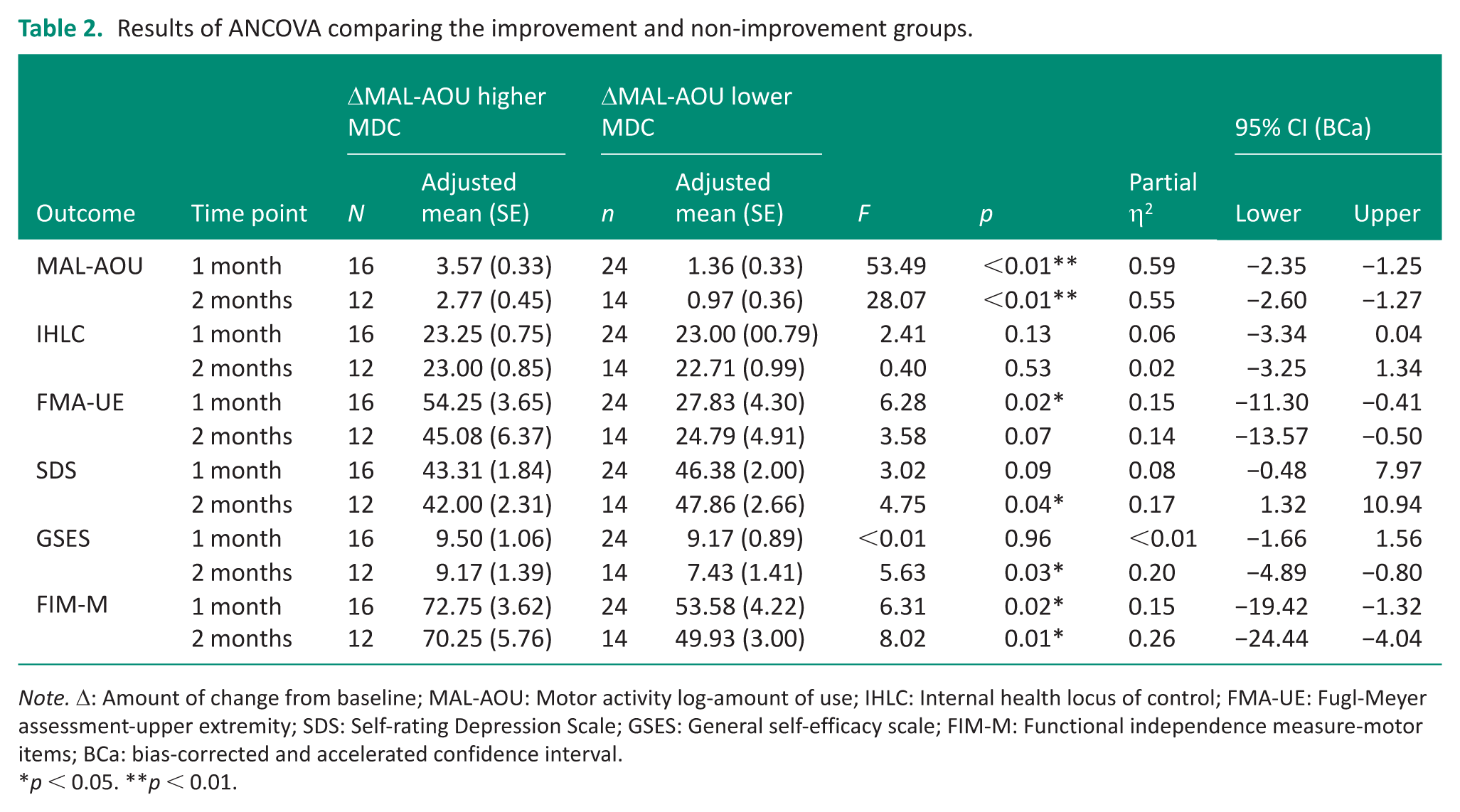
Note. Δ: Amount of change from baseline; MAL-AOU: Motor activity log-amount of use; IHLC: Internal health locus of control; FMA-UE: Fugl-Meyer assessment-upper extremity; SDS: Self-rating Depression Scale; GSES: General self-efficacy scale; FIM-M: Functional independence measure-motor items; BCa: bias-corrected and accelerated confidence interval.
*p < 0.05. **p < 0.01.
FMA-UE (Fugl-Meyer et al., 1975) was significantly higher in the higher MDC group at 1 month (F = 6.28, p = 0.02, partial η2 = 0.15, 95% BCa CI −11.30 to −0.41). At 2 months, the difference did not reach statistical significance (F = 3.58, p = 0.07, partial η2 = 0.14, 95% BCa CI −13.57 to −0.50).
For secondary outcomes, significant group differences were observed at 2 months. The SDS (Fukuda & Kobayashi, 1973; Zung, 1965) score was significantly higher in the lower MDC group (F = 4.75, p = 0.04, partial η2 = 0.17, 95% BCa CI 1.32 to 10.94). In contrast, the GSES (Bandura, 1977; Sakano and Tohjoh, 1986) score was significantly higher in the higher MDC group (F = 5.63, p = 0.03, partial η2 = 0.20, 95% BCa CI −4.89 to −0.80). FIM-M (Granger et al., 1986) was significantly higher in the higher MDC group at both 1 month (F = 6.31, p = 0.02, partial η2 = 0.15, 95% BCa CI −19.42 to −1.32) and 2 months (F = 8.02, p = 0.01, partial η2 = 0.26, 95% BCa CI −24.44 to −4.04).
Table 3 presents results of hierarchical multiple regression analyses with BCa bootstrapping (5,000 resamples) examining whether IHLC mediated the association between FMA-UE and MAL-AOU. At 1 month, FMA-UE showed a significant direct effect on MAL-AOU (β = 0.81, p < 0.01, 95% BCa CI 0.03 to 0.09). In contrast, IHLC was not significantly associated with MAL-AOU (β = 0.13, p = 0.15, 95% BCa CI −0.04 to 0.15), and no mediation effect was observed. At 2 months, FMA-UE remained a significant predictor of MAL-AOU (β = 0.61, p = 0.02, 95% BCa CI 0.01 to 0.08), whereas IHLC did not show a statistically significant association with MAL-AOU (β = 0.21, p = 0.05, 95% BCa CI −0.01 to 0.21). The 2-month model showed high explanatory power (R2 = .90, adjusted R2 = .87).
Mediating effect of IHLC on the relationship between FMA-UE and MAL-AOU (Hierarchical multiple regression analysis).
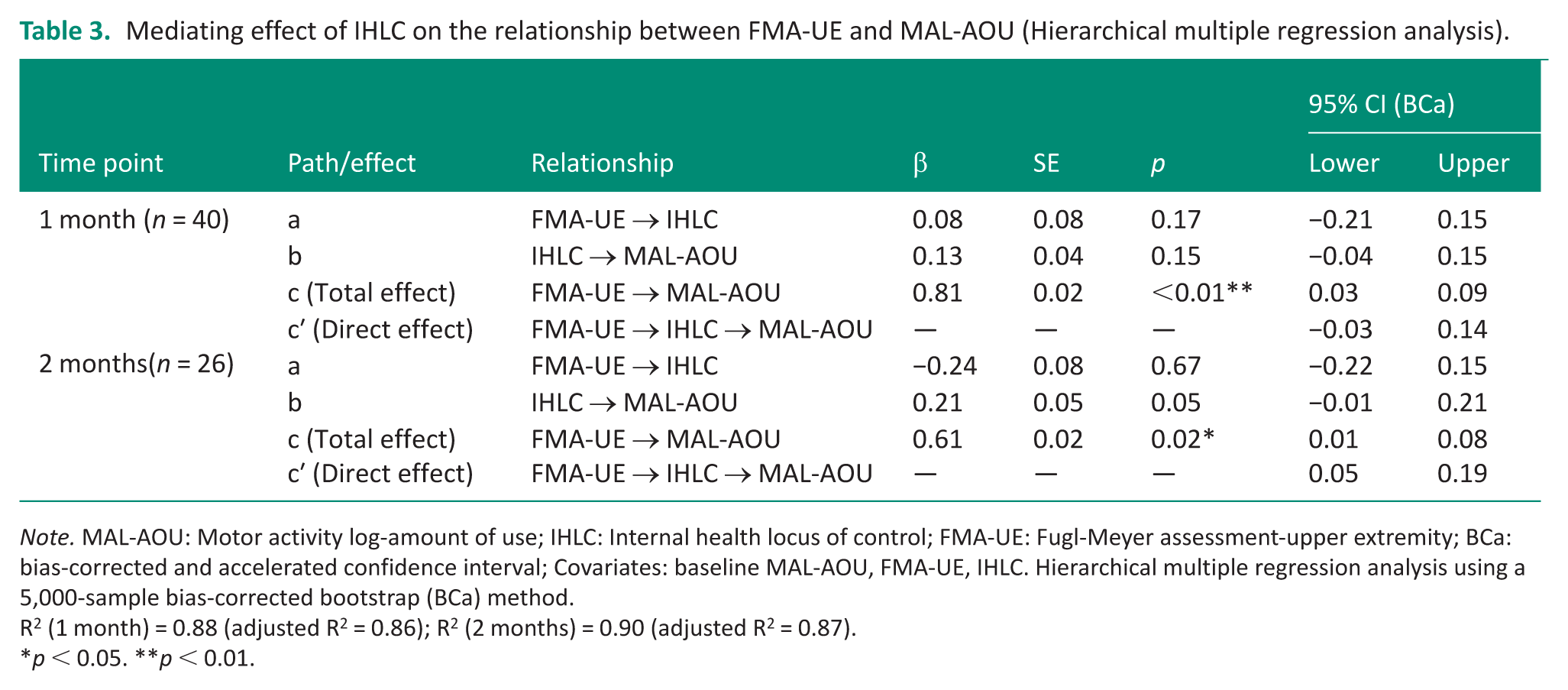
Note. MAL-AOU: Motor activity log-amount of use; IHLC: Internal health locus of control; FMA-UE: Fugl-Meyer assessment-upper extremity; BCa: bias-corrected and accelerated confidence interval; Covariates: baseline MAL-AOU, FMA-UE, IHLC. Hierarchical multiple regression analysis using a 5,000-sample bias-corrected bootstrap (BCa) method.
R2 (1 month) = 0.88 (adjusted R2 = 0.86); R2 (2 months) = 0.90 (adjusted R2 = 0.87).
*p < 0.05. **p < 0.01.
Discussion
This study aimed to examine longitudinal associations between the frequency of paretic upper limb use and both upper limb motor function and IHLC in patients with subacute stroke during inpatient rehabilitation. MAL-AOU (Takahashi et al., 2009; Uswatte et al., 2005) was consistently associated with FMA-UE (Fugl-Meyer et al., 1975) at both 1 and 2 months, suggesting that motor function may be a consistently important factor for understanding real-world paretic upper limb use during the subacute phase.
This finding is consistent with previous studies reporting a close relationship between upper limb function and actual arm use in subacute stroke populations (Chen et al., 2023; Hirayama et al., 2023), and supports the view that a certain level of motor function may be a prerequisite for using the paretic upper limb in everyday life.
Although IHLC (Wallston et al., 1976) has been reported to be associated with QOL and ADL independence (Rapolienė et al., 2018; Van Mierlo et al., 2014), we hypothesised that IHLC might also be associated with MAL-AOU. However, IHLC did not show a significant association with MAL-AOU either directly or as a mediator (Table 3). These results suggest that, under the conditions of inpatient rehabilitation during the subacute phase, IHLC may not be associated with the frequency of paretic upper limb use.
Several interpretations are possible. First, MAL-AOU is a subjective, self-reported measure that reflects how individuals perceive their paretic upper limb use in daily life. Previous research using accelerometry has shown that self-reported arm use does not necessarily correspond with objectively measured arm use after stroke (Rand et al., 2011). Second, it has been suggested that locus of control beliefs may be less strongly related to adjustment when behaviour is not under the individual’s discretion (Wolk, 1976). Similarly, within the theory of planned behaviour, when behaviour is not under sufficient volitional control, the association between beliefs or intentions and actual behaviour is expected to weaken (Ajzen, 1991). In inpatient settings, routines and safety regulations may constrain behavioural choices; therefore, paretic upper limb use may not be determined solely by the individual’s decisions. These factors together may explain why IHLC did not manifest as a predictor of paretic upper limb use in this inpatient subacute context. Future studies should incorporate objective measures such as accelerometry and integrate both the quantity of use and individuals’ perceptions of use, and should examine designs that include environments with greater behavioural choice, such as community or home settings.
In relation to the secondary (exploratory) outcomes, the observed group differences reported in the Results section suggest that depressive symptoms, self-efficacy, and ADL independence may vary between patients who achieve clinically meaningful improvements in upper limb use and those who do not, and that such differences may be more apparent after some time has elapsed rather than in the early phase. However, these results arise from secondary (exploratory) analyses based on MDC-defined group comparisons and do not indicate that depressive symptoms, self-efficacy, or ADL independence causally determine improvements in paretic upper limb use.
Overall, the present findings reaffirm that motor function and its recovery are important for understanding and promoting paretic upper limb use. In addition, assessing depressive symptoms, self-efficacy, and ADL independence alongside motor function may contribute to a more comprehensive understanding of paretic upper limb use during the subacute phase. In this inpatient subacute context, IHLC was not associated with paretic upper limb use. These results indicate that, at least under the assessment methods and environmental conditions used in this study, IHLC may not be related to the frequency of paretic upper limb use. Future research should examine the relationship between IHLC and paretic upper limb use more precisely by incorporating objective measures such as accelerometry and study designs that include environments with greater behavioural choice, such as home or community settings. In addition, larger longitudinal and intervention studies are warranted to clarify how psychological factors, including depressive symptoms and self-efficacy, interact with motor function to influence real-world upper limb use after stroke.
Limitations
At the 2-month assessment, some participants had been discharged and could not be followed up, resulting in a relatively small sample size. In addition, as an observational study, this research cannot directly demonstrate causal relationships. Furthermore, because the same occupational therapists conducted both assessments and treatment, the influence of assessor bias cannot be excluded. Finally, group comparisons for secondary (exploratory) outcomes were conducted, and the interpretation of these results should be made with caution.
Summary
This study suggests that upper limb motor function may be a factor consistently associated with the frequency of paretic upper limb use in hospitalised patients with subacute stroke. In contrast, IHLC was not associated with paretic upper limb use under the conditions of subjective assessment and inpatient rehabilitation during the subacute phase. These findings indicate that, at least under the assessment methods and environmental conditions used in this study, the relationship between paretic upper limb use and IHLC was not clearly demonstrated. In addition, secondary (exploratory) analyses suggested that depressive symptoms, self-efficacy, and ADL independence may differ according to the degree of improvement in paretic upper limb use. Future studies using objective measures such as accelerometry and designs that include living environments with different degrees of behavioural choice are needed to further examine the relationships that were not observed in the present study.
Key findings
In hospitalised patients with subacute stroke, the MAL-AOU was significantly associated with FMA-UE at both 1 and 2 months.
IHLC did not show an association with the frequency of MAL-AOU at either time point.
Secondary (exploratory) analyses identified group differences at 2 months in SDS, GSES, and FIM-M based on the MDC of MAL-AOU.
New knowledge from this study
In hospitalised patients with subacute stroke, IHLC was not associated with subjectively assessed paretic upper limb use, whereas paretic upper limb use was consistently associated with upper limb motor function.
Footnotes
Acknowledgements
We would like to thank the patients and therapists who participated in this study.
Ethical considerations
The study was approved by the ethics committee at the Kanagawa University of Human Services in 2022 (No. 5-22-25).
Consent to participate
We explained the research contents in writing and orally. Those individuals who consented to participate were included in the study.
Author contributions
S.H. and S.S.: conceived the study and planned the research design. S.H.: analysed and interpreted the data. S.H.: contributed reagents/materials/analysis tools. S.H.: drafted the manuscript. All authors contributed to the article and approved the submitted version.
Funding
The authors declared no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Patient and public involvement data
In the course of the development, progression, and reporting of the submitted study, patients to the study were included only in the conduct of the study.