
Abstract
Background:
Occupational therapy remains a predominantly female profession in the United Kingdom (UK) and the United States (US). This study explored the lived experiences of male occupational therapy students and practitioners to understand gender-related dynamics in education and practice
Method:
A qualitative phenomenological mixed-methods design was used. Open-ended responses underwent reflexive thematic analysis, while Likert-scale data were analysed descriptively (means, standard deviations) to support interpretation of findings. No inferential analyses were conducted.
Results:
Participants consistently perceived occupational therapy as a predominantly female profession. Themes included social isolation, stereotyping, and gendered expectations during academic preparation and early career stages. While some reported perceived advantages in visibility and leadership opportunities, these benefits were inconsistent. Mentorship and role models emerged as critical for fostering inclusion.
Conclusion:
Gender imbalance in occupational therapy shapes experiences of belonging, identity, and progression. Findings underscore the need for gender-awareness training, inclusive curricula, and structured mentorship to support male recruitment and retention in the profession.
Keywords
Introduction
Occupational therapy is a holistic, client‑centred profession that supports individuals in engaging in meaningful activities across diverse settings. Despite this inclusive foundation, the profession remains predominantly female worldwide, a pattern that affects workforce diversity and may shape client experiences. Prior research, including Maxim and Rice (2017), has examined men’s perceptions and representation within occupational therapy. Building on this work, the present study explores the lived experiences of male students and practitioners in the United Kingdom (UK) and the United States (US). Although the study focuses on these two countries, the issue has global relevance, as gender imbalance in occupational therapy is well documented internationally (Karaba Bäckström et al., 2023). By adapting and expanding tools used in earlier research, this study integrates structured survey responses with personal accounts to offer deeper insight into factors influencing gender equity in the profession.
Men comprise 8% of the occupational therapy workforce in the UK (Health and Care Professions Council, 2024) and 7.8% in the US (American Occupational Therapy Association, 2023). Similar trends are seen in other predominantly female health professions, including nursing (Prosen and Čekada, 2025) and speech‑language therapy (Campos, et al., 2018). Although diversity initiatives exist, the inclusion of male therapists and students is often overlooked (Bohn et al., 2019; Craik et al., 2001; Zelin et al., 2022).
Men in predominantly female professions may encounter both advantages and challenges. They are sometimes perceived as benefiting from higher salaries, faster promotions, or increased visibility (Michaels, 2023; Son Hing et al., 2023). These assumptions reflect broader societal beliefs that caregiving roles lack prestige and do not align with traditional masculine norms (Gul and Uskul, 2019). Compared with fields such as construction, law, finance, or technology, occupational therapy is occasionally viewed as lower in status or financial reward (Beagan and Fredericks, 2018). However, such assumptions do not always align with the experiences of male therapists. Many report high job satisfaction not because of their gender, but because of their professional roles and work environments, indicating that satisfaction is influenced more by individual and occupational factors than by gender alone (Maxim and Rice, 2017).
Leadership roles may offer opportunities but can also increase scrutiny and reduce patient contact (Beagan and Fredericks, 2018). A Brazilian study found that male OT and OTA practitioners recognised that gender‑based advantages, such as preferential hiring or assumptions of leadership potential, can exist within the profession. However, these advantages were not consistently experienced by all male therapists, reflecting variation in how gender dynamics are perceived and enacted across contexts (Ferreira and de Almeida, 2022). Similar findings in nursing show that men may advance quickly but also face stereotypes and periods of social isolation, particularly during training and early practice (Smith et al., 2021). Bohn et al. (2019) suggested that social isolation, such as feeling like an outsider, lacking same‑gender peers or mentors, and having fewer opportunities for informal connection, can diminish a male practitioner’s sense of belonging in the workplace.
Stereotypes tied to masculine traits can influence how male therapists are perceived (Ferreira and de Almeida, 2022), and limited recognition of gender norms within client interactions may contribute to feelings of invisibility. A gendered norm is a socially shared expectation about how individuals should behave based on their gender. Assumptions that women are inherently more empathetic or better suited to certain practice areas, while men are expected to handle physically demanding clients, reinforce traditional gender expectations and can affect both assignments and workplace relationships. When these expectations go unaddressed, male therapists may feel overlooked or disconnected within predominantly female professional environments.
Male students and therapists may encounter discomfort from patients during intimate care tasks or face stereotypes in educational and clinical settings (Colaianni et al., 2022). Research confirms that these issues, client engagement barriers, gender stereotyping, social isolation, lack of peer and mentor support, and inconsistent career advancement, are common across other predominantly female professions such as nursing and speech-language therapy (Adeyemi-Adelanwa et al., 2016; Birioukova and Barker, 2021). Gendered behaviour in occupational therapy often manifests through unconscious practices known as “doing gender,” where therapists’ assessments are shaped by stereotypes, for instance, emphasising domestic roles with female clients and employment with male clients (Liedberg et al., 2010). These patterns intersect with the therapist’s own gender, as research shows that many female clients and some male clients prefer female therapists due to perceived relational strengths and shared experiences, a phenomenon Skeggs (2014) describes as “feminine cultural capital.”
Feminine cultural capital refers to interpersonal qualities culturally associated with femininity, such as empathy, emotional attunement, and relational competence, which carry value in practice settings (Skeggs, 2014). In occupational therapy, these attributes are often viewed as advantageous and contribute to some clients’ preference for female therapists (Schweitzer et al., 2024). This concept also aligns with findings that male OT students and clinicians may encounter stereotyping, social isolation, and reduced belonging within educational and practice environments (Bohn et al., 2019; Colaianni et al., 2022).
The lack of male representation can limit diversity of thought and experience, reinforcing the need for mentorship and support (Serrano-Diaz, 2025; Silva et al., 2019). Students from less privileged socioeconomic backgrounds, regardless of gender, are vulnerable to poor academic outcomes, including lower self-efficacy and engagement (Raimondi et al., 2025). Serrano-Díaz (2025) noted that male students are particularly affected. Addressing these challenges is vital for fostering an inclusive academic environment and preparing future professionals to thrive and contribute meaningfully to the field (Smith et al., 2021).
The transition from classroom learning to clinical practice is a critical period for OT students, often marked by emotional stress and adjustment challenges. For male students, this phase can be challenging. Gallagher and Hamed (2022) explored the importance of mentorship and role models, noting peer‑mentorship programmes have been linked to improved acclimation, success, and reduced stress among male students. Furthermore, research by Zelin et al (2022) suggests that individuals from underrepresented backgrounds report more positive experiences when supported by mentors or professionals with similar identities, thereby enhancing both learning and well-being. Developing high-quality, identity-conscious resources during the transition to fieldwork is essential for promoting professional competence and a keen sense of identity (Turpin et al., 2021).
This study extends earlier work by examining the lived experiences of male students and practitioners in the UK and the US, integrating structured survey responses with personal accounts to provide deeper insight into gender equity in occupational therapy. Therefore, the central research questions guiding this inquiry are: Do male occupational therapy students and practitioners experience gender-related dynamics in education and practice, and what implications do these experiences have for inclusion and professional identity?
Research design
Following Institutional Review Board approval, the study used a qualitative phenomenological design with quantitative elements. Data were collected through an online survey administered via a secure Qualtrics link, targeting participants in the UK and the US. The survey was adapted from Maxim and Rice (2017) with permission. Building on their study, this data collection method included adding open-ended questions to capture personal experiences, revising demographic items for clarity, and updating language to reflect current discussions on diversity. Likert-scale items were retained to provide structured measures of perception, while open-ended prompts allowed for detailed narratives. This mixed-methods approach offered both measurable trends and deeper insights into lived experiences.
Participants
The study sample included male-identifying individuals within the occupational therapy profession, encompassing both students and practicing therapists. Eligible students were currently enrolled in occupational therapy or occupational therapy assistant programmes or awaiting certification results. Practicing therapists were actively working as occupational therapists or occupational therapy assistants. All participants were required to be at least 18 years old, English-speaking, residents of the US or the UK, and able to provide informed consent.
Recruitment strategies
Participants were recruited from the UK and the US through digital outreach, including professional listservs, online discussion boards, and social media platforms. A recruitment letter developed by the study authors was used to facilitate direct contact and referrals. All study activities were conducted remotely, with no in-person interactions or site visits. Of the 96 individuals who responded, 75 met the inclusion criteria and completed the study.
Data collection
All eligible participants completed a one-time online survey via a secure Qualtrics link. Completion time varied, up to 1 hour, depending on the level of detail in the response. No follow-up participation was required. The survey was voluntary, anonymous, and preceded by electronic informed consent. With permission, the survey was adapted from Maxim and Rice (2017) and modified to fit the context of this study, following core research design principles. It included two distinct branches based on participant roles:
• Therapist Survey Branch: (See Table 1)
A total of 11 Likert-scale items assessing perceptions of male therapists.
A total of 14 demographic/background questions.
Student Survey Branch: (See Table 2)
• A total of 13 Likert-scale items assessing perceptions of male students.
A total of 12 demographic/background questions
A further three open-ended questions on student experiences
All Likert-scale items used a 5-point scale ranging from (1) Strongly Agree to (5) Strongly Disagree. Participants could also leave additional comments on certain questions throughout and at the end of the survey.
Occupational therapists and occupational therapy assistants Likert survey questions.
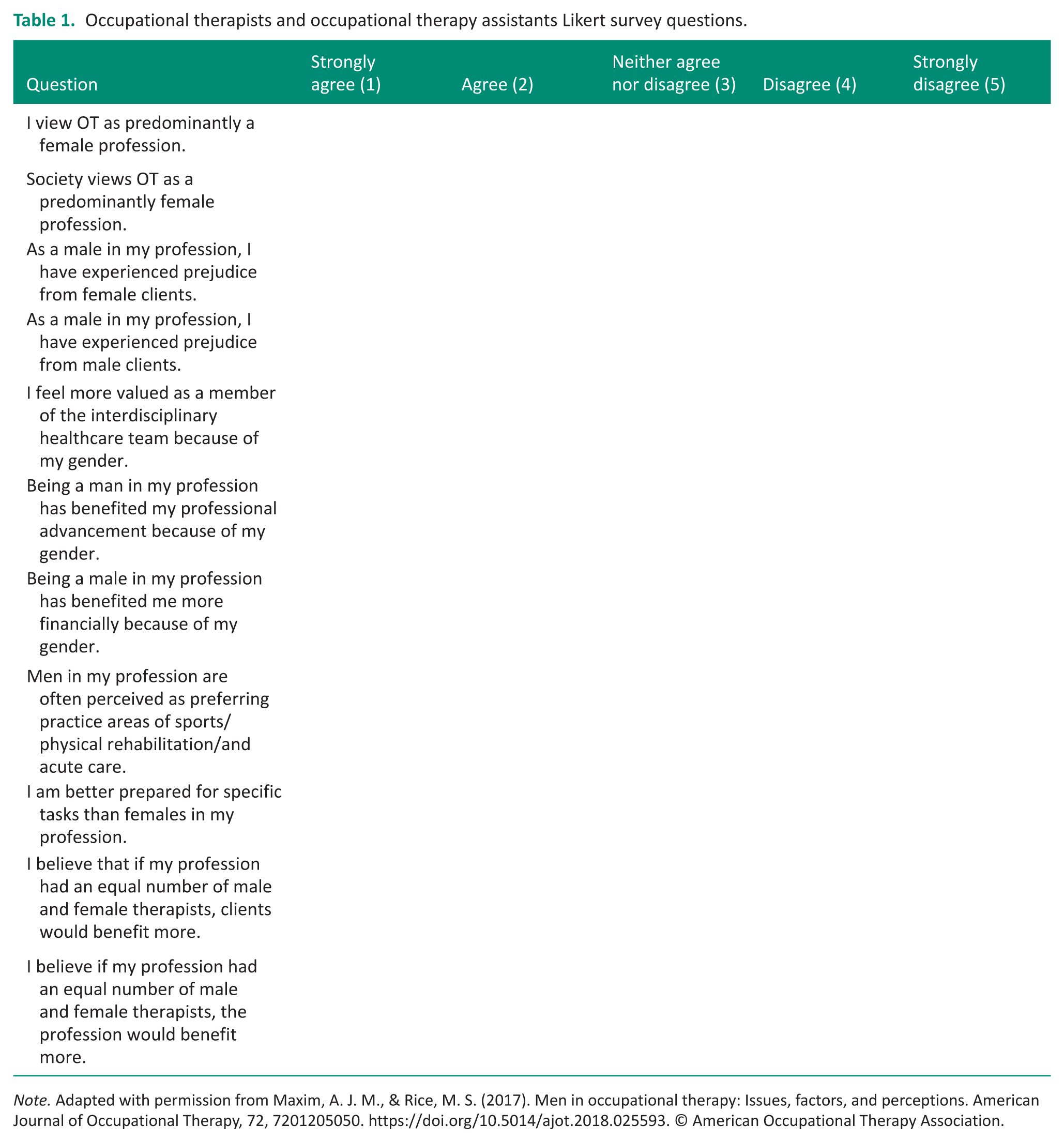
Note. Adapted with permission from Maxim, A. J. M., & Rice, M. S. (2017). Men in occupational therapy: Issues, factors, and perceptions. American Journal of Occupational Therapy, 72, 7201205050. https://doi.org/10.5014/ajot.2018.025593. © American Occupational Therapy Association.
Occupational therapy and occupational therapy assistant student Likert survey questions.
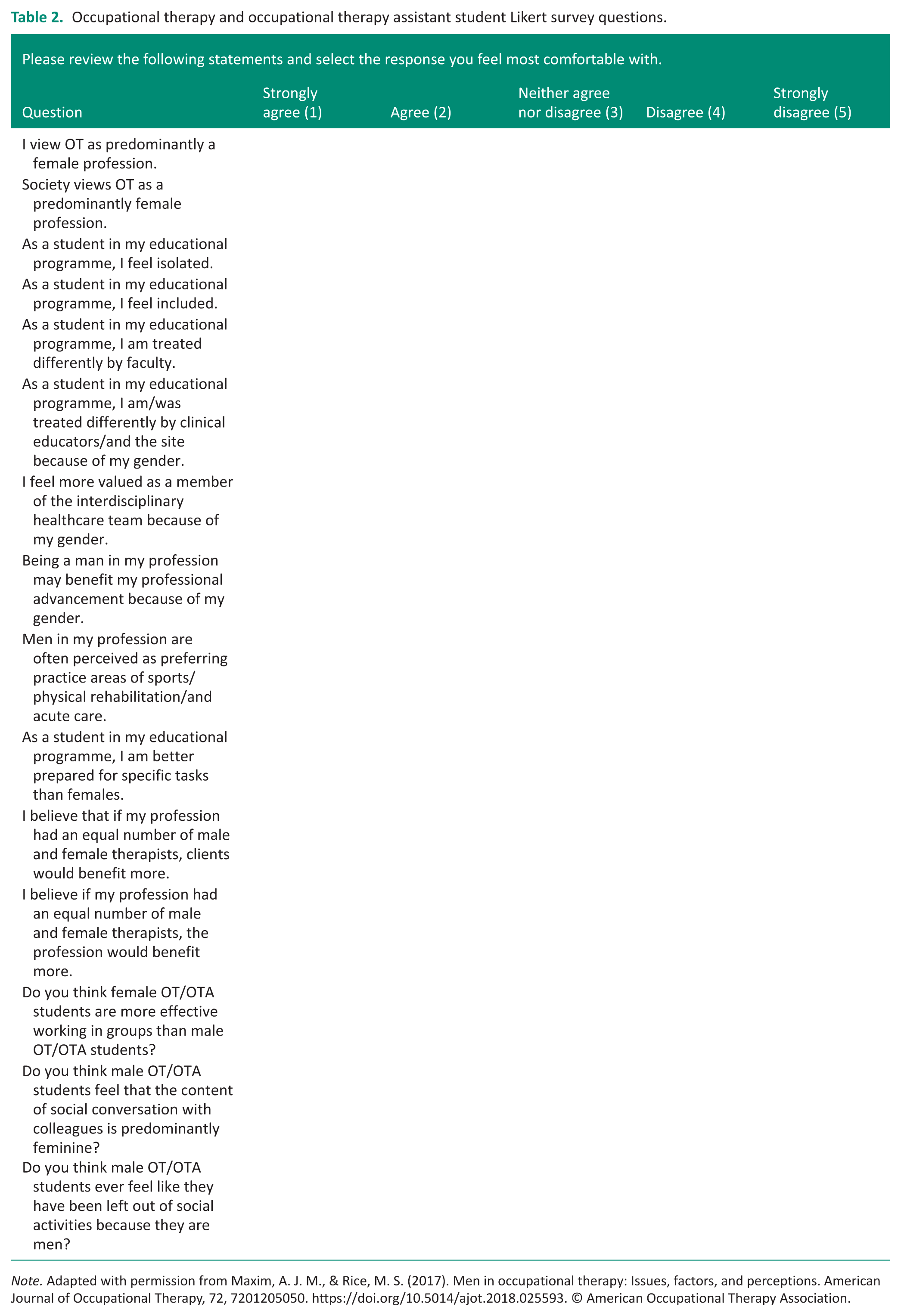
Note. Adapted with permission from Maxim, A. J. M., & Rice, M. S. (2017). Men in occupational therapy: Issues, factors, and perceptions. American Journal of Occupational Therapy, 72, 7201205050. https://doi.org/10.5014/ajot.2018.025593. © American Occupational Therapy Association.
Data analysis
A qualitative dominant mixed-methods approach was used. Responses to open-ended survey questions were analysed using reflexive thematic analysis to identify recurring patterns and shared meanings across participants’ lived experiences (Braun and Clarke, 2022) Likert-scale survey data were analysed using descriptive statistics only, including means and standard deviations, to summarise trends across participants and to support interpretation of the qualitative themes. No inferential statistical tests were conducted or reported. This approach was selected due to the exploratory nature of the survey, small and uneven subgroup sizes, and the primary phenomenological focus of the study. Quantitative findings were used solely to contextualise the qualitative results rather than to test hypotheses or make inferential comparisons. All data were securely stored by the principal author, and the study was completed over a six‑month period.
Results
Demographics
A total of 75 males participated in this study. Table 3 presents demographic information for occupational therapy and occupational therapy assistants.
Therapist Demographics: Similarities and Differences
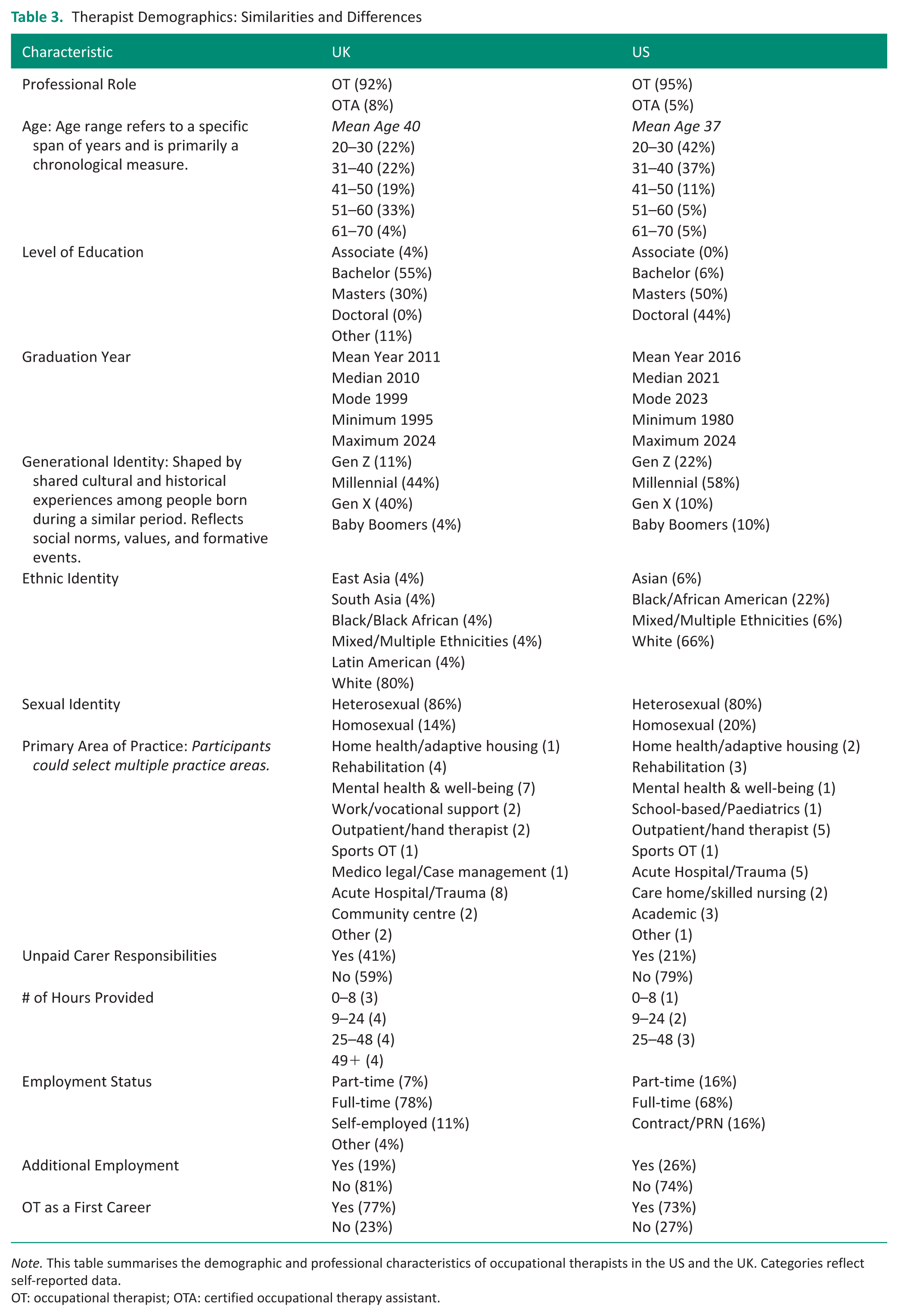
Note. This table summarises the demographic and professional characteristics of occupational therapists in the US and the UK. Categories reflect self-reported data.
OT: occupational therapist; OTA: certified occupational therapy assistant.
Therapist Demographics: Similarities and Differences
This section reports findings from our study sample and should not be interpreted as representative of the entire occupational therapy profession. The data reflect responses from male-identifying occupational therapists and occupational therapy assistants in the UK and the US who participated in the survey. Most respondents identified as occupational therapists (UK: 92%, US: 95%) and were predominantly heterosexual (UK: 86%, US: 80%) and employed full-time (UK: 79%, US: 68%). A majority reported occupational therapy as their first career (UK: 77%, US: 73%).
Several differences were observed between the two groups overall. US respondents were younger, with a mean age of 37 compared to 40 in the UK. Educational attainment reflected distinct academic structures: 55% of UK occupational therapists held a bachelor’s degree and 30% a master’s, while none reported doctoral-level qualifications; in contrast, 50% of US therapists held a master’s degree and 44% a clinical doctorate. These differences reflect distinct academic structures in each country.
Graduation years also differed, with UK therapists graduating earlier (median: 2010) compared to US therapists (median: 2021). Generational identity varied slightly: UK respondents were primarily Millennials (44%) and Gen X (40%), while US respondents were mostly Millennials (58%) and Gen Z (21%).
Ethnic diversity was greater in the US sample (63% White, 22% Black, 5% Asian, 5% Mixed, and no response 5%) compared to the UK (77% White, with smaller representation from other backgrounds (4% Black, 4% East Asian, 4% South Asia, 4% Mixed, and 4% Latin American, and 4% no response). UK respondents reported higher unpaid caregiving responsibilities (41% vs 21% in the US), often exceeding 49 hours per week. Additional employment was more common in the US (26% vs. 19% in the UK), with roles such as PRN (Pro re nata or as needed) inpatient rehabilitation, CARF surveyor (Commission on Accreditation of Rehabilitation Facilities), and assistive technology consultant. Practice areas also differed: UK therapists reported more involvement in mental health and well-being, while US therapists were more likely to work in outpatient and hand therapy settings (Table 4).
Student demographics: Similarities and differences.
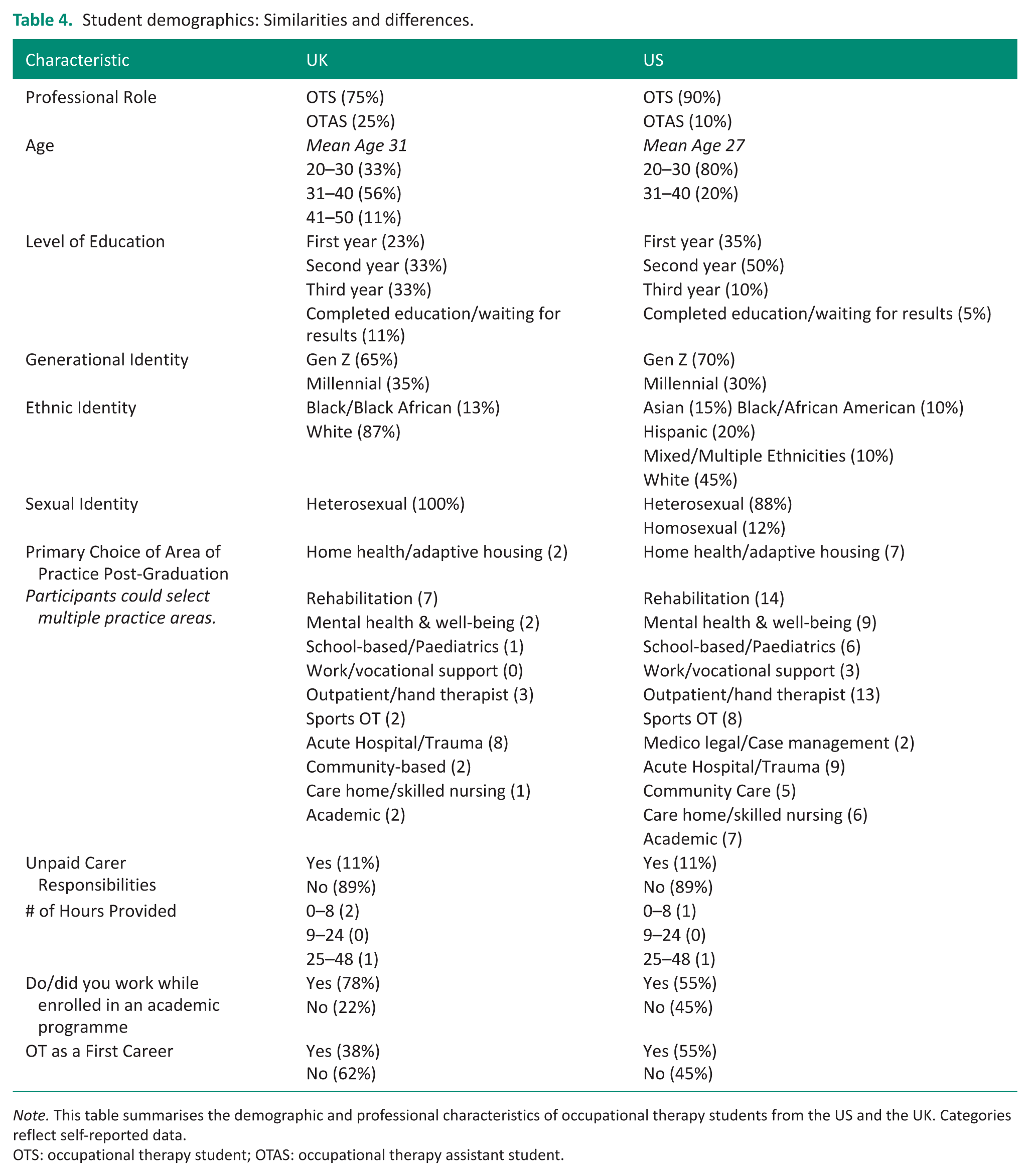
Note. This table summarises the demographic and professional characteristics of occupational therapy students from the US and the UK. Categories reflect self-reported data.
OTS: occupational therapy student; OTAS: occupational therapy assistant student.
Student Demographics: Similarities and Differences
This section reports findings from our study sample and should not be interpreted as representative of all occupational therapy and occupational therapy assistant students. Within our dataset, several demographic similarities were observed between students in the UK and the US. Generational identity was comparable: 65% of UK students and 70% of US students identified as Gen Z. In both countries, 11% of participants reported unpaid caregiving responsibilities. Employment during academic studies was more significant among UK students (78%) than US students (55%). Interest in practice areas such as acute hospital care, trauma, and rehabilitation was consistent across both groups.
Additional distinctions were identified. In the US, 90% of respondents were OT students and 10% OTA students, while in the UK, 75% were occupational therapy students and 25% occupational therapy assistant students. The average age of US students was 27 compared to 31 in the UK. US students were primarily in their second year (50%), whereas UK students were primarily second- and third-year cohorts (33% each).
Ethnic diversity was lower among UK students, with 87% identifying as White and 13% as Black, compared to the US sample, where 45% were White, 10% Black, 15% Asian, 20% Hispanic, and 10% mixed/multiple ethnic groups. Sexual orientation data showed that all UK students identified as heterosexual, while 88% of US students identified as heterosexual and 12% as homosexual.
Career pathways also differed. In the UK, 38% reported occupational therapy as their first career, compared to 55% in the US. Caregiving responsibilities were greater among UK students, with reported loads ranging from 25 to 48 hours per week, compared to 0–8 hours among US students.
Themes across all groups
The perception of OT as a predominantly female profession
Participants across all groups agreed that occupational therapy is viewed as a predominantly female profession. UK and US students both strongly agreed (Mean = 1.44), as did US therapists (Mean = 1.47). UK therapists, however, showed slightly less agreement (Mean = 2.04), suggesting a more moderate perception of men active in the field. UK students expressed strong agreement with this perception personally (Mean = 1.44) and also believed society holds this view, though with slight variation. US therapists showed similar patterns, strongly agreeing that occupational therapy is a predominantly female profession (Mean = 1.47) and rating societal perception slightly higher (Mean = 2.10). These differences suggest that respondents distinguish between their own stance and what they believe society thinks, even though both are subjective judgements.
Feelings of isolation or inclusion as a male student within a predominantly female cohort
UK student participants were neutral about feeling isolated in their educational programmes (Mean = 3.13), while US students somewhat disagreed with the statement (Mean = 3.95), indicating lower levels of perceived isolation. When asked about inclusion, UK students somewhat agreed they felt included (Mean = 2.50), a sentiment echoed by US students (Mean = 1.84). These findings suggest that while male students may experience some degree of isolation, most report feeling included within their predominantly female cohorts.
Experiencing prejudice from patients in the profession
US therapists reported mixed experiences regarding patient prejudice. When asked about interactions with female patients, responses were neutral on average (Mean = 2.89), but the standard deviation (Standard deviation = 1.24) indicated a wide range of views. A similar pattern emerged in responses about male patients, where participants somewhat disagreed with experiencing prejudice (Mean = 3.53), yet the standard deviation (Standard deviation = 1.35) again reflected varied experiences.
Treatment received as a male occupational therapy student or occupational therapist
Student responses revealed regional differences in perceptions of gender-based treatment. UK students were neutral about being treated differently by faculty (Mean = 3.11) and during clinical placements (Mean = 2.56). In contrast, US students tended to disagree with the notion that they were treated differently because of their gender, both in academic settings (Mean = 4.05) and clinical placements (Mean = 4.21).
Feeling valued, professional advancement, and financial gain
Student responses from both the UK and the US indicated ambivalence about feeling more valued on interdisciplinary teams because of their gender (UK: Mean = 2.89; US: Mean = 2.63). UK students were similarly neutral regarding whether being male benefited their professional advancement (Mean = 3.38), while US students leaned slightly toward agreement (Mean = 2.11). At the professional level, US therapists reported feeling somewhat more valued on interdisciplinary teams because of their gender (Mean = 2.53).
Regarding financial gain, UK students generally disagreed that gender provided an advantage (Mean = 3.75), whereas US students were neutral (Mean = 2.79). Among practicing therapists, US participants also expressed uncertainty about gender-related career benefits (Mean = 3.47), with median and mode responses indicating slight disagreement. When asked about financial advantages, US therapists largely disagreed (Mean = 4.26), with median and mode responses of “strongly disagree.” These findings suggest that while some male occupational therapy and occupational therapy assistants perceive modest professional advantages, they do not consistently associate their gender with increased value, advancement, or financial benefit.
Practice areas and gendered tasks
In this context, “gendered tasks” refers to work activities or responsibilities that are perceived as being more suited to one gender based on stereotypes rather than actual competence. Examples include assumptions that male therapists are better prepared for physically demanding tasks or prefer practice areas such as sports rehabilitation, acute care, or trauma settings, while female therapists are associated with roles emphasising emotional support or mental health.
Student perceptions of these preferences varied by region. UK students were neutral (Mean = 2.75) on whether male therapists are perceived as favouring areas such as sports, physical rehabilitation, or acute care. US students agreed more strongly with this perception (Mean = 1.74). Regarding task preparedness, UK students remained neutral (Mean = 3.25), while US students somewhat disagreed (Mean = 3.79), suggesting they did not view male students as better prepared than female peers. When asked whether males were better prepared for specific tasks, both UK and US therapists mildly disagreed (UK Mean = 3.59; US Mean = 3.53), indicating that male therapists do not see themselves as more capable than female colleagues.
Among professionals, US therapists somewhat agreed (Mean = 2.00) that men are perceived as preferring specific practice areas but disagreed (Mean = 3.53) that they are better prepared for work tasks. UK professionals were neutral on both points (Mean = 2.93). One UK respondent (#58) described integrating personal interests into practice, including sport-based mental health programmes, illustrating how individual preferences can shape practice areas beyond gendered expectations.
Gender split within the profession
UK student respondents somewhat agreed (Mean = 3.28) that an equal number of male and female occupational therapy and occupational therapy assistant therapists would benefit clients. US students were more neutral (Mean = 2.95), suggesting mixed views. When asked about the benefit to the profession itself, UK students leaned slightly toward agreement (Mean = 2.38), while US students again remained neutral (Mean = 2.58). Professional respondents from both countries showed slight variation, with neutral responses to both questions (US Mean = 3.53; UK Mean = 3.59). These findings suggest that while students, particularly in the UK, see potential value in gender balance, practicing professionals are less likely to view it as a significant factor.
Effectiveness of working in groups
This study sought to explore perceptions of group dynamics, leadership, and advocacy traits among male and female students, as these qualities are relevant to collaborative practice in occupational therapy. While previous research has not consistently examined gender differences in group effectiveness, understanding these perceptions can provide insight into how male students experience teamwork within predominantly female cohorts.
Responses indicated no significant difference in perceived effectiveness. UK students generally viewed group work as equal, with comments such as “No, I feel it is equal” and “Does not matter.” One respondent noted he was the only male in his cohort and could not make a comparison. US students offered more nuanced views. One participant acknowledged that women might be better suited for certain group settings, but emphasised that both genders contribute effectively. Another participant expressed initial apprehension but anticipated taking on leadership roles within a predominantly female cohort.
Social dynamics in conversation
This study sought to explore whether male students perceived social interactions within predominantly female cohorts as inclusive or shaped by gendered norms. It did not intend to suggest that certain topics are inherently “feminine,” but rather to understand whether participants felt conversations reflected shared experiences that they could or could not relate to.
Responses varied by region. UK participants generally indicated that conversations were balanced and inclusive, with comments such as “Not really” and “I have developed friendships with a majority of the female students and can have general conversations.” US students expressed slightly stronger perceptions of difference, noting that some discussions reflected experiences more common among women, such as childcare or family roles, which they felt less able to contribute to. One respondent described the dynamic as “balanced overall” but acknowledged that certain topics leaned toward those experiences. Another individual attributed this to the predominantly female composition of cohorts. These responses suggest that perceived differences in social interaction are shaped by cohort demographics and cultural context rather than inherent gender traits.
Social exclusion and gender-based interaction
Participants were asked whether male occupational therapy students had been excluded from social activities because of their gender. The UK response suggested mild agreement (Mean = 1.78), though only one student responded. He stated, “No, there is a respect present, yet I am treated differently because of my gender, not negatively, more than a necessity.” While he did not feel excluded, he acknowledged a noticeable difference in treatment based on gender.
US students showed stronger agreement with the theme (Mean = 1.44). One student shared, “Personally, I have experienced this, though I feel that it is a necessary component of being the only male in a social environment. Although I feel accepted by female members of my program, have close friends, and am gay, I am still a man, and I feel that there is a level of equal social acceptance that I can't achieve because of this within my program.” These responses suggest that while exclusion may not be overt, male students are aware of subtle differences in social dynamics that affect their sense of inclusion.
Female-to-male ratio in the profession
When asked whether clients would benefit from an equal ratio of female to male occupational therapists, US therapists were neutral (Mean = 2.74). However, when asked if such a balance would benefit the profession overall, both UK and US therapists showed modest agreement (UK Mean = 2.67; US Mean = 2.16). This contrast suggests that while gender equity is seen as beneficial to the profession’s structure and culture, its direct impact on client outcomes is less clear. The difference in responses raises essential questions about how therapists perceive the role of gender diversity in shaping professional identity and workplace dynamics, independent of clinical effectiveness.
Discussion
This study examines how men in occupational therapy navigate education and practice within a predominantly female profession. Gendered expectations remain visible in training and early practice, especially around physical strength and “masculine” areas such as sports, physical rehabilitation, and acute care. These patterns are well described in the literature and point to the need for explicit gender awareness in curricula and supervision so that task allocation, assessment opportunities, and feedback are guided by competence rather than stereotype (Bohn et al., 2019; Bonde Nissen et al., 2023; Maxim and Rice, 2017). Bringing these issues into routine teaching and supervisory conversations helps avoid a quiet drift toward gendered tasking that can narrow skills and future options (Bonde Nissen et al., 2023; Maxim and Rice, 2017).
Men’s experiences are also shaped by the day‑to‑day social organisation of programmes and teams. Being the only man in a cohort or service can heighten visibility and scrutiny, restrict informal networks, and limit invitations to mentoring relationships, features of tokenism that increase pressure and undermine belonging. Practical responses are straightforward: rotate partners, structure peer support, and make mentoring access routine rather than dependent on ad‑hoc invitations (Bohn et al., 2019; Kanter, 1977). These steps shift responsibility from individuals to systems and make participation less contingent on informal ties.
Career development for men in OT is influenced by local culture and expectations. Perceived status advantages, such as assumptions of leadership potential or greater visibility, are uneven and context‑dependent and can be offset by added scrutiny or narrow role expectations. Team climate matters. Research suggests that men may sometimes report stronger teamwork in predominantly female groups, while women report lower teamwork in predominantly male groups, highlighting how gendered cultures shape collaboration (Williams and O’Reilly, 1999). Qualitative work shows that men in feminised fields may manage or downplay aspects of workplace culture to maintain a socially acceptable masculine identity, what Simpson calls “gender work,” adjusting interactional style to local norms (Simpson, 2004). The practical point is that visibility can function as support or scrutiny depending on supervision, tasking, and opportunities.
Improving representation and clarifying routes to seniority require better data and targeted action. In the UK, publicly available workforce statistics summarise overall gender composition but do not report role‑ or band‑specific distributions, limiting insight into where bottlenecks occur (NHS, 2024). Even with incomplete data, the profession remains strongly feminised. Greater transparency around recruitment, grade, and pay would help separate perception from pattern and guide interventions where they will make the most difference (NHS, 2024). Without band‑level reporting, it is difficult to assess whether perceived advantages or disadvantages for men translate into differential promotion, remuneration, or access to leadership pathways.
These observations suggest clear steps for education and practice. Programmes and placements can use targeted outreach, increase the visibility of male role models, and embed gender‑awareness content that challenges stereotypes and supports equitable task allocation (Bohn et al., 2019; Maxim and Rice, 2017). Fieldwork sites can monitor rotations and caseloads for gendered patterns and provide structured peer support to reduce isolation, in line with tokenism theory’s emphasis on proportion and access (Bohn et al., 2019; Kanter, 1977). Organisations can adopt transparent reporting on recruitment, promotion, and pay by gender to determine whether perceived differences correspond to measurable disparities and to guide corrective action (Brandford and Brandford Stevenson, 2021; NHS, 2024). In service delivery, offering client choice where feasible and encouraging men to enter under‑served areas, such as mental health and vocational rehabilitation, can broaden access without reinforcing stereotypes (Bohn et al., 2019; Maxim and Rice, 2017).
Intersectionality should continue to examine how gender interacts with race, ethnicity, and socioeconomic status to help ensure that inclusion efforts benefit those most likely to encounter barriers. Evidence suggests that structural advantages tend to accrue to White men, while males from unrepresented groups may face additional constraints that limit similar opportunities (Brandford and Brandford Stevenson, 2021; Williams, 1992). Future work should prioritise disaggregated workforce data and longitudinal designs to test which supports, mentoring structures, curriculum design, and equity monitoring, most effectively improve men’s retention, advancement, and professional well‑being, while ensuring that interventions address layered inequities and contribute to culturally responsive, client‑centred care (NHS, 2024; World Federation of Occupational Therapy, n.d.).
Limitations
This study provides valuable insight into the experiences of male‑identifying individuals in occupational therapy; however, several limitations should be noted. As with most qualitative research, the findings are not broadly generalisable and should be considered exploratory. Reliance on self‑reported online survey data may introduce response bias, and voluntary participation could limit the representativeness of the sample. Although thematic analysis added depth, it remains influenced by researcher’s interpretation. Strategies such as data triangulation and collaborative coding were used to enhance rigour.
Additional limitations relate to workforce data and intersectionality. The Electronic Staff Record (ESR) dataset does not include gender‑specific information for Band 7 occupational therapists, restricting analysis of senior‑level representation. While intersectionality was considered conceptually, the sample size and available data were insufficient for detailed subgroup analyses by race or ethnicity. Future research should incorporate disaggregated workforce data and use mixed‑method, longitudinal designs to better understand how intersecting identities shape inclusion, advancement, and professional belonging.
Conclusion
This study highlights the continued underrepresentation of men in occupational therapy in both the UK and the US. Participants generally felt included and did not report discrimination from colleagues or patients. Although some noted assumptions about preferred practice areas and occasional visibility‑related challenges, these experiences were not universal and did not dominate their narratives. Most respondents did not view gender as a barrier to career progression.
The findings suggest that the profession’s strong female majority and limited visibility of male role models may influence recruitment and retention, particularly for men from racially minoritised backgrounds. Strengthening the pipeline will require targeted recruitment efforts, mentorship opportunities, and inclusive curricula that support diverse identities. Future research should explore how intersecting factors such as race, ethnicity, and socioeconomic status influence belonging and advancement. Enhancing workforce diversity will help occupational therapy better reflect and meet the needs of the populations it serves.
Key findings
Occupational therapy is a predominantly female profession shaping men’s experiences and perceptions.
Men report inclusion alongside stereotypes, social isolation, and uneven career advantages.
Challenges are most evident during education and early career, highlighting mentorship needs.
Contribution of the study to occupational therapy
This cross‑national qualitative study extends existing research by showing how gender imbalance shapes male occupational therapists’ identity, belonging, and progression, and by identifying mentorship and gender‑aware education as key supports for retention and inclusion.
Footnotes
Acknowledgements
The authors gratefully acknowledge all participants who contributed to this study. Special thanks to Dr. Rice for granting permission to adapt the original survey instrument on behalf of both himself and Dr. Maxim.
Ethical considerations
Baylor University Institutional Review Board. Principal Investigator: Susan Blair. IRB Reference #: 2180254. Date of Determination: March 21, 2025. Exemption Category: 45 CFR 46.104(d)(2). The above-referenced human subjects research project has been determined to continue to be EXEMPT from review by the Baylor University Institutional Review Board (IRB) according to federal regulation 45 CFR 46.104(d)(2): Research involving the use of educational tests, survey procedures, interview procedures, or observation of public behaviour.
Consent to participate
Informed consent to participate was obtained electronically from all eligible participants via a secure Qualtrics survey.
Author contributions
SB and PM researched the literature and conceived the study. All authors were involved in protocol development, gaining ethical approval, participant recruitment, and data analysis. All the authors contributed to the initial draft of the manuscript. SB and PM compiled the complete draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Funding
The authors declared no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Patient and public involvement data
During the development, progress, and reporting of the submitted research, Patient and Public Involvement in the research was included in the conduct of the research