
Abstract
Objective:
Parents living with and beyond cancer experience significant challenges from their illness and treatment which affect their ability to engage in parental roles and occupations. This study sought to provide in-depth understanding of the daily experiences of parents living with or beyond cancer.
Methods:
Forty-four adults living with or beyond a cancer diagnosis and parenting at least one child under the age of 18 years participated in semi-structured interviews to share their daily parenting experiences. Transcribed interviews were analyzed using thematic analysis.
Results:
Thematic analysis identified four primary themes (1) Cancer changes participation in daily occupations for self and others; (2) Cancer changes the ways parents engage in co-occupations with their children at different developmental stages; (3) Parents worry about the impact of cancer on their children, (4) Parents want help managing the impact of cancer on themselves, their children, and their families.
Conclusions:
Results highlighted daily challenges parents experience beginning at diagnosis and lasting through survivorship. Across age, gender, stage, and type of cancer, parents shared similar concerns that their diagnosis and associated challenges were negatively affecting their children. Parents highlighted a significant need for information and support to facilitate parenting. Results indicate an expanded role for occupational therapy in oncology care.
Plain language summary
This study sought to understand the daily experiences of parents living with and beyond cancer and identify gaps in knowledge and support for these parents and families. We interviewed forty-four parents (both mothers and fathers) who had been diagnosed with cancer in the last 10 years and had at least one child under the age of 18 years. Interviews were analyzed using qualitative methods. Results of this study provide insight into the effects of cancer on parents’ daily activities, concerns parents have for their children, and support parents wished they had received. Results also indicate an expanded role for occupational therapy in supporting everyday parenting roles and occupations.
Introduction
Approximately 20.5% of adults newly diagnosed with cancer are between the ages of 20–54, typical childbearing and child rearing ages (Howlader et al., 2021). As current trends highlight the increased incidence of cancer in younger adults under the age of 50 (Hamilton and Coleman, 2023), there are millions of younger survivors, including parents, who will live with long-lasting impacts of cancer and cancer treatment well into the future. Accordingly, it is important to pay attention to the unique needs of parent survivors of cancer in order to provide high-quality care (Park et al., 2022).
Literature review
Young adult survivors parenting children express concern about changes in their parental role and meaningful engagement in everyday life while navigating their illness (Moore et al., 2015). These changes may be impacted by a wide range of physical, emotional, and psychological sequelae related to the disease, its treatment, and prognosis (Park et al., 2017). These sequelae often lead to restrictions in occupational performance and participation in valued life roles, such as parenting. In a recent scoping review of unmet supportive care needs of parents living with and beyond cancer, parents noted difficulty managing multiple roles as parent, patient, employee, partner, and friend that further impact the ability to care for oneself and others (Newman et al., 2023).
There is a need for a more holistic and in-depth understanding of the experiences of parents living with and beyond cancer in the occupational therapy literature (Newman et al., 2023). While existing literature has described some of the challenges of parenting with and beyond cancer, there is a need for deeper understanding of this unique experience (Glazer et al., 2023). Accordingly, the purpose of this study was to understand: (a) the daily experiences and occupational performance challenges of parents living with and beyond cancer; (b) the gaps in resources, knowledge, and support that could be filled by supportive programming from the perspective of parents.
Method
Recruitment and data collection
Participants in this study were 44 parents (19 mothers and 25 fathers) recruited from safety net and academic hospitals in the Boston area. Safety net hospitals are hospitals that provide care to low income and underserved communities, regardless of their ability to pay. Participants were also recruited from cancer support groups and cancer advocacy groups on social media sites including Reddit and Facebook from June 2021 to January 2022. Of these participants, 36 elected to continue to an optional photo-elicitation interview. Photo elicitation is a research method that inserts a photograph taken by a study participant into a research interview (Harper, 2002). The results of the photo-elicitation interviews are published elsewhere (Glazer et al., 2023).
Multiple efforts were made to recruit a diverse sample to represent the full range of parental experiences, including cancer advocacy groups serving under-represented and diverse populations. The sample of parents in this study spanned 18 states and 3 countries, including Canada, Germany and Zimbabwe. Diversity of the sample highlights cancer groups less represented in the cancer and parenting literature including testicular, prostate, leukemia, and lymphoma as well as fathers (Newman et al., 2023).
Individuals were eligible to participate in the study if they (1) were diagnosed with any kind of cancer in the last 10 years, (2) received a diagnosis of stage 0-IV cancer, (3) were parenting at least one child under the age of 18, and (4) were English-speaking. The study was approved by the University Institutional Review Board and all participants provided written informed consent.
A majority of the participants were White (81.8%), college educated (86.3%), had an income of over $71,000 (77.2%), and shared caregiving responsibilities with one other person who lived with them (72.7%). Approximately half were working full time (54.5%) at the time of the interview. Four parents were undergoing active treatment, and 15 had completed active treatment within 1 year of their interview. The remaining participants had completed treatment up to 7 years prior to the interview, with an average of 3.5 years. See Table 1 for details on sample demographics.
Sociodemographic characteristics of participants.
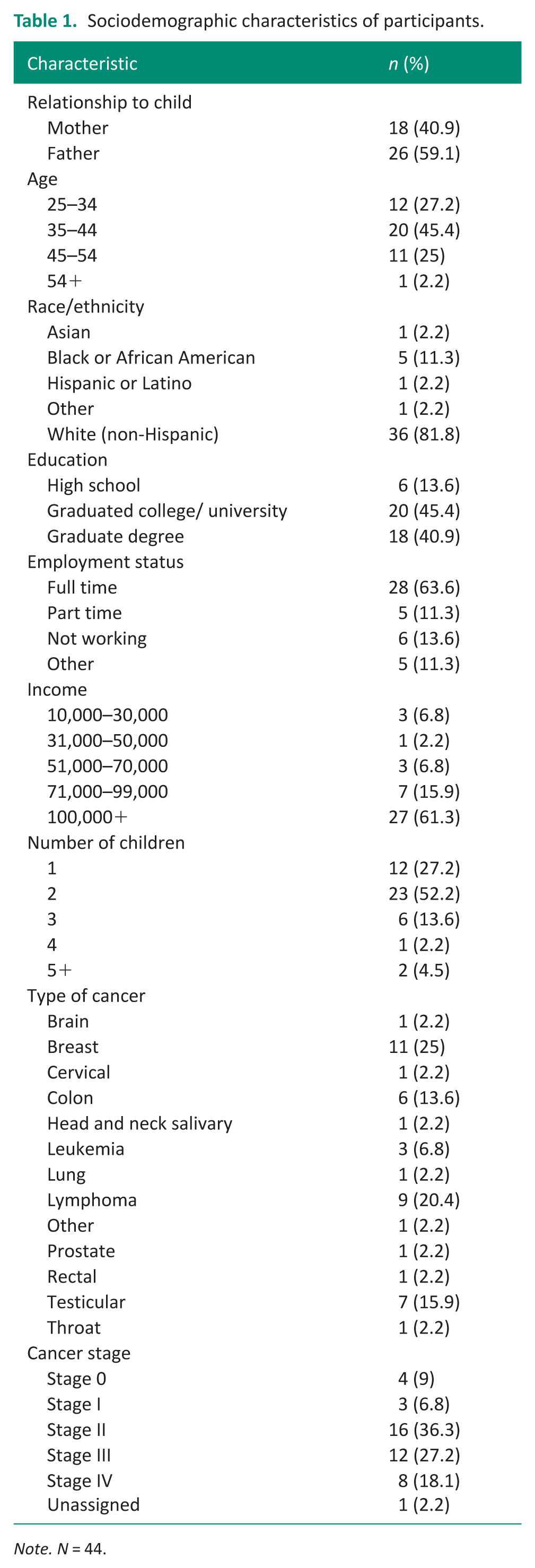
Note. N = 44.
Procedure
After participants provided informed consent, semi-structured interviews were conducted via password-protected Zoom to learn about daily parenting experiences while living with or beyond a cancer diagnosis. (See Supplemental Appendix A for semi-structured interview guide). Researchers provided flexibility for scheduling interviews to accommodate participants’ schedules, use of smartphones for participants without computer access, and compensation for participants’ time. All interviews were conducted between June 2021–January 2022, within the context of the COVID-19 pandemic. This article focuses on content from the first semi-structured interviews.
Data analysis
Interviews were transcribed via Zoom and verified for accuracy by trained research team members. Themes were developed using Braun and Clarke’s (2006) six steps for thematic analysis: (a) data familiarization, (b) initial coding, (c) searching for themes, (d) reviewing the themes, (e) naming themes, and (f) producing the report. Initial codes were created after data collection and focused on occupations, co-occupations, facilitators, barriers, emotional responses, and symptoms.
Team members created an initial codebook which was trialed on two transcripts, iteratively revised, and finalized with six transcripts. Team meetings with study staff and the principal investigator were conducted to reconcile coding differences and reach coding consensus in NVivo (Release 14.23.4) software (Lumivero, 2025). Following coding, research team members created a thematic map and identified initial themes.
Results/Findings
Thematic analysis identified four primary themes: (1) Cancer changes participation in daily occupations for self and others; (2) Cancer changes the ways parents engage in co-occupations with their children at different developmental stages; (3) Parents worry about the impact of cancer on their children, (4) Parents want help managing the impact of cancer on themselves, their children and their families. Refer to Figure 1 for thematic map.
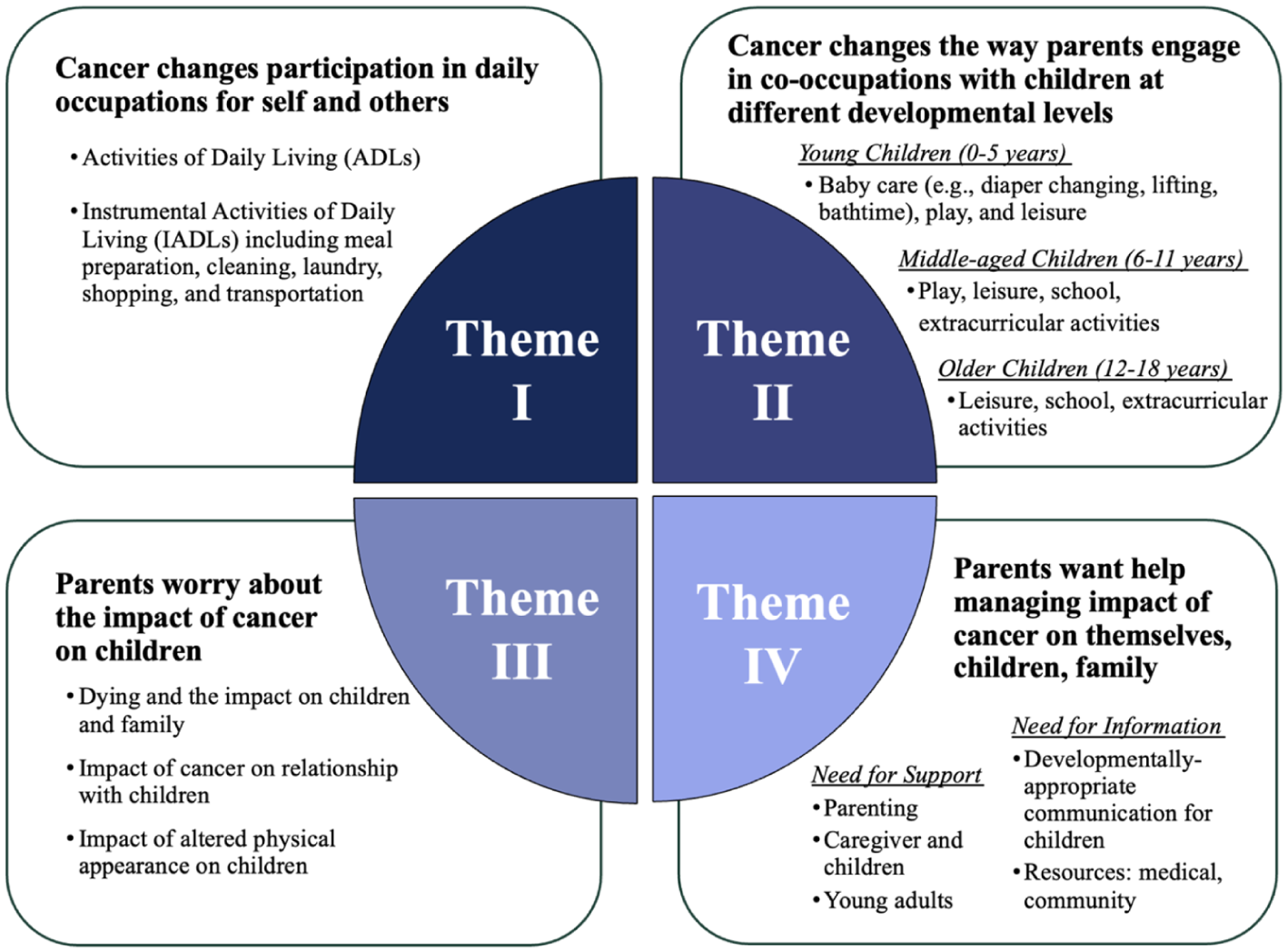
Thematic map.
Across age, gender as well as type and stage of cancer, parents reported a range of symptoms impacting everyday occupations. The most frequently reported symptoms were fatigue, pain, neuropathy, weakness, cognitive dysfunction, anxiety, and depression. The symptom burden reported by parents influenced their ability to care for themselves and their children and families across a wide range of occupations and co-occupations.
Theme I: Cancer changes participation in daily occupations for self and others
Across a range of cancer diagnoses and stages of disease, mothers and fathers reported changes in their ability to perform activities of daily living (ADL) and instrumental activities of daily living (IADL). Approximately one-third of parents reported difficulty performing ADLs such as bathing, dressing, and grooming because of their cancer and cancer treatments. Parents experienced challenges managing their own self-care while adapting to altered physical abilities.
A mother described how the challenge of showering with mobility restrictions was complicated by parenting
With showering after surgery, like I could barely wash my hair and it drove me crazy because I couldn’t get my hands up and I couldn’t ask my husband because he was watching the baby, so it was like very frustrating. (Stage II breast cancer, child aged 10 months)
Parents also experienced challenges managing IADLs with 50% (n = 22) of parents reporting challenges performing occupations such as cooking, cleaning, driving, and shopping. Often, the challenges performing IADLs had a direct impact on activities related to their children. A mother reported
I broke down in tears one, during. . .one kind of flare up of the side effect because I was trying to make my kids sandwiches and I couldn’t hold the tomato because it was too cold, to be able to slice it to put on you know, their lunch. (Stage III colorectal cancer, children aged 8, 10, 11)
Parents expressed guilt and sadness in response to the challenges they experienced performing their daily occupations. Parents navigated complex experiences of being both patient and parent to children of all ages. A mother shared
I was pretty much just numb and waiting for each day to pass and wondering when and if it was ever going to get better. . .I feel a little guilty that I didn’t do more, but I was not capable of that. . .. My kids were orphaned, and my husband was abandoned, and they survived together; and they were just surviving together. (Stage II breast cancer, children aged 14,15)
Theme II: Cancer changes the ways parents engage in co-occupations with their children at different developmental stages
Thirty-eight (86%) parents reported changes to their daily engagement in co-occupations with their children because of their cancer and side effects. Parents reported changes in their ability to participate in baby care, play, or supporting their children with school-related activities such as homework. We describe these effects on co-occupational performance separately for young children (0–5 years), school-aged children (6–11 years), and adolescents (12–18 years).
Co-occupations with young children
Parents reported a range of co-occupations such as play and activities including diaper care, dressing and bathing children, carrying or lifting children, and bedtime activities were disrupted by cancer.
A father shared
There were times during chemotherapy where my parenting consisted of. . . laying on the ground in her room and making sure she wasn’t hurting herself because that’s all the energy I had that day. (Lymphoma, child aged 2)
Both mothers and fathers described difficulty participating in baby care and young childcare. A mother shared
I would put the babies down for a nap and I would just hope that [my husband] got home before I had to get them out because I couldn’t bend my arm. . .to pick them out of the crib. . . sometimes I would leave them in the crib and just read to them until he got home and. . .I’ve never been so tired in my life. (Stage III breast cancer, twins aged 3.5)
Parents frequently describe the impact on play with their young children. One father shared
I wanted to play with her all the time. . . when I was in the hospital, that was the thing I was like, ‘I just want to get out of here and play with my daughter as much as I can,’ and then I got out, and I was tired. . .the concentration, it’s just so hard. (Leukemia, children aged 9 months, 5)
Co-occupations with school age children
In addition to play, parents reported challenges supporting their older children with schoolwork and extracurricular activities. For parents of elementary and middle school aged children, daily or nightly homework took on importance as a central child/parent co-occupation. A mother shared the challenges of balancing her symptoms while trying to support her daughter’s schoolwork
A few weeks ago, I was in the bathroom vomiting and she[daughter] came in with her math homework, and was like ‘Mommy, when you’re done, can you help me with this?’ (Stage II cervical cancer, child aged 9)
Another mother shared
My little one was in kindergarten, and I had to be there for him. . . throughout the whole entire day. . . I was like extremely tired and even just like sitting at the counter with him. . . it was exhausting. (Stage IV colorectal cancer, children aged 7, 9)
Co-occupations with adolescents
Among parents of adolescents, school activities, and IADL were reported as the most common co-occupations. Challenges supporting children with schoolwork continued. One father shared
There was a time when I would need to help them with their homework, but I was in no condition. . . and their grades suffered. (stage IV lymphoma, children aged 15, 17)
In contrast to those with young and school-aged children, parents of adolescents shared accounts of their children ‘stepping up’ and assisting with IADLs such as cooking, cleaning, and shopping. One father shared
I can’t do anything but there’s three people in the house now plus my wife who can do chores, and so that helped a lot when I was feeling really bad. . .. the girls would step up and do things. . . And so occasionally we have like assigned them, ‘Okay you’re making dinner tonight.’ (Stage III rectal cancer, children aged 15, 18)
Theme III: Parents worry about the impact of cancer on their children
The changes in co-occupational performance elicited a range of emotional responses from parents of children of all ages. While some parents reported feelings of gratitude and pride seeing their older children step up, others reported feelings of disappointment, guilt, and helplessness.
Both mothers and fathers expressed a range of concerns because of their cancer diagnosis and prognosis. The major concerns included (a) dying and the impact on children and family, (b) impact of cancer on relationship with children, (c) impact of altered physical appearance on children.
Concerns about dying and the impact on children and family
Approximately half of the parents with both early and late-stage disease expressed existential concerns. Two primary concerns related to mortality: (a) parents’ fear of missing out on seeing their child(ren) grow up, and (b) parents’ concern that their child will grow up without one of their parents. One mother shared
I think it’s a lot harder when you have children. . . When anybody gets cancer they’re constantly [thinking] ‘Am I going to die?’ . . . when you have a child, like it’s sort of doubles the impact. . .you just constantly worry like I do the math in my head like if I was diagnosed now like immunotherapy could maybe keep me alive for at least two years she’d be 11 you know could she fend for herself. . . and that never goes away. (Stage II cervical cancer, child aged 9)
Similarly, a father expressed
The part I struggled with the most was if I died, my kids would not have a father and that really really haunted me. . . that was, almost debilitating. . ., that would just make you want to survive, would make you want to push forward. . . It kind of becomes a fear a phobia and it kind of oozes its way into things. . . The thought of everything that we would miss was just devastating to me. (Stage III colorectal cancer, children aged 12, 14)
Notably, while these concerns were overwhelmingly associated with negative emotional responses such as sadness and guilt, some parents simultaneously expressed gratitude for the time they were able to share with their children and attempted to mitigate the fear or despair associated with mortality. One father shared
A shift in perspective for me as a father and trying to teach my kids. And if the house is messy or if the lawn doesn’t get mowed. . ., it’s not a big deal anymore for me. I just want them to have really good memories of me. (Stage IV colorectal cancer, children aged 5, 10, 12, 14)
Concern about impact of cancer on relationship with children
Parents of young and elementary-aged children expressed concern connecting with their children. One father shared
My doctor. . . said don’t even go into the hospital when he[son] was going to be born, and I did. And they said don’t touch him. . . don’t change his diaper, and I waited as long as I could. . . I don’t know if there is a bonding that was missed in those early times. (Leukemia, children aged 9 months, 5)
Similarly, a mother reported It felt very hard to parent, it felt very hard to make connections . . ., you felt like a robot going through. . . make sure they have their food and they’re in bed, and you try to read to them, but like you feel like you weren’t present. (Stage II breast cancer, children aged 7, 10)
Mothers and fathers expressed concerns about the psychosocial effects of cancer on their children. While parents with both early- and late-stage cancers expressed these concerns, they were reported more often by parents with late-stage cancers. One father shared
. . .my saddest parenting moment was that night. . . I went into my bathroom to get something, and my seven-year-old was just bawling in the shower talking to himself about like how much he didn’t want his dad to die. (Stage III colorectal cancer, children aged 10, 12, 13, 14, 15)
Concerns about the impact of altered physical appearance on children
Multiple parents in this study, particularly those parenting young and elementary-aged children, expressed concern that their altered physical appearance was distressing to their children. One father shared
[My daughter] was two so. . ., the scar scared her a little bit. . . the scar was a big deal because it was pretty gnarly for a while. . . So she knew something was going on. . ..it took a little bit you know, for her to kind of warm back up to me and not be terrified of me. (Stage III glioma, children aged 2, 4, expecting)
Theme IV: Parents want help managing the impact of cancer on themselves, their children, and their families
Mothers and fathers both expressed a heightened need for information and support. They wanted information about parenting with cancer, communicating about illness with children, resources to support patients and families, family planning, and survivorship. Parents desired peer support for young adults with children, mental health support, family programming, support for children from schools, childcare support, and financial support. Parents described how limited access to resources compounded family issues such as caregiver burden, poor communication with family members (children), and financial distress.
Need for information
Parents identified two distinct sources of information they desired better access to (a) information about developmentally appropriate and tailored communication with children and (b) information about accessing resources in the medical system and in the community.
Parents shared their challenges determining how to share their diagnosis with their children, when to do so, and in how much detail. Parents with advanced disease reported an increased desire for communication support compared to parents with early-stage disease. Parents largely ‘figured out’ how to communicate this information to their children on their own with very little input from professionals. A father stated
When I was first diagnosed, it would have helped me to get some direction with how to tell the kids. We kind of, just stumbled into that on our own, my wife and I, like we didn’t really have a lot of direction and my family was pulling us in a different direction of ‘Well, you can’t tell them.’ And the doctor really didn’t offer much of anything. . . I was even seeing a psychologist at the time, and he didn’t really like, he basically said, ‘Do what you feel is right,’ you know and it’s like, I don’t know what’s right, you tell me. (Stage IV prostate cancer, children aged 9, 11)
Parents also shared how lacking information caused feelings of concern and uncertainty among their families. Parents expressed wishes for increased support for themselves, their care partners, and their children. One father living with a terminal diagnosis described his family’s experience of searching for information regarding his diagnosis
There’s just nothing out there. . . specifically for families. . . It was so difficult for [wife] to get any information whatsoever. . . There’s not a ton of resources out there for terminally ill cancer patients like with kids. Because nobody wants to write that book, nobody wants to you know, nobody wants to spend their time on that. (Stage III glioma, children aged 2, 4, expecting)
Need for support
Parents shared challenges associated with a cancer diagnosis in young adulthood and how being a parent compounded their need for more support. A father shared
I always felt like the young adult population kind of gets left out. . .there’s a void that needs to be filled. Because a lot of times, people, they could still be in school, they could just be out of school, they can be starting families, there’s a lot of big moments going on and then cancer comes in, and you have to, to the best of your ability pause a lot of those things like. . . if you have kids and a family, especially if you’re one of the main breadwinners there’s a lot of stuff you can’t just pause. (Leukemia, child aged 3)
Parents also shared a need for caregiver support. Parents explained that in addition to the general caregiving burden experienced by their partners, these individuals had the additional challenge of increased childcare responsibilities. One father shared
When I was sick, the lion’s share of stuff fell on her [wife]. . . She kind of just had to manage all the kids, which was never while she was worrying about me dying, right. . . My wife ended up taking on a lot of the stuff that we would share. . . She really did have to do most of the parenting because I wouldn’t have the energy for it, or I wouldn’t have the attention for it. (Stage IV colorectal cancer, children aged 10, 12, 13, 14, 15)
Discussion
This study had two main purposes: to understand the daily experiences and occupational performance challenges of parents living with and beyond cancer; and to identify gaps in resources, knowledge and support that could be filled by supportive programming. Four main themes emerged from the data. They included (1) changes in occupational performance related to cancer and its treatment, (2) cancer changes co-occupational performance, (3) parent concerns, and (4) need for information and support.
The parent responses in the interview provided clear and compelling descriptions of the impact of cancer on everyday life. Parents described daily challenges they experienced in both occupational and co-occupational performance. They spoke with deep emotions, including guilt and sadness, about the impact that cancer had on their ability to care for themselves while also caring for others. They also spoke of the gratitude and pride they had in their children’s ability to step up and assume family responsibilities. They noted concerns for their own and their children’s mental health and parent child communication. Specifically, parents wanted cancer care teams to provide support for their mental health and the mental health of their children and developmentally tailored resources to promote communication about their illness.
While these results are consistent with the psychosocial oncology literature, they address some important gaps. First, findings from this study provide rich insights into the experiences of fathers, who accounted for approximately 60% of the study sample. Although the existing literature on the experience of fathers with cancer is limited, studies have reported that fathers have concerns about their role as financial provider, their reliance on partners for caring and for communicating with their children about illness concerns, guilt over reduced parental involvement, and a struggle with disrupted role performance (O’Neill et al., 2013, 2018). A recent meta-analysis confirms that fathers voice concerns about their children’s emotional well-being and fear of missing developmental milestones (Li et al., 2024). Our findings are consistent with this literature, but in addition, fathers reported significant restrictions in parenting activities such as playing with children, helping with homework, and performing baby care activities. They emphasized the impact of fatigue, cognitive changes, and physical limitations on their ability to interact with their children and associated missed opportunities for bonding. Despite these challenges, many fathers also reported positive impacts on parenting, such as a re-evaluation of priorities and an opportunity to create positive memories. Mothers and fathers equally expressed concerns about their children’s well-being and deep sadness over disrupted parenting. While parents with both early- and late-stage cancers expressed these concerns, they were reported more often by parents with late-stage cancers. Consistent with previous literature, parents with advanced cancer reported concerns about missing out on their children’s future lives, loss of parental roles, and challenges with communicating around their illness (Caparso et al., 2021).
Second, the study provides important insight regarding the experiences of parents with very young children, including infants and toddlers, a group that has received limited attention in the literature (Newman et al., 2023). Parenting infants and toddlers while living with cancer is characterized as a period of role disruption, emotional stress, and heightened concerns about attachment and development (Li et al.,2024; Migliaccio et al., 2024; Romare Strandh et al., 2025). Parents highlighted challenges associated with hands-on child-centered bonding activities with their young children, including difficulty lifting children into or out of their cribs and providing baby care (e.g. bathing, diapering) due to fatigue, pain, and other physical symptoms. Parents also spoke of the emotional consequences of disrupted early bonding experiences such as children’s reactions to altered appearance from scars. They also had a strong desire to be home, in place of the hospital, to play with their children. These cancer-related experiences are in addition to the challenges generally reported by parents with very young children, including difficulty finding time for self-care and balancing caregiving and other daily routines (Romare Strandh et al., 2025; Semple and McCance, 2010).
Implications for practice
Occupational therapy practitioners are uniquely positioned to address the complexity of parenting with cancer. Using a holistic, occupation-centered approach, practitioners can adopt a ‘parent-centric’ model of care (McGrath et al., 2025) that acknowledges parents’ dual needs for managing their illness while maintaining meaningful engagement with their children and families. In practice, occupational therapy practitioners can focus on interventions that target occupational and co-occupational performance of parents. They can do this by optimizing child and family routines, modifying environments to support child and family focused activities, providing strategies to promote developmentally appropriate parent child communication and supporting the creation of parent-child legacy projects.
Limitations
The study sample consisted of mainly non-Hispanic, highly educated participants primarily living in the United States and, as a result, the findings may not apply to populations from other countries or racial/ethnic groups. As data collection took place during the COVID-19 pandemic, in-person recruitment efforts were difficult. Most participants were recruited via online support groups and cancer organizations, which may also have influenced characteristics of the sample in unknown ways.
Conclusion
This study sought to explicitly understand the daily experiences and occupational performance challenges of parents living with and beyond cancer and the gaps in resources, knowledge, and support that could be filled by supportive programming from the perspective of parents. Results highlighted the daily challenges parents with cancer experience beginning at diagnosis and lasting through survivorship. Across age, gender, stage, and type of cancer, parents shared similar concerns that their diagnosis and associated challenges were negatively affecting their children. Parents also highlighted a significant need for information and support to facilitate parenting. Results indicate an expanded role for occupational therapy in oncology care to support parenting roles and occupations.
Key findings
Parents want help managing the impact of cancer on themselves, their children and families.
A gap exists between the needs of parents living with and beyond cancer and services they receive.
What the study has added
This study provides in-depth understanding of daily experiences of parents living with or beyond cancer and highlights an expanded role for occupational therapy practitioners in oncology practice.
Supplemental Material
sj-docx-1-bjo-10.1177_03080226261454922 – Supplemental material for Parenting with and beyond cancer: Occupational and co-occupational performance challenges and unmet needs
Supplemental material, sj-docx-1-bjo-10.1177_03080226261454922 for Parenting with and beyond cancer: Occupational and co-occupational performance challenges and unmet needs by Robin Newman, Laura Koszer, Margaret Ingolia, Wendy J. Coster and Jana M. Iverson in British Journal of Occupational Therapy
Footnotes
Acknowledgements
The authors wish to thank the parents who shared their experiences with us. The authors also thank Laura Stursberg and Brianna Pinto for their efforts in participant recruitment on this study.
Ethical considerations
The study was approved by the Boston University Charles River Campus Institutional Review Board on 5/24/2021.
Consent to participate
All participants provided written informed consent.
Author contributions
All authors researched literature and conceived the study. RN was involved in protocol development and gaining ethical approval. R.N. and L.K. were involved in patient recruitment. All authors were involved in data analysis and writing of the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this project was supported by Boston University Sargent College of Health and Rehabilitation Sciences.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Patient and public involvement data
During the development, progress, and reporting of the submitted research, Patient and Public Involvement was included in the conduct of the research.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.