
Abstract
Introduction:
Attention Deficit Hyperactivity Disorder (ADHD) significantly impacts children’s social skills and participation, affecting their daily functioning.
Objectives:
This study aimed to compare social skills and participation of children with ADHD to those of typically developing peers, from maternal perspective.
Methods:
A comparative cross-sectional study was conducted with 103 mothers (52 mothers of children diagnosed with ADHD recruited from a child and adolescent psychiatry clinic and 51 mothers of typically developing children recruited using community-based snowball sampling). Groups were matched and comparable in key sociodemographic variables (p > 0.05). Data were collected using the Child and Adolescent Participation Scale (CASP) and Social Skills Questionnaire (SSQ).
Results:
Children with ADHD had significantly lower social skills (SSQ total) and participation (CASP total) scores than the control group (both p < 0.001; r = 0.86 and r = 0.86, respectively). Deficits were noted across all SSQ subdomains. Lower participation was observed in home, school, and home–community domains, while no significant difference was found in neighborhood and community participation (p = 0.506).
Conclusions:
Maternal perspectives provide valuable real-world insights into the social and participation challenges experienced by children with ADHD. The findings suggest that family-centered occupational therapy approaches may be relevant for supporting social competence and participation in everyday occupations.
Introduction
Attention Deficit Hyperactivity Disorder (ADHD) is a neurodevelopmental disorder characterized by persistent patterns of inattention, hyperactivity, and impulsivity that interfere with functioning or development (American Psychiatric Association, 2013). It affects approximately 5–7% of children worldwide, making it one of the most commonly diagnosed childhood psychiatric disorders (Martin et al., 2025; Polanczyk et al., 2014). Recent evidence continues to indicate that ADHD remains highly prevalent in school-aged populations and is associated with broad functional challenges across developmental domains. Contemporary reviews emphasize that beyond core symptoms, children with ADHD frequently demonstrate heterogeneous social functioning profiles that may influence their everyday participation patterns (Miller et al., 2025). Core symptoms of ADHD include difficulties in sustaining attention, excessive motor activity that is not appropriate to the context, and impulsive behaviors such as interrupting others or difficulty waiting for turns (Willcutt, 2012). These symptoms are often observed across multiple settings, such as home, school, and social environments, leading to significant limitations in children’s academic performance, behavioral regulation, and social skills (Barkley, 2015).
Social skills are essential competencies that enable children to build positive peer relationships, accurately interpret social cues, express their emotions appropriately, and adapt to various social contexts. These skills develop gradually throughout childhood and are shaped by the child’s cognitive capacity, emotional maturity, and environmental conditions (Gresham et al., 2010; Parke et al., 2021). In children with ADHD, difficulties in executive functions—such as planning, attentional control, and cognitive flexibility—along with impairments in impulse regulation and emotional self-regulation, often hinder the acquisition of core social abilities. These difficulties may manifest as challenges in adhering to social norms, maintaining reciprocal conversations, understanding others’ perspectives, and responding appropriately in social interactions (Mikami et al., 2017). Deficits in these areas frequently lead to challenges in social engagement and increase the likelihood of developing unsuccessful interpersonal relationships (Hoza, 2007). Consequently, children with ADHD are at heightened risk of experiencing negative social outcomes such as peer rejection, exclusion, teasing, or bullying (DuPaul et al., 2024). Glenn et al. (2021) examined how social skills moderate the relationship between aggression and peer rejection, finding that children with higher social skills experienced less peer rejection even when displaying aggressive behaviors. Exposure to such adverse experiences may result in social withdrawal, diminished self-esteem, and a growing tendency toward social isolation (Kawabata et al., 2012). Ultimately, this process may lead to both a quantitative and qualitative decline in social participation, laying the groundwork for persistent limitations in the child’s overall social development (Coussens et al., 2020). Recent systematic reviews have further highlighted that social skill difficulties in children with ADHD are persistent and often require targeted intervention approaches to support adaptive functioning in daily contexts (Sugma et al., 2025). From an occupational therapy perspective, such social skill limitations may act as barriers to effective occupational performance and participation in age-appropriate roles and routines.
According to the World Health Organization’s International Classification of Functioning, Disability and Health for Children and Youth (ICF-CY), participation refers to active involvement in activities across various life settings such as school, family, community, and peer groups (WHO, 2007). Participation is a fundamental component of children’s development and well-being, contributing significantly to the development of a sense of belonging, competence, and identity (King et al., 2003). Within the ICF-CY framework, participation is influenced by the interaction between individual capacities and environmental factors. Social skills—such as initiating interactions, interpreting social cues, and regulating behavior during social exchanges—may therefore facilitate or constrain children’s involvement in everyday activities. For children diagnosed with ADHD, participation is often limited due to behavioral challenges, social difficulties, and insufficient environmental support (Kara et al., 2025). Previous research has shown that children with ADHD may experience reduced participation across home, school, and community contexts, particularly when environmental supports are inadequate (Shabat et al., 2021). These participation restrictions may further influence children’s opportunities to develop and practice social competencies within natural contexts of daily life. From an occupational therapy perspective, participation is understood as a dynamic construct shaped by the interaction between the child’s abilities and contextual demands. Emerging evidence suggests that social functioning difficulties in children with ADHD may extend beyond interpersonal challenges and influence their engagement in everyday roles and routines (Miller et al., 2025; Sugma et al., 2025). These findings highlight the importance of participation-focused approaches in occupational therapy assessment and intervention planning.
From this perspective, social skills and participation can be understood as closely interconnected constructs. Effective participation in everyday contexts such as school, home, and community environments often requires children to interpret social cues, regulate their behavior, cooperate with others, and maintain reciprocal interactions. These interpersonal competencies are considered essential facilitators of children’s engagement in social and collaborative activities (Mikami et al., 2017). Within participation frameworks, children’s involvement in everyday activities is shaped by the interaction between individual capacities and environmental opportunities (Imms et al., 2016). Therefore, difficulties in social skills may limit children’s opportunities to establish peer relationships, engage in shared activities, and participate in structured social environments.
Previous research highlight that parent reports, particularly those from mothers, provide critical insights into the contextual and dynamic nature of social participation in children (Anaby et al., 2014; Coussens et al., 2020; Tarhan, 2023). As primary caregivers, mothers closely observe their child’s strengths, challenges, and patterns of engagement across daily life. Anaby et al. (2014) examined children’s home, school and community-based participation levels through parental reports, revealing the critical role of parents—especially mothers as primary caregivers—in observing children’s interactions with environmental factors and patterns of participation (Anaby et al., 2014). Similarly, Coussens et al. (2020) highlighted that parents perceive their child’s participation as influenced not only by the child’s abilities but also by environmental barriers, available opportunities, and everyday demands, reflecting a multifaceted and dynamic understanding (Coussens et al., 2020). These findings illustrate that maternal perspectives offer a nuanced understanding of participation, encompassing both personal competencies and broader contextual influences.
Previous studies have extensively documented social skill difficulties in children with ADHD, particularly in relation to peer relationships, emotional regulation, and interpersonal communication (Hoza, 2007; Mikami et al., 2017). In parallel, another line of research has examined participation patterns in children with ADHD, focusing on their engagement in daily activities across home, school, and community contexts (Kara et al., 2025; Shabat et al., 2021). Although these studies provide valuable insights into different aspects of social functioning, social skills and participation have often been investigated as separate constructs. However, social skills and participation are conceptually interconnected, as effective engagement in everyday activities often requires the ability to interpret social cues, regulate behavior, and maintain reciprocal interactions. Despite this conceptual relationship, relatively few studies have examined social skills and participation simultaneously within the same analytical framework (Mebostad et al., 2025; Shabat et al., 2021). Furthermore, studies comparing these constructs between children with ADHD and typically developing peers remain scarce. In addition, much of the existing research relies on teacher reports or standardized assessments, whereas fewer studies have explored these relationships based on parental perspectives reflecting children’s everyday functioning in natural contexts (Anaby et al., 2014; Coussens et al., 2020). As primary caregivers, mothers closely observe their children’s patterns of participation and social engagement across daily environments. Therefore, examining social skills and participation together through maternal reports may provide a more ecologically grounded understanding of children’s everyday functioning.
Accordingly, the present study aimed to compare the social skills and participation levels of children diagnosed with ADHD with those of typically developing children based on maternal perspectives. This study contributes to the literature by simultaneously examining social skills and participation in children with ADHD and typically developing peers through maternal reports reflecting children’s everyday functioning. By integrating these constructs within an occupational therapy perspective, the study provides ecologically grounded evidence regarding how social competencies may relate to participation in daily life contexts.
Based on the existing literature, the study hypotheses are as follows:
Methods
Study design
This study, designed as a comparative cross-sectional study, received ethical approval from the Health Sciences University Hamidiye Scientific Research Ethics Committee on 13 February 2025 with decision number 25/9. A priori power analysis was conducted using G*Power 3.1.9.4 software. Based on an effect size of 0.5, 95% statistical power (β = 0.95), and a 5% margin of error (α = 0.05), the minimum required sample size was calculated as 88 participants, with 44 in each group. However, to strengthen the statistical robustness and compensate for potential data loss, a total of 103 participants were recruited: 52 mothers of children diagnosed with ADHD and 51 mothers of typically developing children. All participants were informed about the purpose and procedures of the study, and written informed consent was obtained prior to data collection. Data collection tools included a sociodemographic information form, the Child and Adolescent Participation Scale (CASP), and the Social Skills Questionnaire (SSQ).
Participants
Mothers of children with ADHD were recruited through the Department of Child and Adolescent Psychiatry at Bezmialem Vakif University Hospital. Mothers of children diagnosed with ADHD through a DSM-5-based clinical interview conducted by the Department of Child and Adolescent Psychiatry were identified and referred to the study by the Department Chair, who is also one of the researchers and directly involved in the diagnostic process. The ADHD diagnoses were established as part of routine clinical practice using DSM-5 criteria. The Department Chair only facilitated the referral of eligible participants during routine appointments and was not involved in data collection. All research data were collected independently by the first author (K.E.T.) through standardized parent-report measures to maintain diagnostic objectivity and data independence. Mothers of typically developing children recruited through snowball sampling in the community. The groups were matched on key sociodemographic variables, and no significant differences were observed between groups (p > 0.05).
All data were obtained through maternal responses to standardized questionnaires assessing children’s social skills and participation. Only mothers were included in this study, as they are often the primary caregivers in our culture and have firsthand knowledge of their child’s daily behavior and functional participation across home, school, and community contexts. From an occupational therapy perspective, maternal report is considered particularly valuable because occupational therapists emphasize children’s participation and occupational performance within natural contexts and daily routines (Anaby et al., 2014). Mothers, as primary caregivers, have extensive knowledge of their children’s functional performance across home, school, and community environments. In line with family-centered occupational therapy practice, maternal reports can provide ecologically valid information to inform participation-focused assessment and guide contextually relevant intervention planning (Coussens et al., 2020). Therefore, maternal reports were considered an appropriate primary data source in the current study.
The inclusion criteria for the group of mothers of children with ADHD were (1) being the mother of a child aged 7–11 years diagnosed with ADHD according to DSM-5 criteria, (2) being 18 years of age or older, (3) ability and willingness to complete the study questionnaires. Exclusion criteria were (1) have serious psychiatric disorders or cognitive impairments that may affect their ability to provide reliable information, (2) having a child with co-morbid neurological, genetic, or developmental disorders in addition to ADHD (e.g., autism spectrum disorder, intellectual disability).
The inclusion criteria for mothers in the control group were (1) having a typically developing child aged 7–11 years, (2) being 18 years of age or older, (3) willingness and ability to complete the questionnaires. Exclusion criteria were (1) have serious psychiatric disorders or cognitive impairments that may affect their ability to provide reliable information; (2) having a child with any diagnosed neurological, developmental, genetic, or psychiatric disorders; (3) having a child with chronic medical conditions affecting participation.
Instruments
In this study, a sociodemographic information form, the CASP, and the SSQ were used. CASP was used to evaluate participation across home, school, and community contexts, whereas SSQ was used to assess social skills such as emotion regulation, assertiveness, and group interaction. All questionnaires were completed by mothers based on their knowledge of their children’s functioning in daily life. From an occupational therapy perspective, mothers, as primary caregivers, are well positioned to report on their children’s participation in daily occupations within natural environments.
Sociodemographic information form
In the study, a sociodemographic information form created by the researchers was used. This form included questions about the child’s age, gender, and class, and also questions about the mothers’ age, education level, and monthly household income.
Child and Adolescent Participation Scale
The level of participation was evaluated using a 20-item scale originally developed by Bedell (2009). It measures participation across home, school, and community settings based on information provided by the family. Each item is scored on a 5-point scale, with response options ranging from “age appropriate (full participation)” to “unable to do.” The scale is applicable for children aged 5 and above, with higher total scores indicating a greater degree of participation. For this study, the Turkish version validated by Atasavun Uysal et al. (2018) was used, which demonstrated excellent internal consistency (Cronbach’s α = 0.94).
Social Skills Questionnaire
SSQ, developed by Ataş et al. (2016), consisting of 76 items and 7 sub-dimensions. It was prepared to evaluate the social skill levels of children and adolescents between the ages of 4 and 15. The sub-dimensions of the scale were determined as relationship initiation and maintenance skills, skills related to emotions, skills to cope with aggressive behaviors and impulses, assertiveness skills, problem-solving skills, and skills to communicate and work with groups. Since the scale developed as a 5-point Likert-type scale does not have any reverse scored items, it is scored between 1 and 5, with “Never” being 1 and “Always” being 5. In this respect, the minimum score that can be obtained from the scale is 76 and the maximum score is 380. The high score indicates a high level of social skills. Cronbach Alpha internal consistency coefficient is 0.97 for the SSQ (Ataş et al., 2016).
Statistical analysis
All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 26.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were used to summarize the demographic and main study variables. For continuous variables, minimum, maximum, mean, and standard deviation values were reported. Categorical variables were presented as frequencies and percentages. The assumption of normality was assessed using the Kolmogorov–Smirnov and Shapiro–Wilk tests. Since the data did not meet the assumption of normal distribution, non-parametric statistical methods were applied. The Mann–Whitney U test was used to compare the ADHD group and the typically developing control group in terms of social skills and social participation scores. Spearman rank correlation analysis was performed within the ADHD group to examine the association between social skills and participation scores. A p-value of less than 0.05 was considered statistically significant.
Results
The ADHD group consisted of 53.85% males and 46.15% females, whereas in the control group, the proportion of males was 62.75% and females 37.25%. Regarding grade distribution, the ADHD group showed a concentration in first and second grades (23.07% and 25.00%, respectively), with a similar majority observed in the control group. In terms of maternal educational status, the highest proportions in both groups were among mothers with high school and university degrees (71.16% in the ADHD group and 66.67% in the control group). Maternal employment status was comparable between groups, with 57.70% of mothers in the ADHD group and 64.70% in the control group employed full-time. Income levels indicated that more than half of the families in both groups reported income equal to expenses (50.00% in the ADHD group and 47.06% in the control group). The ADHD and typically developing groups were similar in terms of the mean ages of the children and their mothers, as well as the gender distribution of the children, grade levels, maternal education, maternal employment status, and family income levels (p > 0.05 for all comparisons). The demographic characteristics of the study participants are summarized in Table 1.
Demographic characteristics of children and their mothers.
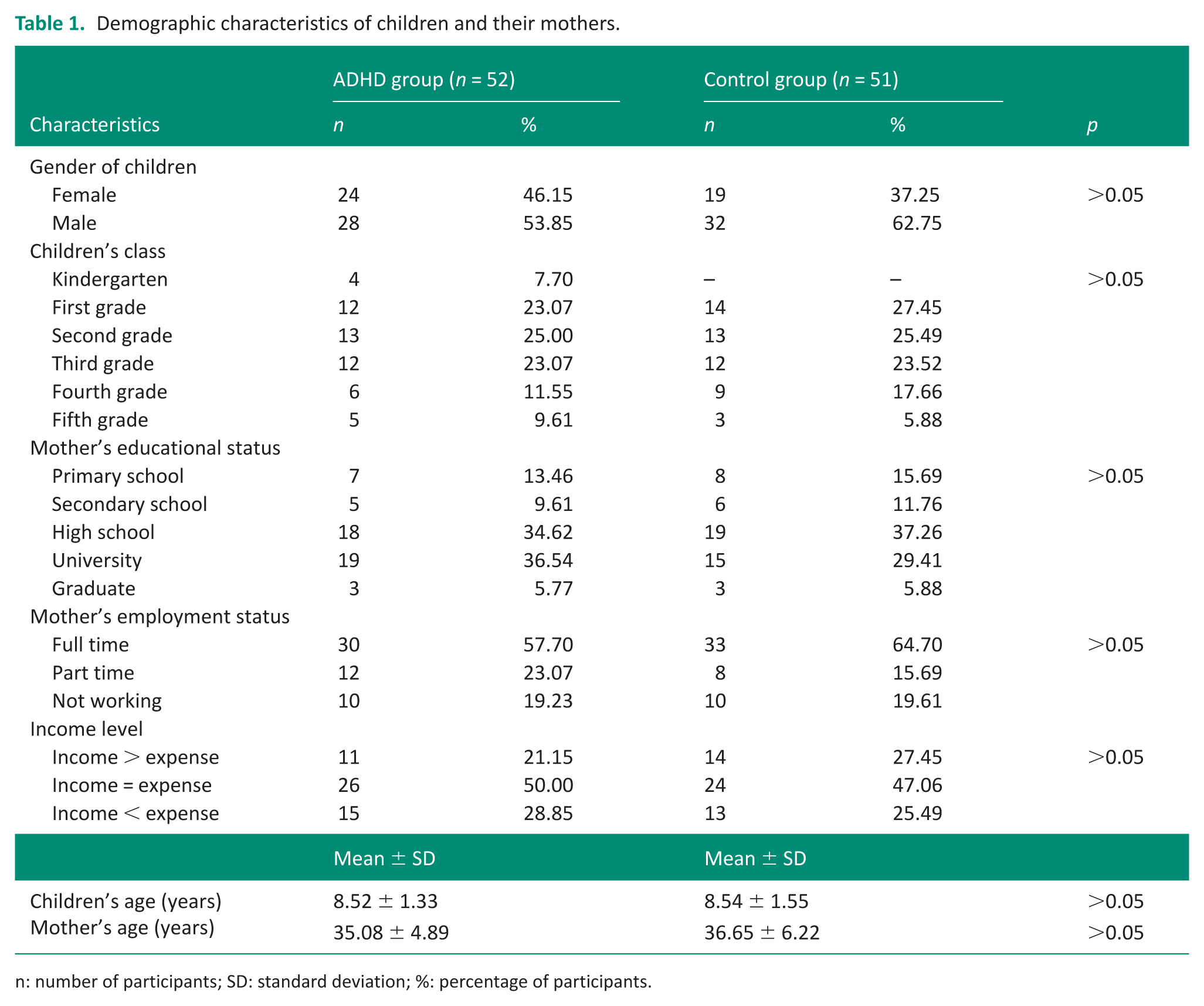
n: number of participants; SD: standard deviation; %: percentage of participants.
The results of children’s social participation and social skills scores filled in according to the mothers’ views are presented in Table 2.
Descriptive statistics of scale scores.
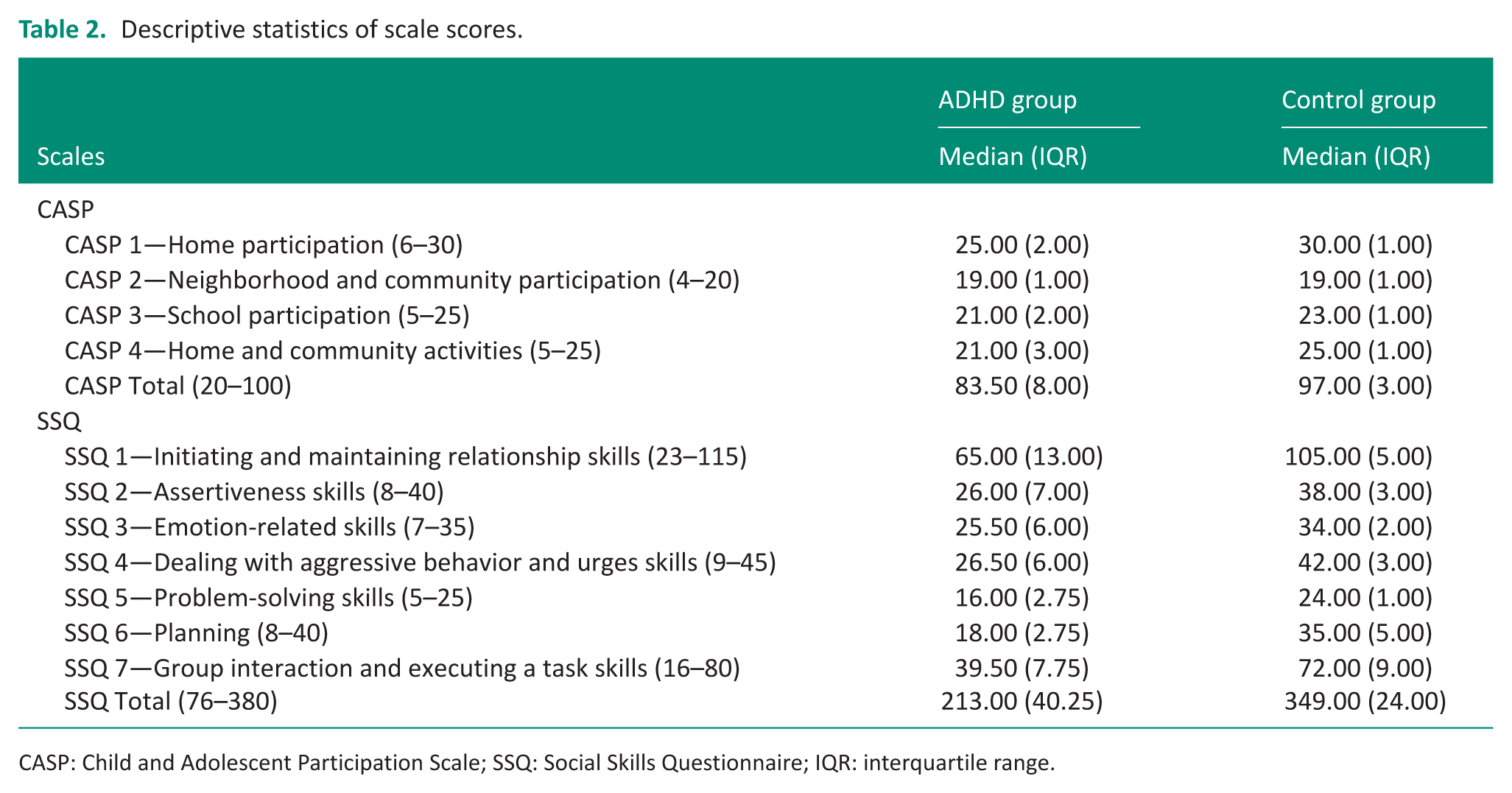
CASP: Child and Adolescent Participation Scale; SSQ: Social Skills Questionnaire; IQR: interquartile range.
The findings revealed that children in the ADHD group had significantly lower levels of social participation and social skills compared to the control group (p < 0.001). In the subscales of the CASP, the ADHD group showed notably lower median scores in home participation (25.00 vs 30.00), school participation (21.00 vs 23.00), and home and community activities (21.00 vs 25.00). However, no significant difference was observed between the groups in neighborhood and community participation (p = 0.506). Regarding the SSQ, the ADHD group scored significantly lower across all subdomains including initiating and maintaining relationships, assertiveness, emotion-related skills, dealing with aggressive behaviors, problem-solving, planning, and group interaction (p < 0.001). The total social skills score was also markedly lower in the ADHD group compared to controls (median: 213.00 vs 349.00). The comparison results are presented in Table 3. Spearman correlation analysis conducted within the ADHD group revealed a strong positive correlation between social skills and participation scores (ρ = 0.919, p < 0.001).
Comparison of social skills and participation.
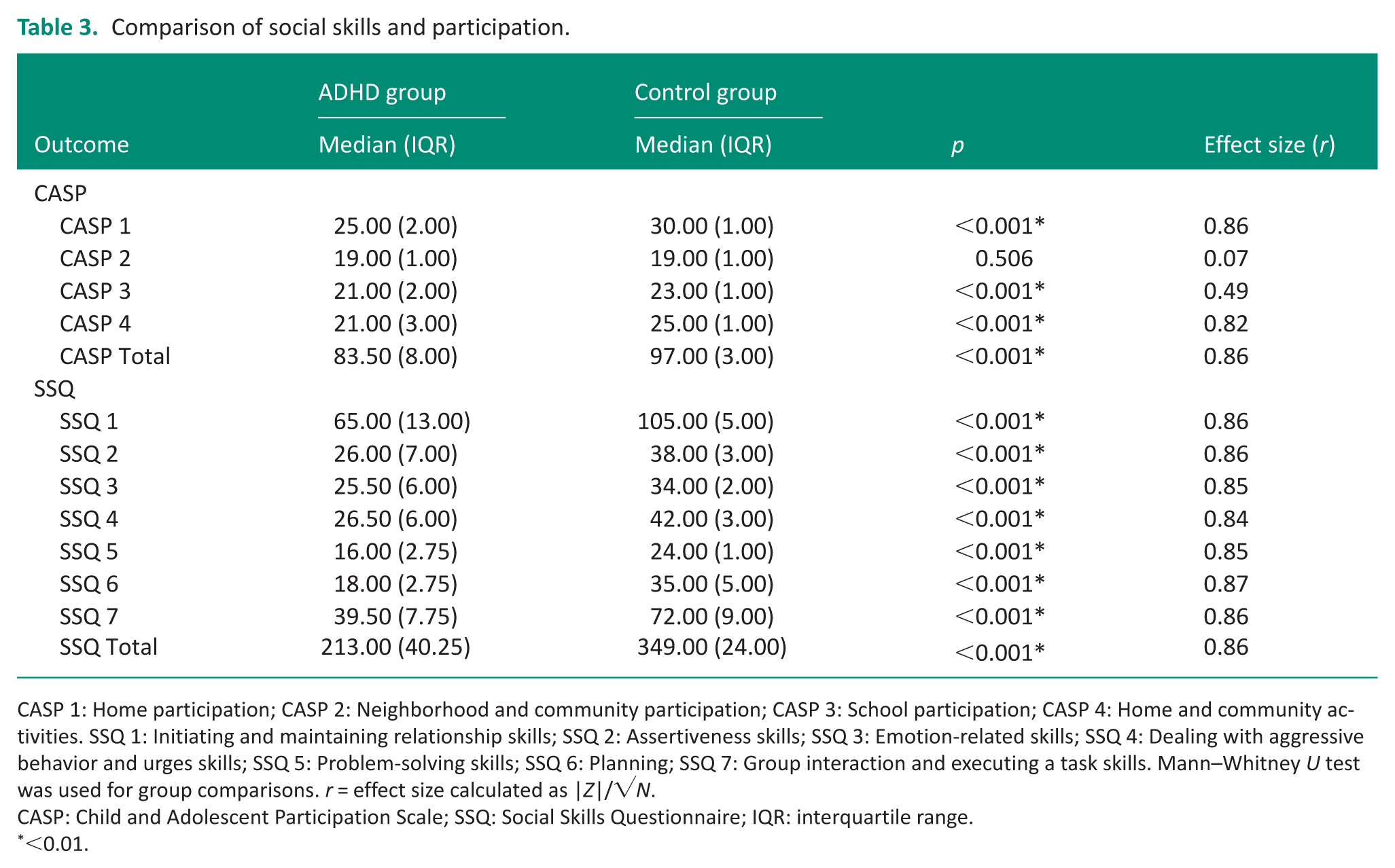
CASP 1: Home participation; CASP 2: Neighborhood and community participation; CASP 3: School participation; CASP 4: Home and community activities. SSQ 1: Initiating and maintaining relationship skills; SSQ 2: Assertiveness skills; SSQ 3: Emotion-related skills; SSQ 4: Dealing with aggressive behavior and urges skills; SSQ 5: Problem-solving skills; SSQ 6: Planning; SSQ 7: Group interaction and executing a task skills. Mann–Whitney U test was used for group comparisons. r = effect size calculated as |Z|/√N.
CASP: Child and Adolescent Participation Scale; SSQ: Social Skills Questionnaire; IQR: interquartile range.
<0.01.
Discussion
The current study aimed to compare the social skills and participation levels of children diagnosed with ADHD and typically developing children based on maternal perspectives. The results revealed that children with ADHD in the present study demonstrated significantly lower levels of participation and social skills compared to the control group. These findings may reflect the multidimensional and complex effects of ADHD on children’s social functioning and suggest that social skills and participation may be important factors influencing overall social functioning.
Participation
In their systematic review, Mendes et al. (2018) reported that children with ADHD have significantly lower levels of engagement in household activities compared to typically developing children, interpreting this as a reflection of their limited social participation. This finding highlights that social participation is not confined solely to interactions in social settings, but represents a multidimensional construct encompassing involvement in daily responsibilities and roles. In line with this perspective, Kara et al. (2025) reported that community participation in children with ADHD may be influenced by the level of social support they receive and the environmental barriers they encounter. The authors further noted that participation may decline particularly in highly structured environments with elevated social expectations. Consistent with the literature, children with ADHD in the current study demonstrated significantly lower levels of social participation in home, school, and combined home–community activities compared to the control group. These findings suggest that ADHD may be associated with multidimensional limitations in children’s daily life functioning and that observed participation restrictions may reflect not only individual characteristics but also contextual and environmental conditions.
One possible explanation for these participation restrictions may be related to executive functioning difficulties commonly observed in children with ADHD. Executive functions play a central role in organizing behavior, maintaining attention, and regulating goal-directed actions in everyday activities. Difficulties in inhibitory control, working memory, and planning may make it challenging for children with ADHD to sustain engagement in structured environments such as home routines and school tasks. Previous studies have shown that executive functioning abilities are closely associated with children’s behavioral regulation and social adjustment (Al-Yagon et al., 2020; Irwin et al., 2021).
Participation is widely recognized as a multidimensional construct shaped by the interaction between individual abilities and environmental opportunities (Imms et al., 2016). Therefore, difficulties in cognitive regulation may interact with contextual demands and limit children’s engagement in everyday occupations. Supporting this perspective, Irwin et al. (2021) reported that working memory deficits in children with ADHD are associated with difficulties in activities of daily living, suggesting that executive functioning challenges may influence children’s ability to manage everyday tasks and participation demands. This perspective, the participation restrictions observed in the present study may partially reflect underlying difficulties in behavioral regulation and goal-directed activity management.
In the current study, participation data were derived from maternal evaluations. This approach offers ecologically meaningful insight, as mothers typically observe their children’s functioning across natural daily contexts. From an occupational therapy perspective, these findings may help clarify how participation restrictions are reflected in children’s everyday contexts. As the questionnaires were completed by mothers based on their observations of their children’s functioning in daily life, the findings may provide clinically relevant information to support participation-focused assessment and family-centered intervention planning for children with ADHD.
A noteworthy finding of the current study was the absence of a statistically significant difference between the ADHD and control groups in neighborhood and community participation. This result suggests that, although children with ADHD in this sample demonstrated marked participation restrictions in home and school contexts, their participation in community-based environments may be more comparable to that of typically developing peers. In a study conducted by Shabat et al. (2021), it was emphasized that environmental modifications and parental support can positively influence community participation. The accessibility of physical environments such as neighborhood parks and playgrounds was highlighted as a factor that may mitigate barriers to participation (Shabat et al., 2021). Furthermore, the less structured nature and more flexible social norms of neighborhood and community activities may enable children with ADHD to express themselves more comfortably and feel less excluded in these settings. Considering that our study relied on maternal perspectives, it is also possible that mothers perceived their children’s community participation as less problematic compared to more structured settings such as the home or school. Additionally, in the Turkish context, the persistence of neighborhood culture as a natural setting for social interaction and the opportunity for children to form more spontaneous relationships in these environments may have influenced this outcome. This finding indicates that community-based activities can be considered as a potential opportunity area in strategies aimed at enhancing the social participation of children with ADHD.
Social skills
Chaudhari (2021) reported that children with ADHD often demonstrate difficulties in recognizing social cues, responding empathetically, and displaying behaviors consistent with social norms, all of which may negatively affect the development of social skills. Similarly, Kožárová (2022) noted that students with ADHD may experience challenges not only with basic social skills such as turn-taking and active listening but also with perceiving subtle social cues within different interaction contexts. In addition to observable behavioral difficulties, executive functioning processes may also play an important role in explaining social skill challenges among children with ADHD. Executive functions such as inhibitory control, working memory, and cognitive flexibility are essential for regulating behavior, interpreting social cues, and responding appropriately during social interactions. Previous research has shown that deficits in executive functioning are closely associated with poorer social skills, emotional regulation difficulties, and challenges in peer relationships among children with ADHD (Al-Yagon et al., 2020; ElAdl, 2024). These regulatory difficulties may limit children’s ability to monitor their behavior, adjust their responses during interactions, and maintain cooperative engagement with peers. From this perspective, the social skill difficulties observed in the present study may partially reflect underlying executive functioning challenges that influence children’s ability to navigate complex social environments. In line with these findings, the current study revealed that children with ADHD demonstrated significantly lower levels of social skills across all subdomains compared to their typically developing peers. These findings suggest that children with ADHD in this sample may experience difficulties in acquiring age-appropriate social competencies and effectively applying these skills in different social environments. In particular, challenges related to initiating and maintaining relationships, emotional regulation, collaborative task engagement, planning, and problem-solving may limit children’s opportunities for social interaction and participation. Moreover, the variability of social skill difficulties observed across different settings (e.g., home, school, and community) highlights the importance of considering contextual influences when evaluating children’s social functioning. These findings underscore the need for individualized and context-sensitive approaches when planning support strategies for children with ADHD.
The magnitude of the group differences observed in SSQ scores was notable, suggesting that these social skill difficulties may be clinically meaningful in the everyday lives of children with ADHD. Although the typically developing group demonstrated relatively high SSQ scores, the distribution of scores did not indicate a clear ceiling effect. Nevertheless, the potential influence of ceiling or floor effects should be considered when interpreting the magnitude of these differences.
Social skills may also play a critical role in shaping children’s participation in everyday contexts. Successful participation in home, school, and community activities often requires effective interpersonal communication, cooperation, and behavioral regulation during social interactions. Difficulties in these areas may therefore limit children’s opportunities to engage in collaborative activities, peer relationships, and structured group environments. In this sense, social skill difficulties may contribute to participation restrictions by affecting children’s ability to navigate the social demands of everyday occupations.
A strength of the current study is that it provides a holistic perspective by examining children’s social skills and participation levels based on maternal perspectives. This approach offers useful insights into children’s functioning in home and community contexts, as mothers typically observe their children across a range of everyday situations. In addition, evaluating both social skills and social participation domains together contributes to a more comprehensive understanding of the social functioning challenges experienced by children with ADHD. However, several limitations should be considered when interpreting the findings. First, the reliance on maternal reports may have increased the influence of subjective perceptions in the evaluations. Because both primary outcome measures were based on maternal reports, the findings may also be susceptible to common method variance. Although standardized and well-validated instruments were used, reliance on a single informant may have contributed to higher observed associations. Second, the cross-sectional design of the study precludes causal interpretations. Additionally, although the groups were comparable in key sociodemographic characteristics, the use of different recruitment strategies for the ADHD and control groups may have introduced potential selection bias. Furthermore, ADHD subtype, symptom severity, and medication status were not systematically analyzed in the present study and may have acted as uncontrolled confounders. Finally, as the sample was drawn from a single geographic and cultural context, the generalizability of the findings may be limited. Future studies may benefit from employing multiinformant and longitudinal research designs, including teacher and child reports, to provide a more comprehensive and dynamic understanding of the social development of children with ADHD.
Conclusion
This study compared the social skills and participation levels of children diagnosed with ADHD with those of typically developing children, based on maternal perspectives. The findings indicated that children with ADHD in this sample demonstrated significantly lower levels of participation in home, school, and combined home–community contexts. These results highlight potential functional challenges in everyday participation among children with ADHD. Notably, the absence of a significant difference in neighborhood and community participation highlights the multidimensional and context-specific nature of social participation, underscoring the importance of evaluating environmental factors. Furthermore, pronounced deficits in social skills emphasize the challenges these children face in social relationships and daily life activities. The reliance on maternal perspectives provides valuable insight into how children’s social functioning is perceived within the family context. Given that the findings were derived from mother-completed questionnaires reflecting mothers’ knowledge of their children’s daily functioning, the results may also help inform participation-focused occupational therapy assessment and family-centered intervention planning.
Key findings
From a maternal perspective, children with ADHD demonstrated significantly lower social skill performance—such as initiating relationships, managing emotions, and engaging in group interactions—compared to their typically developing peers.
Mothers reported lower participation levels of children with ADHD across several environments, including home, school, and combined home–community activities.
A strong positive correlation was found between social skills and participation within the ADHD group, suggesting that lower social skills are associated with greater participation restrictions in everyday activities.
What this study adds
The findings contribute to the evidence base for family-centered practice by highlighting the value of maternal perspectives in understanding children’s occupational performance and participation in everyday contexts.
By examining the relationship between social skills and participation, this study provides empirical evidence that may inform participation-focused assessment and intervention planning in occupational therapy.
The findings provide empirical support for the importance of addressing social skills as a key factor influencing participation in children with ADHD, highlighting the relevance of occupation-focused and family-centered approaches.
Footnotes
Acknowledgements
We thank the participants in this study.
Ethical considerations
The study protocol was approved by the local ethics committee (Health Sciences University Hamidiye Scientific Research Ethics Committee; No: 25/9, Date: 13 February 2025), and written informed consent was obtained from all participants prior to data collection.
Consent to participate
Prior to data collection, all participants were provided with a detailed information sheet outlining the purpose, procedures, and potential risks of the study. Participation was entirely voluntary, and participants were informed of their right to withdraw at any time without any consequences. Written informed consent was obtained from all participating mothers.
Author contributions
Conceptualization: K.E.T. and H.Y. Methodology: K.E.T. and H.Y. Patient referral/recruitment: S.D. Formal analysis: K.E.T. Data curation: K.E.T. Writing—original draft: K.E.T. Writing—review and editing: K.E.T., S.D., and H.Y. Supervision: S.D. and H.Y. All authors read and approved the final version of the manuscript.
Funding
The authors declared no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated and analyzed during the current study are not publicly available due to the confidential nature of the personal health information they contain. The data are securely stored and will only be shared with institutional ethics committees or authorized review boards upon request, in compliance with the informed consent agreement signed by the participants.
Patient and public involvement data
During the development, progress, and reporting of the submitted research, Patient and Public Involvement in the research was included in the conduct of the research.