
Abstract
Introduction:
Distal radius fractures, common in females and males aged ⩾65 and 40–50 years, respectively, cause prolonged pain and activity limitations. Although occupational therapy is a standard postoperative intervention, the relationship between time use, and pain intensity and self-efficacy during the acute recovery phase remains unclear. This study examined these associations shortly after distal radial fracture surgery.
Methods:
This multicentre, prospective, cross-sectional, observational study included 9 facilities. Patients, who underwent volar locking plate fixation and occupational therapy with a splint, were assessed within 1 week postoperatively. The measures included the Occupational Questionnaire, Pain Self-Efficacy Questionnaire, and Numerical Rating Scale. Spearman’s rank correlation coefficient was used because of nonnormal data distribution.
Results:
Twenty-seven participants (25 female; mean age 64.15 ± 9.03 years) were analyzed. Significant positive correlations were found between the time spent on work-related activities and pain self-efficacy on weekdays, and weekends. Contrastingly, we detected no significant correlations between pain-related measures and leisure activities or activities of daily living.
Conclusion:
Work-related activities were positively associated with pain self-efficacy during acute postoperative phase, consistent with findings from populations with chronic pain. As the work activity types were not specified, further research is warranted to clarify on which activities satisfy this relationship.
Introduction
Distal radius fractures are particularly common in women aged ⩾65 years and men aged 40–50 years, and often require occupational therapy (OT) as postoperative treatment (Hagino et al., 1990; Koo et al., 2013; MacIntyre and Dewan, 2016). Postoperative interventions include internal fixation with a palmar locking plate or immobilization with a wrist splint (Orbay, 2000). Occupational therapists are responsible for improving patients’ physical function and providing guidance on daily living activities.
Many patients with distal radius fractures experience severe pain immediately after injury, with approximately 60% reporting moderate-to-severe pain at the time of injury. Moreover, 6 months later, 40% of patients still experience pain or functional impairments (MacDermid et al., 2003). Dekkers and Søballe (2004) evaluated activity limitations and difficulties in early rehabilitation among patients who underwent conservative therapy for Colles fractures using the Canadian Occupational Performance Measure (COPM). The COPM is a client-specific assessment tool of occupational balance, designed to evaluate the patients’ self-rated functionality and satisfaction with that function. It emphasizes the activities usually performed by the patient and highlights the patient’s prioritization of problems in these activities (Dekkers and Søballe, 2004). Although the COPM is one of the measures related to occupational balance, occupational balance itself is associated with occupational domains, the characteristics of specific occupations, and patterns of time use (Wagman et al., 2012). They reported that more than half of the patients experienced difficulties with self-care 1 week after fixation removal, and at 5 weeks, pain and grip strength deficits persisted, with one-third unable to perform self-care adequately (Dekkers and Søballe, 2004). Additionally, Nielsen and Dekkers (2013) conducted a 1-year follow-up study of patients with distal radius fractures, tracking their occupational performance from the time of immobilization removal, and found that problems persisted in self-care, work, and leisure activities even 1 year later. These findings suggest that distal radius fractures are more common in women and patients tend to experience prolonged pain and difficulties with activities of daily living (ADL).
Pain is defined as an unpleasant sensory and emotional experience associated with actual or potential tissue damage (Raja et al., 2020); it is a complex phenomenon involving not only tissue damage but also perception and emotion. Therefore, recent studies have suggested that pain assessment using a single scale is insufficient and that multifaceted evaluation, including emotional aspects, is necessary (Malhotra and Mackey, 2012).
Furthermore, pain is classified into acute and chronic; acute pain can progress to chronic pain (Glare et al., 2019). In distal radius fractures, pain during the acute phase may progress to chronic pain, accompanied by complex regional pain syndrome or prolonged postoperative pain (Dutton and Rhee, 2021).
Moreover, in patients with distal radius fractures, a gap between patient expectations and reality regarding pain and functional recovery during the recovery period has been identified, along with pain-related psychological issues such as fear and anxiety (Moos et al., 2024). While psychological factors such as self-efficacy are considered important for improving these issues, specific intervention methods have not yet been sufficiently established (Moos et al., 2024). In pain research, self-efficacy has been assessed using the Pain Self-Efficacy Questionnaire (PSEQ), designed to measure self-efficacy in the presence of pain (Adachi et al., 2014). This instrument measures multiple domains of self-efficacy, encompassing not only physical functioning but also social interactions and engagement in valued activities (Adachi et al., 2014). However, in patients with chronic pain, a correlation has been demonstrated between pain self-efficacy and occupational balance (Nielsen et al., 2024), and the importance of occupational balance has also been highlighted in the field of pain research. However, studies on acute pain are limited.
Additionally, occupational balance is influenced by the occupational domain, the characteristics of different occupations, and patterns of time use (Wagman et al., 2012). Against this background, this prospective observational study aimed to investigate the associations among occupational balance (assessed using an occupational questionnaire), pain intensity, and pain self-efficacy in patients in the acute phase following distal radius fracture surgery. The results were statistically analyzed.
Methods
This study was conducted as a prospective, multicenter, cross-sectional observational study in accordance with the Strengthening the Reporting of Observational studies in Epidemiology: Explanation and elaboration statement.
Study design
This was a prospective, multicentre, collaborative, cross-sectional observational study. The Ethics Committee of the affiliated institution and the Ethics Committees of the participating institutions approved this study. Informed consent was obtained from all patients via video. The research collaborators were responsible for playing the video used for informed consent and receiving the data recorded by the participants, while the researchers collected and analyzed the data.
Study population
The inclusion criteria for the research facilities were facilities where orthopedic surgeons were employed and underwent bone fixation surgery, occupational therapists conducted rehabilitation for distal radius fractures, and where occupational therapists created palmar cockup splints. Facilities that met these criteria were invited to participate in the study. Facilities that provided informed consent for research collaboration were also included. The inclusion and exclusion criteria were based on previous studies and legal considerations for Japanese adults (Nielsen and Dekkers, 2013). The selection criteria for the patients were (1) adult patients aged 20 years or older, (2) patients with a unilateral distal radius fracture, (3) patients who underwent palmar locking plate surgery at the study facility, (4) patients receiving OT at the study facility, and (5) patients who could understand the questionnaire items and answer them in their own handwriting (either hand was acceptable). Additionally, patients for whom occupational therapists had created splints were included in this study. Given the variety of external fixation methods, these criteria were adopted to ensure consistency in surgical intervention across participants. The exclusion criteria were (1) history of stroke (cerebral infarction, cerebral hemorrhage) or neuromuscular disorders, (2) bilateral distal radius fractures or tissue damage involving nerves or blood vessels, (3) patients with concomitant injuries such as lower limb fractures, (4) patients under 20 years of age, (5) patients with obvious cognitive impairment, mental disorders, or higher brain dysfunction, and (6) patients unable to answer the questionnaire in their own handwriting (either hand was acceptable). In this study, the PSEQ and OQ were self-administered questionnaires requiring responses that reflected participants’ intentions; therefore, the exclusion criteria were defined to account for this requirement.
Ethics
This study was conducted after sending request letters to each participating institution, explaining the purpose and procedures of the study and obtaining written consent for participation from each facility. All participating institutions provided written consent prior to the commencement of the study. Informed consent was obtained from all participants through video explanations, and data were collected only from those who agreed to participate. This study was approved by the Ethics Review Committee of the affiliated institution.
Sample size
The sample size was calculated using free software G*Power for statistical power analysis, with power set at 0.8, significance level (α) at 0.05, and effect size set at 0.5 based on correlation coefficient testing, resulting in 21 participants. Considering potential study dropouts, the sample size for this study was set to 30 participants.
Data collection
Following surgery for distal radius fractures, occupational therapists created splints and administered the following assessments within 1 week: Occupational Questionnaire (OQ), Numerical Rating Scale (NRS), and Japanese version of the PSEQ. The NRS was selected as the pain assessment tool because it has been widely used in previous studies on distal radial fractures (Blomstrand et al., 2023). Furthermore, as chronic pain-related studies have reported correlations between NRS and PSEQ, both scales were included in this study (Hirata et al., 2021).
Additionally, demographic information (age, sex, AO classification, preoperative waiting period, presence of cohabitants, dominant hand, and injured side) was collected from the medical records. The AO system provides a comprehensive classification of long-bone fractures, providing standardized terminology and classification (Marsh et al., 2007; Meinberg et al., 2018).
Occupational Questionnaire
The OQ was developed by Smith et al. (1986). It is an evaluation tool based on the Model of Human Occupation (MOHO) designed to collect information about how individuals use their time, measure the types of activities performed during the day, and evaluate satisfaction, value, and enjoyment of activities. This is a standard assessment scale used to evaluate daily activities. Participants record specific activities performed every 30 minutes from waking up to bedtime. Activities are classified into one of the following categories: work, ADL, leisure, or rest. The time spent in each category (work, ADL, leisure, and rest) was evaluated. Its reliability and validity were demonstrated in a pilot study conducted by Smith et al. (1986). The OQ has also been utilized in occupational therapy research in Japan (Sasaki and Tanimura, 2025).
Additionally, occupational balance is related to time use (Wagman et al., 2012). Because the OQ evaluates time use, it was used in this study.
Numerical Rating Scale
Pain was assessed using the NRS. Participants are asked to rate their current level of pain on a 10-point scale, with 10 representing the worst pain they experienced and 0 representing no pain.
In this study, two items were measured: the degree of pain felt during daily activities and the degree of pain felt at bedtime. The measurement method for NRS was reported by Jensen et al. (1994); the present study used the 11-item method.
PSEQ Japanese version
The Japanese version of the PSEQ Japanese version was used to assess pain self-efficacy. The PSEQ is a self-report questionnaire consisting of 10 items, with responses ranging from 0 (no confidence at all) to 6 (complete confidence). The total score was calculated using a 7-point scale. The reliability and validity of this assessment method were demonstrated by Adachi et al. (2014). The Japanese version of the PSEQ has demonstrated high internal consistency (Cronbach’s α = 0.94), confirming its reliability and validity in Japanese populations (Adachi et al., 2014).
Measurement method
Occupational therapists at the collaborating research facilities created the splint, and the study participants completed the questionnaire within 1 week. Basic information (age, sex, AO classification, waiting period for surgery, medical history, presence of cohabitants, dominant hand, and injured side) was obtained from the medical records by the occupational therapists at the collaborating research facilities.
Data analysis
For the OQ, the total minutes for each item was calculated, and for the PSEQ the total score across all items was computed. For each item of the OQ (work, ADL, leisure, and rest), the time, NRS, and PSEQ scores were analyzed using the Shapiro–Wilk test. If normality was confirmed, Pearson’s correlation coefficient was used; otherwise, Spearman’s rank correlation coefficient was used. The significance level was set at 5%. Statistical analyses were performed using IBM SPSS Statistics for Windows, Version 28.0 (IBM Corp., Armonk, NY, USA).
Results
Demographic characteristics
Nine facilities were selected as the target facilities. The basic characteristics of the participants and the evaluation results are presented in Table 1. Thirty participants were initially enrolled, but due to missing data, the final sample consisted of 27 participants (2 men, 25 women). The mean age was 64.15 ± 9.03 years. The AO classification was C in 17 cases, B in 7, and A in 3. The right hand was injured in 16 patients and the left hand in 11 patients. The right and left hand was dominant in 25 patients and 1 patient, respectively; 1 patient was ambidextrous. The mean preoperative waiting period was 5.15 ± 3.06 days.
Participants characteristics and evaluation measures.
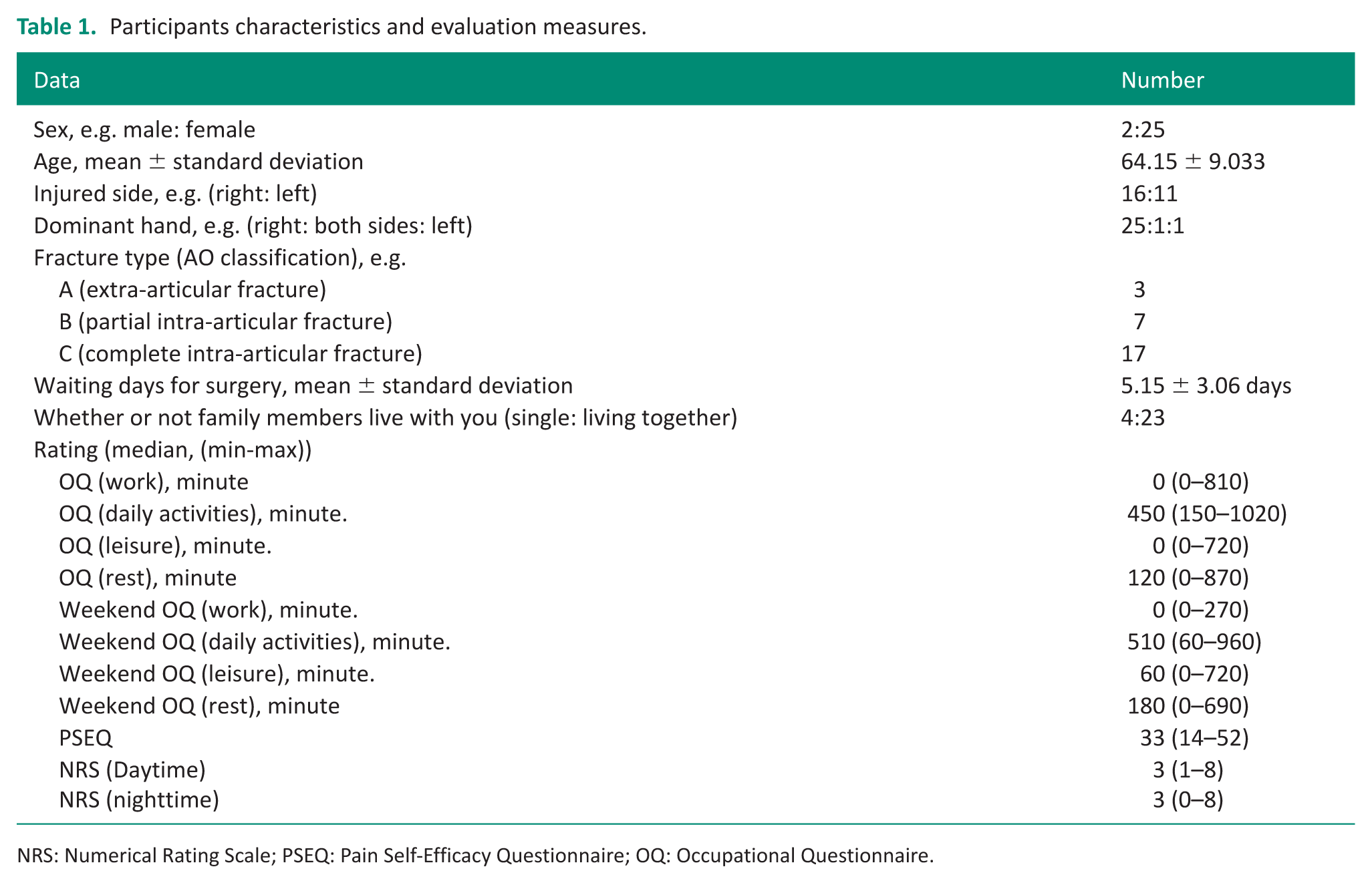
NRS: Numerical Rating Scale; PSEQ: Pain Self-Efficacy Questionnaire; OQ: Occupational Questionnaire.
Correlation between OQ and other evaluations
Correlation with OQ was assessed using the Shapiro–Wilk test, which did not confirm normality; therefore, Spearman’s rank correlation coefficient was used. The detailed results of the statistical analyses are presented in Table 2. The main results are summarized as follows.
Relationship between OQ and other evaluations.
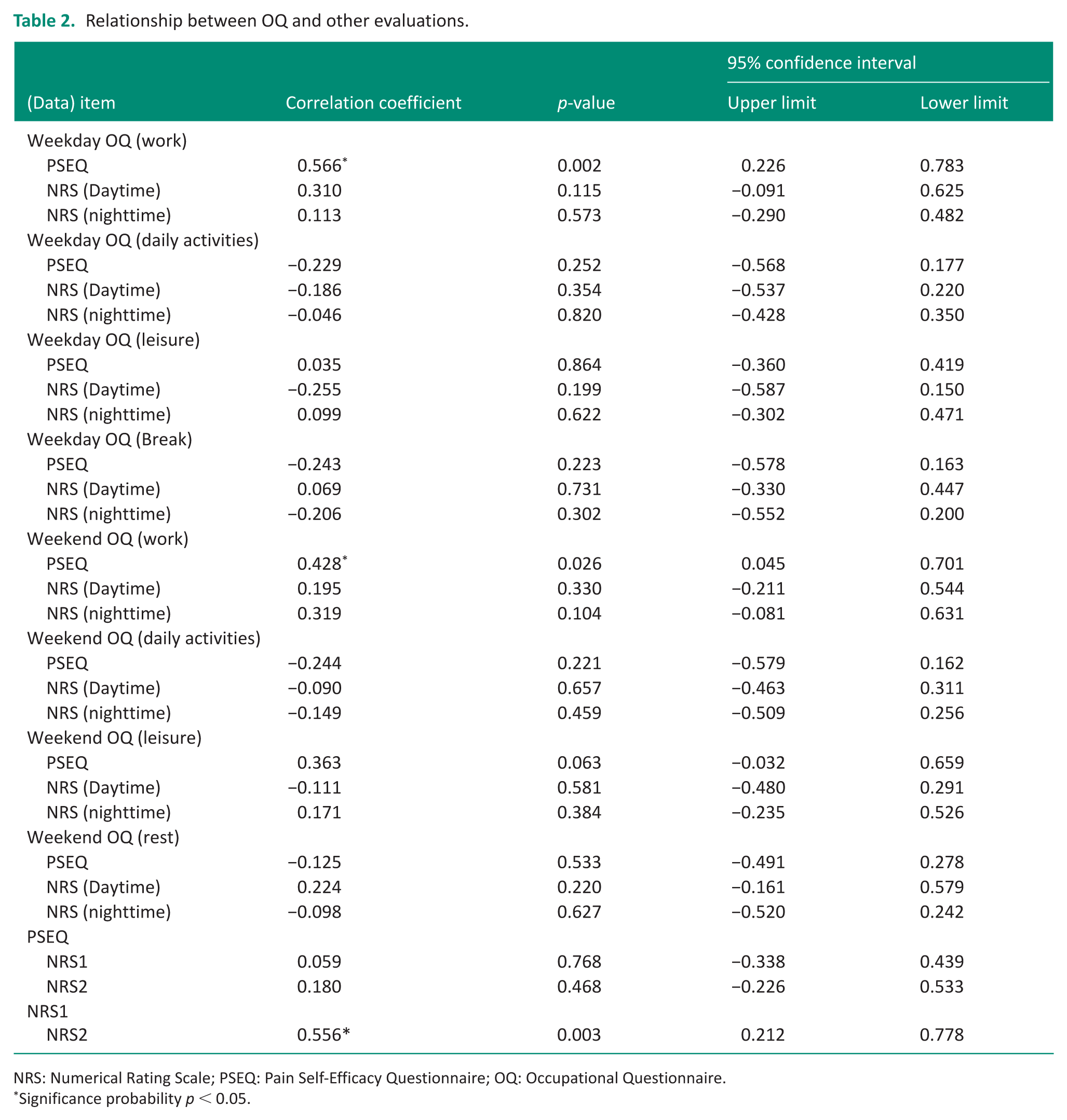
NRS: Numerical Rating Scale; PSEQ: Pain Self-Efficacy Questionnaire; OQ: Occupational Questionnaire.
Significance probability p < 0.05.
The correlations between OQ (weekdays) and pain intensity and pain self-efficacy were Work and PSEQ: rs = 0.566 (p = 0.002), work and daytime NRS: rs = 0.310 (p = 0.115), and work and nighttime NRS: rs = 0.113 (p = 0.573). No significant correlations were found between daily activities and PSEQ: rs = −0.229 (p = 0.252), daily activities and daytime NRS: rs = −0.186 (p = 0.354), and daily activities and nighttime NRS: rs = −0.046 (p = 0.820). No significant correlations were found between leisure and PSEQ: rs = 0.035 (p = 0.864), leisure and daytime NRS: rs = -0.255 (p = 0.199), and leisure and night time NRS: rs = 0.099 (p = 0.622)
No significant correlations were found between rest and PSEQ: rs = −0.243 (p = 0.223), rest and daytime NRS: rs = 0.069 (p = 0.731), and rest and nighttime NRS: rs = −0.206 (p = 0.302).
The associations between OQ (weekend), pain intensity, and self-efficacy were as follows: work and PSEQ, rs = 0.428 (p = 0.026); work and daytime NRS, rs = 0.195 (p = 0.330); and work and nighttime NRS, rs = 0.319 (p = 0.104). No significant correlations were found between weekend daily activities and PSEQ: rs = −0.244 (p = 0.221), weekend daily activities and daytime NRS: rs = −0.090 (p = 0.657), and weekend daily activities and nighttime NRS: rs = −0.149 (p = 0.459). No significant correlations were found between weekend leisure and PSEQ: rs = 0.363 (p = 0.063), weekend leisure and daytime NRS: rs = −0.111 (p = 0.581), and weekend leisure and nighttime NRS: rs = 0.171 (p = 0.384). No significant correlations were found between weekend rest and PSEQ: rs = −0.125 (p = 0.533), weekend rest and daytime NRS: rs = 0.224 (p = 0.220), and weekend rest and nighttime NRS: rs = −0.098 (p = 0.627).
Statistically significant differences (p < 0.05) were observed between the OQ work items and PSEQ on weekdays and weekends, indicating moderate positive correlations. The analyses demonstrated that daily activities, leisure activities, and rest showed no significant correlation with pain self-efficacy or pain intensity.
Discussion
This study investigated the relationship between pain self-efficacy (PSEQ) and work items on the OQ in patients who underwent surgery for distal radius fractures in the acute phase and had splints applied.
This study was conducted without restricting participants by sex; however, women comprised a higher proportion of the sample, which is consistent with the findings of previous epidemiological studies (Hagino et al., 1990; MacIntyre and Dewan, 2016). The NRS and PSEQ scores exhibited a correlation similar to the findings of previous studies on chronic pain (Tsuji et al., 2019).The results showed a significant positive correlation between pain self-efficacy and the work items on the OQ on weekdays and weekends. Based on these findings, the following points are discussed:
Relationship between occupation and pain self-efficacy
The results of this study demonstrated a significant positive correlation between occupation (particularly work-related activities) and pain self-efficacy. While studies on pain self-efficacy in patients with distal radius fractures are limited, previous research has shown that OT can improve pain self-efficacy and quality of life (Theofilou and Tzavella, 2023). In a study on patients with chronic pain, pain self-efficacy was reported to have a stronger correlation with occupational balance than with COPM satisfaction (Nielsen et al., 2024), suggesting a relatively low association with COPM.
Occupational balance is related to the occupational area, characteristics of different occupations, and time use (Wagman et al., 2012). Using the OQ, an assessment tool for occupational balance, to examine its association with pain self-efficacy yielded similar results. However, these findings should be interpreted with caution. The median time spent in work-related activities on both weekdays and at weekends was 0 minute, with wide ranges, indicating a skewed distribution. Consequently, the significant association between work-related activities and pain self-efficacy may have been influenced by a subgroup of participants who engaged in work-related activities. The present findings thus tend to indicate that among some patients, work-related activities may be associated with pain self-efficacy, although these associations should not be interpreted as evidence that work is beneficial for all patients following distal radius fracture surgery.
In this study, we detected no significant correlations between pain-related measures and leisure activities or ADL. Although there was a wide range of time spent in these activities, variability alone may be insufficient to explain the absence of significant correlations, given that correlation analysis examines relationships over a range of values. Consequently, the factors contributing to the lack of significant associations between leisure activities and ADL and the intensity of pain or pain self-efficacy remain to be established. However, recent studies have examined pain during leisure time and reported that physical activity may reduce the need for pain medication and alleviate chronic pain (Johansson et al., 2025; Kyriakidis et al., 2025). On both weekdays and at weekends, the time spent engaging in leisure activities showed wide variability (weekdays: median 0 minute, range 0–720 minutes; weekends: median 60 minutes, range 0–720 minutes). However, this variability should be interpreted as a descriptive characteristic of the sample population rather than as a sufficient explanation for the absence of significant correlations.
Furthermore, we detected no significant correlations between pain-related measures and ADL, which similarly showed wide variability on both weekdays and at weekends (weekdays: median 450 minutes, range 150–1020 minutes; weekends: median 510 minutes, range 60–960 minutes). However, as with leisure activities, this variability should be viewed a descriptive characteristic rather than an explanation for the absence of significant correlations. In occupational therapy studies on distal radius fractures, interventions targeting early return to ADL beginning 2 weeks postoperatively have been investigated, reporting positive outcomes, including promotion of the rehabilitation process and development of psychosocial resources and abilities in patients with distal radius fractures (Collis et al., 2022, 2024).
Although this present study demonstrated a correlation only between pain self-efficacy and work, recent research suggests that leisure activities may also be effective in reducing pain, and interventions in ADL are currently being explored. Furthermore, occupational therapists’ consideration of individual, work, and environment can enhance activity and participation (Bredy et al., 2025). Therefore, future research may clearly elucidate the relationship between work and pain by analyzing the amount of time spent working.
Relationship between Occupation (specific work) and pain self-efficacy from a pain medicine perspective
In pain medicine, prolonged pain following surgery is referred to as postoperative chronic pain (Montes et al., 2015). Psychological and social factors (psychological vulnerability, stress, anxiety, catastrophic thinking, and low expectations or anxiety regarding returning to work) have been identified as risk factors (VanDenKerkhof et al., 2013). This study focused on the acute pain phase. However, the association between work and self-efficacy regarding pain was clarified, and the results were similar to those of previous studies on chronic pain and postoperative chronic pain. However, research on the acute pain phase is limited, and further studies are needed to clarify the psychosocial factors specific to the acute phase.
Additionally, self-efficacy regarding pain is associated with reductions in psychological distress and physical disability, and is widely used as an indicator for evaluating chronic pain (Keefe et al., 2004). Recently, its application during the acute pain phase has advanced (Wang et al., 2024); and studies involving populations without chronic pain have reported that pain self-efficacy mitigates pain and anxiety (Karkkola et al., 2019). Patients with high self-efficacy can effectively manage their pain (Jackson et al., 2014). In this study, the positive correlation between work activity and pain self-efficacy suggests that patients’ mental states and social connections may contribute to their ability to cope with pain. Consequently, it is conceivable that engagement in work-related or other meaningful activities during the acute postoperative phase may be associated with the confidence of patients in managing pain. However, given the cross-sectional design of this study, we were unable to determine any causal relationships or the potential role of early activity engagement in preventing chronic pain.
Strengths and limitations
The results of this study demonstrated a correlation between occupation (especially work) and pain self-efficacy. Based on these findings, future studies focusing on time use within a MOHO are recommended.
This study included a large proportion of female participants, the findings for whom may not be directly applicable to male patients with distal radius fractures. In addition, we focused exclusively on the early postoperative period, during which the characteristic of patients may differ from those with long-term conditions. Moreover, the mean participant age was 64.15 ± 9.03 years, and it is conceivable that the findings may not be applicable to older adults. Furthermore, the study was limited to patients who used splints, and thus the results may not be generalizable to patients who undergo other types of external fixation after distal radius fractures. In addition, although we analyzed the total time spent in each OQ category, we did not examine the specific types of work-related activities. Accordingly, in future studies, work-related activities should be classified in more detail to identify which types of activities are associated with pain self-efficacy.
As work content was not specified in this study, it is necessary to clarify the relationship between specific work content and self-efficacy regarding pain in future research.
Conclusion
The results of this study demonstrated that pain self-efficacy was associated with OQ assessments in patients with distal radius fractures during the acute pain phase. In addition, we found that time spent in work-related activities was positively associated with pain self-efficacy during the acute postoperative phase, which is consistent with findings previously reported for populations with chronic pain. However, these finding should be interpreted cautiously as we did not examine the specific types of work-related activities. Collectively, these findings indicate that the use of time may be associated with pain self-efficacy during the acute postoperative phase and should be considered in occupational therapy assessments.
Key findings
In patients with distal radius fractures, pain self-efficacy was positively associated with Occupational Questionnaire scores during the acute pain period.
Work-related activities were positively associated with pain self-efficacy during the acute postoperative phase, consistent with previous findings in chronic pain populations.
What the study has added
This study investigated the relationship between pain assessments and Occupational Questionnaire scores during the acute pain period.
Footnotes
Acknowledgements
The authors wish to thank all the participants who participated in this research.
Ethical considerations
This study was approved by the Ethics Review Committee of Kanagawa University of Human Services (No. 5-22-30).
Consent to participate
Written informed consent was obtained from all the participants at the beginning of the study. The participants were reminded that they could withdraw their consent at any time.
Author contributions
Y.I. and S.S. co-wrote and co-edited this editorial and data analysis.
Funding
The authors declared no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Patient and public involvement data
During the development, progress, and reporting of the submitted research, Patient and Public Involvement in the research was not included at any stage of the research.