
Abstract
Background:
Occupational therapy (OT) in Spain faces challenges of limited visibility and professional integration, particularly for newly graduated therapists. Early years of practice are often marked by isolation and the absence of structured mentorship, hindering skill consolidation and professional identity. Peer mentorship has shown promise internationally as a supportive strategy, but formal programs in Spain remain scarce. This study protocol presents MenTOras, a pilot peer mentorship program designed to enhance professional integration, emotional well-being, and self-confidence among newly graduated occupational therapists in Aragón, Spain.
Methods:
A mixed-methods, quasi-experimental pilot study without a control group will be conducted. Around 20 mentor–mentee pairs will be recruited through the regional professional association. The program comprises six structured mentorship sessions across three phases: initiation, development, and closure. Data will be collected at baseline, post-program, and 6-month follow-up, including quantitative measures of integration, well-being, confidence, and satisfaction, complemented by qualitative interviews.
Results:
Findings will assess feasibility, acceptability, and preliminary effects of the program, and identify mechanisms through which mentorship supports professional growth.
Conclusion:
MenTOras addresses a key gap in Spanish OT by providing a structured, context-sensitive mentorship model. Outcomes will inform future initiatives to strengthen retention, professional identity, and visibility within the healthcare system.
Keywords
Introduction
Occupational therapy (OT) is a well-established health profession in many countries, contributing to the promotion of functional independence, participation, and well-being across diverse populations (Boop et al., 2020; Kannenberg et al., 2015). However, the degree of development, recognition, and integration of OT varies considerably across countries and healthcare systems. Although limited public visibility has been reported in other international contexts, in Spain the profession continues to face particularly low recognition, both within the healthcare system and among the general public (González-Román et al., 2023; León-Herrera et al., 2025). This lack of visibility has specific implications for newly graduated therapists, as it reduces opportunities for workplace integration and hinders participation in structured professional development pathways. It also contributes to the underutilization of occupational therapists within multidisciplinary teams (Atwal and Caldwell, 2005; Simpson et al., 2005), while the absence of systematic mentorship or peer support mechanisms further limits guided learning and professional consolidation for new graduates (Moir et al., 2021; Toal-Sullivan, 2006).
The early years of professional practice are a critical period for consolidating clinical skills, professional identity, and workplace integration (Bowman et al., 2024; Hayward et al., 2013). For many newly graduated occupational therapists, this period is marked by professional isolation—particularly in contexts where they are the sole practitioner within a facility or team. Such isolation can hinder reflective practice, reduce access to experienced role models, and limit opportunities for guided skill acquisition (Solomon et al., 2001; Turpin et al., 2021). In this sense, professional integration can be understood as a multidimensional process that extends beyond employment status alone and encompasses perceived inclusion within professional and organizational contexts, effective participation in multidisciplinary teams, access to professional support networks, confidence in performing professional roles, and alignment with professional identity and values (Moores and Fitzgerald, 2017; Turpin et al., 2021). Without adequate support, early-career professionals may experience heightened stress, uncertainty, and a diminished sense of belonging, factors that negatively impact job satisfaction and retention within the profession. These challenges are compounded by the transition from the structured environment of academic training to the complex and often under-resourced realities of clinical practice (Chee et al., 2023; Kutsyuruba et al., 2022; Parry et al., 2024).
Mentorship has long been recognized as a cornerstone of professional development in health and social care professions. A growing body of international evidence demonstrates that mentorship programs can significantly enhance professional integration, emotional well-being, and self-confidence among novice practitioners (Burgess et al., 2018; McCray et al., 2014). Mentorship provides a structured framework for learning through guided experience, enabling mentees to develop problem-solving strategies, receive constructive feedback, and build a stronger professional identity (Venktaramana et al., 2023). For mentors, these programs offer opportunities for personal reflection, reinforcement of professional roles, and the satisfaction of contributing to the growth of their profession (Gilles and Wilson, 2004). Among various models, peer mentorship has gained increasing attention for its emphasis on reciprocal learning, shared experiences, and egalitarian relationships. These characteristics often make it more accessible and relatable to novice professionals, enhancing its acceptance and perceived value (Cree-Green et al., 2020; Dickson et al., 2021).
Within occupational therapy specifically, mentoring has been explored across a range of international contexts and professional roles. A scoping review by Doyle et al. (2019), synthesizing 20 empirical studies, showed that mentoring is used with occupational therapy students, clinicians, educators and researchers, and across diverse practice settings. Despite heterogeneity in program designs and definitions, common elements include mentoring as a supportive, goal-oriented learning process that develops over time within a relational framework. Reported outcomes include professional skill development, professional identity formation, increased confidence, and the strengthening of professional networks and communities of practice (Doyle et al., 2019).
However, this review also identified important gaps in the occupational therapy mentoring literature, including the limited number of structured programs specifically targeting newly graduated occupational therapists, the predominance of cross-sectional designs, and the lack of clearly described mentoring processes and longitudinal evaluations (Doyle et al., 2019). Individual studies included in the review, such as the evaluation of a formal occupational therapy mentorship program in Canada (Milner and Bossers, 2005), suggest potential benefits but remain context-specific and methodologically heterogeneous.
Despite the recognized benefits of mentorship internationally, few formal mentorship programs exist for occupational therapists in Spain. As a result, many early-career occupational therapists rely on informal support networks or self-directed professional development, which may not fully meet their needs during this critical stage of career transition. This lack of structured peer support represents a missed opportunity to strengthen professional integration, enhance job satisfaction, and improve retention within the workforce. In this context, structured peer mentoring also holds potential to foster professional communities of practice, which are essential for advancing the visibility and impact of occupational therapy within the broader healthcare and social systems (Doyle et al., 2019; Germeroth et al., 2024; Milner and Bossers, 2005).
The MenTOras program was developed to address these gaps by providing a structured peer mentorship model tailored to the needs of recently graduated occupational therapists. The program connects early-career occupational therapists with experienced colleagues, facilitating professional guidance, reflective practice, and emotional support through a series of structured mentoring sessions. By fostering peer connections and professional solidarity, MenTOras seeks to create a supportive environment for early-career occupational therapists to navigate the complexities of practice, build confidence, and develop a stronger professional identity.
This study protocol describes the design and methodology of the MenTOras pilot study. The primary aim is to evaluate the impact of a structured peer mentorship program on professional integration, emotional well-being, self-confidence, and perceived professional development among recently graduated occupational therapists in Aragón (Spain). We hypothesize that participation in MenTOras will significantly improve these outcomes and contribute to the creation of sustainable models of peer mentorship within the profession.
Methods
Study design
This is a mixed-methods, prospective, quasi-experimental pilot study without a control group, employing a successive cohort design (Eldridge et al., 2016). The intervention consists of a structured peer mentorship program pairing experienced occupational therapists with recently graduated colleagues. Data will be collected at baseline (pre-program), immediately after program completion, and 6 months later. The study protocol has been registered in ClinicalTrials.gov (Identifier: NCT07173283) in September 2025.
Participants and eligibility
The study includes two participant groups: recently graduated occupational therapists (mentees) and experienced occupational therapists (mentors).
Recently graduated occupational therapists are defined as individuals who completed their degree within the previous 2 years, regardless of whether they are currently employed in the profession. This intentionally broad definition recognizes that some new graduates may still be navigating their transition into the workforce; accordingly, mentorship can support not only early clinical socialization but also initial professional integration. The ⩽2-year post-graduation window is consistent with skill-acquisition models derived from the Dreyfus framework and Benner’s application of it to clinical practice (Benner, 2004; Dreyfus, 2004). In Benner’s original account, “competent” performance is typically associated with approximately 2–3 years in a comparable clinical role (Benner, 1982). Although the Dreyfus model does not specify timeframes, it emphasizes qualitative shifts in situational understanding and perceptual discrimination as practitioners accumulate meaningful experience rather than simply time in post (Dreyfus, 2004). Crucially, these timelines are heuristic rather than prescriptive: both Benner and the Dreyfus framework stress that experience is not the mere passage of time, but the refinement of practice through repeated engagement with real situations, shaped by contextual factors such as case complexity, supervision, and learning opportunities (Benner, 1982; Dreyfus, 2004).
Mentors, in contrast, must have at least 5 years of clinical or community-based OT experience and be actively practicing at the time of enrollment. Both recently graduated OTs and mentors must be registered members of the Aragon Professional Association of Occupational Therapists (Colegio Profesional de Terapeutas Ocupacionales de Aragón, COPTOA).
The exclusion criteria are applied specifically to the mentor group: occupational therapists who are no longer practicing are not eligible to serve as mentors, as maintaining current clinical engagement is considered essential for providing relevant and credible guidance. For all participants, involvement in other mentorship programs or structured training initiatives with overlapping objectives constitutes an exclusion criterion, to avoid confounding influences on the study’s outcomes.
The study aims to recruit approximately 20 mentor–mentee pairs, yielding a total sample of 40 participants. Given the exploratory nature of this pilot, this sample size is expected to be sufficient for detecting trends and generating hypotheses for larger, future studies.
Justification for absence of control and pilot character
As a pilot study, the focus is feasibility, acceptability, implementation, and detection of potential signals of effect, with the aim of informing the design of subsequent controlled studies with larger samples and validated measures (Thabane et al., 2010).
Recruitment procedures
Recruitment is coordinated through COPTOA and professional social media channels, including LinkedIn and Instagram. Digital posters, infographics, and targeted posts are used to disseminate information about the program ( Supplemental Material, S1 ). Additionally, an informational talk was given at the University of Zaragoza to fourth-year students in the OT degree program, aimed at engaging those who will become new members of COPTOA upon graduation.
Interested individuals voluntarily register by completing a Google Form (provided as Supplemental Material, S2 ), where they provide informed consent and basic demographic and contact data. The form includes a description of the study, data protection information, and a mandatory acceptance of the privacy policies of COPTOA and Google before submission. The research team oversees all aspects of participant screening, matching, and enrollment, ensuring that participation is entirely voluntary and free from any external pressures.
Written informed consent is obtained from all participants prior to commencing the program. After initial registration, participants receive a detailed participant information sheet and a consent form by email. Consent forms are returned to the research team before enrollment and may be signed either manually or using a digital signature, in accordance with the approval granted by the Research Ethics Committee of the University of Zaragoza.
Program development
The MenTOras mentorship program was developed through an iterative process informed by multiple sources. First, the research team reviewed the international literature on mentoring and peer mentoring in occupational therapy and related health professions to identify key components, mechanisms, and reported outcomes of effective programs (Burgess et al., 2018; Dickson et al., 2021; Doyle et al., 2019; Germeroth et al., 2024; Milner and Bossers, 2005; Venktaramana et al., 2023). Second, the structure and content of the program were shaped through discussions among members of the research team, who have experience in occupational therapy education, professional development, and early career support. Finally, informal consultation took place with key stakeholders, including members of the regional professional association (COPTOA) and recently graduated occupational therapists, to ensure that the program was contextually relevant, feasible, and responsive to the needs of early-career practitioners in the Spanish setting.
Intervention
The MenTOras mentorship program spans approximately 6 months and is structured into three main phases: initiation, development, and closure. Each mentor–mentee pair participates in a minimum of six structured mentoring sessions, conducted either online or in person according to participant preference and geographical considerations.
Mentor–mentee pairs are expected to meet on average every 2–3 weeks, with each session lasting approximately 60–90 minutes. The exact frequency, duration, and scheduling of sessions are agreed upon by each pair, allowing flexibility to adapt to individual needs, availability, and professional contexts, while ensuring a minimum level of engagement across all participants.
The duration and frequency of the MenTOras mentorship program were informed by evidence from the OT mentoring literature. A scoping review of mentoring research in occupational therapy reports substantial variability in program length and intensity, with mentoring interventions ranging from short-term programs of 6–8 weeks to longitudinal models lasting up to 2 years, and meeting frequencies varying from weekly to monthly or needs-based formats (Doyle et al., 2019). Within this range, the 6-month duration and bi-weekly to tri-weekly meeting schedule of MenTOras were intentionally designed as a pragmatic and feasible midpoint, allowing sufficient time for relationship development, goal setting, reflective practice, and professional identity formation, while remaining compatible with the clinical workloads of early-career practitioners and volunteer mentors.
In addition to individual mentoring sessions, the research team, in collaboration with COPTOA, will facilitate two to three group-based training sessions during the development phase of the program. These sessions will address cross-cutting and in-demand professional topics relevant to early-career occupational therapists and will be delivered in an online or hybrid format.
Mentors receive initial orientation and ongoing support from the research team, ensuring consistency and quality in program delivery. Digital tools and structured templates are provided to facilitate communication, goal tracking, and feedback.
During the initiation phase (first 2–3 weeks of the program), the pair establishes rapport, sets expectations, and co-defines the mentee’s professional development goals.
During the development phase (approximately months 2–5), sessions focus on fostering professional identity, reflective practice, and emotional support. Mentors provide guidance, share professional experiences, and help mentees navigate challenges in early career integration. Sessions are flexible yet goal-oriented, encouraging active participation and self-directed growth from mentees. In addition, COPTOA will organize training sessions on specific and in-demand topics to address emerging professional needs. Matching of pairs considers practice area (e.g. geriatrics, pediatrics, mental health), years of experience, and geographical proximity to maximize relevance and engagement.
The closure phase (final 1–2 weeks of the program) consolidates learning through reflection on progress and identification of next steps for continued professional growth.
Figure 1 illustrates the three phases of the MenTOras mentorship program—initiation, development, and closure—highlighting the key activities and objectives within each stage.
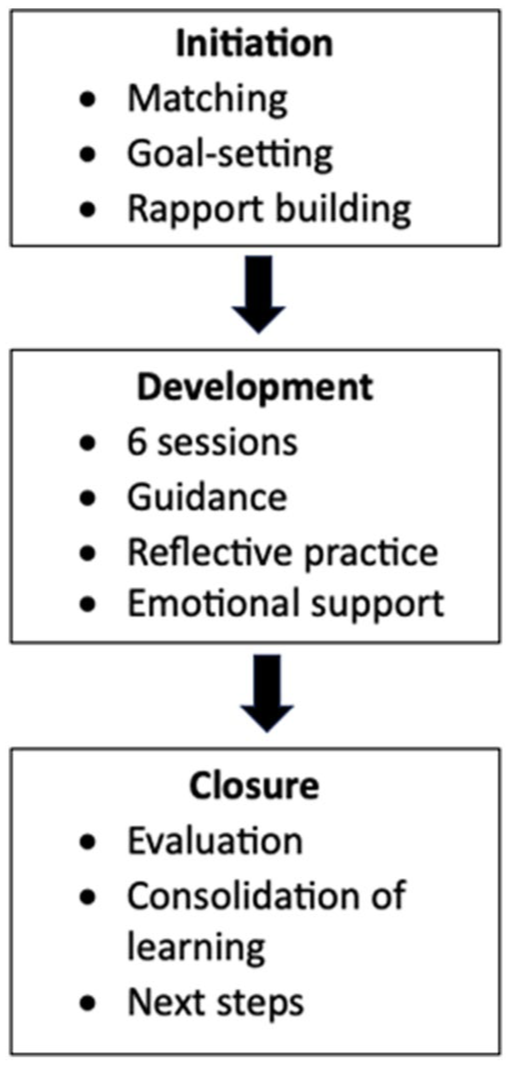
Structure and phases of the MenTOras Mentorship Program.
Data collection and measures
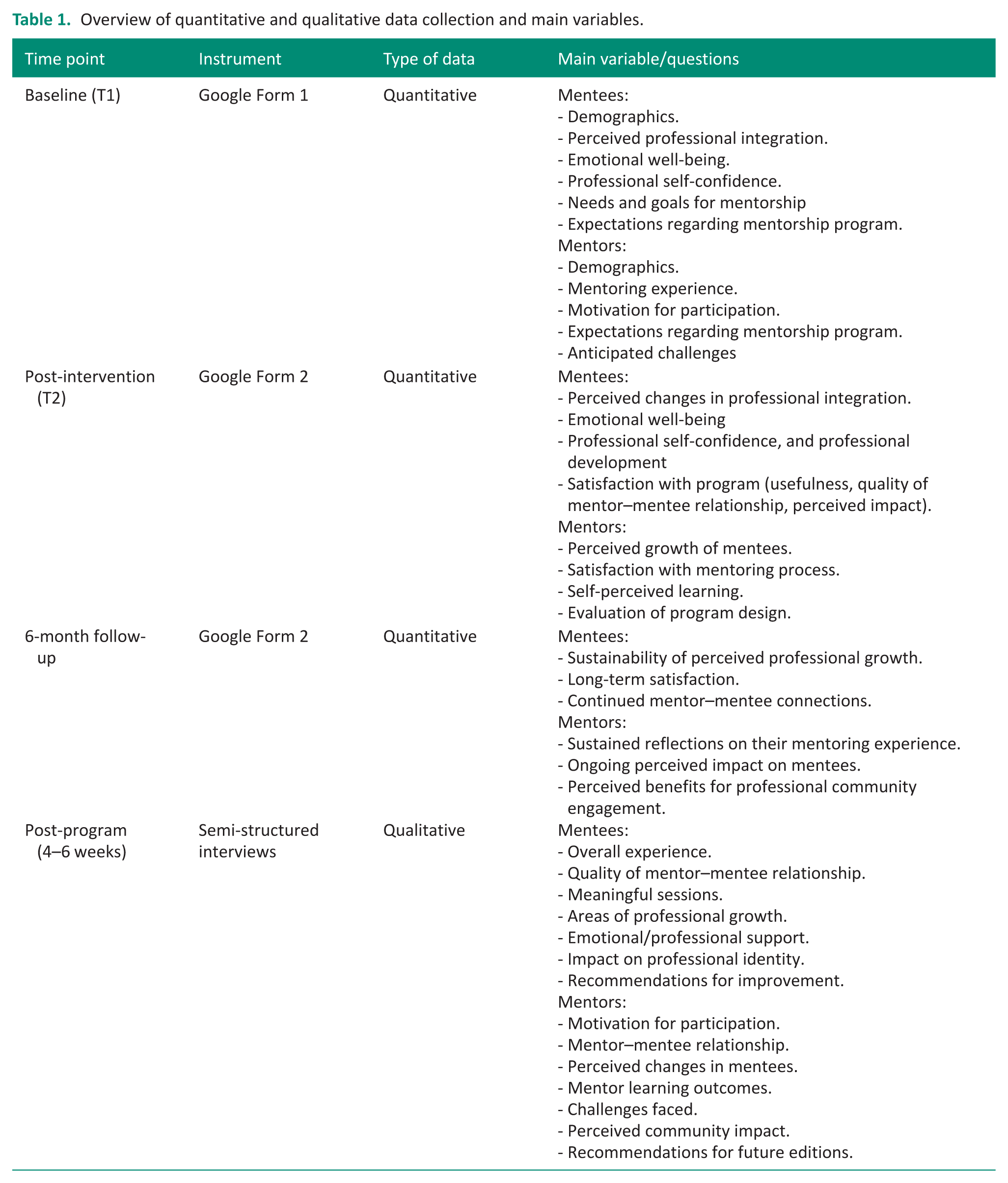
Data collection occurs at three time points for each mentee: prior to starting the program (baseline), immediately upon program completion, and at a 6-month follow-up. Standardized Google Forms are used for all data collection phases ( Supplementary Material, S3 ).
The baseline form includes demographic and professional information (e.g. age, gender, years of experience, and practice area), as well as purpose-built items assessing mentees’ initial perceptions of their emotional well-being, professional self-confidence, expectations regarding the mentorship program, and professional integration. In this study, professional integration is operationalized as participants’ self-reported perceptions of their inclusion and participation in professional contexts, including their sense of belonging within the profession, confidence in fulfilling professional roles, access to professional support, and perceived integration within organizational and multidisciplinary work environments. Mentors complete a similar baseline form focused on demographics, mentoring experience, motivation for participation, expectations, and anticipated challenges.
The post-intervention and 6-month follow-up forms consist of similar purpose-built items to allow for evaluation of perceived changes over time, in addition to questions assessing satisfaction with the program (e.g. perceived usefulness of sessions, quality of the mentor–mentee relationship, and perceived impact on professional growth). Mentors also report on perceived mentee growth, their satisfaction with the mentoring process, self-perceived learning, and evaluation of program design, as well as sustained reflections at follow-up.
All quantitative questions were developed by the research team, informed by the program’s theoretical framework and objectives, and use Likert-type or short-answer formats to capture nuanced participant feedback.
In addition to quantitative measures, qualitative data are obtained through semi-structured interviews conducted with a purposive subsample of mentors and mentees approximately 4–6 weeks after the mentorship program concludes ( Supplemental Material, S4 ). The interview guides explore participants’ overall experiences, mentor–mentee relationships, meaningful sessions, perceived professional growth, emotional and professional support, and the program’s impact on professional identity. Mentors are also asked about their motivations, perceived changes in mentees, personal learning outcomes, challenges faced, and views on the broader value of such programs for the OT community. Both mentees and mentors are invited to offer recommendations for improving future iterations of the program.
Table 1 summarizes the data collection time points, instruments used, data types, and main variables or questions addressed for both mentees and mentors throughout the study.
Overview of quantitative and qualitative data collection and main variables.
Data analysis
Quantitative data collected via Google Forms will be exported into SPSS software for analysis. Descriptive statistics, including means, standard deviations, and frequencies, will be calculated to characterize participant demographics and baseline variables. To evaluate changes over time in mentees’ perceived professional integration, emotional well-being, professional self-confidence, and satisfaction with the program, repeated measures analyses (such as paired t-tests or repeated measures ANOVA) will be conducted comparing baseline, post-intervention, and 6-month follow-up scores. For mentor data, similar analyses will assess perceived mentee growth, satisfaction with the mentoring process, and self-perceived learning.
Correlational analyses will be performed to examine relationships between demographic factors, baseline characteristics, and outcome variables such as program satisfaction and perceived professional growth. Missing data will be addressed using appropriate methods, such as multiple imputation or listwise deletion, depending on the extent and pattern of missingness.
Qualitative data from semi-structured interviews will be transcribed verbatim and imported into NVivo software for management and analysis. Thematic analysis following Braun and Clarke’s (2012) methodology will be used to identify, analyze, and report patterns (themes) within the data. Two researchers will independently code transcripts to ensure reliability, with discrepancies resolved through consensus discussions. Themes will be developed to capture participants’ overall experiences, mentor–mentee relationships, perceived professional growth, emotional and professional support, and recommendations for program improvement.
The integration of quantitative and qualitative findings will occur during the interpretation phase in accordance with established mixed-methods approaches. A side-by-side narrative integration strategy will be used, whereby quantitative results and qualitative themes addressing similar domains (e.g. professional integration, emotional well-being, professional confidence, and perceived program impact) will be compared and interpreted together. This approach will allow identification of areas of convergence, complementarity, or divergence between data sources. Where appropriate, integrated narrative summaries will be used to illustrate how qualitative findings help explain, expand, or contextualize quantitative results.
Ethics considerations
The study was reviewed and approved by the Research Ethics Committee (CEIN) of the University of Zaragoza on July 15, 2025 (Reference: RAT 2025-178). The committee concluded that the project complies with the ethical principles adopted by the University of Zaragoza for research involving human interaction and/or the collection of personal data for non-biomedical purposes. All participants will provide informed consent prior to enrollment.
Discussion
This protocol describes the design and rationale for the MenTOras program, a peer mentoring intervention aimed at supporting the early professional development of newly qualified occupational therapists in Spain. Based on internationally available evidence, the program seeks to address well-documented gaps in professional integration, emotional support and consolidation of professional identity during the transition from university to clinical practice (Hayward et al., 2013; Moir et al., 2021; Turpin et al., 2021).
Although mentoring is widely recognized as a key component of professional development in various health professions (Burgess et al., 2018; McCray et al., 2014), its implementation in OT is still limited, especially in the Spanish context (Doyle et al., 2019; Milner and Bossers, 2005). The absence of structured mentoring programs leaves novice practitioners exposed to situations of professional isolation, low visibility of their role and limited opportunities for guided learning (Solomon et al., 2001; Toal-Sullivan, 2006). By designing a structured peer mentoring framework, MenTOras offers a potentially replicable model that aligns with the discipline’s core values of collaboration, critical reflection, and person-centered growth (Dickson et al., 2021; Venktaramana et al., 2023).
The proposed mixed methodological approach allows for a comprehensive evaluation of program impact by combining quantitative outcome analysis with qualitative exploration of participants’ lived experiences (Palinkas et al., 2011). This strategy is particularly suitable for pilot studies and exploratory evaluations, where understanding the mechanisms of change is as relevant as identifying outcomes (Craig et al., 2008). In addition, the inclusion of mentors and mentees in the evaluation process allows the reciprocal nature of mentoring to be captured, generating a more complete picture of its two-way benefits (Gilles and Wilson, 2004; Venktaramana et al., 2023).
The implementation of the program in a real context, with voluntary participation and face-to-face or virtual sessions depending on geographical availability, reinforces its ecological validity. This approach is consistent with methodological recommendations for the evaluation of complex interventions, which emphasize the importance of considering the context, the adaptability of the intervention and the real conditions of implementation to ensure the applicability and sustainability of the results (Moore et al., 2015). Nevertheless, as a pilot study, they can inform us about the best research process and occasionally about likely outcomes (Van Teijlingen et al., 2001), but certain limitations must also be acknowledged. The absence of a control group restricts the ability to attribute changes exclusively to the intervention. Also, the sample size, although adequate for an exploratory design, limits the generalisability of the findings (Leon et al., 2011; Van Teijlingen et al., 2001). Furthermore, the use of ad hoc instruments created without prior validation may introduce measurement bias, although this risk is mitigated by triangulation with qualitative data (Craig et al., 2008).
Despite these limitations, MenTOras brings valuable evidence to the field of health professions mentoring and provides a solid foundation for future research. If promising results are obtained, future editions of the program could benefit from the use of randomized controlled designs, validated measures and larger samples, including other professional bodies in the country (Craig et al., 2008). Also, longer-term follow-up could explore the sustainability of the impact of mentoring on professional identity, job retention, and career trajectory (Craig et al., 2008).
Ultimately, MenTOras responds to a critical need in the OT field: the development of structured and contextualized strategies to support new entrants. By fostering peer mentoring, reflective practice and emotional well-being, peer mentoring not only facilitates the transition to professional practice but can also act as a catalyst to strengthen the collective identity and visibility of the profession (Doyle et al., 2019; Germeroth et al., 2024; Milner and Bossers, 2005).
Conclusion
This protocol describes the design of a pilot study to evaluate the feasibility and perceived impact of MenTOras, a peer mentoring program aimed at newly graduated occupational therapists. In response to the scarcity of formal professional mentoring initiatives in the Spanish context, MenTOras proposes a structured model that integrates emotional support, reflective practice and professional identity strengthening.
Using a mixed approach to data collection and analysis, the study will explore both the subjective effects of the intervention and the underlying mechanisms that may explain its usefulness. The inclusion of mentors and mentees provides a two-way perspective on the mentoring experience, broadening the interpretative scope of the results.
Findings from this pilot will be essential to identify strengths and areas for improvement of the program, as well as to inform the development of future controlled trials, with larger samples and more robust designs. They could also contribute to the design of professional policies aimed at improving transition to practice and retention of occupational therapists in the health and social care system.
The MenTOras experience can serve as a reference for other health professions seeking to strengthen peer mentoring as a sustainable professional development strategy, contextualized and focused on the real needs of new professionals.
Key findings
MenTOras Protocol: peer mentoring for newly qualified occupational therapists, with six sessions in three phases and implementation coordinated by the professional association.
Mixed, quasi-experimental pilot without a control group: ~20 mentor–mentee pairs; baseline, post and 6-month measurements of professional integration, well-being, self-confidence and satisfaction, plus qualitative interviews.
Assesses feasibility and acceptability and identifies mechanisms for change to refine and scale up future editions and controlled trials in the Spanish context.
What the study has added
Introduces a context-sensitive peer-mentoring program for newly qualified occupational therapists in Spain, and pilots feasibility, acceptability and preliminary effects on integration, well-being, and confidence.
Supplemental Material
sj-pdf-1-bjo-10.1177_03080226261461172 – Supplemental material for MenTOras: Study protocol for a peer mentorship program to support the professional integration of recently graduated occupational therapists
Supplemental material, sj-pdf-1-bjo-10.1177_03080226261461172 for MenTOras: Study protocol for a peer mentorship program to support the professional integration of recently graduated occupational therapists by Sandra León-Herrera, Enrique Villa-Berges, Rafael Sánchez-Arizcuren, María Cristina Ruiz-Garrós and Marta Marín-Berges in British Journal of Occupational Therapy
Footnotes
Acknowledgements
The authors would like to thank the Colegio Profesional de Terapeutas Ocupacionales de Aragón (COPTOA) for their collaboration in the recruitment and dissemination of the program.
ORCID iDs
Ethical considerations
The study was reviewed and approved by the Research Ethics Committee (CEIN) of the University of Zaragoza on July 15, 2025 (Reference: RAT 2025-178). The committee concluded that the project complies with the ethical principles adopted by the University of Zaragoza for research involving human interaction and/or the collection of personal data for non-biomedical purposes.
Consent to participate
All participants will provide informed consent prior to enrollment.
Author contributions
Sandra León-Herrera and Marta Marín-Berges conceived the study. Sandra León-Herrera coordinated the development of the protocol. All three—Sandra León-Herrera and Marta Marín-Berges—contributed to the methodological design and participated in refining the research questions, eligibility criteria, and data extraction framework. All authors contributed intellectually to the development of the protocol, provided critical input, and reviewed, edited, and approved the final version.
Funding
The authors declared no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
No datasets were generated or analyzed during the current study protocol. Data collection is ongoing. Upon study completion, de-identified data will be made available from the corresponding author on reasonable request.
Patient and public involvement data
During the development, progress, and reporting of the submitted research, Patient and Public Involvement in the research was included at all stages of the research.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.