
Abstract
Introduction:
Individuals with severe mental illness (SMI) often experience limited community participation and reduced quality of life. Occupation-based group interventions informed by culturally responsive models such as the Kawa Model may support well-being and engagement. This study aimed to examine the effects of a Kawa Model–guided occupation-based group intervention on quality of life and community participation in individuals with SMI.
Method:
A single-group pretest–posttest design was used. Eight adults with SMI participated in a 10-week group intervention guided by the Kawa Model. Quantitative outcomes were assessed using the World Health Organization Quality of Life–BREF (WHOQOL-BREF) and the Community Integration Questionnaire. Qualitative data were collected through Kawa-based interviews and real-time reflections.
Results:
Post-intervention improvements were observed in community integration and social relationships. Participants reported enhanced self-expression, motivation, and a greater sense of belonging. River drawings illustrated changes in occupational identity and perceived life flow.
Conclusion:
A Kawa-guided group intervention may enhance participation and well-being among individuals with SMI. Findings support the utility of culturally grounded, metaphor-driven approaches in occupational therapy mental health practice.
Keywords
Introduction
Severe mental illness (SMI) is a multidimensional condition that profoundly affects not only the individual’s inner world but also their social, occupational, and daily life domains (Xie et al., 2022). These challenges often result in disruptions in interpersonal relationships, decreased functioning, and difficulties in fulfilling societal roles (Defar et al., 2023). Cognitive impairments, including problems with decision-making, problem-solving, and emotional regulation, can further limit individual functioning and community participation (Defar et al., 2023; Nagata et al., 2020). Consequently, such limitations can diminish life satisfaction and negatively impact overall well-being (Choo et al., 2019). Although many individuals with SMI find meaning in life and seek greater engagement, barriers such as stigma, economic hardship, and internalized negative attitudes often hinder participation (Barlott et al., 2020; Nagata et al., 2020). Thus, reclaiming social roles and community connections becomes essential for improving quality of life. This highlights the need for interventions grounded in lived experiences and responsive to cultural and environmental contexts (Solaru et al., 2023; Townley et al., 2018).
Occupational therapy plays a crucial role in supporting individuals with SMI by enhancing occupational performance, promoting autonomy, and improving life satisfaction (Valverde-Bolivar et al., 2022). According to the World Federation of Occupational Therapists (Hocking et al., 2022), occupational therapy contributes to quality of life and participation through skill development, group interventions, and community engagement (Hocking et al., 2022). To address the complexity of challenges faced by individuals with SMI, various theoretical models have been developed to help occupational therapists holistically evaluate barriers and facilitators to participation.
Among these models, the Kawa Model—rooted in Japanese cultural metaphors—offers a culturally responsive framework that conceptualizes life as a flowing river. In this metaphor, water represents life flow, rocks symbolize life challenges, riverbanks reflect the social and physical environment, and driftwood denotes personal strengths and liabilities (Iwama, 2006). This metaphorical structure allows individuals to externalize their experiences through visual representations, offering insight into the interactions between internal resources and external contexts. By engaging with their personalized river drawings, individuals can clarify goals, enhance self-awareness, and better understand the dynamic factors shaping their occupational engagement and well-being (Iwama et al., 2009; Ober et al., 2022).
When applied in group settings, the Kawa Model facilitates shared reflection, encourages interpersonal dialogue, and fosters a sense of connection by highlighting both common and unique aspects of participants’ life flows. It serves not only as a conceptual framework but also as a flexible tool for assessment, therapeutic conversation, and intervention planning (Ober et al., 2022). The collaborative nature of the model in group contexts supports mutual understanding and collective meaning-making, promoting both individual insight and social cohesion (Hsiao et al., 2024; Ober et al., 2022).
Guided by these principles, this study examined the effects of a Kawa Model-guided group intervention on quality of life and community participation, while also exploring participants’ perceived changes in social connection and self-understanding.
Materials and methods
Research design
This study employed a single-group pretest–posttest design to examine the effects of an occupational therapy intervention based on the Kawa Model in enhancing quality of life and community participation among individuals with mental health disorders.
Participants
Participants were community-dwelling adults with severe mental illness (SMI) who were recruited through convenience sampling from the outpatient clinic of the Department of Occupational Therapy at Hacettepe University. Eligibility criteria were a diagnosis of chronic mental health disorder based on DSM-5 criteria, age between 18 and 65 years, fluency in Turkish, and sufficient cognitive and communicative abilities to participate in semi-structured interviews. Individuals were excluded if they had cognitive impairments that could hinder participation, experienced acute psychiatric episodes requiring hospitalization within the past 6 months, or were actively engaged in substance abuse.
A total of eight participants met the inclusion criteria and agreed to participate in the study. The sample size was limited due to the specialized nature of the intervention and the clinical availability of eligible individuals during the study period.
Outcome measures
At baseline, demographic and clinical information were documented, including age, gender, primary psychiatric diagnosis, duration of illness, educational background, psychiatric hospitalizations, marital, and employment status. Primary outcomes were assessed through standardized instruments, including the World Health Organization Quality of Life—Short Form (WHOQOL-BREF), the Community Integration Questionnaire (CIQ), and the Kawa Model-based qualitative evaluation.
KAWA Model-based assessment
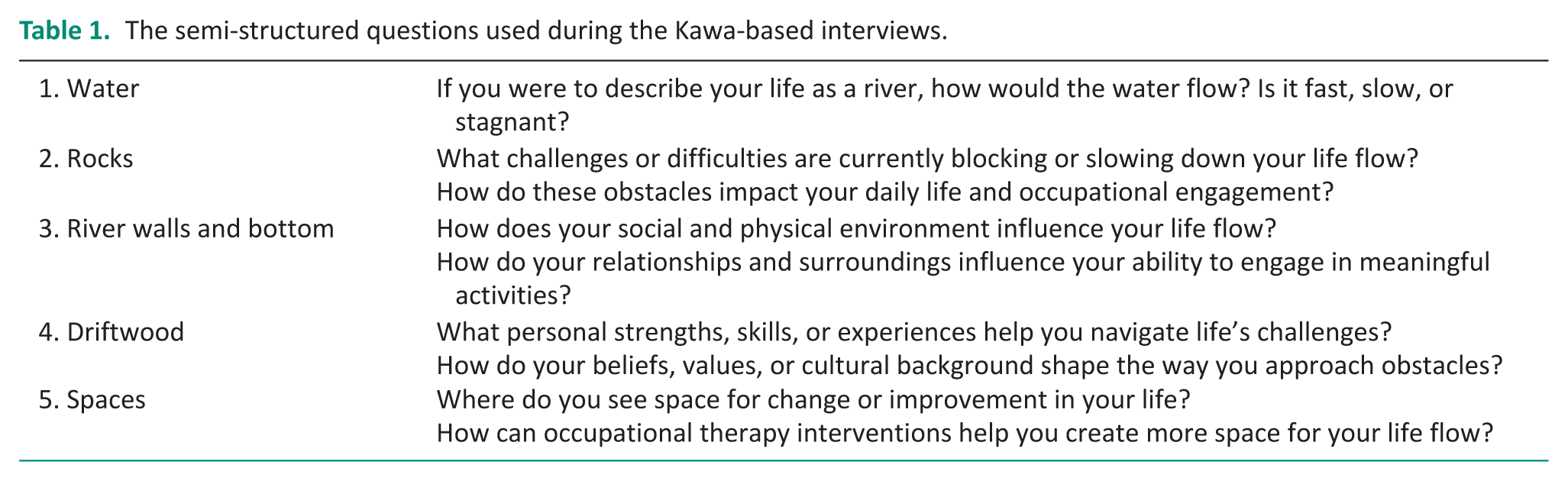
The Kawa Model conceptualizes life as a river, using metaphorical elements to represent the dynamic interaction among personal resources, environmental contexts, and life challenges (Gregg et al., 2015; Iwama, 2006; Iwama et al., 2009). At the start of the intervention, participants created individualized “life river” drawings with the therapist to visually represent factors affecting their occupational flow. These served as the foundation for therapeutic goal-setting and were revisited throughout the 10-week program to monitor changes in perceived barriers, supports, and life direction. The process emphasized participants’ subjective experiences and cultural contexts. Semi-structured interview prompts are presented in Table 1.
The semi-structured questions used during the Kawa-based interviews.
Quality of life
Developed by the World Health Organization (1998), the WHOQOL-BREF is a 26-item self-reported measure assessing 5 domains: general health status, physical health, psychological well-being, social relationships, and environmental factors. Each item is rated on a 5-point Likert scale, with higher scores indicating better quality of life. The Turkish version’s validity and reliability were established by Eser et al. (1999). Reported Cronbach’s alpha coefficients for the Turkish version were 0.83 for Physical Health, 0.66 for Psychological Health, 0.70 for Social Relationships, 0.73 for Environment, and 0.92 for the total scale, demonstrating acceptable to excellent internal consistency across domains (Eser et al., 1999).
Community participation
The CIQ was initially developed by Willer et al. (1993) to assess participation in home and family life, social activities, and productive activities. It consists of 15 items covering 3 primary domains: Home Integration (items 1–5; 0–10 points), Social Integration (items 6–11; 0–12 points), and Productivity (items 12–15; 0–7 points). Many items offer three response options, and the total score ranges from 0 to 29, with higher scores indicating greater community integration. The Turkish adaptation, validity, and reliability study of the CIQ was conducted by Akyurek et al. (2016). The internal consistency coefficients (Cronbach’s alpha) reported for the Turkish version were 0.70 for Home Integration, 0.71 for Social Integration, 0.78 for Productivity, and 0.82 for the total scale, demonstrating good reliability for both the subscales and the overall instrument.
Real-time reflections
At the end of each session, participants completed real-time reflections to capture immediate reactions to the session (Zarbo et al., 2022). Participants were asked questions such as, “What are your thoughts on today’s session?” and “Can you summarize your feelings, thoughts, and key takeaways from this session in one sentence?” These reflections provided qualitative data representing evolving engagement and shifting perspectives over the 10-week program.
Intervention: K-FLOW (Kawa-focused life and occupation for well-being)
The Kawa Model was employed both as an assessment tool and as a guiding framework for intervention. Based on the insights gained from the Kawa Model assessment, participants and the occupational therapists collaboratively developed personalized therapeutic goals. Over the 10-week period, participants attended weekly Kawa-focused life and occupation for well-being (K-FLOW) group intervention sessions lasting approximately 90 minutes. Each session incorporated occupation-based activities, guided reflections, and interactive discussions.
Sessions followed a consistent structure that included:
A warm-up activity to foster group cohesion and active participation,
A core occupation-based task aimed at skill development and community participation,
A guided discussion to encourage self-reflection and peer learning,
A real-time reflection exercise to capture participants’ immediate experiences and insights.
Rather than adhering to a fully predetermined structure, the program was dynamically refined based on participants’ needs, allowing person-centered and culturally responsive adjustments. Following initial Kawa interviews, themes such as interpersonal difficulties, emotional regulation challenges, and environmental barriers were incorporated into the content.
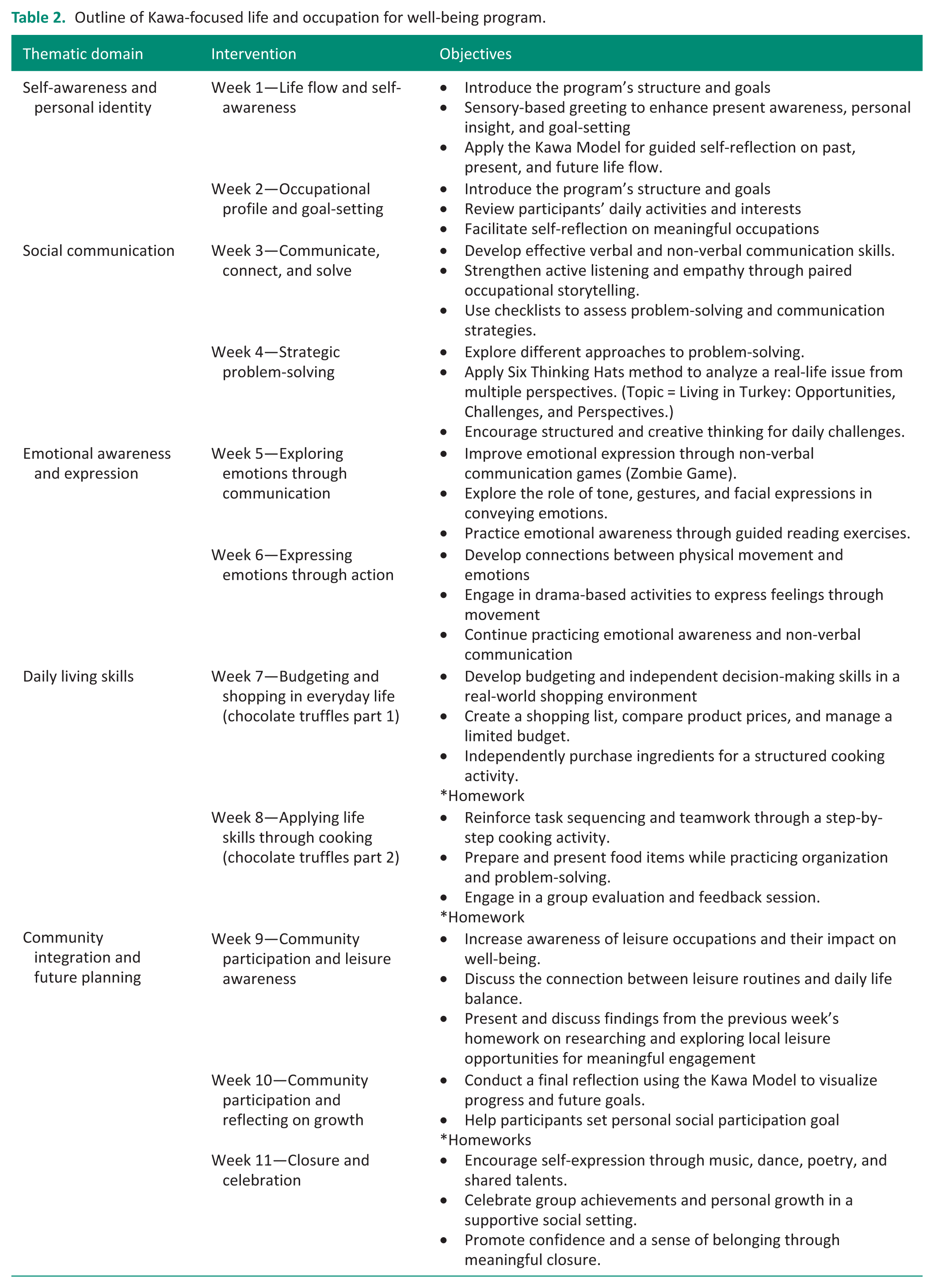
The intervention followed five thematic stages: self-awareness, social communication, emotional expression, daily living skills, and community integration. Early sessions explored life flow and values through the Kawa Model; later sessions focused on interpersonal skills and independence via tasks like budgeting and cooking. The program ended with participants reflecting on progress and setting future participation goals (see Figure 1 and Table 2).
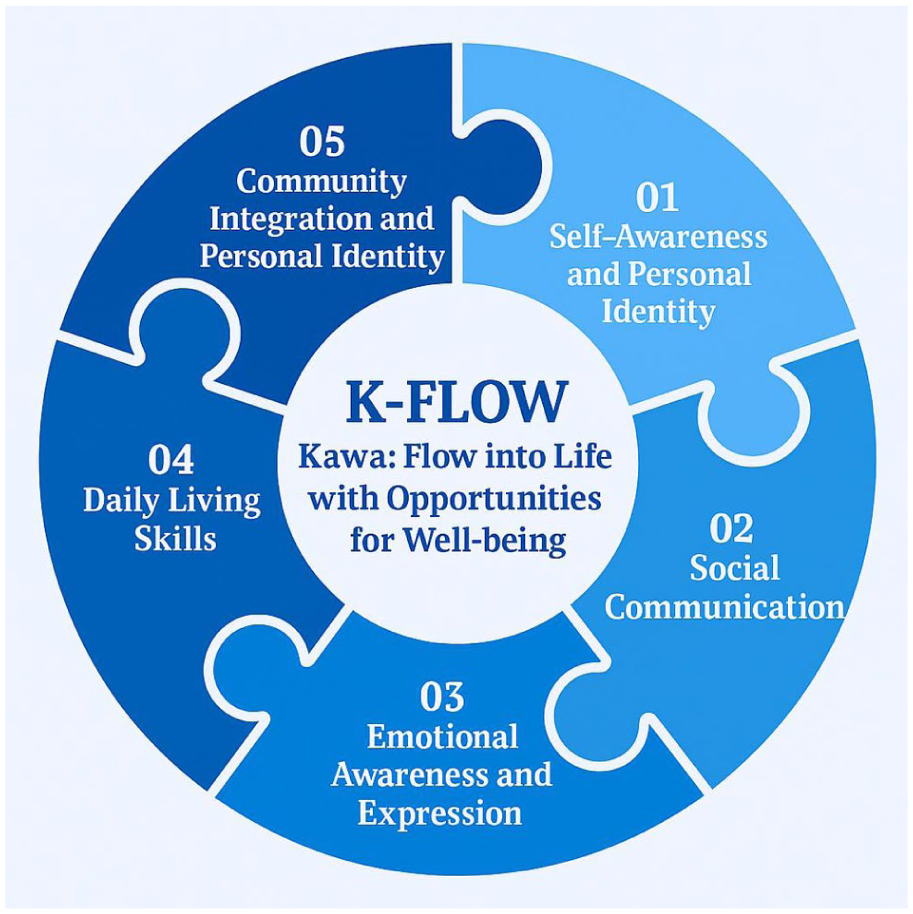
K-FLOW.
Outline of Kawa-focused life and occupation for well-being program.
Throughout the intervention, the Kawa Model was revisited to facilitate reflection on progress, shifting obstacles, and emerging opportunities. Pre- and post-intervention river drawings offered qualitative evidence of participants’ evolving experiences and guided the therapeutic process toward promoting improved life flow and community integration.
Data collection and analysis
All data were collected through face-to-face interviews. Qualitative data were collected individually during 60-minute sessions before the K-FLOW intervention. Real-time reflections were recorded after each group session to capture immediate impressions and emotions.
Qualitative data analysis
Qualitative data consisted of researcher memos written during and immediately after each session, together with participants’ written real-time reflections collected throughout the program. Data were analyzed using a theoretical thematic analysis guided by the Kawa Model framework. As the interview questions were structured around the core elements of the Kawa Model, coding and theme development were conducted within this conceptual structure. Two researchers independently reviewed the dataset to achieve familiarization and generated initial codes aligned with the Kawa elements. Through iterative discussion and comparison, themes were refined and organized under the five Kawa components (water, rocks, riverbanks, driftwood, and spaces). This approach ensured analytic coherence with the intervention framework while remaining grounded in participants’ reflections and session-based observations.
Quantitative data analysis
Descriptive statistics were used to summarize demographic and clinical characteristics. Categorical variables are presented as frequencies and percentages, while continuous variables are reported as medians and ranges. Since the normality assumption was not met, the Wilcoxon signed-rank test was conducted to assess changes in the quality of life and community participation from pre- to post-intervention. Statistical significance was determined at a p-value of less than 0.05. All data analyses were performed using IBM SPSS Statistics for Windows, Version 23 (IBM Corp., Armonk, NY, USA).
Statistical considerations
Given the exploratory nature and pretest–posttest design, no formal sample size calculation was conducted. Small-sample designs are widely accepted in early-stage intervention research to identify preliminary effects and inform future trials (Hertzog, 2008; Marsden and Torgerson, 2012). The inclusion of eight participants was considered appropriate for this study’s pretest–posttest design.
Research team and trustworthiness
The research team consisted of three researchers. FŞ holds a master’s degree, has completed training in creative drama instruction, and is currently pursuing a PhD focused on positive occupation and motivation in schizophrenia. ZYT is completing a master’s degree in mental health, specializing in occupational performance among individuals diagnosed with obsessive-compulsive disorder. HA holds a doctorate in occupational therapy with expertise in life skills training and functionality in schizophrenia and provided methodological supervision and critical oversight throughout the research and analytic process.
Two researchers (FŞ and ZYT) conducted the qualitative analysis. Coding decisions and theme development were discussed iteratively between these researchers and subsequently reviewed with HA to enhance analytic depth and consistency. Discrepancies were resolved through reflective discussion. An audit trail, including coding notes and analytic memos, was maintained throughout the analytic process.
Triangulation was achieved by integrating quantitative findings (WHOQOL-BREF, CIQ) with Kawa-based reflections and session-based real-time reflections, thereby strengthening the credibility of interpretations (Creswell and Creswell, 2017). Rich descriptions were used to provide a comprehensive account of participants’ experiences.
Ongoing memo-writing functioned as a reflexive tool, allowing the researchers to critically examine their interpretations and clinical assumptions throughout the analytic process.
Ethical considerations
Ethical approval was obtained from the Çankırı Karatekin University Health Sciences Ethics Committee (Approval Code: E6B9CE2A02D84BAF). All participants provided written informed consent. Procedures followed institutional and national ethical standards and the revised Helsinki Declaration; confidentiality and data security were maintained throughout.
Results
Participant flow and demographics
Of the 17 individuals initially interested in the K-FLOW program, 8 met inclusion criteria and completed all assessments and sessions. Six declined due to scheduling issues, and three were ineligible. All eight attended the full 10-week program, which consisted of weekly 90-minute group sessions and related individual sessions. No adverse events were reported.
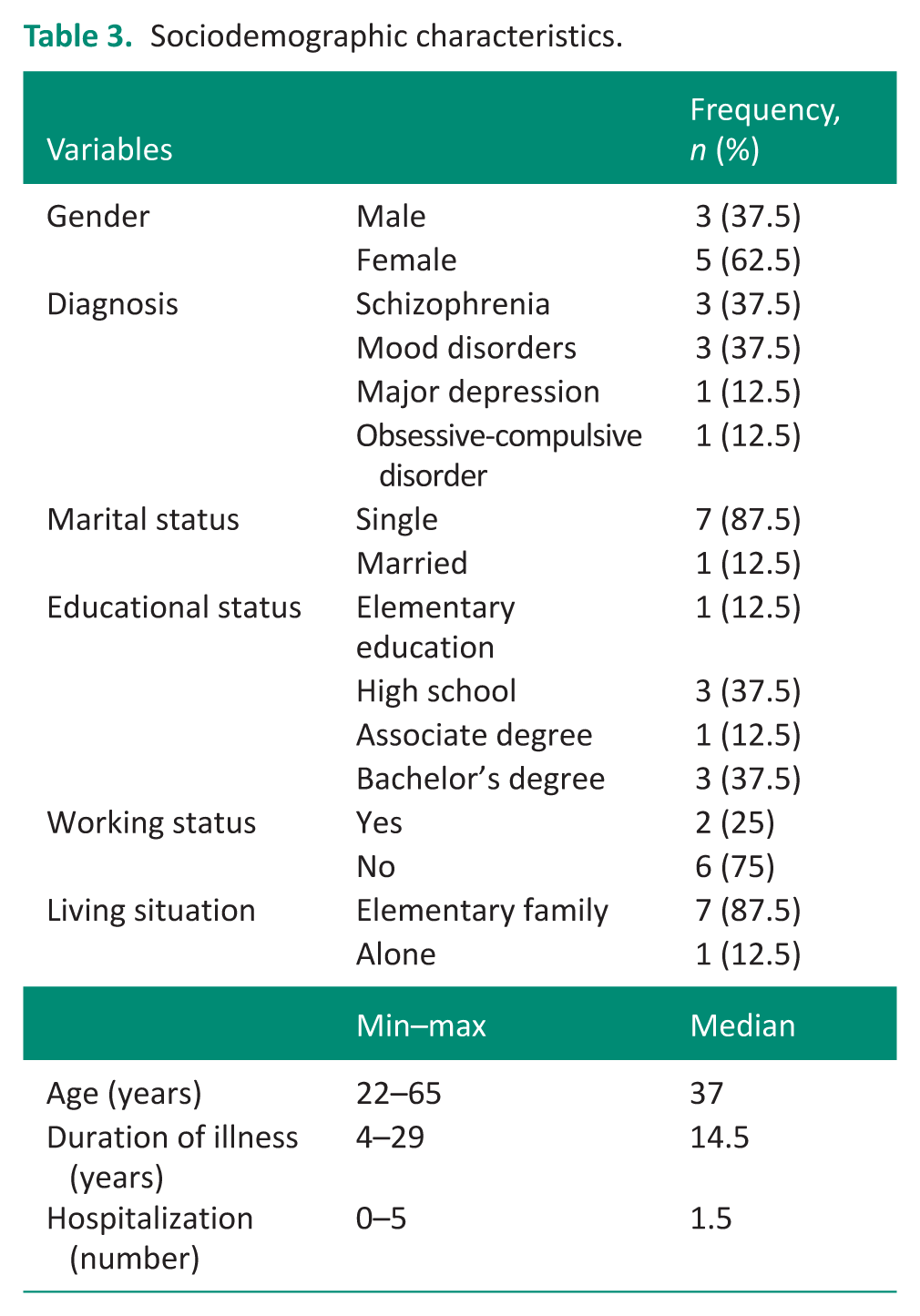
Participants’ ages ranged from 22 to 65 years, and the duration of illness ranged from 4 to 29 years. The sample was predominantly female (62.5%) and single (87.5%). Diagnostic categories included schizophrenia (37.5%), mood disorders (37.5%), major depressive disorder (12.5%), and obsessive-compulsive disorder (12.5%). Additional sociodemographic characteristics are summarized in Table 3.
Sociodemographic characteristics.
Occupational change reflections through the Kawa Model
Qualitative analyses of river drawings and real-time reflections revealed meaningful changes in participants’ occupational engagement and self-perception. Themes were organized using the five Kawa Model elements: Water (life flow), rocks, riverbanks, driftwood, and spaces.
Water (life flow)
In the Kawa Model, the metaphor of water represents the dynamic flow of a person’s life force, encompassing emotional, cognitive, and physical functioning. In the present study, participants initially depicted their life flow as weak, fragmented, or stagnant—visualizing narrow or shallow streams in their river drawings. These representations reflected the cumulative effects of psychiatric stressors, limited occupational engagement, and both self-directed and societal stigma.
As the intervention progressed, participants reported renewed vitality, motivation, and psychological energy. Final drawings became more fluid and expansive, symbolizing increased hope, direction, and engagement in daily life.
“My drawing had barely any flow. It’s how I feel: stuck in one place with no idea where to go.”
“I was psychologically asleep, but now I feel like I am running instead of walking.”
Rocks (obstacles)
In the Kawa Model, rocks symbolize the persistent challenges and life stressors that restrict occupational engagement and disrupt the flow of daily life. In this study, participants initially represented smaller rocks near the water’s surface to reflect issues like weight gain, environmental barriers, and limited healthcare access, while larger, deeper rocks symbolized chronic challenges such as economic hardship, fear of death, illness, and difficulties forming or maintaining social relationships. These elements were consistently identified as central disruptions to life flow.
Post-intervention drawings showed that while major rocks remained, their proximity to the surface had shifted. Some smaller rocks had shifted or fractured, symbolizing improved coping. Reflections indicated enhanced emotional expression, communication, and social confidence. P7: “Sports had a positive impact and helped me express my emotions better.” P8: “The work we did on emotional expression made me happy.”
“I learned to convey my emotions through gestures and facial expressions.”
At first, I didn’t talk about my stress. Now I feel like I have a few ways to express what’s going on inside.”
“I said hello to a neighbor today. I wouldn’t normally do that—it felt different, but good.”
Riverbanks (environment)
In the Kawa Model, the riverbanks represent the social and physical environment that shapes the individual’s occupational flow. In the pre-intervention drawings, participants often illustrated narrow riverbanks, reflecting limited social interaction and isolation. They described spending most of their time alone or struggling to engage meaningfully with others, which visually translated into constrained environmental boundaries. Physical elements such as individual bedrooms, home interiors, and street paths were frequently mentioned as dominant spatial references. While physical settings remained mostly unchanged post-intervention, participants’ revised drawings showed slightly wider riverbanks in some cases, suggesting a perceived expansion of their social world. P3: “(For the market shopping activity) It was good practice for adapting to social life; I feel positive.”
“Being in this group made me feel like I was part of something again.”
“Going outside still feels exhausting. I tried walking to the market, but I get anxious about bumping into things—especially uneven sidewalks and bright streetlights.”
Driftwood (personal strengths and resources)
Within the Kawa Model, driftwood symbolizes the personal traits, values, and resources that influence an individual’s life flow—either as supports or as obstacles. Initially, participants struggled to identify strengths without prompting but eventually named honesty, helpfulness, punctuality, knitting, digital design, vocational courses, religious faith, and language skills (e.g., German, English). Negative driftwood included limited education, loneliness, forgetfulness, low motivation, pessimism, high stress, stigma, and lack of support.
Post-intervention drawings showed a notable increase in the number of positive driftwood elements. Participants demonstrated improved awareness of their existing resources and personality strengths, rather than newly acquired traits. This heightened self-recognition was accompanied by greater articulation of occupational roles and engagement.
“(For the problem-solving activity) We had great communication today, fostering empathy and trust.” P2: “Expressing emotions through facial expressions and tone of voice was very effective.”
“During the session, I realized that I’m more resilient than I thought. I’ve always seen my stress as weakness, but now I see it as something I’ve learned to manage.”
“They said I’m funny, and that made me feel seen. I’ve always used humor, but now I know it matters.”
Spaces (opportunities for flow)
In the Kawa Model, spaces refer to the open areas between obstacles (rocks), environmental constraints (riverbanks), and the river’s bottom, symbolizing the potential for occupational engagement and growth. In the pre-intervention drawings, participants illustrated these spaces as narrow, fragmented, or absent, indicating limited perceived opportunities for engagement in meaningful occupations.
Following the K-FLOW intervention, participants’ river drawings depicted wider and more fluid spaces. This visual change reflected an increased capacity for occupational engagement, such as initiating leisure activities, participating in daily routines, or setting personal goals. P1: “I reflected on my current situation and noticed my positive progress.” P6: “Compared to before, I can see that I am in a much better place now. We talked about meaningful time use—I realized I want to spend more time outside and maybe volunteer.” P5: “As always, I am leaving here feeling happy and more open to the outside world.”
“(For the cooking activity) We added a little sweetness to life—both literally and figuratively.”
“(For the Kawa Model application) It was an interesting method—it showed me that I need to externalize my emotions. My self-awareness has increased.”
Quality of life
Descriptive analysis showed slight decreases in physical health scores but increases in psychological health, social relationships, environment, and general health. Only the improvement in social relationships was statistically significant (Z = −2.371, p = 0.018, r = 0.838), indicating a large effect size. Other domains—physical (p = 0.705), psychological (p = 0.121), environment (p = 0.105), and general health (p = 0.106)—did not reach significance, though moderate effect sizes were observed (see Table 4).
Pre- and post-intervention comparison of community integration and quality of life scores.
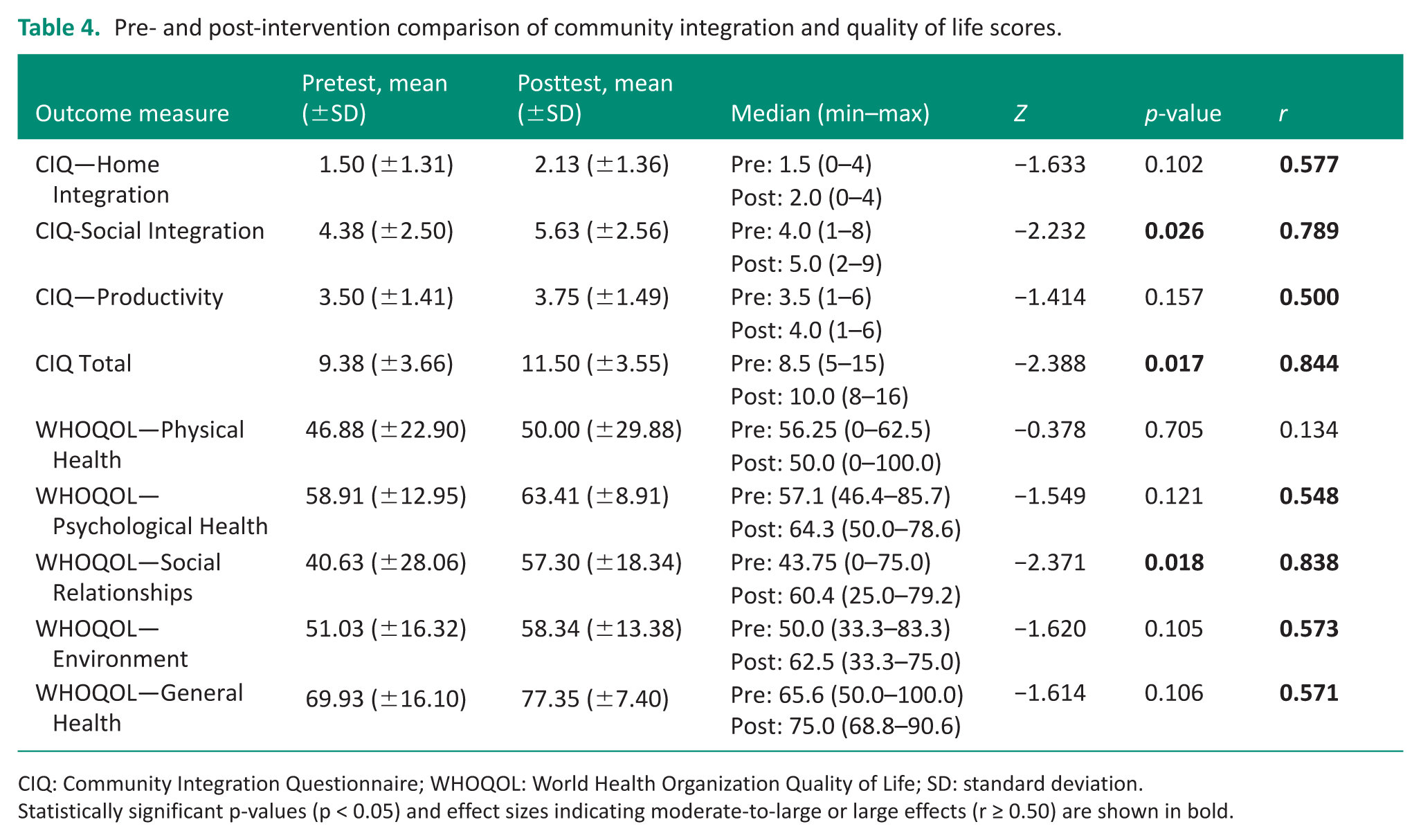
CIQ: Community Integration Questionnaire; WHOQOL: World Health Organization Quality of Life; SD: standard deviation.
Statistically significant p-values (p < 0.05) and effect sizes indicating moderate-to-large or large effects (r ≥ 0.50) are shown in bold.
Community integration
Median scores increased across all CIQ domains post-intervention: home integration (1.5–2.0), social integration (4.0–5.0), productivity (3.5–4.0), and total score (8.5–10.0). Significant improvements were found in social integration (Z = −2.232, p = 0.026, r = 0.789) and total CIQ score (Z = −2.388, p = 0.017, r = 0.844), both with large effect sizes. Gains in home integration (p = 0.102) and productivity (p = 0.157) were not statistically significant, though moderate effect sizes were observed (see Table 4).
Discussion
The primary aim of this study was to examine the effects of a group-based occupational therapy intervention guided by the Kawa Model on quality of life and community participation in individuals with severe mental illness. By exploring both quantitative outcomes and participants’ lived experiences, the study sought to evaluate whether a culturally grounded, metaphor-driven group format could foster meaningful engagement and psychosocial recovery.
This study makes a significant contribution to occupational therapy as one of the first to implement a group-based intervention grounded in the Kawa Model for individuals with severe mental illness. By integrating metaphor, narrative, and structured occupational engagement, the intervention created a culturally responsive and reflective space in which participants could explore both personal and interpersonal challenges. This aligns with Iwama’s conceptualization of well-being as a dynamic life flow shaped by individual, social, and environmental contexts (Iwama, 2006; Teoh and Iwama, 2015).
Our findings indicate that the Kawa Model functions not only as a narrative assessment tool but also as a therapeutic medium that facilitates emotional processing, insight, and peer connection. In line with previous research (Naidoo et al., 2023; Newbury and Lape, 2021; Paxson et al., 2012), participants used river drawings to externalize complex experiences in a non-pathologizing format. The shared use of metaphor enabled individuals to articulate inner challenges (rocks), personal strengths (driftwood), and life trajectories (water; Brown et al., 2023; Naidoo et al., 2023).
While the Kawa Model has traditionally been employed in individual therapy, this study adds to a growing body of evidence supporting its application in group-based interventions. Studies by Brown et al. (2023), Naidoo et al. (2023), and Paxson et al. (2012) highlight how sharing metaphorical narratives in group contexts promotes empathy, interpersonal cohesion, and culturally responsive dialogue. These processes allowed participants to share personal occupational narratives while engaging with others’ experiences, fostering empathy and emotional validation. The Kawa Model thus served as a relational tool for healing in mental health contexts.
Weis et al. (2019) found that the Kawa Model supported emotional expression in bereaved parents. In our group, visualizing challenges as river blockages fostered insight, emotional processing, and mutual validation. Listening to others’ river stories helped participants reframe personal struggles, while co-creating and sharing visual metaphors strengthened group cohesion, psychological connectedness, and a sense of belonging—outcomes consistent with previous research (Gregg et al., 2015; Lim, 2018). However, consistent with prior literature, some participants initially struggled with the abstract nature of the river metaphor, requiring additional scaffolding and concrete examples from the therapeutic team to support comprehension (Aygün and Akel, 2018; Owen, 2014).
Our findings further illuminate how the group format deepened participants’ engagement with core components of the Kawa Model. Post-intervention river drawings revealed a distinct expansion in open spaces, symbolizing a meaningful shift in participants’ perceived occupational opportunities and sense of agency. Within the Kawa framework, such spatial openness reflects an individual’s growing ability to manage life flow despite obstacles and highlights key areas for therapeutic focus (Iwama, 2006). In our study, this transformation was supported by the structured rhythm of the K-FLOW sessions, which progressively addressed themes such as community participation, life skills, and future planning. These sessions appeared to foster awareness, purpose, and readiness to engage in meaningful occupations beyond the therapeutic setting.
Changes were also evident in riverbanks, which appeared more stable and supportive after the intervention, especially among participants living with family. While physical environments remained largely constant, drawings suggested a subjective shift in environmental perception, marked by new social routines and community engagement. This pattern reflects the role of relational scaffolding in supporting occupational flow, particularly in collectivist cultural contexts (Iwama et al., 2009).
Participants’ depictions of rocks shifted as well, with many obstacles repositioned or reduced in size, suggesting enhanced coping strategies and decreased psychological burden. These visual changes appeared to reflect greater confidence in initiating communication, discovering new social spaces, and adopting adaptive habits—processes that contributed directly to occupational re-engagement.
Driftwood elements, symbolizing personal strengths and liabilities, became more prominent post-intervention. Although participants initially struggled to identify their assets, structured group discussions and peer validation helped surface previously unrecognized internal resources. This shift aligns with studies emphasizing the power of guided reflection in enhancing self-awareness and occupational identity (Gregg et al., 2015; Iwama et al., 2009).
Finally, the visual depiction of water—the flow of life—transitioned from stagnant or fragmented in early drawings to more fluid and cohesive forms by the end of the program. This evolution parallels gains in psychological well-being, emotional processing, and proactive goal-setting. As in Newbury and Lape’s (2021) study with older adults, participants in our intervention experienced a renewed sense of empowerment and forward momentum. Together, these symbolic changes across the Kawa elements reflect meaningful therapeutic gains in how participants understood, managed, and narrated their occupational lives.
Quality of life
In this study, participants demonstrated statistically significant improvements in the social relationships domain of the WHOQOL-BREF, indicating enhanced interpersonal connection and social engagement following the intervention. While no statistically significant changes were observed in other WHOQOL-BREF domains such as physical health, psychological well-being, or environmental conditions, positive trends suggest the potential for broader life quality improvements with extended or repeated engagement. This pattern reflects the notion that social connectedness often serves as a foundational domain from which other aspects of quality of life can develop.
Community integration
Participants reported improved quality of life and significant gains in community integration, particularly in social participation. These results align with evidence supporting occupation-based group programs in enhancing community engagement for individuals with psychiatric conditions (Birgitta Gunnarsson et al., 2018; Queiroz et al., 2021). By fostering shared occupational experiences and encouraging proactive social behaviors—such as initiating conversations, navigating community spaces, and developing daily living routines—the intervention appeared to support real-world functional gains.
Implications for occupational therapy practice in community settings
The findings suggest that the K-FLOW program may be particularly relevant for community-based mental health services aiming to enhance social participation and occupational identity. In community outpatient settings, day programs, and psychosocial rehabilitation services, the Kawa Model can provide a structured yet flexible framework to facilitate reflective dialogue and collective meaning-making (Iwama, 2006; Taylor, 2017).
The use of metaphor and visual narrative tools may be especially beneficial for individuals who experience difficulties articulating internal experiences verbally. Organizing intervention sessions around progressive themes—from self-awareness to community participation—may support graded re-engagement in meaningful occupations.
For occupational therapists working in community settings, the Kawa-guided group format offers a culturally responsive approach that integrates assessment, goal-setting, and intervention within a single coherent framework (Iwama et al., 2009; Scaffa and Reitz, 2020). However, effective implementation requires therapist competence in group facilitation, reflective dialogue, and the application of metaphor-based therapeutic techniques. In community mental health contexts, attention to session structure, group composition, and opportunities for real-world occupational carryover is essential to maximize sustainable participation outcomes.
While the integration of culturally responsive metaphor and a pretest–posttest design represents a strength of this study, several limitations must be acknowledged. The small-sample size, absence of a control group, variability in group dynamics, and short follow-up period limit the generalisability of findings and restrict conclusions regarding causal relationships. Future studies should involve larger, more diverse samples and incorporate controlled, longitudinal designs to better assess the effectiveness and sustainability of such interventions.
Conclusion
In conclusion, this study provides promising preliminary evidence for the use of the K-FLOW program as a foundation for occupation-based group interventions targeting individuals with severe mental illness. By integrating culturally sensitive metaphors, visual narrative tools, and structured occupational engagement, the intervention fostered emotional insight, interpersonal empathy, and renewed occupational identity among participants. Statistically significant improvements in social participation and relationship quality, alongside meaningful visual and narrative transformations in river drawings, highlight the model’s potential to support both measurable outcomes and lived experience. Future studies should replicate these findings using larger, diverse samples and controlled longitudinal designs to refine the model’s broader applicability.
Key findings
Kawa-guided group intervention significantly enhanced social connectedness and community participation in individuals with severe mental illness.
Participants experienced renewed motivation and self-expression through metaphor-based engagement and reflective river drawings.
What the study has added
This study provides preliminary evidence that metaphor-based, occupation-focused group interventions can support psychosocial recovery and community participation in individuals with severe mental illness.
Footnotes
Acknowledgements
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The authors would like to thank all group participants for their valuable contribution to the intervention sessions and data collection process.
Ethical considerations
Ethical approval was obtained from the Çankırı Karatekin University Health Sciences Ethics Committee (Approval Code: E6B9CE2A02D84BAF) on July 8, 2024. Procedures followed institutional and national ethical standards and the revised Helsinki Declaration; confidentiality and data security were maintained throughout.
Consent to Participate
Written informed consent was obtained from all participants prior to their participation in the study.
Funding
The authors declared no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the analyses and findings of this study are available on request from the corresponding author.
Patient and public involvement data
During the development, progress, and reporting of the submitted research, Patient and Public Involvement in the research was included in the conduct of the research