
Abstract
Introduction:
While occupation-based intervention is the core concept of occupational therapy, the ongoing challenge of the medical model’s dominance over occupation-based practices persists worldwide. To facilitate the optimal implementation of occupation-based intervention within the Malaysian context, it is essential to explore pragmatic approaches that consider the developmental stage of the healthcare system, government policies, and the diverse cultural values and psychosocial statuses of the Malaysian population.
Methods:
Twenty-one experienced Malaysian occupational therapists were recruited through snowball sampling method for three focus group discussions, with each group comprising six to eight participants. Data were analysed by incorporating content and micro-interlocutor analysis.
Results:
This study presents findings from a large qualitative inquiry, focusing on solutions to enhance OBI in Malaysian occupational therapy practice. These solutions are further classified into five categories: (1) individual level, (2) public level, (3) professional level, (4) system and policy level, and (5) education level.
Conclusion:
This study highlights the measures that should be implemented at all these levels to ensure comprehensive solutions.
Introduction
Occupational therapy is a client-centred profession deeply committed to advancing the holistic health and well-being of individuals through the facilitation of purposeful engagement in meaningful occupations. The overarching objective of occupational therapy is to empower individuals to actively participate in the full spectrum of their everyday life activities (World Federation of Occupational Therapists, 2020). As a result, the professional identity of occupational therapy is grounded in occupation through occupation-based practice (Estes and Pierce, 2012). How occupational therapists shape their practices according to the profession’s philosophical beliefs has a positive dynamic relationship with professional resilience and occupation-based practice (Turner and Knight, 2015; Wilding and Whiteford, 2008). This includes the use of occupation-based intervention (OBI), as a well-established professional identity aligns therapists’ values and actions with the use of meaningful occupations to promote health and well-being (American Occupational Therapy Association, 2020a). Professional resilience, on the other hand, is a quality that enables occupational therapists to recover from adversity and persevere through difficulties when implementing OBI.
The literature supports the use of OBI and its effectiveness in diverse areas of occupational therapy practice (Che Daud et al., 2016; Colaianni et al., 2015; Novak and Honan, 2019; Tomori et al., 2014). However, translating the theory and research findings of OBI into practice may be demanding due to a range of internal and external barriers, including factors related to the client, occupational therapists, and the environment. These barriers may hinder the implementation of OBI in practice, especially for therapists who are early in their careers, as their limited experience in clinical reasoning and decision-making abilities can constrain practice (Shafaroodi et al., 2014). While previous work has suggested solutions to facilitate the implementation of OBI (Colaianni et al., 2015), these solutions may not be adequate to capture and address all the barriers to practising OBI in the Malaysian context.
While occupational therapy practice in Malaysia faced with similar barriers in implementing OBI as those reported in developed Western countries, there are also some differences. Barriers to occupational therapy practice in Malaysia stem from various factors, reflecting the country’s levels of development, sociocultural dimensions, socioeconomic and psychosocial status, public and professional awareness, and prevailing family beliefs and team mindsets that are further shaped by policy-related challenges. Specifically, within the Malaysian context, these barriers are classified as client factors, occupational therapy factors, and contextual factors (Che Daud et al., 2022). Since the barriers to implementing OBI vary across different contexts (Kaunnil et al., 2020; Klerk et al., 2016; Mahani et al., 2015), it is crucial to adopt strategies tailored to the local context.
The culture and beliefs of collectivist Asian societies, including Malaysia, differ significantly from the Western context, particularly in how independence is perceived and valued for individuals with illnesses or disabilities (Yang et al., 2006). In Malaysian culture, family roles are emphasized, and caregiving is often viewed as the responsibility of the family rather than the individual. This perspective can reduce the perceived importance of an individual’s participation in meaningful occupations, as reliance on family due to illness or disability is often normalized. In some cases, the sick role may also be culturally accepted, which can further encourage dependence on family members (Che Daud et al., 2022). Consequently, prioritizing individual autonomy and active engagement in meaningful occupations presents a challenge, even though the value of meaningful occupation is central to the principles of OBI. The socio-cultural dimensions, which reflect the society’s values and perceptions towards health, beliefs, and behaviours, also add unique challenges to the implementation of OBI in Malaysia. These challenges may include stigma towards illness or disability, and cultural expectations that family members should take over daily responsibilities when a person becomes unwell (Che Daud et al., 2022; Yang et al., 2006).
In addition, Malaysian occupational therapy practice is constrained by the bureaucratic system and biomechanical dominance as rehabilitation physicians govern this profession, thus reducing its’ professional autonomy (Loh et al., 2017). A study suggested that focusing on occupation-based theory can promote occupation-based practice (Colaianni et al., 2015). However, the lack of professional autonomy among occupational therapists may limit their flexibility and decision-making, which should ideally be framed by the practitioners’ philosophical beliefs rather than being constrained by the medical model.
Moreover, the Malaysian healthcare system and socioeconomic status influence the implementation of occupation-based practice. For example, Colaianni et al. (2015) describe building an occupation-focused context in occupational therapy departments, such as home-simulated settings that promote occupation-focused practice (Colaianni et al., 2015). However, such strategies may not be applicable across all healthcare settings in Malaysia due to varying contextual limitations. Limited resources and budget constraints, coupled with low awareness of the importance of occupational therapy itself, pose significant challenges. Additionally, for low-income earners, the need to prioritize financial necessities over therapy sessions may conflict with participation in OBI.
Given that, implementing OBI in clinical practice can be challenging. However, overcoming barriers will enable optimal integration into practice, allowing the profession to reconnect with its foundational principles. This, in turn, will support the reestablishment of a strong professional identity. Therefore, occupational therapy practitioners and researchers need to develop strategies to strengthen the application of OBI, thereby helping to restore and reinforce the professional identity. More realistic and precise strategies should be developed to enhance OBI within the Malaysian context through local perceptions, experiences, and opinions. This study aimed to explore the possible ways to enhance the implementation of OBI through a series of focus group discussions.
Methods
Design
This study is an extension analysis of rich qualitative data from a previously conducted study (Ahmad et al., 2022). Data were obtained from three focus group discussions (FGDs), and the analysis yielded three main content groups: (1) the use of OBI; (2) perceived barriers to OBI implementation; and (3) solutions to enhance OBI. This article addresses the third group, specifically, potential solutions for enhancing OBI in Malaysian occupational therapy practice. The FGD method was utilised within a qualitative phenomenological approach to explore participants’ perceptions, opinions, and lived experiences regarding OBI in the Malaysian context.
Three FGDs were conducted at the Faculty of Health Sciences, Universiti Teknologi MARA (UiTM) Selangor, Malaysia. Ethical approval to conduct the study was obtained from the UiTM Research Ethics Committee [Approval code: REC/07/2020 (MR/161)] and the Medical Research and Ethics Committee (MREC), [Approval number: NMRR-18-2913-44105(IIR)].
Participants
A snowball sampling method was employed to recruit participants. The research team identified potential and suitably qualified candidates to participate in this FGD based on the designated inclusion and exclusion criteria. Participants were eligible for inclusion if they (1) were Malaysian occupational therapists working in clinical or academic settings; (2) were identified by colleagues or professional contacts as occupation-based practitioners; (3) had experience of using occupation in practice, either as an end or as a means, across any practice area; and (4) held a senior position with at least 5 years’ clinical experience in either the government or private sector. Participants were excluded if they practised outside Malaysia or did not provide consent to participate in the FGD. These exclusion criteria were applied to ensure that all participants had relevant local experience and were able to contribute meaningfully to the FGD.
The research team emailed 23 shortlisted candidates from various practice areas and settings to ascertain their willingness and availability before joining the FGD. A formal letter was then sent to each potential candidate outlining the details of the FGD. The formal letter clarified how this study might benefit the participants and the research team to ensure transparency. They were also asked to sign the consent section of the letter if they agreed to participate. All contacted candidates confirmed their participation except two, who withdrew for personal reasons. Participants were not given any financial incentive to participate in the FGD.
Data collection procedure
All three FGDs were facilitated by experienced moderators and assisted by assistant moderators to take field notes. The study followed a semi-structured FGD guide developed through a discussion among the research team members. During the FGD, the research team consisted of six members, five of whom were PhD-qualified occupational therapy academics with extensive experience in qualitative research and the topic, and one clinical instructor who served as the main author. Some participants were previously acquainted with members of the research team. To minimise potential bias, participants who had close relationships with the moderators were assigned to different FGDs. The FGD began by introducing participants to the consensus definition of OBI within the Malaysian context reported by Ahmad et al. (2022), as well as the barriers to implementing OBI identified in a previous study by Che Daud et al. (2022). The discussion then explored participants’ perceptions, opinions, and lived experiences related to solutions of employing OBI in the Malaysian context. Each FGD was recorded using a digital recorder and lasted approximately 60–90 minutes. The discussions were facilitated in either Malay or English or a combination of both languages (i.e., pidgin) to encourage casual conversations that could generate rich and meaningful insights, effectively capturing the participants’ intentions and expressions. No follow-up FGDs were conducted, as the research team collectively agreed upon sufficient data richness after the three FGDs.
Data analysis
Data analysis followed the framework proposed by Nili et al., (2017), which provides a structured approach to analysing FGD data. The transcripts were organised based on the identified content group: solutions to enhance OBI in Malaysian occupational therapy practice, and irrelevant data were excluded from the analysis. Data from all three FGDs were analysed together rather than separately. The unit of analysis was the condensed meaning unit (Nili et al., 2017), which referred to a phrase, sentence, or short segment of dialogue that conveyed a single idea related to solutions for enhancing OBI.
The analysis was conducted individually by the first author using both manifest content analysis (MCA) and latent content analysis (LCA). MCA was used to identify explicit statements and visible meanings in the participants’ responses, while LCA was used to interpret the underlying meanings, assumptions, and contextual implications of the data (Nili et al., 2017). This approach was appropriate because the study aimed to identify both practical solutions stated directly by participants and deeper meanings embedded within the FGD. Discussions between the first author and the research team were conducted after every stage of the content analysis, including the coding process, manifest content analysis, latent content analysis, and the final stage of categorizing the findings.
In MCA, the first author coded sentence fragments or phrases from condensed meaning units (CMUs). The codes were first grouped into subcategories and then organised into categories based on similarities and differences across all three FGD transcripts. Discussions between the first and research team ensured consensus on the coding process. Each category was interpreted based on the underlying meanings, and the entire research team reached consensus on the final interpretation. For CMUs with unclear meanings, LCA was applied, allowing the research team to interpret them in more depth. The LCA subcategories were either grouped with existing MCA subcategories or new subcategories. In the end, the subcategories from MCA and LCA were merged to form the final findings, which were then presented as categories and subcategories. Micro-interlocutor analysis was also employed to record the number or proportion of participants who agreed, disagreed, or expressed no view on each category. Supporting or dissenting statements were documented to reflect the range of perspectives (Onwuegbuzie et al., 2009).
Trustworthiness of study
The trustworthiness of the study was established through several strategies. To ensure credibility, the research team collaboratively agreed on all stages of the study, including the development of the FGD guides, data analysis, and final findings. Credibility was further enhanced through member checking, in which two participants who were selected based on their expertise and higher qualifications reviewed the transcripts and preliminary analysis to ensure accurate representation of their perspectives. An audit trail was maintained to document decisions made during data analysis to track any changes during coding decisions and provide a transparent trace of the research process. The use of Consolidated Criteria for Reporting Qualitative Studies (COREQ) guidelines further enhanced the rigour and transparency of reporting (Tong et al., 2007).
Findings
Table 1 presents the demographic characteristics of the participants, who represented diverse areas of occupational therapy practice. Their qualifications ranged from bachelor’s to doctorate levels in occupational therapy. Most participants worked in the public sector, including community health facilities, tertiary hospitals, and schools, while those in the private sector, mainly specializing in paediatrics, worked at independent centres. One participant was a freelance therapist providing services at a private centre and clients’ homes. In total, 21 participants were recruited across three FGDs (eight, seven and six participants). Paediatric specialists formed the largest group, with 14 out of 21 participants.
Demographic characteristics of participants.
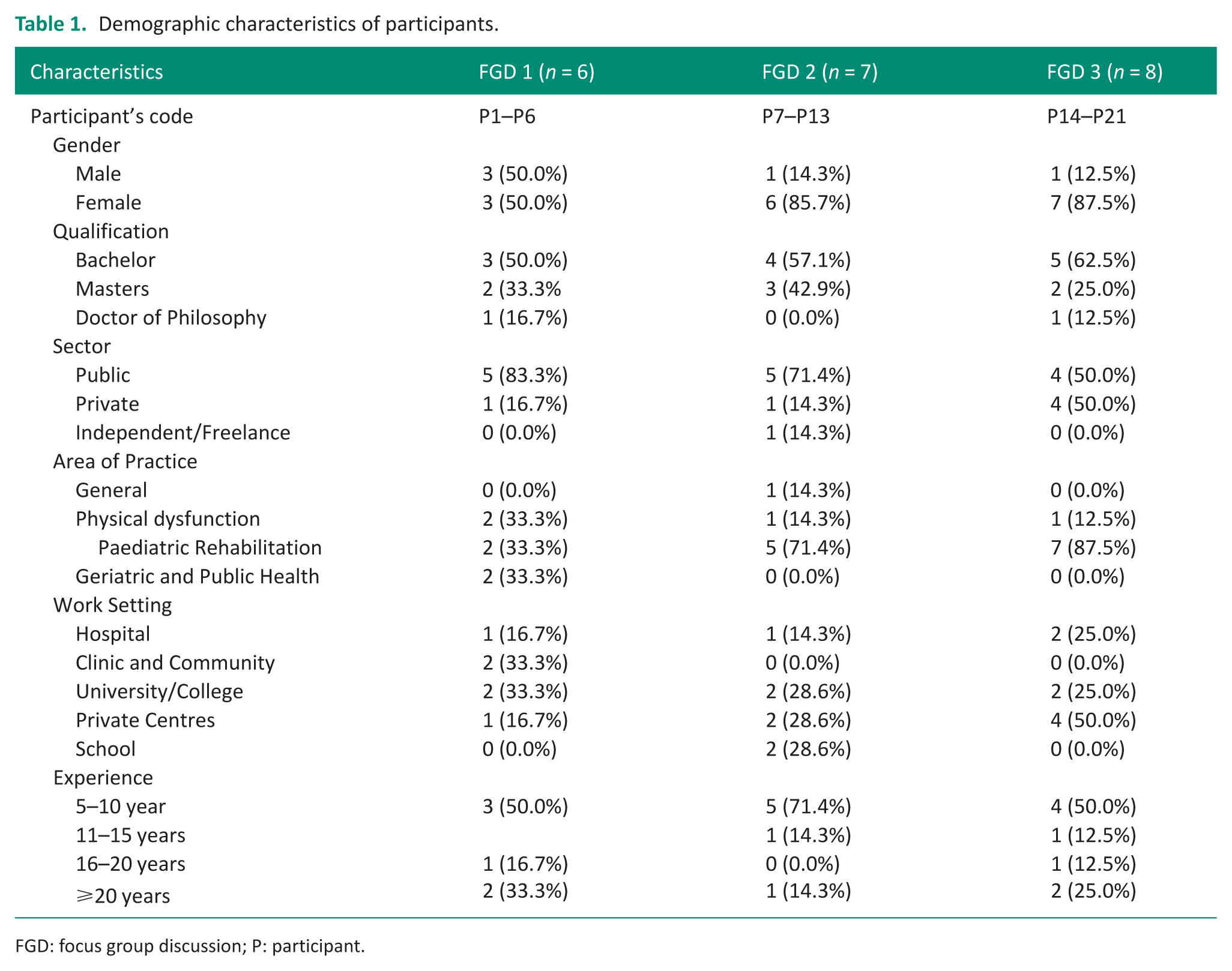
FGD: focus group discussion; P: participant.
Five categories emerged from the analysis of the content area related to the third group of the study findings (Figure 1). These categories were formed after reviewing the transcriptions multiple times: [1] individual level, [2] public level, [3] professional level, [4] system and policy level, and [5] education level. Based on the participants’ inputs, these categories primarily addressed solutions to enhance OBI implementation in the context of Malaysian occupational therapy practice.
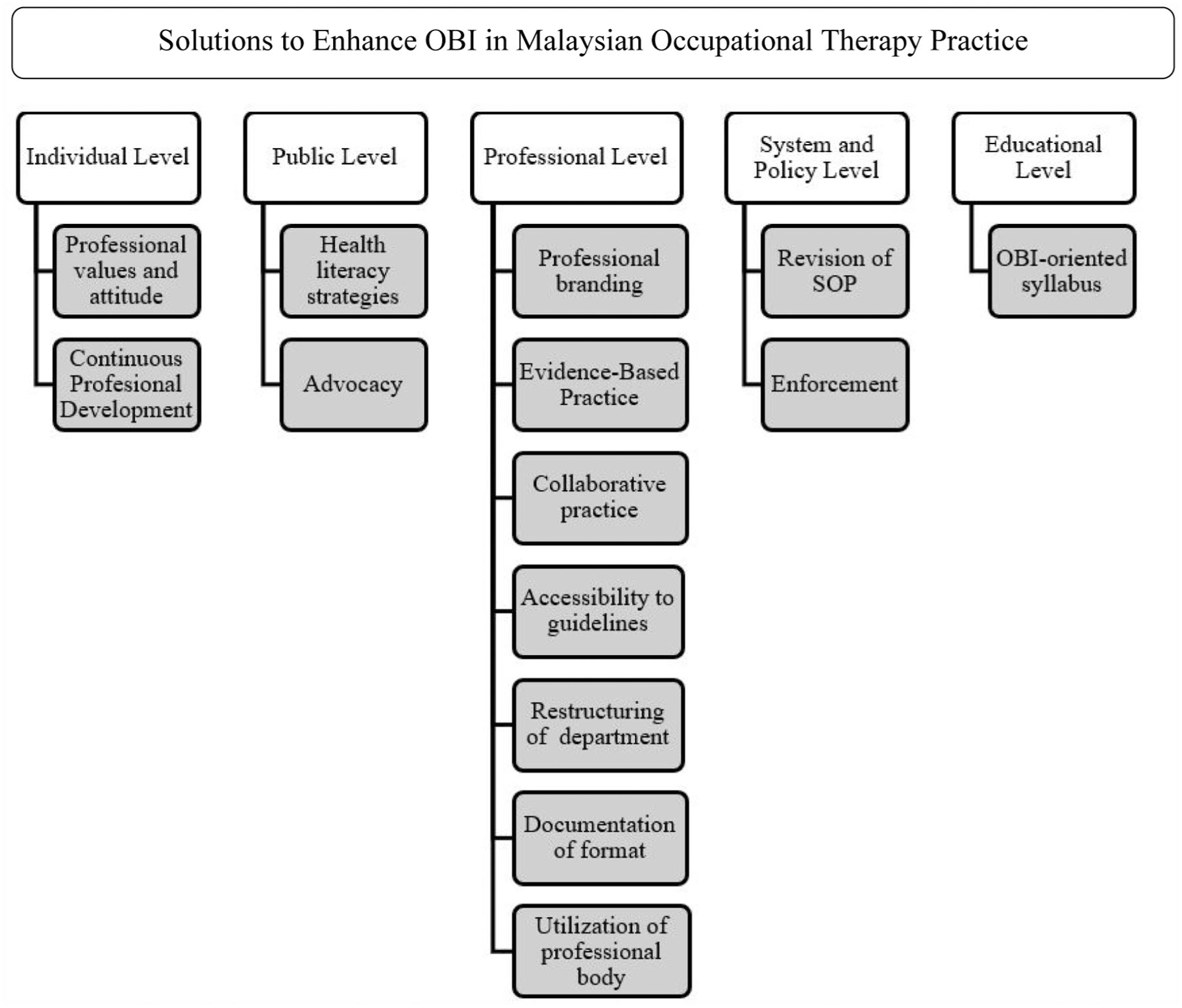
The categories emerged after integrating the MCA and LCA.
Individual level
Individual occupational therapists play a role in making OBI a viable option in practice. Proactive strategies to address the barriers to implementing OBI should be carried out beyond a one-party level to ensure its entirety and comprehensiveness in addressing the wide range of barriers. The approach to resolving issues at the individual level should be rooted in professional values and attitudes, supported by a commitment to continuous professional development.
From the FGD, key values identified include sound judgement in delivering OBI and the prudence to provide well-reasoned clinical decisions for each intervention, as highlighted in the core values of the Occupational Therapy Code of Ethics (American Occupational Therapy Association, 2020b). Clinical reasoning is of cardinal importance in ensuring the compatibility of occupational therapy practice within the medical model dominant setting. Sound clinical reasoning can be used in professional interactions with the multi-disciplinary team (MDT). Therapists have a right within the profession to give a professional justification but must be complemented with evidence. (P6, FGD 1)
Therapists are also expected to commit to self-reflection, thoughtfully integrating their knowledge through careful reflection on their practice attitudes: Therapists need to embrace the client and family-centered approach while reducing the therapist-centered approach in practice. Through this, we will be able to provide something necessary for clients and ensure the intervention's feasibility. (P1, FGD 1) I think it goes back to the therapists’ attitude and how they do it. Therapists should not be in their comfort zone and do the same thing repeatedly without trying to improve the practice. (P8. FGD 2) To practice the OBI, therapists must be creative and able to modify and tailor the intervention appropriate to the client's needs. (P19, FGD 3)
Continuous professional development, including training, sharing sessions, and discussion through various media has been suggested by the participants in this study to strengthen the skills and knowledge of Malaysian occupational therapists, We can overcome these issues by providing lots of training for therapists. Maybe we can organize a symposium to have a sharing and discussion session among occupational therapists. To meet up and share experience and listen to opinions from the experts. (P8, FGD 2)
Workplace mentoring is another measure that can keep therapists constantly endowed with continuous education, As a senior, we need to mentor the junior. (P7, FGD 2) I think I have the responsibility to educate the young therapists. Whenever I come to the fieldwork setting, I will share and train the therapists. (P19, FGD 3)
Public level
Public awareness and understanding of occupational therapy are still lacking in Malaysian society. The lack of public awareness and understanding has consequently challenged the implementation of OBI in Malaysian practice. Therefore, it is important to develop public engagement strategies that actively involve the community. Insights from this FGD study suggest incorporating health literacy and advocacy to promote OBI.
The strategies included using various methods to spread awareness and increase understanding regarding the importance of health and participation. The participants in this study have not explicitly stated the term health literacy but alluded to some statements, such as As therapists, we need to educate and tell the caregivers or parents why we give that particular intervention to their children. Before ending my session, I will recall everything I have done and show it to the caregivers. (P6, FGD 1)
These participants indirectly suggested providing caregiver training through demonstration to enable the recipients of services to understand the treatment’s purpose and process Sometimes it happens when the occupational therapists and special educators do the same things. However, when we provide an example to them by doing it, we are educating them to focus on occupation in their children. So, they will be able to know our roles. (P18, FGD 3)
One of the suggestions to ease the provision of education despite the time constraints and challenges is to gather clients and conduct classes for them, We have to use the educational approach. If clients don't understand, we cannot go further with the treatment, or it will just be a waste of time. As we may have a very limited time, maybe we can gather the clients of the same conditions and make a class to explain and educate them. (P19, FGD 3)
Another strategy to address the lack of understanding of occupational therapy roles is by providing explanations tailored to the client’s educational level and cultural background without using occupational therapy’s jargon, which can make the information easier for clients to understand: I will explain the role of OT during the evaluation and screening process. I will prepare my treatment plan and use simple explanations by using an appropriate term to allow a comprehensive understanding. (P9, FGD 2)
Advocacy was ambiguously defined, and its broad definition has distanced the term from practical application in Malaysian occupational therapy practice. However, a participant’s statement has depicted the action-oriented measure to recognize any opportunities provided and assist clients with equitable treatment as a part of advocacy. The research team had discussed in detail and agreed to regard this as an act of advocacy, Every month, we will find any students [paediatric] who are entitled to get the Islamic welfare (Zakat benefits) depending on the family incomes and the parents' salary. We will support the clients to obtain welfare benefits. (P20, FGD 3)
According to this statement, it could be inferred that the therapist assists clients in recognizing the opportunities and support for welfare entitlement. The advocacy efforts were primarily undertaken at the public level, although they could extend beyond this, as addressing policy changes requires more unified and strategic planning.
Professional level
Additionally, the findings from the FGD highlight several measures that need to be implemented at the professional level. The measures are professional branding, evidence-based practice, collaborative practice, accessibility of practice guidelines, department restructuring, documentation format, and utilization of a professional body.
Occupational therapy should be empowered and recognized, especially by the MDT and the service beneficiaries. Professional branding was an empowerment strategy to promote the profession. It can be performed by occupational therapy personnel through various techniques, as stated by participants in this study.
The profession’s core principle and main role should be displayed to encourage visibility. There are several ways therapists can adopt in practice to improve their visibility and promote the profession, It will be a good idea to provide a folder or materials with the lists of suggested activities for clients. These kinds of things can make our profession visible. The doctor or MDT can see the example of occupations; hence they will know about our roles. (P1, FGD 1) Some clinics have started developing their occupational kits that could aid in the OBI practice which are based in biomedical settings. (P3, FGD 1)
The visibility also includes a professional’s logo as a way to market the profession, . . .and do not forget to put our logo on the kit. The occupational therapy logo. Then make sure to emphasize occupation. (P1, FGD 1)
Besides, occupational therapists need to use the standardized assessment as a communication tool with the MDT for professional branding. It can indirectly help define occupational therapy practice, especially when using occupation-based assessments. Two of six participants in FGD 1 had raised the importance of using occupation-based assessments in practice, Here comes the importance of using occupation-based assessment. (P1, FGD 1) In MDT, we should use the assessment as a communication tool. What we charge, we should be the expert. We can show them the assessment that we have conducted. (P4, FGD 1)
In response to these opinions, a participant suggested a solution to establish a specific occupation-based assessment to portray the profession’s identity, other than the Modified Barthel Index (MBI) assessment, because it was not sufficient to represent the overall picture of occupational therapy. As mentioned, the MBI assessment has become the primary assessment in Malaysian occupational therapy practice, We may need to establish a specific occupation-based assessment as a tool to support our identity. For instance, currently, in the clinic’s domiciliary practice, we are using the Modified Barthel Index (MBI) assessment as an indicator to measure the client’s disability and progress. When we communicate with the MDT, they will know the MBI assessment. So, why not try to add another assessment to bring along with the profession. (P3, FGD 1)
Another method to display the role of occupational therapy is through the referral form. It was argued that occupational therapists had received a lack of referrals for OBI because the MDT was unfamiliar with the terminology. Therefore, the MDTs will only go for what is available on the referral form, which mostly focuses on the impairment aspects or just a generic form of occupation: The unfamiliarity with the terminology itself may be the cause. The MDT is not familiar with it. We can shift the paradigm so people can see our significant role by stating the term “OBI” in the referral form. (P11, FGD 2)
Two other participants from this FGD agreed to this suggestion by stating, Even if the doctor knows about our role, but the option in the referral form is limited and not comprehensive as it does not include the OBI. Hence the doctor cannot make a referral directly stating the OBI. (P7, FGD 2) We need to broaden the option. (P10, FGD 2)
Evidence-based practice was another solution to enhance OBI implementation in Malaysia. There is a paucity of evidence to support the practice of OT in Malaysian practice. The lack of a platform to publicize the power of occupation has made it difficult for OTs to stand up for righteous practice. However, the occupational therapy personnel can be the mediator to convey the message to the MDT and the clients, We need to prove it while serving. (P6, FGD 1)
One participant suggested research as a solution to aid in the understanding of the MDT and clients regarding the use of occupation in practice, We need to prove through research. (P3, FGD 1)
A participant had called for OTs to carry out clinical research to combat the scarcity of research investigating the effectiveness of OBI, particularly in the Malaysian context, It is imperative to publish the results. Even if we have done so many with clients for months, but if we did not have widespread the result or effectiveness of our intervention, people remain unknown. (P1, FGD 1)
Occupational therapists can come up with the evidence to underpin the practice and an effort to bring changes and improve the current practice, which is restricted due to the policy and system, To change the existing standard operation procedure and policy in Malaysian OT practice to be more towards OBI, we need to do a lot of assignments to prove why we need to centralize OBI in practice or something to support the current statistic requirements. (P1, FGD 1)
Additionally, collaborative practice is vital to allow more chances to implement OBI within the practice. The partnership between the academician and the clinician is essential to ensure an overarching understanding of the ideal and current reality. The sharing of knowledge can be used to complement the gap practice, while the real and hands-on experience in the fieldwork can inform the pragmatic implementation of OBI within the real environment, We need to increase the collaboration between the clinician and the academician and between the private and public practitioners. Among the efforts is through a symposium. A clinician can share the clinical experience while the academician can share the theoretical knowledge and current evidence. (P3, FGD 1)
The academicians and the clinicians can join forces to collaborate in conducting research. This effort can help to publish more gold-standard evidence to inform practice, If the clinicians have the data, they can collaborate with other parties who can design the study. (P1, FGD 1)
Besides, the inter-sectoral collaboration between the public, private, and other organisations was also suggested to be integrated into practice. The public–private integration was mentioned in the discussion, A system needs to be developed to link the public and private practice. There are many limitations in public practice. Therefore, there should be a linkage to ensure the continuation. (P21, FGD 3)
Another participant agreed by stating another supporting statement, To settle the issue of the difficult care continuum, just like mentioned, we need networking. Secondly is to have a medium to ensure continuity from one stage to another, which will not stop only in the public sector since the practice there is limited. The transition process is from the early stage until the end stage. (P18, FGD 3)
A crucial solution is to work integratively with the MDT. Participants agreed that by working in the MDT, the healthcare profession’s distinct roles are more evident than when working solo: We can avoid the overlapping of work by working in a team. Sit together and have a discussion for intervention planning. (P8, FGD 2) If we work together with a team in one session, we can be more focused on our real aim and be able to perform OBI. For example, if to train a client for toileting, physiotherapists can do what they should be doing, and we can proceed with our role. (P15, FGD 3)
A participant further clarified this opinion by stating, I agree with the opinion because I have worked in a rehabilitation hospital. We worked in a team [MDT] and did the treatment together. Hence, every professional can perform their roles, and OT can do OBI. (P14, FGD 3)
Occupational therapists need to have OBI practice guidelines readily available. Participants in this study had substantially mentioned the profession’s requisite to develop a more comprehensive practice guideline on OBI. It should be accessible to all members of the profession, OTs should move towards developing its own guidelines of practice or module. (P3, FGD 1)
One suggestion is to set up a one-stop library to fulfil the occupational therapists’ need to have access to references when needed, especially if any members work alone in a private centre. However, it was not mentioned what type of library, whether a physical or an electronic library, but the idea was to gather the compendium of relevant information in one place, OTs can propose to have a library to which all members can have access. In the library it should have the evidence-based assessments, tools, equipment and training. (P18, FGD 3)
Restructuring the department was another solution that the participants proposed, If we only have exercise equipment in the department. By changing the setting, then only it can fulfil the need of OBI. (P4, FGD 1)
As mentioned by the participant, the current set-up of the department, especially for the physical area, is more towards a medical set-up with exercise equipment. In the facility, the environment should accommodate the requirement for occupational training with appropriate and related instruments instead of a medical-based set-up of departments that only have exercise modalities and impairment-based equipment.
Besides, therapists also need to use creativity to restructure the department and construct a specific area for OBI, It might be difficult to change the set-up in the public settings. What therapists can do is to use their creativity by arranging the equipment and have a designated area for OBI. (P21, FGD 3)
A participant highlighted the professional body’s current efforts to standardize the documentation format, ensuring it better reflects the unique role and identity of occupational therapy. The aim is to incorporate more occupational therapy-specific jargon and frameworks into the current SOAP format so it can better represent the role and identity of occupational therapy. It is also beneficial to promote an understanding of occupational therapy roles. As one participant explained, We want to update the documentation format and its’ contents because sometimes even the progress report was not sufficient to portray the roles and identity of OT. We wanted to go back to occupation. (P3, FGD 1)
The suggestion was to use the same language to ensure uniformity in communication. Occupational therapists can use a standard language using the Occupational Therapy Practice Framework (OTPF) (Ahmad et al., 2022; American Occupational Therapy Association, 2020b), and consider using the International Classification of Functioning, Disability, and Health (ICF) (World Health Organization, 2013) when dealing with other healthcare professionals, We want to encourage OTs to incorporate the use of OTPF in the internal documentation. However, when communicating with other professionals, we need to use the universal language as in the ICF for others to have the same understanding. (P3, FGD 1)
Malaysian Occupational Therapy Association (OT Malaysia) spearheads the profession. Therefore, the OT Malaysia can be utilised as a medium to lead the development and evolution of the profession: For me, a profession can forge ahead when they work in unity, which means in our context, we can ask for the OT Malaysia and Malaysian Allied Health Professions Division to assist in the process. For example, if we want to refine the Standard Operating Procedure (SOP). (P11, FGD 2)
The professional body should recognize the concerted efforts and solidarity of the professionals. It can be the platform for members to bring up the subject of matter to the governing body.
System and policy level
Under the system and policy level, the participants suggested revising and refining the existing standard operating procedure (SOP) by emphasizing the top-down approach and occupation-based assessments and intervention. Three of six and three of seven participants in FGD 1 and 2 believed that the current SOP needs to be revised by emphasizing occupation-based practice in the SOP: We need to establish Standard Operation Procedure for OBI. (P3, FGD 1)
A participant further elucidated the opinion to refine the existing SOP instead of developing a new one, OTs should move towards developing its own guidelines of practice or module. (P3, FGD 1) It is not to develop a new SOP, but to refine the existing SOP so it will not only focus on impairment-based treatment. We want to highlight the occupation. (P11, FGD 2) The OTs in the public sector need to enhance the SOP according to the current practice. Because sometimes the elements in the existing SOP are outdated. (P13, FGD 2)
Nevertheless, a participant stated a different opinion regarding the use of SOP in the private sector, The practice in the private sector is not restricted by the SOP. (P8, FGD 2)
The remaining three have neither stated any dissenting view nor provided any related statement to support this suggestion. However, they also did not exhibit any negative responses through verbal and non-verbal actions. Additionally, enforcement is another suggested solution for resolving the existing issues in implementing OBI. The enforcement will be in terms of using assessment and establishing an occupational therapy assistant (OTA) position to lessen the burden and workload. One participant had generally stated the necessity for enforcement to be initiated as a solution to this issue, It is about our enforcement, policy, SOP and key performance indicator (KPI) measurement. (P16, FGD 3)
Other participants have indicated agreement with this statement by nodding their heads and voicing agreement towards P16’s general statement. Another participant further commented regarding this matter, Enforcement is critical in the public sector’s practice. When I was working in a private hospital, I had to use the Canadian Occupational Performance Measure (COPM). Therefore, I have to learn and get used to it no matter what. (P15, FGD 2).
Another participant from FGD 1 mentioned a point regarding the establishment of an OTA position since Malaysia has yet to adopt this position in the hierarchy of the organisation, I think we already need to think about it. The position of OTA should be established to have a more productive workflow. In the current situation, the 41-grade officers (U41) are in charge of management but at the same time still need to handle the clinical duty. (P1, FGD 1)
Education level
Finally, the solution should be addressed at the educational level, ensuring future occupational therapists are well prepared before embarking on their fieldwork journey. One participant emphasized the need for a specific subject for OBI and suggested revising the syllabus to make it more OBI-oriented, The measure should start from the education because the first exposure to knowledge is from the college or university. So, the syllabus should contain a specific subject on OBI. (P3, FGD 1)
Early exposure to OBI practice at the university level equips students with the theoretical knowledge and practical skills necessary to implement OBI effectively. A participant raised concerns about students being easily influenced by impairment-based practices when they go for clinical placement, Sometimes, when I visit my students during their clinical placements, they focus more on impairment-based practices despite trying to promote occupation-based knowledge to them in college. (P13, FGD 2)
This statement indicates the need for educational measures to train future occupational therapists as early as possible, focusing on shaping their mindset during their academic years to become an occupation-based practitioner.
Discussion
This study gathered insights from Malaysian occupational therapists on strategies to overcome barriers to implementing OBI. Solutions must be initiated at the individual level and carried forward by therapists at the professional level before extending to the system and policy domains. At the individual level, therapists must cultivate professional values, such as knowledge, competence, and experience, through clinical practice, mentoring, and continuous professional development (Colaianni et al., 2015). This indicates that individual therapists have a crucial role in ensuring OBI’s feasibility despite multifaceted barriers. Given the organizational and bureaucratic challenges within the public sector in Malaysia (Ahmad et al., 2021; Che Daud et al., 2022), therapists need to adopt a creative approach to adapt their practice (Estes and Pierce, 2012; Murray et al., 2020).
At the professional level, evidence-based practice is crucial. Pilot testing and advanced clinical research are necessary to establish the effectiveness of interventions and support OBI with robust evidence (Berlet and Kaskutas, 2020). Therefore, continuous professional development should also focus on enhancing research skills to foster evidence-based practice among occupational therapists (Mulligan et al., 2014). As occupational therapy needs to shift away from a medical-model-dominated approach, robust evidence is critical to support OBI, including initiatives like professional branding and department restructuring (Wilding, 2011). Clinicians should collaborate with academic institutions to bridge the gap between theoretical knowledge and practice (Colaianni et al., 2015; Crist et al., 2005). For example, this collaboration can raise awareness about OBI, help define meaningful occupations within a specific environmental context; therefore, making occupation-based setups more relevant to practice. Research also plays a pivotal role in developing comprehensive OBI guidelines (Colaianni and Provident, 2010), as it is vital for demonstrating the effectiveness of OBI and advocating for its adoption among other healthcare professionals, therapy recipients, and policymakers (Cramm et al., 2013).
Health-seeking behaviours in Malaysia may differ from those in Western contexts, particularly in terms of accessibility and localization. A study in Malaysia found that rural adults in Malaysia are less likely to seek healthcare from professional practitioners compared to their urban counterparts (Mohd Noh et al., 2022). Therefore, adapting practices to align with local cultural norms is essential. Clinical research within this context, as part of evidence-based practice, can guide culturally relevant interventions. Occupational therapists should leverage cultural diversity to enhance client-centred care, working collaboratively to achieve client well-being based on their definitions. Research and development at the professional level, as suggested in this study, can facilitate this adaptation. For instance, developing tools like the Aid for Decision Making in Occupation Choice can streamline client-centered practice and OBI (Nagayama et al., 2016). Moreover, culturally specific activities, such as prayer, should be better integrated into standardized assessments to align with cultural expectations.
Documentation revision is needed to convince stakeholders of the value of occupation in promoting health and well-being, equal to impairment-based treatments within the medical model. This effort should begin at the professional level and extend to system and policy levels, such as revising SOPs and establishing legislative standards to protect occupational therapy practice (Jackman and Stagnitti, 2007). At the broader workforce level, the suggestion to consider an occupational therapy assistant role should be viewed as a workforce consideration rather than a confirmed need in Malaysia. Any future consideration of this role would require careful evaluation of role boundaries, regulation, and supervision to ensure that OBI is supported without weakening occupational therapists’ professional identity. Expanding research and development on OBI will provide the scientific evidence necessary to support and publicize occupational therapy’s value.
Closer partnerships between clinicians and academics are essential for enhancing the understanding of OBI, grounded in occupational science (Vermaak and Nel, 2016). Such collaborations should extend beyond the academic–clinician relationship, involving interdisciplinary teams and professionals such as doctors, other health professionals, and teachers (Jackman and Stagnitti, 2007; White et al., 2013). Promoting access to guidelines at the professional level can help align academic curricula and clinical training with occupation-focused outcomes, increasing the likelihood of OBI adoption (Di Tommaso et al., 2016). In pursuit of evidence-based practice (Thomas et al., 2017), education curricula must be revised to emphasize OBI, with a focus on professional identity and occupation-based education (Estes and Pierce, 2012). Revising university-level curricula to focus more on OBI is essential to prepare future practitioners by strengthening the foundation for occupation-centred practice at both educational and professional levels. This includes providing structured opportunities for students to translate theory into practice, strengthening their occupational therapy knowledge, skills, and competence prior to placement, and ensuring adequate theoretical preparation before undertaking fieldwork education (Pashmdarfard et al., 2021; Pashmdarfard et al., 2022).
Conclusion
This study highlights the need for solutions at multiple levels, including individual, public, professional, system and policy, and educational to preserve the profession's identity while embracing its core concept. These solutions are dynamic and interrelated. For instance, individual therapists must actively equip themselves with OBI knowledge, while education should foster an early understanding of the OBI framework and approaches. The public should be educated on strategies to enhance health literacy and advocacy. Meanwhile, at the professional level, prioritizing research and development, including evidence-based practice, is crucial for advancing OBI practice across diverse contexts and challenges. Key initiatives such as professional branding, fostering collaborative practices, ensuring accessibility to guidelines, restructuring departments, improving documentation and utilization of professional body are vital to strengthening OBI implementation. Additionally, at the system and policy level, revising SOPs and enforcing regulations can further support the adoption of OBI practices. Although the findings offer practical solutions for addressing OBI barriers among Malaysian occupational therapists, the study’s scope is limited to specific practice areas and relies solely on a FGD methodology. Future research adopting a more empirical approach is needed to refine these strategies and ensure their relevance to local needs and broader applicability.
Key findings
OBI in Malaysia must operate at multiple levels, including individual, public, professional, system and policy, and education.
Therapists’ professional values, clinical reasoning, and commitment to continuous development are central to maintaining OBI within medically dominated systems.
Collaborative efforts across clinicians, academics, professional bodies, and policymakers are essential to develop guidelines, restructure services, and align documentation and education with occupation-based practice.
What the study has added
This study provides the first in-depth exploration of Malaysian occupational therapists’ perspectives on multi-level strategies to strengthen OBI. It highlights context-specific actions that can be taken at individual, organisational and system levels to promote occupation-based practice within a collectivist, resource-constrained healthcare context.
Footnotes
Author’s Note
Mohammed Alrashdi is now affiliated to Department of Health Information Management and Technology, College of Applied Medical Sciences, University of Hafr Albatin, Hafr Albatin, Saudi Arabia.
Ethical considerations
This study was approved by the Ethics Committee of Universiti Teknologi MARA, Malaysia (Ref. No: REC/07/2020 (MR/161) and the Medical Research and Ethics Committee (MREC; Ref No: NMRR-18-2913-44105(IIR).
Consent to participate
Written informed consent to participate in this study was obtained from all participants prior to data collection. No identifiable personal data, images, or videos are presented in this manuscript.
Author contributions
AA, AZCD, FWY, and MHR conducted the study, reviewed the literature, and led data collection. Data analysis was conducted by all members of the research team. AA drafted the manuscript and critically reviewed by AZCD, FWY, KT, MHR, MA. All the authors approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the World Federation of Occupational Therapists through the Thelma Cardwell Foundation Award for Research (Grant Number: 100-IRMI/INT 16/6/2(021/2018)) and Universiti Teknologi MARA.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Patient and public involvement data
During the development, progress, and reporting of the submitted research, Patient and Public Involvement in the research was not included at any stage of the research.
Reporting guidelines
This study was conducted and reported in accordance with the COREQ (consolidated criteria for reporting qualitative research) guidelines.
Device status
No devices were used in this study.