
Abstract
Introduction:
Becoming a father is a major life transition, and some men experience mental ill health during this period. As occupational therapists view wellbeing as fundamentally linked to participation in meaningful occupations, it is important to understand how fatherhood affects occupational engagement. This study explores first-time fathers’ perceptions of how their occupations change across the perinatal period.
Method:
Participants were recruited through father specific groups and social media. Six first-time fathers, all within 2 years of becoming parents, took part in semi-structured interviews. Data were analysed inductively using reflexive thematic analysis.
Findings:
Fathers described significant shifts in their occupational engagement, with both beneficial and challenging effects on wellbeing. Many noted conflicting societal expectations surrounding the ideal of the “involved father,” which influenced how they perceived their new role. Participants frequently felt unprepared for parenthood and highlighted the lack of accessible, father-specific support.
Discussion:
The transition to fatherhood brings substantial changes to daily occupations, as new roles emerge and existing activities are renegotiated. The tension between expectations of active involvement in parenting and ongoing workplace demands presents unique challenges, which are insufficiently addressed by current service provision. Occupational therapists are well placed to offer interventions to fathers during the perinatal period.
Introduction
Becoming a parent represents a significant life transition, during which fathers experience elevated rates of depression and anxiety compared with men who do not have children (Cameron et al., 2016; Leiferman et al., 2021). These rates are likely underestimated, as men are more prone to underreporting symptoms, and most perinatal mental health screening tools have been developed and validated primarily for use with mothers (Fisher et al., 2021; Psouni et al., 2017).
In the United Kingdom, perinatal mental health has increasingly emerged as a government policy priority. Policy directives emphazise accessible, early, and family focused service provision to ensure that each child has the best start in life (Health Education England, 2018; National Health Service (NHS) England, 2018; Public Health England, 2019). Some progress has been made in relation to accessibility. For example, the Maternity Transformation Programme has sought to implement the vision articulated in Better Births, advocating for perinatal mental health services that are delivered closer to home (NHS England, 2016). Similarly, the NHS Long Term Plan (NHS, 2019) recommends extending the perinatal period from the traditional timeframe of conception to 12 months, up to 24 months postpartum. This extension reflects recognition that the first 2 years of a child’s life are crucial for the formation of parent–child attachments, which play a central role in shaping children’s future mental health and developmental outcomes (Department of Health and Social Care, 2021).
Policy reform has also occurred in relation to parental leave. The Children and Families Act (2014) introduced shared parental leave, enabling fathers to assume greater responsibility for infant care during the first year. This legislation aligns with broader societal shifts across western contexts, where fathers are increasingly expected to take on a more active caregiving role (Letourneau et al., 2012; Yogman and Eppel, 2022). Despite these shifts, and despite recognition that paternal mental ill health can adversely affect children’s emotional and developmental trajectories (Ramchandani et al., 2005, 2008) as well as maternal mental health (Philpott, 2022), policy actions to ensure genuinely family focused perinatal mental health provision have been limited.
In England, specialized perinatal mental health teams (PMHTs), which include occupational therapists, continue to be commissioned exclusively to support mothers. Fathers are typically offered only a carer’s assessment and signposting to external services (NHS, 2019). Consequently, fathers whose partners are not receiving perinatal mental health care, as well as fathers who do not identify as carers, are unable to access support. This structure means that existing services for fathers function primarily to indirectly support maternal wellbeing rather than addressing fathers’ needs in their own right (Hodgson et al., 2021).
Within occupational therapy, health and wellbeing are understood as intrinsically linked to engagement in meaningful occupations (Wilcock, 1998). During the transition to parenthood, this engagement can be substantially disrupted as new parenting occupations become integrated into fathers’ existing roles and daily routines. Although occupational therapy research has explored maternal experiences, far less attention has been paid to fatherhood. Recent scholarship suggests this is an important gap and highlights the need for further investigation into paternal experiences from an occupational perspective (Lim et al., 2022).
Literature review
A growing body of health-related research has examined new fathers’ wellbeing and their experiences of healthcare support during the perinatal period, which starts at the point of pregnancy (antenatal stage) and extends after the birth (post-natal stage). Poh et al. (2015), in an integrative review of men’s needs during pregnancy and childbirth, identified the antenatal period as characterized by mixed emotions and a clear need for additional support. Systematic reviews by Baldwin et al. (2018) and Genesoni and Tallandini (2009) further suggest that the postnatal period is psychologically the most challenging for fathers.
Qualitative studies provide deeper insight into these experiences. Baldwin et al. (2019) and Kowlessar et al. (2015), both recruiting fathers through UK NHS antenatal services, found that the stresses of new fatherhood could evoke feelings of helplessness and psychological distress, and in some cases contribute to the emergence of mental ill health. Similarly, Darwin et al. (2017) reported that returning to work shortly after birth generated feelings of disconnection for many fathers. Philpot et al. (2017), in a systematic review, identified several factors contributing to paternal stress, including role restrictions associated with becoming a father and feelings of incompetence regarding infant care.
Several studies have also highlighted a lack of father specific support within existing perinatal services. Poor communication from healthcare professionals, inadequate inclusion in antenatal education, and services perceived as inaccessible or not father-friendly are consistent themes across research (Baldwin et al., 2019; Darwin et al., 2017; Hodgson et al., 2021; Kowlessar et al., 2015). Fathers also commonly report reluctance to seek help, partly due to concerns that doing so might detract attention from their partner’s needs (Baldwin et al., 2019; Darwin et al., 2017). Relationship dynamics during the transition to parenthood have additionally been examined. Kluwer’s (2010) review found considerable variability, with some couples experiencing strengthened relationships while others reported increased strain. In seeking support, some fathers turn to online peer communities. Niela-Vilan et al.’s (2014) synthesis of 38 studies, five of which were father-specific, concluded that online peer support can be beneficial but should complement, rather than replace, face-to-face professional intervention.
Within occupational therapy, research focused explicitly on fatherhood remains limited. White and Jarvis (2024), in a synthesis of seven qualitative studies exploring paternal experiences in the first postnatal year, found only two high-quality studies (Baldwin et al., 2019; Darwin et al., 2017), both discussed in the present review. Although the included studies were not discipline-specific, the analysis adopted an occupational therapy lens. The authors concluded that new fatherhood disrupts engagement in previously established occupations, creating challenges that can affect wellbeing and necessitate personal adjustment. They suggest that occupational therapists may play an important role in supporting fathers during the antenatal and postnatal periods.
Other discipline-specific work includes Hamilton and DeJonge’s (2010) interviews with four fathers of infants aged 9–12 months, which examined changes to paternal roles. Participants valued their worker role and typically did not modify it following the birth. Many reported feeling unprepared for fatherhood, and because their parenting role was initially limited, they developed parenting skills more slowly than mothers. However, as infants grew older, fathers felt increasingly able to participate in parenting activities such as collecting children from nursery or engaging in play.
Research on occupational therapy practice more broadly reveals further gaps. Hackett and Cook (2016) found that occupational therapists in UK community mental health teams often provide counselling interventions to parents, an approach that Lim et al. (2022) suggest may stem from a lack of occupational therapy-specific literature regarding parenting. Their scoping review developed a conceptual framework for the “doing” of parenting occupations but revealed that most literature adopts a micro-level focus on discrete parenting tasks. Only five texts pertained specifically to fathers, and these concentrated on individual occupations, father–child interactions, experiences of separation, or the impact of disability. Lim et al. (2022) argue that there is substantial scope for occupational therapy to support the development of parenting skills and engagement in parenting occupations, while emphasising the need for further research exploring fathers’ experiences in a holistic and comprehensive manner.
Although these studies highlight that the transition to parenthood can affect fathers’ roles and, consequently, their occupational engagement, a significant gap remains regarding fathers’ detailed perspectives on how this major life transition influences their engagement in occupations (Crider et al., 2015). Given that occupational therapists conceptualize health and wellbeing as transactionally related to engagement in meaningful occupations (Wilcock, 1998), understanding changes in paternal occupational engagement during the perinatal period is essential. Such knowledge will be crucial for informing evidence-based services for fathers experiencing mental ill health, particularly if perinatal mental health provision is extended to include the whole family (Health Education England, 2018; Public Health England, 2019). It would also be valuable in other healthcare and community settings where new fathers are encountered.
While occupational engagement has been explored extensively among new mothers, who report constraints on meaningful occupations and disruptions to social connections that negatively affect wellbeing (Horne et al., 2005), fathers’ occupational experiences remain unexplored and may differ due to distinct occupational demands and role expectations. This study therefore aims to explore first-time fathers’ experience of changes to their occupational engagement during the perinatal period.
Method
The study was ethically approved by York St. John University Research Ethics Committee (Ethics Reference: BELL/MESA/26/04/2023).
Research design
This qualitative exploratory study was informed by an interpretivist paradigm and employed a phenomenological approach. Reflexivity, including explicit consideration of researcher subjectivity and potential bias, is central to qualitative analysis (Braun and Clarke, 2022). In this study, both researchers were female and did not have personal experience of fatherhood. The first author was not a parent but had previous professional experience within a perinatal service. To support reflexive practice, they maintained a reflective diary throughout data collection and analysis. Regular reflexive discussions were also held with the second author, who is a parent, to critically examine emerging interpretations and minimize potential bias.
Sampling and recruitment
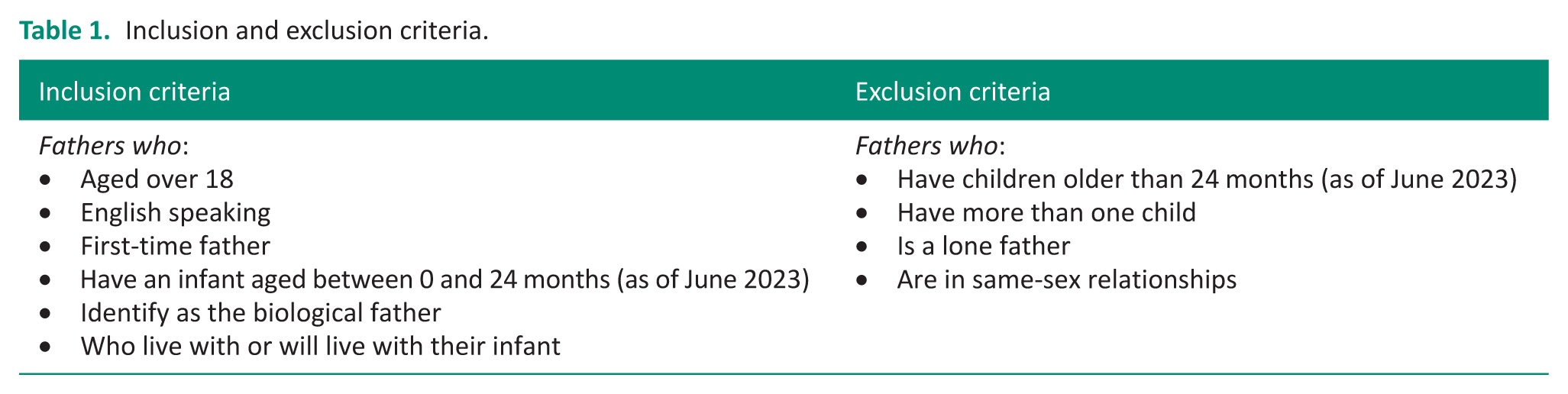
Chairpersons of three father support groups, identified through Google searching and social media and all located in the North of England, acted as gatekeepers to facilitate purposive recruitment of new fathers. Inclusion criteria is outlined in Table 1. Eligible participants were required to be English speaking, identify as the biological father, and reside with their first child, who was aged up to 24 months. This upper age limit aligns with the extended period during which NHS perinatal services are available in the United Kingdom (NHS, 2019). To enhance diversity within the sample, additional recruitment was undertaken through social media using a snowballing approach. Fathers in the antenatal period were excluded, as the study aimed to explore experiences of the transition to parenthood by examining occupational engagement both antenatally and postnatally. Fathers not living with their infant, fathers in same-sex relationships, and lone fathers were also excluded, as their experiences were expected to differ considerably from those of the target population.
Of the 19 fathers who initially responded to the advertisement and were provided with an information sheet and consent form, six first-time fathers met the inclusion criteria and consented to participate within the timeframe available for the study.
Inclusion and exclusion criteria.
Data collection
Semi structured interviews were used, and interview questions were developed following a review of relevant literature on mothers’ occupational engagement (Horne et al., 2005). The interview guide was piloted by the first author, with two parents, and minor revisions made based on their feedback. The interviews explored fathers’ patterns of occupational engagement before and after the transition to fatherhood, their experiences of changes to these patterns, and the types of support they had accessed or would have found beneficial during this transition. Participants were offered a choice between an online or in-person interview; all elected to be interviewed online. At the beginning of each interview, the concept of “occupation” was defined as anything you need to do, want to do, or are expected to do (WFOT, 2012) to ensure shared understanding. All interviews were audio and video recorded using Microsoft Teams. Interviews were transcribed verbatim, with all identifying information removed during the transcription process. Audio and video recordings were destroyed following transcription. Transcripts were then returned to participants for member checking to verify accuracy.
Data analysis
Inductive thematic analysis, guided by Braun and Clarke’s (2022) six step approach, was conducted by the first author. This analytic framework enabled a detailed exploration of the meaning underpinning fathers’ lived experiences and supported the identification of socially constructed connections within their patterns of occupational engagement across the perinatal period.
The analysis began with repeated review of the audio recordings alongside iterative reading of the interview transcripts, during which initial observations and reflections were noted. Each transcript was coded independently, and preliminary codes were compared across transcripts and consolidated where overlap occurred. All data segments relevant to each code were collated, supporting the development of initial themes and subthemes. These were subsequently refined through an iterative process in which some themes were combined, reorganized, or discarded if insufficiently supported by the dataset. Ongoing rereading of the transcripts ensured that the thematic structure accurately represented the breadth and depth of the data. Final theme names and working definitions were then generated, and illustrative extracts were selected to demonstrate each theme.
To enhance rigor, the second author reviewed the final themes and associated data extracts against the original transcripts. Following collaborative discussion, several final refinements were made to strengthen coherence and analytic credibility.
Findings
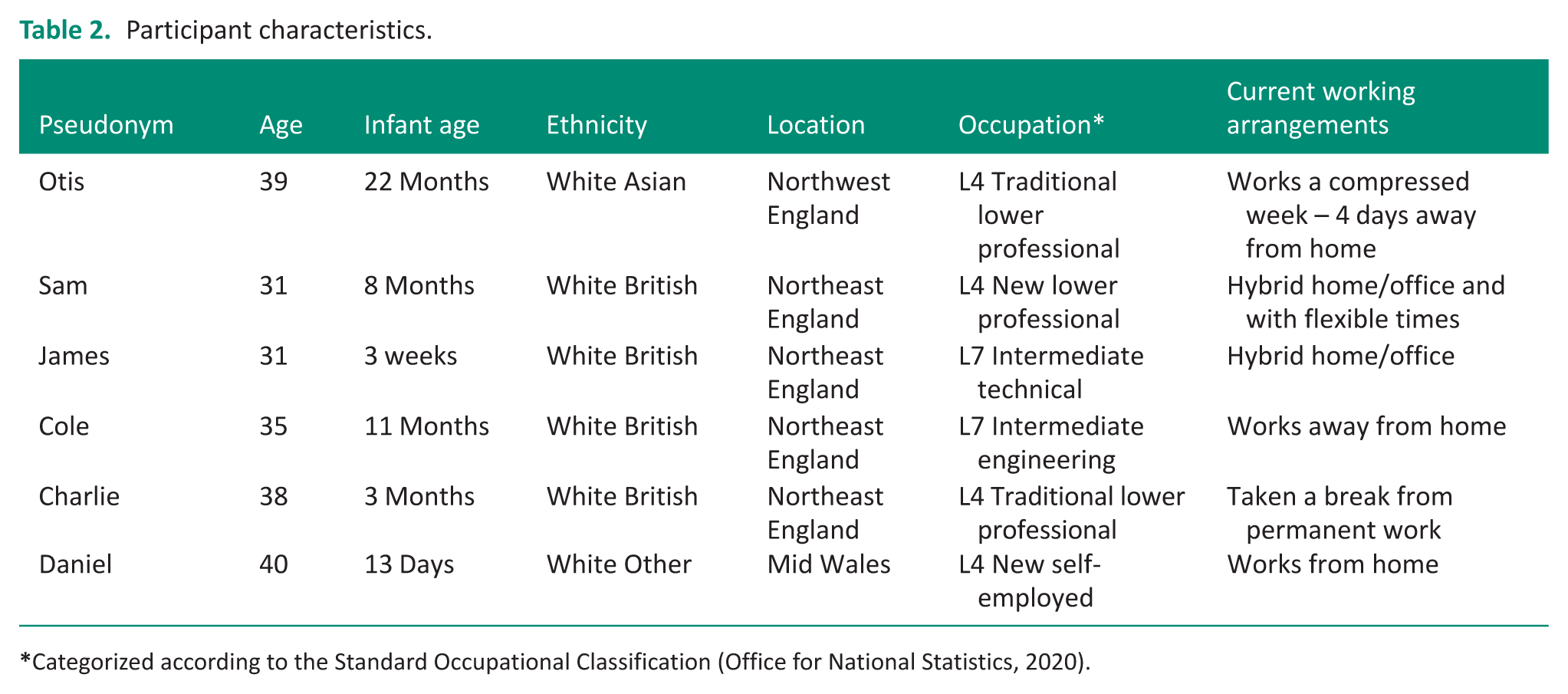
Six fathers were recruited for the study: two via a father support group gatekeeper and four through social media posts. Demographic information for participants is presented in Table 2, using pseudonyms, which are used throughout this article. The mean interview duration was 29 minutes. Data analysis generated three overarching themes, each comprising several subthemes, which are presented visually in Figure 1.
Participant characteristics.
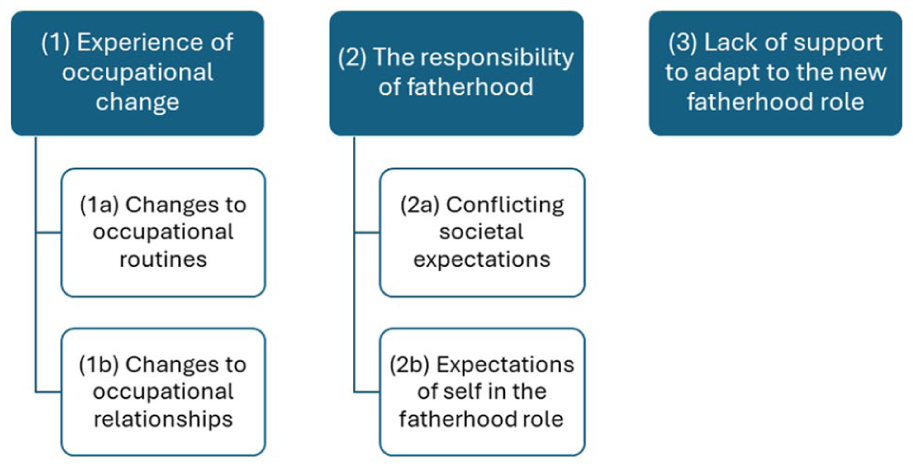
Thematic map.
Theme 1: Experience of occupational change
Father reported substantial changes to their occupational engagement across the perinatal period, describing alterations to both their occupational routines (Sub theme 1a) and to their relationships (Sub theme 1b).
(1a) Changes to occupational routines
Across their transition to parenthood, fathers described significant disruptions to established daily routines as they assumed practical caregiving occupations alongside their partners. These occupations included feeding, dressing, bathing, changing their infant, supporting sleep routines, and engaging in play. Some fathers benefitted from flexible or home-based work arrangements that enabled greater involvement in these parenting tasks. Others, such as Sam, who worked away from home, discussed the need for stricter boundaries around work time to facilitate caregiving: “I try and like, have a pretty much like a hard stop at 5:00pm.”
Certain early caregiving tasks, such as feeding when partners were breastfeeding, were inaccessible to some fathers and occasionally generated feelings of incompetence. To compensate, fathers often assumed responsibility for specific caregiving tasks, which fostered a sense of autonomy and involvement: I've sort of taken on bathtime as my responsibility so that we have that kind of time once or twice a week together just so I’ve got a little bit of kind of some autonomy with parts of kind of looking after him. (Charlie)
Fathers also noted increased responsibility for domestic tasks, motivated by a desire to support their partners: “to give [her] a rest” (Charlie). Many described a reprioritisation of values, with personal needs being deprioritized. As James stated: “I’m third on the list of priorities,” while Otis similarly reflected: “you do really restrict your own needs.”
This reprioritization often meant personal and leisure occupations were reduced or paused and infant centered occupations were given precedence: I’ve not gone to the gym like literally at all. [. . .] Definitely prioritising more, I say for her, but at the same time I feel like it’s for me as well, I like spending time with her [. . .] if I did really want to go to the gym, I would make it work, but I know I would be sacrificing, like, either time with her, or sacrificing like that evening time with my wife. (Sam) You used to revolve your life around the stuff you wanted to do, but now you have to revolve it around her. (Cole)
Although these shifts disrupted previously established routines, many fathers perceived their new parenting occupations as enhancing their wellbeing: Things that I do to improve my wellbeing and mood is spending time with my daughter. (James) Seeing him develop and grow and change, I think that’s been amazing for wellbeing. (Charlie)
Others were however mindful of the importance of maintaining previously valued occupations to preserve wellbeing, “otherwise you go mad” (Cole). This however required “a lot more logistics around planning” (Sam), which could be difficult as they responded to the rapidly changing needs of their infant: We are trying to be good and find things that are important to us [. . .] it’s difficult isn’t it because we don’t know what he’s [infant] gonna be like in five minutes. (Charlie)
Whilst the ever-changing routines related to their infants evolving needs could be difficult to navigate, planning the changes and slowly adapting to them together, was an effective way of managing: We’ve got a bit more of a plan going into the night, so things have gotten a bit better [. . .] we’re just slowly trying to enter into our new routines. (James)
For some participants, however, the time spent engaging in new parenting occupations had a knock-on effect on the time available for other meaningful occupations, with consequent implications for wellbeing. Sam, for example, described no longer having time for his daily walk and noted that this loss negatively affected his productivity at work. Otis similarly reflected on the wellbeing impact of becoming more restricted in his occupational choices: Now it’s very different, it’s not spontaneous, we use to do a lot of random stuff but it’s not spontaneous at all now [. . .] having those routines with my writing and reading and going to gigs with my partner is preventative [of poor mental health]. It gets me down [. . .] the relentlessness, the sort of always knowing what’s coming. (Otis)
Charlie discussed the challenge of juggling the demands of his work role and his fatherhood role: For the first year particularly, I had to take quite a bit of time off work. . . just cause the balance and she wasn’t sleeping at all, then, the little one, she is better now, but the challenge of not sleeping, erm, and, trying to do my job, at the time, again, I’ve moved jobs. . .I couldn't cope with it at the time, so I’d say that time off work actually led to me deciding that I needed to get out of that line of work if I wanted to be the dad I wanted to be.
(1b) Changes to occupational relationships
Fathers discussed the ways in which their relationships changed as they transitioned into fatherhood. Many described changes with their partners, and that the adjustment brought both challenges and opportunities for growth. While some experienced strain during this period, fathers also highlighted how shared responsibilities and increased time together contributed to deeper connection.
As Daniel reflected: “It’s brought my wife and I even closer together, I think we kind of respect and love each other even more.” Otis, described a mixture of difficulties and positive developments, noting that parenthood required greater relational collaboration: “Our relationship changed in some difficult ways and in some really good ways [. . .] we have to be more connected now [. . .] we were often living together but in our own world a lot of the time, so that’s been positive.” Similarly, James emphasized the importance of teamwork: “The main thing is learning to work with my partner, so we can give each other a break.”
Fathers also discussed notable changes in their friendships during the transition to fatherhood. Many described reduced availability as a key factor, with competing demands of work and parenting limiting opportunities for social connection. As Sam explained, “That challenge of keeping up to date and feeling involved in their [friends’] lives and activities they’re doing has definitely proved a big challenge.”
For some, such as Otis, becoming a father altered the basis of connection with friends who did not have children. He reflected on a growing sense of divergence, noting that certain friendships faded as priorities shifted: Friendships have sort of withered away [. . .] some friends aren’t really that interested once you’ve got a kid [. . .] they want to do the things that you still did prior to having a kid; they don’t want to do the new things that involve the kid.
Otis simultaneously described a strengthened relationship with friends who were parents, highlighting how shared experience fostered connection: the people that I know who have got kids, some of those friendships have really grown and changed [. . .] I’ve kind of got a new respect for parents now.
Theme 2: The responsibility of fatherhood
Fathers described tensions between evolving societal expectations of fatherhood (Subtheme 2a) and their internal expectations of themselves in the fatherhood role (Subtheme 2b).
(2a) Conflicting societal expectations
Fathers discussed the changing sociocultural expectations in which they are expected to be more involved in childcare: There’s a much greater expectation that dads will be more involved [. . .]. There are psychological challenges and that kind of feeling of pressure to be more than just like a typical dad cause a typical dad now is very different to how it was in, you know, previous generations. (Charlie)
This shift toward expectations of active caregiving often sat alongside enduring norms positioning fathers as primary financial providers. Some highlighted how UK parental leave policy reinforces these traditional role expectations, requiring fathers to return to work quickly after birth, which some described as emotionally challenging. Charlie reflected: [Dads] have to go back to work [. . .] and feeling sad and they were left out, they weren't really part of things because they couldn’t do the same things as the mum. But also, a little bit of jealousy, and not quite have that bond, the same bond, and difficult, potentially really negative, really harmful emotions to experience.
Similarly, Otis critiqued the gendered assumptions embedded in this policy: The whole system is stuck in the past about the dad’s meant to be the breadwinner and the mums meant to be the carer [. . .] even like paternity leave [. . .] it just means the mum has to do all these things on their own and the dad gets made to feel like they’re outside of it all [. . .] its very stuck in gender roles.
Fathers whose work arrangements allowed flexible hours, home-working, or unpaid leave described feeling fortunate to have greater involvement in early caregiving. As Charlie expressed: I have this extra bit of time to be at home and help out and kind of be part of things. I think if I had to go back to work after two weeks, you know. . .that would be really difficult, cause I’d feel really, I’d feel really guilty, but also I’d feel quite left out I think.
(2b) Expectations of self in the fatherhood role
Fathers reported positive feelings of personal responsibility that accompanied fatherhood, in relation to providing for their child and being a positive role model. This new sense of responsibility often reshaped meaning previously assigned to everyday occupations. Charlie reflected on this shift: Having such great responsibility [. . .] it did make me look at my life a little more because he [infant] needs me to look after myself so I can look after him.
For some this changed the nature of their motivation for occupations: I’m more motivated to do things like that [health and fitness] cause I don’t want her to like grow up, you know, not valuing those. (Sam) I am more motivated to do that [writing] now that I have a child to support as well, which makes it something I’m more interested in doing. (Daniel)
Despite these positive shifts, several fathers discussed the perception that their role was sometimes viewed as less important or less central than the mother’s. This contributed to internal conflict and inhibited openness about their experiences: Socially as men our duty is to act [. . .]. As a man you don’t have a job to do [at birth of infant] and that’s quite a challenging thing to get your head round [. . .], so it was sort of an experience of emasculating, but in a good way. (Daniel) People think dads aren’t as involved a lot of the time anyway, dads don’t care as much, and it felt like sometimes for me [. . .] if I was to admit that there were days when I didn’t wanna be a dad [. . .] people would judge that. (Otis)
Theme 3: Lack of support to adapt to the new fatherhood role
Fathers consistently reported that available support services were directed primarily toward mothers and did not address fathers’ distinct needs or experiences. Many described feeling overlooked by both professionals and wider support systems. As Cole summarized: “The help and support would be easier to get if you were a mum.”
Several fathers noted that their own wellbeing was rarely enquired about, with Otis reflecting: “Nobody asked how I was.” Fathers also highlighted that antenatal education focused heavily on supporting mothers, offering limited guidance on how fathers could prepare themselves. Daniel described: Information around parenthood is geared at women [. . .] men have different fears, different experiences, different concerns, different needs’. (Daniel)
Many fathers reported feeling unprepared for their new role and described learning primarily through experience. This lack of preparation drew attention to the insufficiency of father-specific support during the transition into their new role. Otis reflected: I didn’t have no idea what it’s like becoming a parent [. . .] it’s just made me realise how much support is lacking [. . .] particularly for dads [. . .] so we found our own way of figuring things out.
Daniel echoed this, noting that he and his partner “had to do a heck of a lot of our own research [. . .] because official available information is really limited and quite poor quality.”
Some fathers sought alternative resources, such as books and podcasts, to support their development in the role: I've read a book ....that was kind of aimed at Dad's and written in a really nice kind of way, and I listened to a podcast which was written by two journalists, like about kind of some of the issues and stuff that they face and some of the challenges that they experience, which was, which was helpful. (Charllie)
They also emphasized that more meaningful support would include opportunities for connection with other fathers. Sam suggested the value of: “groups [. . .] where dads can get together and just [. . .] talk through what’s going on with them that week,” while Daniel highlighted the need for “a community where men can talk about [. . .] the things that may be scary about becoming a father.”
Discussion
This study explored first-time fathers’ perceptions of their patterns of occupational engagement during the perinatal period as they transitioned into parenthood. Fathers reported that this period brought about substantial occupational change, with routines associated with previously valued occupations disrupted and re-prioritized, while new parenting occupations were integrated into daily life. Overall, participants described feeling under prepared for their new role and the unfamiliar occupations that accompanied it, and consistent with other research, often relying on trial and error to develop competence (Baldwin et al., 2019; Darwin et al., 2017; Hamilton and DeJonge, 2010).
Echoing wider health research, fathers perceived antenatal and postnatal services as predominantly mother-focused (Baldwin et al., 2019; Darwin et al., 2017; Hodgson et al., 2021; Kowlessar et al., 2015), and felt that their own needs were insufficiently recognized. Given that occupational therapy can support the development of parenting skills (Lim et al., 2022) and assist individuals in navigating major life transitions and the occupations associated with them (Crider et al., 2015), these findings align with recommendations by White and Jarvis (2024), who argue that occupational therapists may be well placed within antenatal care to prepare new fathers for their emerging roles and the practical demands they entail.
Despite initial feelings of being unprepared, fathers reported active involvement in many parenting occupations identified by Lim et al. (2022), including attending to basic care needs, communicating with their child, and providing emotional support and stability. Most participants engaged in these occupations alongside their existing work roles. This contrasts with the findings of Hamilton and DeJonge (2010), who observed that fathers tended to participate in only a limited number of child-related occupations during the early transition phase, becoming more involved as their child grew older, particularly in play-related occupations. Given that Hamilton and DeJonge’s study was conducted over a decade ago, this divergence may reflect documented shifts in societal expectations surrounding fatherhood (Letourneau et al., 2012; Yogman and Eppel, 2022), with contemporary fathers experiencing stronger cultural expectations to be involved, emotionally attuned, and hands-on from the earliest stages of parenthood.
Fathers identified these societal expectations as sitting uneasily alongside the expectation that they continue to fulfil the breadwinner role. This tension is reinforced by UK paternity leave policy, which typically requires fathers to return to work after only two weeks of leave. Participants described challenges in negotiating the demands of both roles, and for some, this had a detrimental impact on their wellbeing. They also reported that individuals within their social networks seldom inquired about their wellbeing, suggesting that despite increasing societal expectations of father involvement, an implicit assumption persists that fatherhood does not affect men’s mental health. This assumption may contribute to the well-documented under-reporting of mental ill health among fathers (Fisher et al., 2021). Fathers additionally described feelings of “sadness,” “jealousy,” and a general sense of exclusion from family life when work required them to be physically absent from the home. For those with access to flexible working arrangements or the ability to work from home, greater involvement in parenting occupations and partner support fostered positive wellbeing.
These findings reinforce the argument for increased flexibility in working practices for new fathers as a means of supporting both parents to manage the transition into parenting roles. Given the strong associations reported between paternal and maternal mental ill health, and between parental mental health and child development (Department of Health and Social Care, 2021; Philpott, 2022; Ramchandani et al., 2005, 2008), supporting fathers’ wellbeing is likely to have benefits for the whole family. Trade Union Congress (2023) research indicates, however, that many fathers are unaware of their right to request flexible working or avoid doing so due to fears regarding their employer’s response; of those who do request flexibility, 54% of applications are rejected, with higher rates of refusal occurring among those in lower-paid employment.
Although none of the fathers in this study were in lower-paid jobs, one participant described working in a professional role where flexibility was unavailable. He reported considerable difficulty balancing work with his new parenting responsibilities, culminating in a period of sickness absence due to mental ill health. He subsequently moved to more flexible employment. While not directly related to flexible working, Heshmati et al’s. (2023) systematic review exploring parental leave and paternal mental health found the evidence base to be inconclusive compared with clear associations identified for mothers, but noted substantial methodological limitations. Taken together, these findings indicate that the relationship between job flexibility and paternal wellbeing warrants further investigation.
When not at work, fathers reported consciously prioritizing occupations related to caring for their child over previously valued leisure occupations, a pattern also observed in studies of new mothers (Horne et al., 2005). They described feeling both responsible for participating in parenting occupations and intrinsically motivated to “be with” their infant and partner, not wanting to miss important moments in early family life, consistent with Baldwin et al. (2019). This motivation to “do” for, or alongside, their infant and partner aligns with the concept of co-occupation, involving shared meaning, emotionality, physicality, and intentionality (Bonsall, 2014; Pickens and Pizur-Barnekow, 2009).
Existing literature highlights the importance of parent–child co-occupations in fostering the attachment bond (Whitcomb, 2012), and fathers in this study described a transactional relationship between their wellbeing and that of their child. This was particularly notable when fathers had assumed specific caregiving responsibilities. With regard to their partners, although some fathers acknowledged challenges, most described the co-occupation of parenting, and the shared problem-solving and mutual support it required, as strengthening their relationship and enhancing their sense of connection (Baldwin et al., 2019; Kluwer, 2010).
Despite willingly compromising previously valued occupations in favor of parenting ones, fathers reported that this shift affected their wellbeing. They described feelings of incompetence in their new role, reduced spontaneity in occupational choice, and the “relentlessness” of new parenting occupations, which rapidly evolved as their child developed. These effects were reported by fathers with infants up to 22 months old, suggesting that wellbeing can be affected beyond the immediate transition phase, even within a seemingly healthy population. This finding supports current UK policy extending perinatal mental health service eligibility to 24 months postpartum (NHS, 2019).
Where fathers were able to maintain engagement in previously meaningful occupations, many described a shift in the meaning attributed to them. They reported being more motivated to engage in occupations they perceived as indirectly benefiting their child, for example, by modeling positive behavior or supporting family financial stability. They also reported changes in the meaning and importance of friendships. Some friendships became more difficult to maintain, as peers without children continued social and leisure occupations that fathers had deprioritized. This echoes findings in research with new mothers (Horne et al., 2005). Fathers reported placing greater emphasis on friendships with other parents with whom they shared lived experience.
Fathers found learning about other fathers’ experiences reassuring, often through books or podcasts, and many expressed a desire for face-to-face, father-specific support groups. Research with mothers demonstrates that peer-support relationships, such as those formed at mother-and-baby groups, are protective for mental health as they reduce isolation, stress, and enhance confidence in parenting (McLeish and Redshaw, 2015). Although two fathers in this study were recruited through father-support group networks, neither described accessing such groups themselves.
White and Jarvis (2024) suggest that occupational therapists could offer follow-up support to fathers in the postnatal period to help them adapt to their new roles alongside ongoing work responsibilities, potentially outside standard working hours. While the present study supports the need for this type of intervention, careful consideration is required regarding timing and accessibility, particularly given that participants reported prioritizing parenting responsibilities during time outside work, often at the expense of occupations supporting their own wellbeing. An additional recommendation, therefore, is that UK work policy could be adapted to allow fathers protected time within the working week to access postnatal support, thereby safeguarding their time with their new family unit.
Strengths and limitations
The strength of this study lies in the depth and richness of the qualitative data generated regarding fathers’ experiences of changes in occupational engagement across the perinatal period. Notably, this depth was achieved despite relatively short interview durations, which largely reflected the contextual constraints of new fatherhood, with interviews often conducted during work lunch breaks or while participants were simultaneously providing infant care. This context underscores the very occupational challenges the study sought to explore.
Several limitations should be acknowledged. As a small-scale qualitative study, the sample size and demographic composition are not representative of the wider population of new fathers. No participants identified as belonging to an ethnic minority group, nor were fathers at the highest or lowest ends of the socioeconomic spectrum included. These factors may limit the transferability of the findings. The study focused specifically on first-time fathers in the UK who were residing with their child; consequently, the experiences of fathers in same-sex relationships, lone fathers, adoptive fathers, fathers of multiple children or newborns, and those in blended families remain unexplored. Future research could also examine paternal experiences across different cultural and geographical contexts. Investigating the experiences of fathers with health conditions or disabilities, or of those parenting children with additional needs, would further extend the scope of this work. Additionally, research exploring occupational therapists’ perspectives on the potential scope of perinatal support for fathers may provide valuable insights for service development.
A further limitation relates to the single time point at which data were collected. The ages of participants’ first children ranged from 13 days to 22 months, meaning that some fathers reflected on the transition as it was unfolding, whereas others described their experiences retrospectively. All participants were aged between 31 and 41 years, which may not capture the perspectives of younger or older fathers. Future longitudinal research following fathers from the antenatal period into the postnatal period, or across subsequent transition points, such as a partner’s return to work, or a child’s entry into nursery or school, would support deeper understanding of how occupational engagement continues to evolve over time.
Conclusion
This study provides new insights into first-time fathers’ experiences of occupational engagement during the perinatal period and highlights the complex interplay between managing emerging parenting occupations, sustaining existing ones, navigating work commitments, and responding to evolving societal expectations of fatherhood. Fathers described significant occupational disruption and reprioritization, frequently reporting that they felt unprepared for the practical and emotional demands of their new role. While many embraced active involvement in caregiving and experienced strengthened relationships with their partner and child, tensions arising from limited paternity leave, inflexible work arrangements, and the absence of father-specific support contributed to feelings of stress, exclusion, and decreased wellbeing.
These findings reinforce the need for greater recognition of fathers’ occupational needs within perinatal services, which remain predominantly mother-focused. Occupational therapists are well positioned to address this gap by offering antenatal and postnatal interventions that support fathers to develop parenting skills, negotiate new routines, and integrate parenting occupations alongside existing roles. The study also highlights the importance of wider structural support, including enhanced workplace flexibility and opportunities for peer connection, both of which appear central to supporting fathers’ wellbeing during the transition to parenthood.
Overall, the study strengthens the argument that fatherhood is an occupational transition warranting attention within occupational therapy practice, research, and policy. Ensuring that fathers are adequately supported not only benefits paternal wellbeing but also has the potential to enhance family functioning. Future research should continue to examine the relationship between occupational engagement, work flexibility, and paternal mental health, and explore how occupational therapy can best contribute to inclusive, family centered perinatal care.
Key findings
Fatherhood involves substantial disruption and reprioritization of occupational roles and routines.
Fathers experience tension in managing their occupational roles, positioned between the evolving societal ideal of the engaged, hands-on father and long-standing expectations of fulfilling the traditional breadwinner role.
Fathers feel unprepared and underserved by existing perinatal support, expressing a need for father-specific resources and peer connection.
What this study had added
This study adds new insight into how fathers experience significant shifts in occupational roles and routines, manage tensions between modern and traditional role expectations of fatherhood, and experience gaps in support that hinder their adaptation to this role.
Footnotes
Funding
The authors declared no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Patient and public involvement data
During the development, progress, and reporting of the submitted research, Patient and Public Involvement in the research was not included at any stage of the research.