
Abstract
Introduction:
This scoping review aimed to identify and synthesize the occupational therapy (OT) interventions for return to work after acquired brain injury.
Methods:
A comprehensive search was conducted across four electronic databases (PubMed, Scopus, Web of Science, and OTsekeer) up to November 2025. The review followed the PRISMA-ScR guidelines. Methodological quality was appraised using the Oxford Center for Evidence-Based Medicine classification. The protocol was prospectively registered on the Open Science Framework (available at https://doi.org/10.17605/OSF.IO/SU8Z3).
Results:
A total of 1341 records were identified, of which seven randomized controlled trials met the inclusion criteria. The studies evaluated interventions such as early stroke specialist vocational rehabilitation, which integrates functional performance assessment and employer coordination; RETurn to work After stroKE (RETAKE); and combined compensatory cognitive training and supported employment (CCT-SE), aimed at promoting return to competitive work after acquired brain injury.
Conclusions:
OT interventions support return to work after acquired brain injury, especially when they are initiated early, individualized, cognitively focused, and coordinated with employers.
Introduction
Acquired Brain Injury (ABI) is characterized as a sudden trauma to the brain that happens unexpectedly, leading to a wide range of consequences according to the location and severity of the injury (Martin et al., 2023). These consequences may influence perception, communication, and physical, cognitive, and emotional functioning (Goldman et al., 2022). The predominant causes of ABI encompass traumatic brain injury and stroke; nevertheless, tumors, anoxic events, and central nervous system infections also frequently contribute to its etiology (Fernández-Sánchez et al., 2022).
ABI is recognized as one of the most prevalent neurological disorders worldwide and is characterized by specific diagnostic criteria involving acute onset, objectively verifiable impairments, and substantial impact on quality of life, while excluding degenerative or hereditary conditions (Rodríguez et al., 2022). The incidence of ABI varies according to its etiology. Traumatic ABI occurs at an estimated rate of 200 cases per 100,000 population per year, with approximately 21% of cases leading to long-term disability. Non-traumatic ABI encompasses a more heterogeneous range of conditions, including cerebrovascular events with an incidence of roughly 190 cases per 100,000 individuals annually and disability rates reaching 44% as well as anoxic encephalopathy, primary brain tumors, and encephalitis, each associated with distinct clinical and public health implications (Rodríguez et al., 2023).
ABI-related consequences include neurological deficits that significantly impede functional capacity. Included are movement disorders like hemichorea and dystonia, impacting approximately 20% of individuals with acquired brain lesions (Tater and Pandey, 2021), as well as post-stroke spasticity, which exhibits a prevalence between 18% and 42% depending on the recovery phase (Rodríguez et al., 2023). Lesions in the left hemisphere can result in language deficits, including aphasia (Goldberg et al., 2021), while cognitive impairment is noted in approximately 43% of patients within the first-year post-neurological event, even among those without a history of dementia, with an additional 34% at heightened risk for cognitive deficits during the same timeframe (Alexandrova and Danovska, 2016). In this situation, rehabilitation is pivotal. Occupational therapists modify tasks and surroundings to meet individual requirements, fostering sensory control, emotional well-being, and early participation in meaningful activities during rehabilitation (Brown et al., 2023; Vásquez-Carrasco et al., 2024). Forming a secure and cooperative therapy connection is crucial, facilitating discourse that promotes shared decision-making and fosters personal empowerment.
Interventions that emphasize personal strengths and active participation form a core component of therapeutic practice (Brown et al., 2023; Vásquez-Carrasco et al., 2025). Throughout rehabilitation, occupational therapy (OT) is pivotal in fostering functional recovery and supporting reintegration into meaningful activities, including work-related roles (Vásquez-Carrasco et al., 2025). This involves implementing environmental modifications, providing targeted supports, and coordinating with workplace contexts to promote autonomy and sustainable return-to-work outcomes (Kurihara et al., 2024). Interventions encompass vocational support, interpersonal skills development, compensatory strategy training, and collaborative goal setting, all aimed at strengthening occupational identity and psychosocial well-being in individuals with ABI (La Torre et al., 2022).
Training in activities of daily living is a fundamental rehabilitative strategy that improves motor, cognitive, and behavioral abilities while promoting functional learning in real-world situations (Fernández Gómez et al., 2009; Vásquez-Carrasco et al., 2025). Consequently, occupational therapy is established as a vital discipline for holistic recovery and reintegration into daily responsibilities, including job, which is a crucial aspect of identity, economic stability, and social involvement. This comprehensive analysis sought to identify and synthesize occupational therapy strategies for reintegration into the workforce following acquired brain damage.
Methods
Protocol and registration
This scoping review adhered to the methodological standards of the Cochrane Collaboration (Higgins et al., 2023) and was reported in alignment with the PRISMA-ScR guidelines, incorporating the corresponding checklist and flow diagram (Tricco et al., 2018). The protocol was prospectively registered on the Open Science Framework (available at: https://doi.org/10.17605/OSF.IO/SU8Z3).
Eligibility criteria
This scoping review included peer-reviewed original research limited to randomized controlled trials (RCTs), without restrictions on language or publication date up to November 2025. Exclusion criteria encompassed non–peer-reviewed sources and non-RCT designs, including conference abstracts, books and book chapters, editorials, letters, protocols, reviews, case reports, and other non-randomized studies. Study selection followed the Population, Intervention, Comparator, Outcome, Study design (PICOS) framework, as summarized in Table 1.
Selection criteria used in the scoping review.
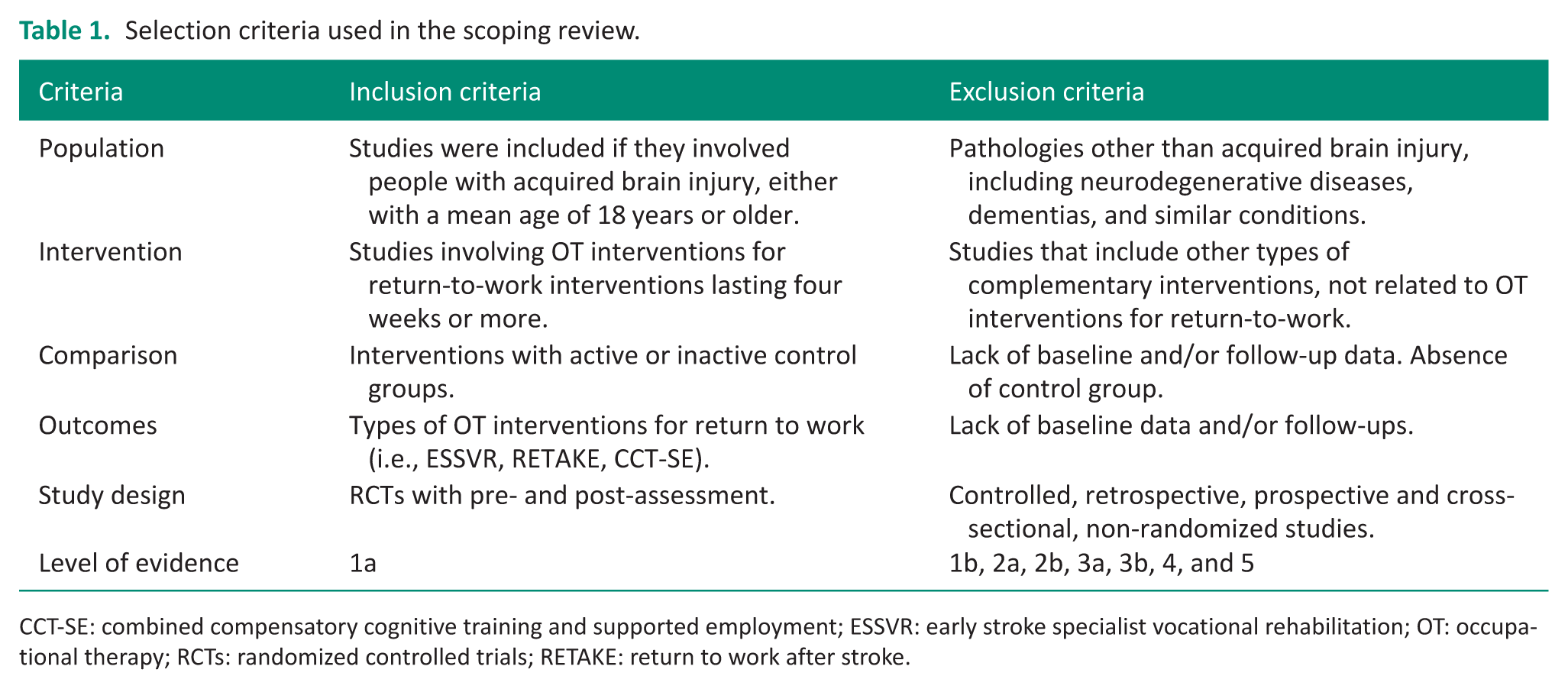
CCT-SE: combined compensatory cognitive training and supported employment; ESSVR: early stroke specialist vocational rehabilitation; OT: occupational therapy; RCTs: randomized controlled trials; RETAKE: return to work after stroke.
Information and database search process
An electronic search was performed across four databases: Scopus, Web of Science (Core Collection), MEDLINE/PubMed, and OTseeker. Using a strategy that integrated Medical Subject Headings (MeSH) from the U.S. National Library of Medicine with relevant keywords describing OT interventions aimed at facilitating return to work after ABI: (“stroke” OR “stroke” OR “cerebrovascular accident” OR “cerebral infarction” OR “brain ischemia” OR “ischemic stroke” OR “hemorrhagic stroke” OR “cerebral hemorrhage” OR “acquired brain injury” OR “acquired brain damage” OR “brain injury” OR “traumatic brain injury” OR “traumatic brain injury” OR “non-traumatic brain injury” OR “anoxic brain injury” OR “hypoxic brain injury” OR “encephalitis”) AND (“return to work” OR “return to work” OR “work reintegration” OR “vocational rehabilitation” OR “job reintegration” OR “occupational reintegration” OR “workforce reentry” OR “employment outcomes”) AND (“middle aged” OR “middle-aged adults” OR “middle age” OR “working-age adults” OR “midlife adults”). Two independent experts evaluated the articles for eligibility based on the predefined inclusion and exclusion criteria. Both reviewers held a Ph.D. in health sciences and had published in Journal Citation Reports® indexed journals. To reduce bias, they were not given access to the search strategy. A final search was conducted on November 30, 2025, to identify any errata or retractions associated with the included studies.
Study selection and data collection process
All studies were imported into Zotero Reference Manager (Version 7.0.30, Roy Rosenzweig Center for History and New Media, George Mason University), and the selection process is depicted in the PRISMA flow diagram. Four researchers (M.M., V.O., K.R., and M.R.) and a field expert (E.V.-C.) independently screened the records. Duplicate entries were removed in Zotero. The screening proceeded in two stages: an initial review of titles and abstracts, followed by full-text evaluation based on the predefined inclusion criteria. Studies that met the eligibility criteria and achieved consensus among reviewers were included in the final analysis (Figure 1).
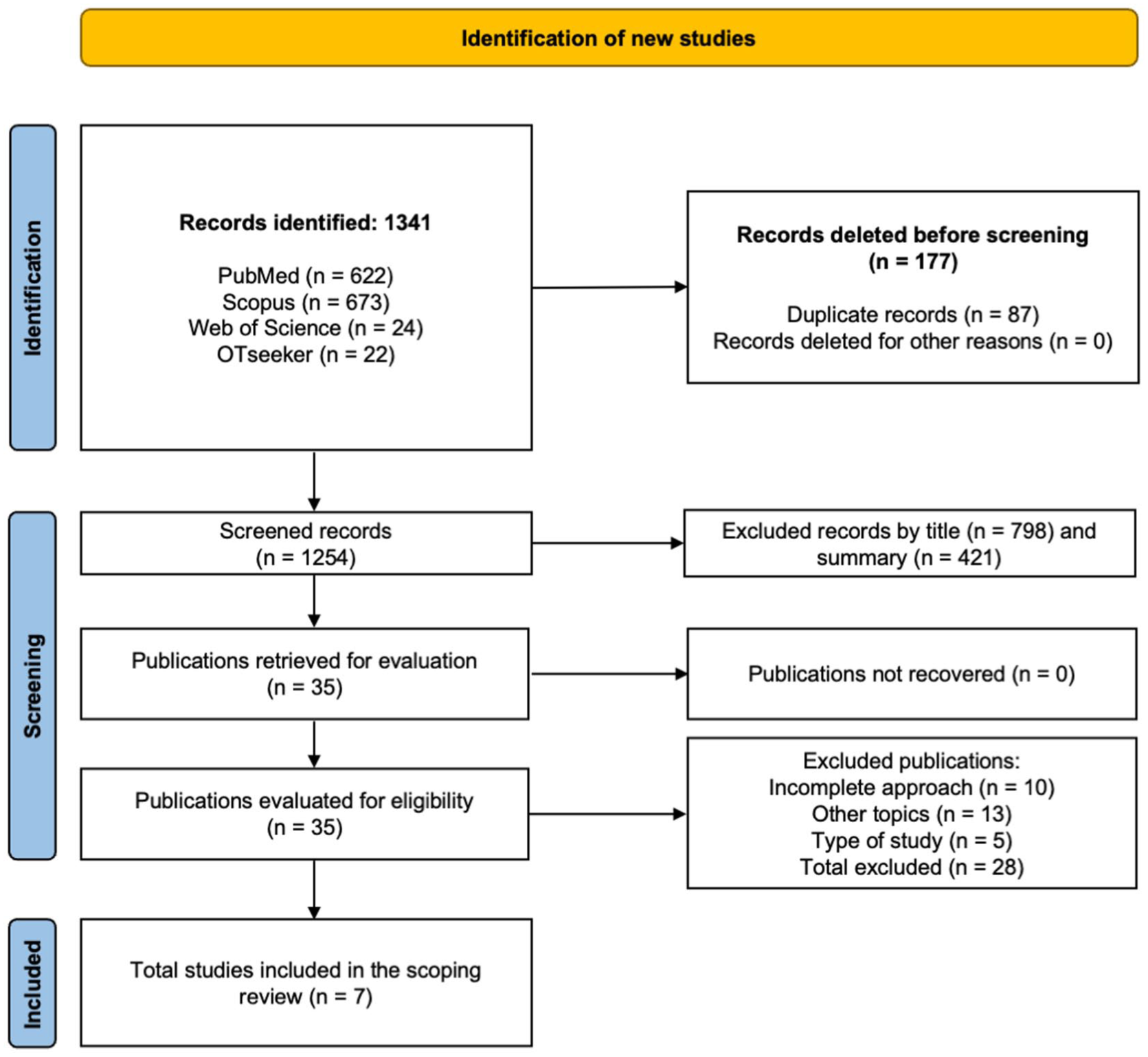
Flowchart of the scoping review (Page et al., 2021).
Methodological quality assessment
Methodological quality and evidence level were assessed using the Oxford Center for Evidence-Based Medicine criteria (Manterola and Zavando, 2009). Only Level 1a RCTs were included, while studies classified as levels 1b–5 were excluded. Trials were downgraded when issues related to bias, consistency, precision, or reporting transparency were identified.
Data synthesis
Data from the included studies were extracted into a standardized form using Microsoft Excel® (version 16.81; Microsoft Corporation, Redmond, WA, USA), following Cochrane methodological guidance (Higgins et al., 2023). Four reviewers (M.M., V.O., K.R., and M.R.) independently conducted the extraction and cross-checked the results for consistency. The extracted information included (i) author and year, (ii) country, (iii) study design, (iv) intervention components, (v) sample size per group, (vi) intervention characteristics, and (vii) outcome measures.
Results
Study selection
The database search yielded 1341 records, of which 87 were removed as duplicates. The remaining 1254 records underwent title and abstract screening, resulting in the exclusion of 1219 articles (798 based on title and 421 based on abstract relevance). Thirty-five full-text articles were assessed, and 28 were excluded for failing to meet the inclusion criteria, 10 due to insufficient methodological focus, 13 for addressing unrelated subject matter, and 5 for employing non-eligible study designs. Consequently, 7 studies met all criteria and were retained for the scoping review (Clarke et al., 2024; Craven et al., 2021; Fure et al., 2021; Pyne et al., 2024; Radford et al., 2018, 2024; Vikane et al., 2016).
Methodological quality
The methodological rigor of the studies included in this scoping review is considered high. All the investigations adopted RCT designs, ensuring a robust evidentiary foundation consistent with Level 1a standards of the Oxford Center for Evidence-Based Medicine (Clarke et al., 2024; Craven et al., 2021; Fure et al., 2021; Pyne et al., 2024; Radford et al., 2018, 2024; Vikane et al., 2016).
Characteristics of the studies
Seven RCTs were conducted in adult populations who had been employed prior to experiencing a stroke or traumatic brain injury. The study populations comprised individuals returning to work following stroke, adults with traumatic brain injury, and therapists involved in vocational rehabilitation. Participant ages ranged from 32 to 56.4 years. All the trials were conducted in two countries: the United Kingdom and Norway (Table 2).
Selected studies on occupational therapy interventions for return to work after acquired brain injury.
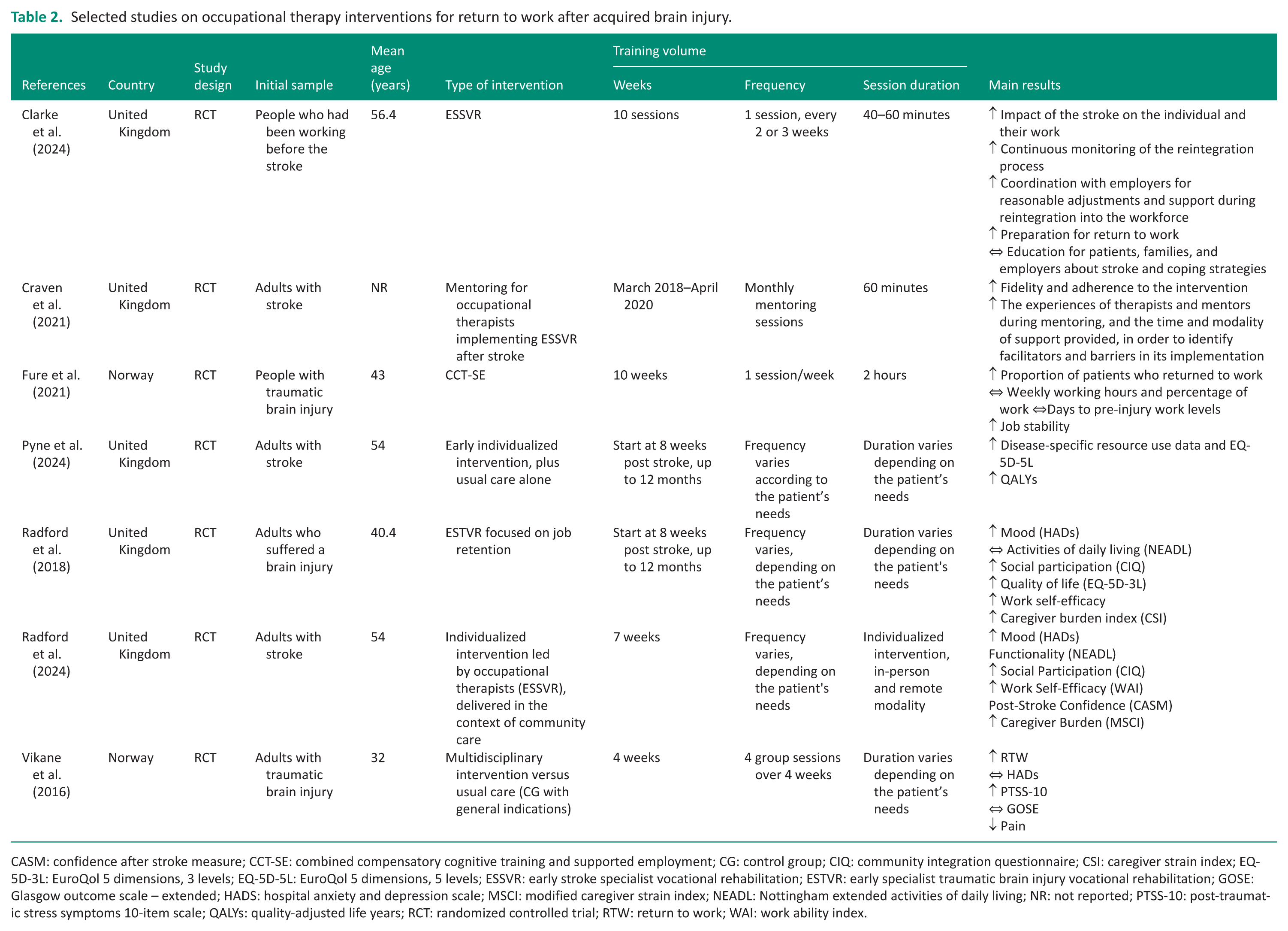
CASM: confidence after stroke measure; CCT-SE: combined compensatory cognitive training and supported employment; CG: control group; CIQ: community integration questionnaire; CSI: caregiver strain index; EQ-5D-3L: EuroQol 5 dimensions, 3 levels; EQ-5D-5L: EuroQol 5 dimensions, 5 levels; ESSVR: early stroke specialist vocational rehabilitation; ESTVR: early specialist traumatic brain injury vocational rehabilitation; GOSE: Glasgow outcome scale – extended; HADS: hospital anxiety and depression scale; MSCI: modified caregiver strain index; NEADL: Nottingham extended activities of daily living; NR: not reported; PTSS-10: post-traumatic stress symptoms 10-item scale; QALYs: quality-adjusted life years; RCT: randomized controlled trial; RTW: return to work; WAI: work ability index.
Overview of included studies and thematic mapping of occupational therapy interventions for return to work after acquired brain injury
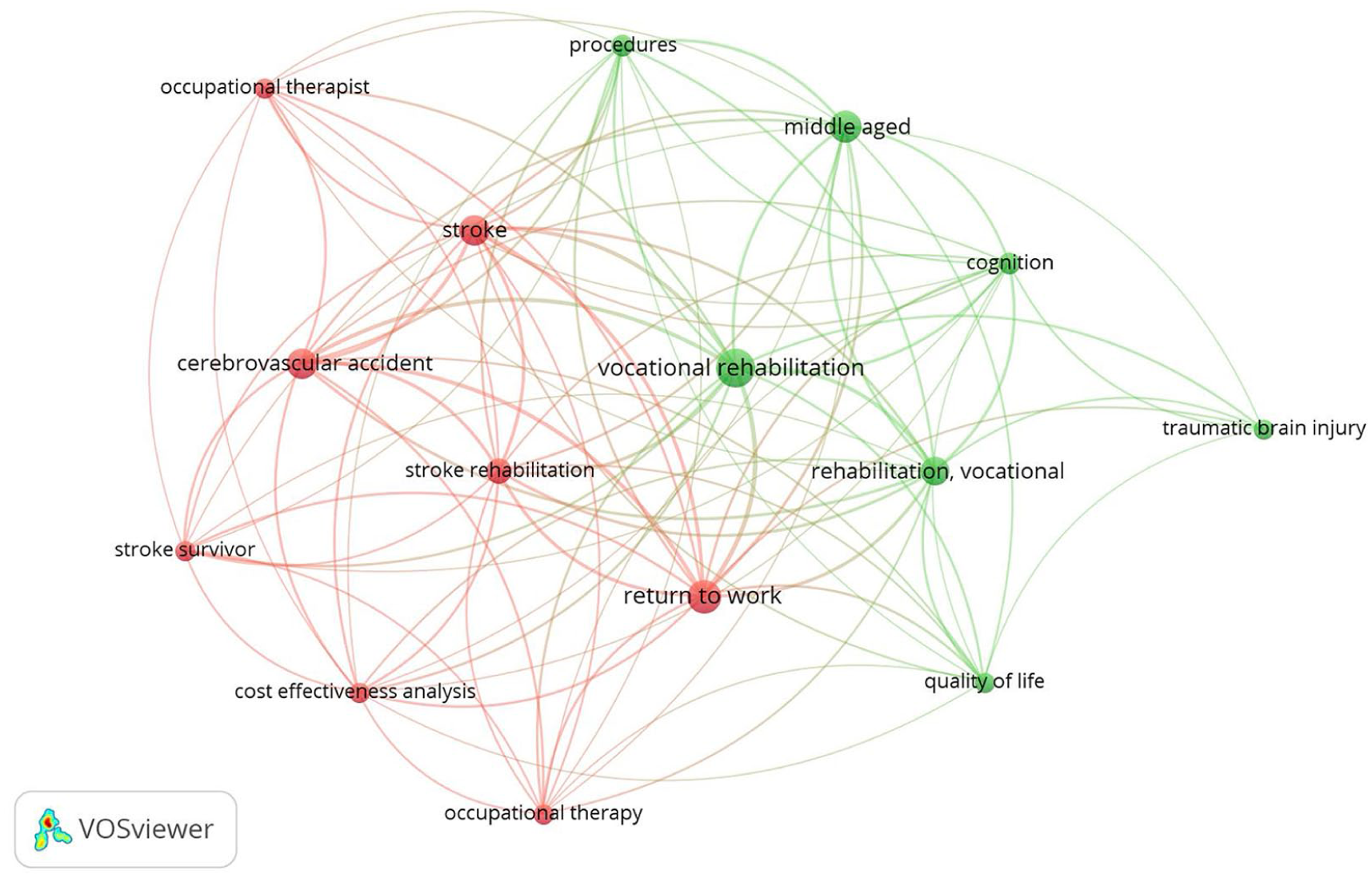
All included studies evaluated OT interventions for return to work after ABI. The evidence, comprising RCTs and pilot studies published between 1979 and 2025, reflects the current relevance and development of this research area. The database with the largest number of records was Scopus. A thematic map was generated using VOSviewer (Version 1.6.20, Center for Science and Technology Studies, Leiden University) to represent the conceptual structure of OT interventions for return to work after ABI. Figure 2 presents the general thematic organization of these interventions, while Figure 3 illustrates the grouping of specific intervention types (e.g., early stroke specialist vocational rehabilitation (ESSVR), RETurn to work After stroKE (RETAKE), and combined compensatory cognitive training and supported employment (CCT-SE)). Both figures were derived from the selected descriptors and their co-occurrence patterns.
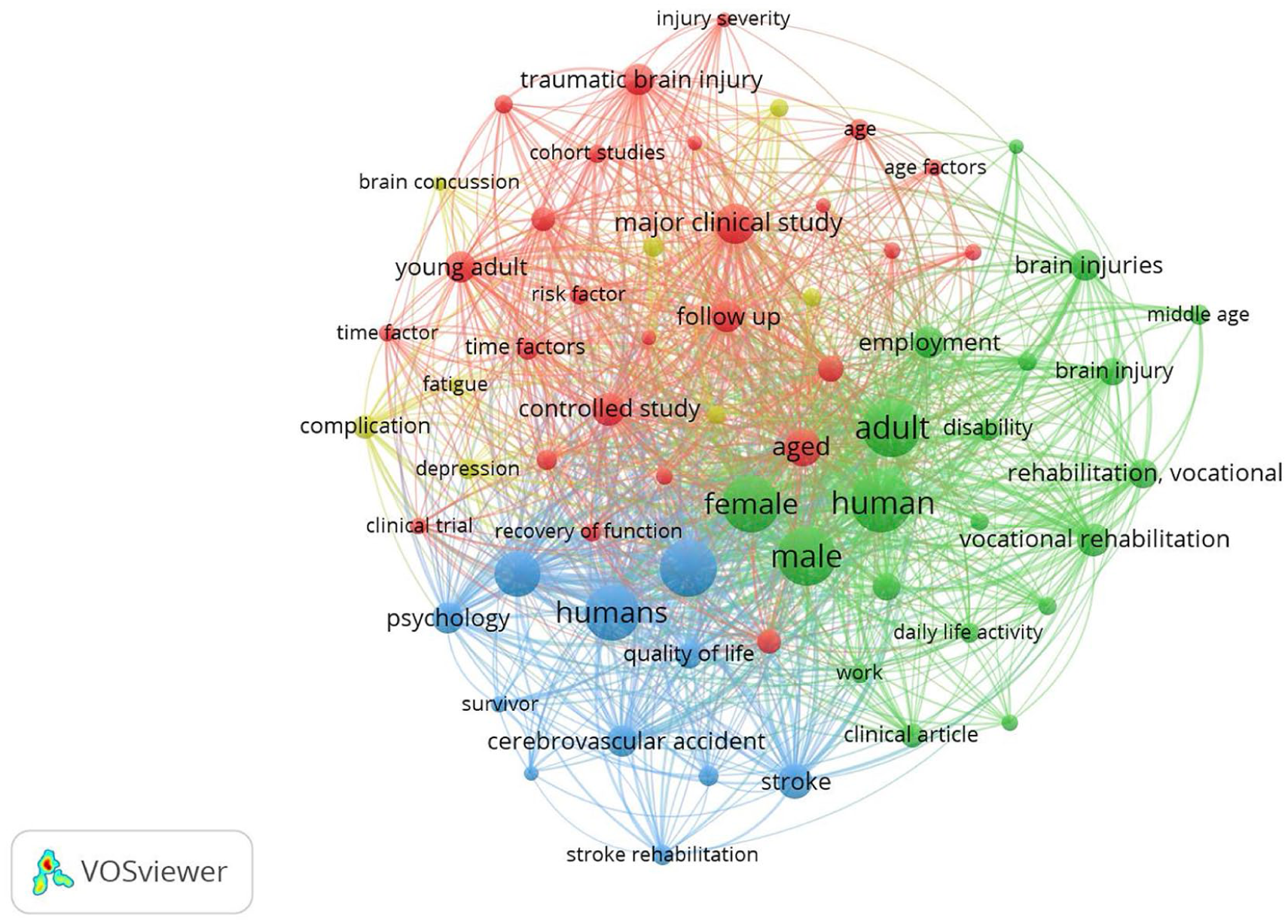
Topical distribution of the literature on occupational therapy interventions for return to work after acquired brain injury.
The literature on specific intervention types (e.g., ESSVR, RETAKE mentorship, and CCT-SE).
Occupational therapy interventions in job reintegration for people with acquired brain injury
The studies analyzed indicate that OT interventions aimed at facilitating return to work following a stroke or traumatic brain injury are predominantly defined by specialized, sustained, and personalized approaches. Clarke et al. (2024) reported that participants enjoyed ESSVR, a form of job assistance that involves evaluating functional performance, collaborating with employers, and receiving individualized support from a therapist. This program helped people get back to their old jobs or find new ones when full reintegration was not possible. In the study by Craven et al. (2021), the RETAKE program, a training and mentoring framework designed to strengthen occupational therapists’ capacity to deliver complex vocational rehabilitation, was identified as a key component for supporting implementation in this field. Fure et al. (2021) demonstrated that CCT-SE a dual approach that integrates cognitive strategy training with individualized employment support promoted a faster return to competitive work, suggesting an accelerating effect on early vocational recovery. Conversely, Pyne et al. (2024) observed no significant differences between early vocational rehabilitation and usual care regarding return to work at 12 months and reported low cost-effectiveness for ESSVR. Findings from Radford et al. (2018) and Radford et al. (2024) similarly showed high return-to-work rates across both groups, with no evidence of superiority for specialized vocational rehabilitation over usual care, although certain subgroups such as older people or individuals with greater post-stroke impairment appeared to benefit more from the structured support characteristic of ESSVR. Lastly, Vikane et al. (2016) identified psychological distress and a history of prior work disability as negative predictors of job reintegration, while pain and neuroimaging findings did not demonstrate predictive value. The reviewed studies show that vocational rehabilitation programs based on specialized support, mentorship, and combined strategies (including ESSVR, RETAKE, and CCT-SE) can facilitate early return to work among individuals with neurological sequelae. However, more recent trials indicate that overall return-to-work rates are generally comparable to those achieved with usual care, with benefits mainly observed in specific subgroups. Additionally, psychological factors and a history of prior work disability emerge as negative predictors of successful return to work.
Effects adverse and adherence
Adherence reached 88% across the seven RCT with no harmful effects reported. These findings highlight the feasibility and tolerability of the interventions for adults returning to work after ABI, reinforcing their potential for broader clinical implementation.
Discussion
Role of occupational therapy and effectiveness of early interventions
The findings of this review reinforce the central role of OT in early vocational rehabilitation programs following ABI, particularly when these include specialized support strategies, functional cognitive training, and systematic coordination with the workplace. Evidence consistently shows that the most effective interventions are those initiated early, tailored to job demands, and aligned with individual worker needs, incorporating mediation between the patient, family, and employers (Clarke et al., 2024). Nonetheless, some studies highlight the need to consider program efficiency and cost-effectiveness when implementing these approaches (Pyne et al., 2024). The review identified a comprehensive mapping of various Occupational Therapy interventions aimed at reintegration into the workforce, including the ESSVR and RETAKE models, and combined CCT-SE interventions. These strategies, while heterogeneous in structure, share a focus on addressing early on the functional, cognitive, and contextual barriers that limit the return to work after a stroke or ABI. Together, they constitute essential intervention processes that integrate functional assessment, individualized planning, ongoing support, and intersectoral coordination, allowing not only for optimized occupational recovery but also facilitating a sustainable reintegration adapted to the demands of the work environment.
Quality of evidence, intervention modalities, and qualitative contributions
The systematic review by Pearce et al. (2023) underscores the scarcity of high-quality studies on return to work after stroke, marked by methodological heterogeneity and a lack of standardized definitions for work reintegration. Still, individualized and multidisciplinary interventions led by occupational therapists such as environmental assessment, task adaptation, and employer coordination show promising but still inconclusive results. Studies on traumatic brain injury further reinforce this perspective: Mullins et al. (2025) demonstrate that combining cognitive rehabilitation, vocational training, and workplace adaptations supports safer and more sustainable work reintegration, with occupational therapists playing a central role in planning and monitoring the process. Additionally, Powers et al. (2022) highlight the importance of implementation fidelity within ESSVR programs, while the qualitative insights of Kurihara et al. (2024) identify six key domains of OT support from work performance to compensatory strategies illustrating therapists’ multifaceted role as guides, mediators, and facilitators of social and occupational participation. Importantly, the studies suggesting greater benefit in specific subgroups, such as older adults or individuals with greater post-stroke impairment, involved interventions of varying duration, ranging from short, structured programs of 4–10 weeks to individualized vocational rehabilitation delivered over several months and up to 12 months. Therefore, the current evidence does not allow firm conclusions regarding an optimal intervention duration for these populations; rather, benefit appears to depend on a combination of early initiation, individualized support, and coordination with workplace demands.
Psychosocial factors and needs for a sustainable practice
A recurring theme across studies is the relevance of psychosocial and emotional factors in determining return-to-work outcomes (Morris et al., 2012). Self-efficacy, social participation, and reconstruction of occupational identity emerge as facilitators, while psychological distress, global disability, and prolonged sick leave act as barriers (Matos et al., 2024). These findings highlight the need for comprehensive interventions that integrate physical, cognitive, and emotional dimensions, addressing stress regulation and beliefs about work ability (La Torre et al., 2022). Finally, the evidence emphasizes the importance of ongoing professional development, mentorship, and clinical supervision for occupational therapists to ensure the quality and fidelity of interventions. Together, these elements point to a person-centered, integrated, and sustained approach that optimizes return-to-work outcomes and reduces persistent barriers following ABI.
Limitations and strengths
This review has several limitations. Heterogeneity in intervention characteristics, outcomes, and patient profiles limits direct comparison across studies and prevents firm conclusions regarding the superiority of any single vocational rehabilitation model. In addition, all included studies were conducted in the United Kingdom and Norway, which may reflect country-specific rehabilitation systems and labor contexts, thereby limiting the transferability of the findings to other settings. Nevertheless, the inclusion of randomized controlled trials, together with the consistent reporting of good adherence and the absence of adverse effects, supports the feasibility of occupational therapy-based vocational rehabilitation after ABI. Therefore, the evidence should be interpreted as supportive, but not definitive, particularly with regard to the optimal intervention format, duration, and subgroup-specific effects.
Practical applications
From an OT perspective, the findings of this scoping review emphasize the importance of early, individualized, and contextually grounded vocational rehabilitation for adults recovering from stroke or traumatic brain injury. Programs such as ESSVR and ESTVR reported that structured interventions integrating workplace assessment, employer coordination, cognitive strategy training, and patient-family education can facilitate a safer and more efficient transition back to employment. The results also support the value of mentorship frameworks like RETAKE, which strengthen therapist competencies and ensure fidelity in the delivery of complex vocational intervention. Furthermore, interdisciplinary collaboration particularly among occupational therapists, employers, case managers, and mental health professionals emerges as a key component for addressing the psychosocial, cognitive, and environmental barriers that commonly hinder return-to-work trajectories. These interventions can be adapted to community-based, hybrid, or remote formats, allowing flexible implementation according to patient needs and service availability. Importantly, the evidence highlights the relevance of addressing emotional well-being, self-efficacy, and occupational identity reconstruction, all of which contribute to sustainable work participation ABI.
Research and policy implications
At the research level, this review highlights the need for larger, methodologically consistent trials that employ standardized definitions of return-to-work and long-term follow-up beyond 12 months. Future studies should explore subgroup effects, as evidence suggests that older people and individuals with higher post-stroke impairment may derive particular benefit from structured vocational rehabilitation. Incorporating mixed-methods approaches and implementation research such as fidelity evaluations like those conducted in the RETAKE trial will be essential to understanding how vocational interventions function in real-world contexts.
At the policy level, these findings underscore the importance of integrating OT interventions and vocational rehabilitation services into standard care pathways for individuals recovering from stroke and traumatic brain injury. Given the comparable return-to-work rates between specialized and usual care observed in more recent trials, policymakers should prioritize identifying which subpopulations benefit most and ensure equitable access to tailored services. Additionally, early coordination with employers, financial support systems, and community resources should be embedded into national return-to-work frameworks. Investment in cost-effectiveness studies is also needed to determine the economic sustainability of large-scale implementation of interventions such as ESSVR and CCT-SE within healthcare and social security systems.
Conclusions
The individual results of the analyzed studies report positive effects on supporting return-to-work processes after ABI, particularly when they incorporated early initiation, individualized planning, functional cognitive training, and coordinated engagement with employers. Programs such as ESSVR, RETAKE mentorship, and CCT-SE highlight the value of structured, therapist-driven approaches that address cognitive, functional, and psychosocial barriers to reintegration.
Key findings
Early, individualized occupational therapy with employer coordination facilitates safer work reintegration.
Benefits are greatest for specific subgroups; overall return-to-work rates resemble usual care.
What the study has added
This review maps high-quality randomized evidence on occupational therapy-led vocational rehabilitation after ABI, clarifying intervention components, subgroup effects, and implementation features that inform targeted, person-centered return-to-work practice.
Footnotes
Acknowledgements
This publication fulfills the publication commitment assumed within the framework of the Competition for Support for Assistance to Academic Activities, second semester 2024, Approved by D.E. No. 1107/2024, charged to UPA Agreement 21992.
Author contributions
Conceptualization, E.V.-C., P.V.-B., and P.M.-D.; methodology, E.V.-C., M.M., V.O., K.R., M.R., J.H.-M., C.S.-V., P.V.-B., and P.M.-D.; software, E.V.-C., M.M., V.O., K.R., M.R., and J.H.-M.; formal analysis, E.V.-C., M.M., V.O., K.R., M.R., J.H.-M., C.S.-V., P.V.-B., and P.M.-D.; investigation, E.V.-C., M.M., V.O., K.R., M.R., J.H.-M., C.S.-V., P.V.-B., and P.M.-D.; writing – original draft preparation, E.V.-C., M.M., V.O., K.R., M.R., J.H.-M., C.S.-V., P.V.-B., and P.M.-D.; writing – review and editing, E.V.-C., M.M., V.O., K.R., M.R., J.H.-M., C.S.-V., P.V.-B., and P.M.-D.; supervision, E.V.-C., P.V.-B., and P.M.-D. All the authors have read and agreed to the published version of the manuscript.
Funding
The authors declared no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Patient and public involvement data
During the development, progress, and reporting of the submitted research, Patient and Public Involvement in the research was not included at any stage of the research.