
Abstract
Introduction:
Frailty among older adults is a growing public health concern worldwide. Although interventions have traditionally focused on exercise and nutrition, there is limited evidence from an occupational perspective regarding simple, practical indicators—such as the total volume of daily activities—and the combined impact of environmental factors in community settings. This study aimed to examine the association between the total number of daily activities, environmental factors, and frailty status among older adults utilizing community-based senior salons.
Method:
A cross-sectional study was conducted with 271 older adults (aged ⩾65 years) in Kashiwara City, Osaka Prefecture. Frailty was assessed using the Kihon Checklist (KCL) and categorized as robust, prefrail, or frail. Independent variables included the number of current activities, ICT use, exercise habits, and environmental characteristics. Multiple imputation was used to handle missing data, and ordinal logistic regression analysis was performed to identify factors associated with frailty severity.
Results:
Of the participants, 22.1% were classified as frail and 40.6% as prefrail. Ordinal logistic regression analysis revealed that a higher number of current activities was significantly associated with lower odds of having severe frailty (odds ratio (OR) = 0.91, 95% CI: 0.87–0.95, p < 0.001). ICT use (OR = 0.57, p = 0.049) and regular physical activity (OR = 0.61, p = 0.048) were also independent protective factors. Environmental factors showed no significant associations.
Conclusion:
Engaging in a greater number of daily activities is independently associated with lower frailty risk, whereas physical environmental factors showed no direct correlation. These findings suggest that the total volume of daily activities serves as a practical occupational indicator for frailty screening. For community-based interventions, moving beyond exercise-centric models to promote “activity diversification”—including modern IADLs such as ICT use—and meaningful occupational engagement may offer a highly effective strategy for frailty prevention in older adults.
Introduction
The rapid aging of the global population poses major challenges to sustaining the health and well-being of older adults worldwide. Among these challenges, frailty has emerged as a critical public health concern, affecting a significant proportion of older adults across the globe (O’Caoimh et al., 2021). Frailty is a complex condition involving physical, psychological, and social vulnerabilities that, if not addressed, can impair daily functioning and increase the likelihood of needed long-term care (Fried et al., 2001). The number of years individuals live in a frail state is projected to rise globally (Kasajima et al., 2022). Moreover, healthcare costs are substantially higher for those who are frail compared to their prefrail or robust peers (Chi et al., 2021). Consequently, addressing frailty through prevention and management has become a pressing issue in global public health and social care. As a “super-aged” society at the forefront of this demographic shift, Japan serves as a critical context for this issue; currently, frailty affects approximately half of its older population, with 8.7% classified as frail and an additional 40.8% as prefrail (Murayama et al., 2020).
In Japan, senior salons rooted in the community have gained recognition as a practical approach to preventing frailty by fostering local engagement. These salons offer venues where older adults can participate in social interactions and health-related activities (Hikichi et al., 2015). According to Abe et al. (2020), involvement in social activities is significantly linked to a lower risk of developing physical prefrailty. Additionally, participants in senior salons have shown better physical, cognitive, and social functions than nonparticipants (Ide et al., 2023). However, some studies have indicated that simply establishing senior salons does not automatically lead to improvements in physical frailty (Tsuji et al., 2022). It has been proposed that engaging in a variety of social activities is more beneficial in preventing frailty (Abe et al., 2020). Furthermore, the range of activities, extending beyond social interaction alone, has been found to impact frailty onset even when accounting for social factors (Takahashi et al., 2023). These results suggest that engaging in a wide variety of activities is important for preventing frailty among senior salon users.
To fully grasp the significance of engaging in such diverse activities, it is essential to shift from a purely biomedical perspective focused on functional capacity to a more holistic understanding. From an occupational therapy perspective, framed by the Occupational Therapy Practice Framework (OTPF-4; American Occupational Therapy Association, 2020), frailty prevention extends beyond merely addressing physical or functional deficits. Health and well-being are inextricably linked to the meaning, quality, and balance of an individual’s occupational engagement. Participating in a “Senior Salon” is not solely about physical movement; it represents a vital form of social participation that fosters a sense of purpose, role fulfillment, and social belonging. Furthermore, based on the Person-Environment-Occupation (PEO) model (Law et al., 1996), occupational performance and participation emerge from the dynamic interaction between the individual, meaningful activities, and the environment. While the physical built environment may present barriers or facilitators, it is crucial to understand how the total volume of daily activities interacts with environmental factors to maintain occupational balance and prevent frailty in this specific cohort.
Environmental factors are increasingly acknowledged as important components of frailty prevention efforts. Specific physical characteristics of the environment—such as residential density (Arakawa et al., 2021), access to parks (Hanibuchi et al., 2011), proximity to grocery stores (Momosaki et al., 2019; Mori et al., 2022), and the density of bus stops (Okuyama et al., 2021)—have been found to influence frailty status. Additionally, the distance between a person’s home and local community centers has been linked to frailty risk (Okuyama et al., 2020). These observations emphasize the significance of residential surroundings in developing effective approaches to frailty prevention. Integrated interventions that address both activity and environmental factors have been demonstrated to support healthy aging. Turcotte et al. (2018) found that enhancing the frequency of activities along with the environmental adjustments promoted social participation among older adults and contributed to lower healthcare costs. More recent research indicates that higher levels of eHealth literacy are linked to reduced frailty, likely due to better access to health information, improved self-care, and greater involvement in preventive actions (Eto and Yamatsu, 2024; Guo et al., 2024). Similarly, Papageorgiou et al. (2016) observed that engaging in educational and leisure activities related to health maintain social connections and decreases social isolation. Furthermore, De Coninck et al. (2017) reported that interventions focused on both activity and environmental modifications for frail older adults were effective in preventing falls, alleviating joint pain, and preserving cognitive abilities, offering both health and economic advantages. These findings indicate that promoting access to varied activities and enhancing the living environment may be effective approaches for preventing frailty.
In light of these developments, the Japanese Ministry of Health, Labor and Welfare (2024) has emphasized the role of rehabilitation professionals in senior salons as part of frailty prevention initiatives. While much of the evidence regarding social participation has been developed in East Asia, the protective effects of community-based engagement are a global phenomenon. For instance, studies in Western contexts have consistently shown that participation in community centers and social groups significantly delays the onset of disability and enhances quality of life among older adults (Gale et al., 2018; Glass et al., 1999). By identifying the “number of activities” as a key predictor, the present study builds upon this global evidence by offering a practical, low-cost screening metric applicable to diverse community settings worldwide. Although previous research has separately explored the effects of activity variety and environmental factors on frailty, there is limited evidence on how rehabilitation professionals can simultaneously address both aspects in senior salon interventions. Therefore, this study aimed to investigate the relationship between the number of activities performed, environmental factors, and frailty status among older adults attending community-based senior salons. The goal is to offer evidence-based guidance for practical interventions that encourage diverse activities and environmental adjustments, thereby supporting frailty prevention in aging populations.
Methods
Ethics
Ethics approval was granted by the University Ethics Committee (2024).
Study design
A cross-sectional study design was employed to analyze the relationship between the number of activities and environmental factors with frailty among older adults who utilize community-based senior salons.
Participants
In 2023, Kashiwara City in Osaka Prefecture had a total population of 66,849, with 20,104 individuals (30.1%) aged 65 and older. Cooperation was sought from representatives of all 31 senior salons in Kashiwara City, with 21 salons (67.7%) agreeing to participate. The survey took place from March to December 2023. Of the 394 salon users, 278 individuals (70.6%) gave consent to participate. Inclusion criteria were (1) age 65 or older, (2) regular attendance at the senior salon for at least 1 month, and (3) cognitive ability to understand the questionnaire and independence in activities of daily living (ADL). In Japan, long-term care insurance is a public system separate from health insurance, which classifies care needs into seven levels (Support levels 1–2 and Care levels 1–5) based on ADL and instrumental ADL (IADL) assessments (MHLW, 2016). Since this study targeted older adults who are independent in ADL, those with certified care levels were excluded. After excluding 7 participants with care levels and 1 with incomplete data, 271 participants (68.8%) were included in the final analysis.
Initially, an a priori power analysis was conducted using the pwr package in R. Assuming a medium effect size based on previous studies (Abe et al., 2020), an alpha level of 0.05, and a power of 0.80 for 17 independent variables, the required minimum sample size was calculated to be 127 participants. However, for a multiple regression model with 17 predictors, relying solely on this power analysis is insufficient. To ensure model stability and generalizability, it is necessary to incorporate rules of thumb for regression, which recommend a minimum of 10–15 observations per independent variable. Based on the more conservative requirement of 15 participants per predictor, a minimum sample of 255 is advisable. Furthermore, given the epidemiological context of the target population—consisting of 20,104 older adults in the municipality—a larger and more representative sample is essential to adequately capture the variability of this specific population. While 127 participants may provide sufficient statistical power, our actual recruited sample of 271 participants successfully exceeds the conservative requirement of 255. This larger sample size allows us to obtain reliable parameter estimates, ensure external validity, and mitigate the risk of overfitting.
Outcome variable
The primary outcome was frailty status measured using the Kihon Checklist (KCL), a tool used in Japan’s long-term care insurance system. The KCL consists of 25 yes/no questions covering seven domains: instrumental activities of daily living (IADL), physical strength, nutritional status, oral function, isolation, memory, and mood. The total KCL score correlates strongly with the Fried frailty phenotype (Satake et al., 2016). A KCL score of ⩾4 was defined as prefrail and ⩾8 as frail (Satake et al., 2016; Watanabe et al., 2022). The KCL has demonstrated validity in identifying frail older adults.
Explanatory variables
Explanatory variables included the number of current activities, number of desired activities, exercise habits, information and communication technology (ICT) use, and environmental factors such as population density, housing density, number of parks, grocery stores, and bus stops in the local district.
Ongoing activities and activities of interest were assessed using the Interest and Concern Checklist, a common assessment method employed to understand the needs of individuals before implementing rehabilitation under Japan’s Long-Term Care Insurance system. This checklist is part of the Life Performance Enhancement Management tool developed by the Japan Association of Occupational Therapists (JAOT, 2012). The assessment covers a broad range of daily life activities and interests, including activities of daily living (ADL, e.g., personal care, eating, dressing), housework (e.g., cleaning, cooking, shopping), hobbies and leisure (e.g., reading, sports, crafts), and social participation (e.g., outings, community activities, socializing with friends). This self-administered tool includes 46 life-related activities, for which participants indicate “currently doing,” “want to do,” or “interested in.” We counted the number of ongoing activities (0–46) and activities of interest (up to 92 for “want to do” and “interested in” combined).
Exercise habits were determined by whether participants engaged in ⩾40 minutes of physical activity, as recommended by the Ministry of Health, Labour and Welfare (2023).
ICT use was assessed by asking whether participants used the LINE app, utilized by over 90% of Japanese people (MIC, 2024).
Environmental data at the salon level—such as population and housing density—were obtained using geographic information systems (GIS) based on publicly available data from the Ministry of Land, Infrastructure, Transport, and Tourism (2024). The number of parks and bus stops in each district was manually verified and aggregated using Google Maps. To assess accessibility and environmental barriers, buffer distances of 500 m and 1000 m were selected based on established gerontological literature regarding older adults’ walking capacities. A 500 m radius is widely recognized as a standard, manageable daily walking distance (approximately a 10- to 15-minute walk) for community-dwelling older adults, defining their immediate functional neighborhood. In contrast, a 1000 m radius captures a broader community boundary necessary for accessing essential services. Importantly, as physical frailty progresses, even a 500 m distance can become a significant environmental barrier. Therefore, examining these specific buffer zones is crucial for understanding how the built environment interacts with daily activity volume to influence frailty status.
Covariates
Covariates included potential confounders of social participation and frailty. Basic demographic attributes included age, smoking status, alcohol use, years of education, family composition, and number of chronic diseases. Smoking status was recorded as “currently smoking: yes or no.” Alcohol consumption was categorized as “daily,” “occasionally,” or “none/unable to drink.” Education was recorded by number of years, and family composition by number of cohabitants. Chronic disease count was based on the presence of conditions common among older adults in Japan: hypertension, diabetes, hyperlipidemia, stroke, leg fractures, dementia, hearing impairment, joint disorders, cancer, heart disease, liver disease, and kidney disease.
Data collection
In March 2024, the research objectives and methods were explained at a city meeting attended by salon representatives. Following informed consent—provided both orally and in writing with the support of public health nurses and care managers from community care centers—a self-administered questionnaire was distributed. Contact information for study collaborators was included in the materials to address participant inquiries. Questionnaire collection was conducted in person by the research team.
Statistical analysis
To address missing data (which had a proportion of less than 10% across all variables), we assumed the data were missing at random (MAR). Multiple imputation by chained equations (MICE) was performed using the mice package in R (van Buuren and Groothuis-Oudshoorn, 2011). We generated 20 imputed datasets. To support the MAR assumption and improve imputation accuracy, the imputation model included the comprehensive set of all variables used in the analysis (i.e., the dependent variable and all independent predictors), which collectively served as robust predictors for the missing values. The results from the subsequent ordinal logistic regression models were then pooled using Rubin’s rules. As a sensitivity analysis to assess the robustness of our findings, the same analysis was conducted on complete-case data (excluding missing values) and compared with the multiple imputation results.
Descriptive statistics were calculated for all variables. Since the Shapiro–Wilk test indicated that the continuous variables were not normally distributed, comparisons among the three frailty status groups (robust, prefrail, and frail) were conducted using Kruskal–Wallis tests for continuous variables and chi-square tests for categorical variables. Spearman’s rank correlation was used for an initial assessment of multicollinearity among the explanatory variables.
To identify factors associated with frailty status, an ordinal logistic regression analysis was employed, given that the dependent variable consisted of three ordered categories (robust, prefrail, and frail). Variables demonstrating significant associations in the univariate analyses were incorporated as explanatory variables in the multivariate model. The proportional odds assumption was verified using the Brant test. Furthermore, variance inflation factor (VIF) values were calculated; values below 2.5 were considered acceptable to confirm the absence of problematic multicollinearity.
All statistical analyses were conducted using R version 4.4.3. A two-tailed p-value of less than 0.05 was considered statistically significant.
Results
A descriptive and univariate analysis was conducted. Among the 271 participants in the study who utilized community-based senior salons, 22.1% were classified as frail and 40.6% as prefrail. The majority of the participants were female (87.1%), and 34.7% reported engaging in regular physical activity. Moreover, a significant proportion of the participants, amounting to 72%, reported their ability to utilize ICT (Table 1).
Table 2 presents the results of the univariate analysis by frailty status. The median number of current activities differed significantly across frailty groups: 28 activities (interquartile range (IQR): 24–32) for the robust group, 24 activities (IQR: 20–28) for the prefrail group, and 22 activities (IQR: 18–24) for the frail group (p < 0.01). A number of additional variables were found to demonstrate statistically significant differences among the groups. These variables included age (p < 0.01), physical activity (p < 0.01), and ICT use (p < 0.01; Table 2).
Demographic and health characteristics of the study participants.
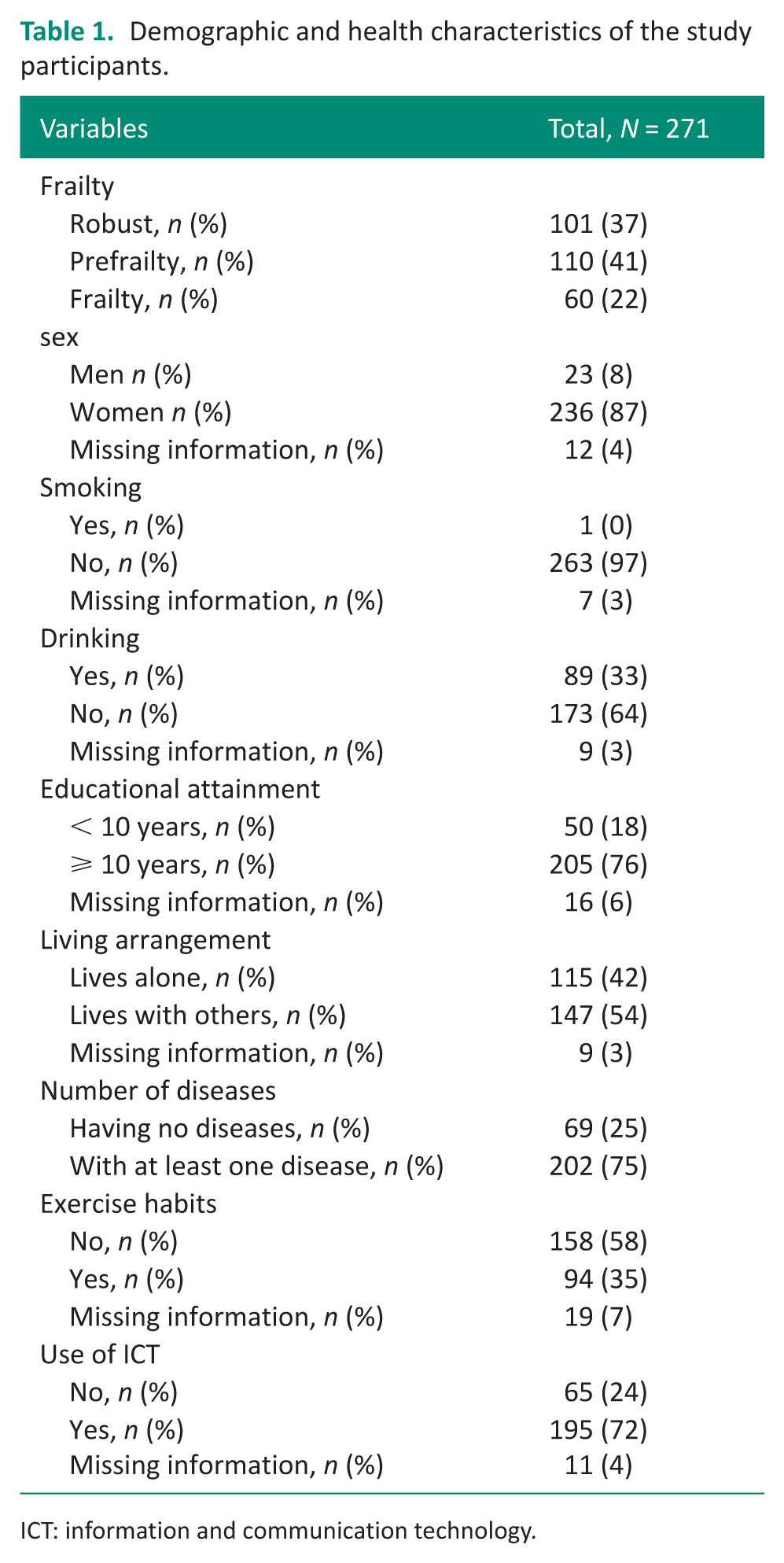
ICT: information and communication technology.
Comparison of daily activities, environmental factors, and characteristics according to frailty status.
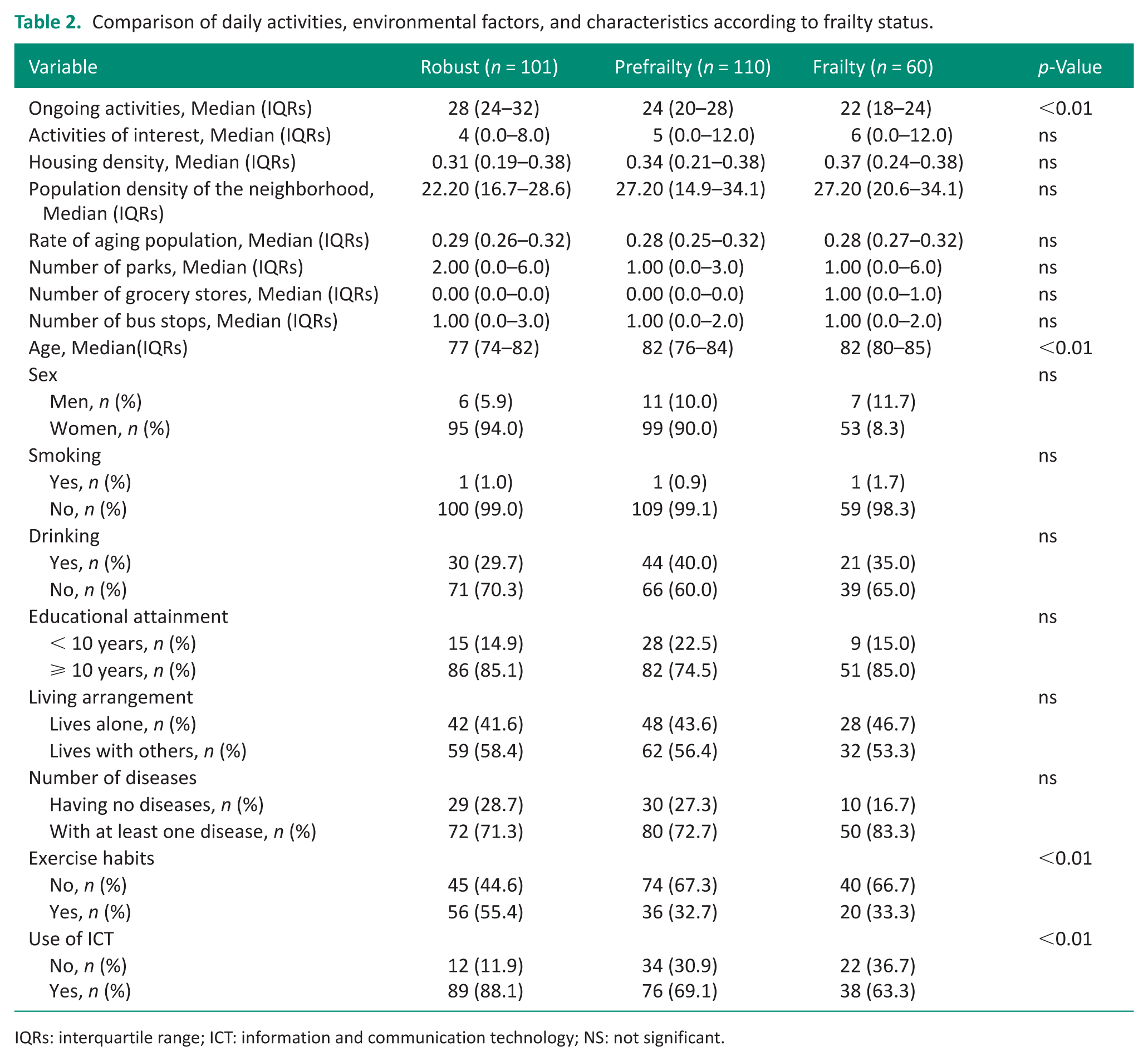
IQRs: interquartile range; ICT: information and communication technology; NS: not significant.
Given the conceptualization of frailty status as an ordered categorical variable, an ordinal logistic regression analysis was conducted to identify independent predictors. Prior to interpreting the model, the proportional odds assumption was evaluated using the Brant test. The results indicated that the assumption was not violated (overall χ2 = 8.61, p = 0.57), confirming the model’s validity across all levels of frailty. Additionally, all VIF were confirmed to be below 2.5, indicating no issues with multicollinearity. The results presented below are derived from the multiple imputed datasets aggregated using Rubin’s rules, which were also consistent with a complete-case sensitivity analysis. The multivariate model (Model 2, Table 3) revealed that several factors were significantly associated with a lower risk of having a more severe frailty status (i.e., protective factors, OR < 1.0). Specifically, the number of current activities emerged as the strongest predictor, with a one-unit increase in activities corresponding to a 9% reduction in the odds of being in a more severe frailty category (OR = 0.91, 95% CI: 0.87–0.95, p < 0.001). Furthermore, the utilization of ICT (OR = 0.57, 95% CI: 0.32–1.00, p = 0.049) and the maintenance of regular exercise routines (OR = 0.61, 95% CI: 0.37–0.99, p = 0.048) were identified as significant protective factors. In contrast, age was identified as a significant risk factor, with a one-year increase in age corresponding to a 5% increase in the odds of having a more severe frailty status (OR = 1.05, 95% CI: 1.00–1.09, p = 0.037). The investigation revealed that environmental variables, encompassing housing density, the aging population rate, and proximity to facilities, exhibited no substantial correlation with frailty status.
Results of ordinal logistic regression analysis identifying factors associated with frailty severity.
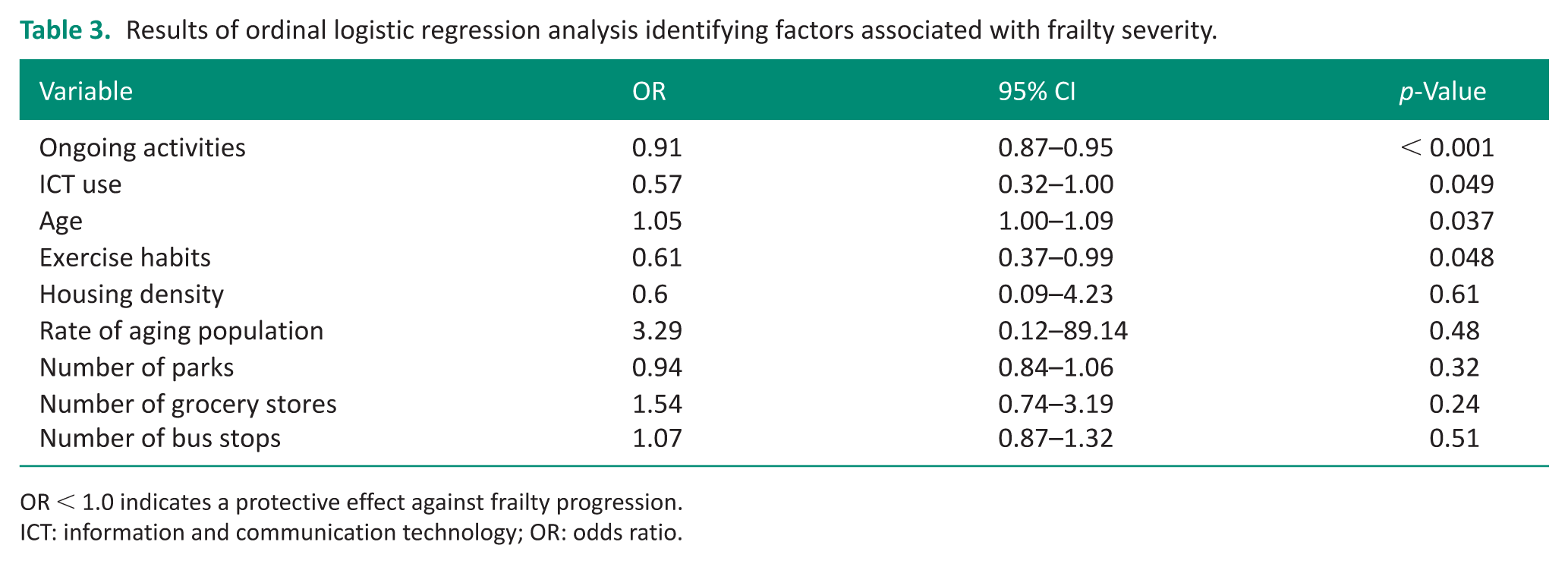
OR < 1.0 indicates a protective effect against frailty progression.
ICT: information and communication technology; OR: odds ratio.
Discussion
The present study found that robust older adults engaged in a significantly greater number of activities compared to those categorized as prefrail or frail. It has been hypothesized by researchers that engaging in a combination of activities, including physical, cultural, and community-based pursuits, may contribute to the prevention of both frailty and prefrailty (Yoshizawa et al., 2019). Furthermore, robust older adults have been found to participate in a greater number of social activities than their prefrail or frail counterparts (Abe et al., 2020). Moreover, the quantity of social participation has been demonstrated to correlate with ADL and IADL capabilities, serving as an indicator of successful aging (Tomioka et al., 2017). Reduced activity is frequently identified as a pivotal element in the frailty cycle (Fried, 2016).
Despite the fact that the present study concentrated on “senior salons” within the Japanese context, it is evident that these entities exhibit functional characteristics that are analogous to those of “senior centers” in the United States and “community hubs” in the United Kingdom. Consequently, the observation that the quantity of activities is significantly associated with a lower prevalence of frailty suggests a high degree of transferability to community-based interventions on a global scale. It is suggested that such centers worldwide should prioritize programs that not only foster social interaction but also explicitly expand the repertoire of users’ daily occupations.
Nevertheless, contemporary frailty prevention strategies predominantly emphasize exercise, nutrition, and social support (Antoniadou et al., 2024), with a paucity of studies acknowledging the sheer number of activities. It is noteworthy that interventions aimed at enhancing physical activity through exercise have exhibited substantial efficacy in mitigating the risk of developing frailty (Bray et al., 2016; Eidam et al., 2024; Xu et al., 2024). Resistance training has been demonstrated to enhance sit-to-stand performance and balance in frail older adults (Nagata et al., 2023). However, exercise-centered interventions often face barriers such as fall risk (El-Khoury et al., 2013), cardiovascular concerns, and adherence issues, which necessitate access to facilities and trained professionals.
Furthermore, the concept of frailty is influenced by a multitude of factors operating at both the community and societal levels (Boucham et al., 2024). Consequently, alternative approaches that focus on nonexercise physical activities have emerged. These include leisure-oriented activities, which have been associated with reduced frailty risk among community-dwelling older adults, independently of formal exercise routines (Lyu et al., 2025). For instance, it has been demonstrated that regularly engaging in above-average levels of light housework over a prolonged period is associated with a 39% reduction in the odds of becoming prefrail or frail (Lee et al., 2022).
Alongside these physical tasks, the present study identified the utilization of ICT as a highly significant protective factor against frailty progression (OR = 0.57). In the context of an increasingly digital society, we propose framing ICT use not merely as a leisure activity, but as a “Modern Instrumental Activity of Daily Living (IADL).” From a humanistic and occupational perspective, digital literacy and ICT engagement represent a vital bridge to maintaining social participation, accessing community resources, and sustaining interpersonal connections. Indeed, recent evidence among older adults in Japanese community gathering places demonstrates that ICT use directly expands social networks, which in turn facilitates meaningful social participation and mitigates cognitive decline (Nakahara and Yokoi, 2024). Therefore, facilitating ICT use and addressing the digital divide among older adults should be considered a critical, actionable component of contemporary frailty prevention strategies.
Despite the absence of a statistically significant discrepancy in the number of desired activities across the various frailty groups, a discernible trend toward heightened interest was observed, with interest increasing from robust to frail individuals. This suggests that, while exercise remains important, supporting older adults in transforming their desired activities—including leisure and household tasks—into actual participation may help mitigate or reverse frailty and prefrailty.
With regard to environmental factors, walkable environments have been demonstrated to be inversely associated with frailty (Kim et al., 2019; Mitsutake et al., 2021). At the community level, the presence of physical barriers, such as slopes and stairs, has paradoxically been linked to a lower risk of frailty in certain contexts (Mori et al., 2022). The influence of the physical environment remains unclear and may vary by gender (Koohsari et al., 2020), demographics, and lifestyle patterns (Okuyama et al., 2020). As Duppen et al. (2019) demonstrate, social environments, including social networks, support, participation, community characteristics, and subjective neighborhood experiences, are also integral. Crucially, in the present study, the macroscopic built environment (e.g., parks, housing density) was not significantly associated with frailty status. Rather than viewing this merely as a null finding, it provides a compelling opportunity to consider the “Social Buffer” hypothesis through the lens of the PEO model (Law et al., 1996). The PEO model emphasizes that occupational performance is the product of the dynamic, transactional relationship between these three domains. When viewed from this perspective, it is highly plausible that a robust social environment—characterized by strong peer interactions, social support, and a sense of belonging fostered within the senior salons—alongside meaningful occupational engagement, functions as a powerful compensatory mechanism. This dynamic interaction can effectively mitigate and override the limitations of a restrictive physical environment. This finding challenges the strict notion of environmental determinism in frailty prevention, implying that interventions focusing on maximizing social capital and meaningful participation can be highly effective, even for older adults residing in physically challenging or resource-limited neighborhoods. Furthermore, from an occupational perspective, social capital and community cohesion do not merely buffer physical barriers; they act as vital catalysts that naturally drive an increase in activity volume. A rich social environment provides both the diverse opportunities and the intrinsic social motivation necessary for older adults to engage in a wider array of daily occupations, thereby creating a virtuous cycle of expanded participation and frailty prevention.
The present study posits that the promotion of a greater number of activities may offer a novel perspective in the development of frailty prevention strategies for community-dwelling older adults. Specifically, from a clinical perspective, the finding that incorporating just one additional daily activity is associated with a 9% reduction in the odds of being prefrail or frail provides a highly actionable and encouraging message. For occupational therapists, these findings necessitate a paradigm shift from solely remediating physical deficits to actively managing the “total volume of occupations” in a client’s life. It is the position of therapists that they are uniquely positioned to engage in lifestyle redesign approaches that identify latent interests and facilitate their translation into actual performance. By strategically increasing the number of daily activities, ranging from IADLs to leisure tasks, occupational therapists can provide a potent, nonpharmacological defense against the progression of frailty.
While this study underscores the protective value of activity volume, we must approach these findings through an occupational science lens, acknowledging the balance between quality and quantity (Eklund et al., 2017). As highlighted by existing literature, both occupational deprivation and occupational overload pose significant risks to older adults’ health and well-being (Park et al., 2021). Therefore, merely increasing the number of activities without considering their subjective meaning and contextual appropriateness could be counterproductive. In this context, these findings highlight the potential contribution of occupational therapists not merely as exercise instructors, but as “prescribers of occupations.” For frailty prevention and healthy aging, activity volume serves as a practical and sensitive indicator for initial community screening. Following this assessment, occupational therapists can individualize and monitor interventions, prescribing a diverse range of daily occupations—from modern IADLs such as digital literacy to leisure and social participation. This ensures that engagement is not only numerous but also meaningful, balanced, and contextually appropriate.
Future studies should explore the minimum number of activities required to maintain robustness and aim to develop new frailty assessment measures based on the diversity, quantity, and quality of activities.
Limitations
This study has several limitations. First, the cross-sectional design within a single Japanese municipality limits generalizability and precludes causal inference. Although capturing a “current snapshot” provides immediate, actionable insights for community health screening, the possibility of reverse causality must be explicitly acknowledged. While lower activity volumes independently correlated with frailty, a bidirectional relationship is highly plausible: reduced activity may exacerbate frailty, or existing physical/cognitive decline may restrict daily activities. Thus, activity volume currently serves as a practical clinical marker rather than a definitive determinant, necessitating future longitudinal studies to establish temporal sequences.
Second, our purely quantitative approach measured activity volume without assessing quality or subjective meaning. From an occupational therapy perspective, this limits our holistic understanding of the elderly experience and the potential risks of “occupational overload.” Furthermore, while the Kihon Checklist (KCL) is a validated tool, its inherently deficit-based nature may overlook the subjective well-being older adults maintain despite physical vulnerabilities. Future research must incorporate subjective assessments to capture the critical balance among activity quantity, quality, and meaningfulness.
Finally, the lack of significant associations between the physical environment and frailty must be interpreted cautiously, as we relied on macroscopic, objective indicators. Foundational models (MOHO, CMOP-E) emphasize that subjective environmental perceptions (“environmental press”) and immediate micro-environments (e.g., home hazards) are equally critical to occupational performance. Our null findings may therefore reflect the limitations of relying solely on macroscopic variables. Future studies should employ multilayered assessments combining objective macro-level data with subjective micro-level evaluations to fully capture person-environment transactions.
Conclusion
This study demonstrated that a greater number of activities are significantly associated with lower levels of frailty and prefrailty among older adults who participate in community-based senior salons. While traditional frailty interventions have emphasized exercise and nutrition, our findings highlight the clinical importance of promoting “activity diversification”—incorporating a broader range of daily occupations, including leisure, household tasks, and digital literacy—as a potent strategy for frailty prevention.
The observed trend of increased interest in activities among frail individuals suggests significant potential for behavioral interventions aimed at converting desired activities into actual engagement. Notably, the number of activities emerged as a more robust and practical indicator of frailty status than physical environmental factors. While the sheer number of activities serves as a sensitive and time-efficient indicator for initial community screening, our findings necessitate a paradigm shift in intervention design. For occupational therapy practice, this implies moving beyond exercise-centric models toward a comprehensive approach that optimizes a client’s overall occupational engagement, ensuring that daily routines are both diverse and personally meaningful.
In conclusion, these findings advocate for community-based interventions that prioritize both the quantity and diversity of daily engagement. Specifically, fostering ICT use as a “Modern IADL” represents a vital bridge to social participation in an increasingly digital world. Future research should focus on establishing evidence-based thresholds for activity levels while developing assessment indicators that integrate the quantity, quality, and diversity of occupational engagement to maintain robustness in aging populations.
Key findings
Higher total volume of daily activities is independently associated with lower frailty risk, serving as a practical occupational indicator.
Physical environmental barriers may be effectively mitigated by the strong “social buffer” provided by community-based senior salons.
Community interventions should prioritize “activity diversification” and modern IADLs (e.g., ICT use) over traditional exercise-centric models.
What the study has added
This study identifies that the total volume of daily activities serves as a highly practical occupational indicator for frailty screening, demonstrating that active engagement can override physical environmental barriers among community-dwelling older adults.
Footnotes
Ethical considerations
This study was conducted with approval from the Institutional Review Board of Kansai University of Welfare Sciences (Approval No. 24-10).
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Author Contributions
KN conceptualized the study, performed the data analysis, and drafted the manuscript. YF provided supervision and guidance during the data collection process. KY supervised the preparation of the manuscript and critically reviewed its content. All authors have read and approved the final manuscript.
Funding
The authors declared no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Patient and public involvement data
During the development, progress, and reporting of the submitted research, Patient and Public Involvement in the research was included at all stages of the research.