
Abstract
Introduction:
Experience of gravitational insecurity (GrI) is evident in heightened fear responses to movement during everyday activities. In adults, it has been suggested to lead to increased anxiety and avoidance of activities to minimise the impact of GrI. The perceptions of adults on the lived experience of GrI are absent from the existing evidence base, and this study aims to begin to meet this gap.
Method:
Semi-structured interviews were completed with six participants from the UK and Ireland who experience gravitational insecurity. Participant responses were analysed using interpretative phenomenological analysis to identify themes.
Findings:
Three main themes were identified: a not-so-disproportionate response, moving from judgement to acceptance, and learning to manage gravitational insecurity. Participants reflected on how having an explanation for their difficulties supported a more compassionate reframing. Rather than avoidance, participants described prioritising and planning as key strategies to enable occupational engagement.
Conclusion:
Increased awareness and knowledge of GrI are needed to enable occupational therapists to best support individuals who experience this difficulty. Providing information to support understanding of GrI is likely to be a key first step when working with adults to reduce negative self-perceptions and support self-management.
Introduction
Gravitational insecurity (GrI) is a sensory processing difference thought to primarily relate to alterations in processing of vestibular input (Potegal et al., 2022). Historically GrI has been defined as a fear response to movement that is out of proportion to the level of threat and any postural deficiencies (Fisher and Bundy, 1989; Lane, 2020). There is thought to be no one specific presentation, but commonly reported themes include a strong desire to keep the feet on the ground and difficulty with movement activities that involve moving the head out of an upright position or navigating across unstable or changeable surfaces (May-Benson and Koomar, 2007; Potegal, 2025). Examples of where this may occur for adults include using an escalator or lift, travelling in a car or an aeroplane, going up or down stairs, or tipping the head back during activities such as hair washing (Lane, 2020; May-Benson et al., 2020a). Recent literature has also highlighted potential relationships with heightened anxiety and autonomic responses (Matson et al., 2025; May-Benson et al., 2020a). However, insight into the lived experiences of GrI is largely absent from the evidence base, other than in proxy reports from professionals and anecdotal accounts. Therefore, this study aims to give voice to the perspectives of adults who experience GrI. While in much of the existing literature terms such as sensory processing disorder or dysfunction are present, within this article, the term sensory processing differences will be used wherever possible to reflect a focus on neuro-affirmative language (Speilmann, 2025).
Literature review
GrI is often evident in more everyday linear movements that others would not consider problematic, and characterised by an autonomic fear response, rather than an experience of dizziness or the spinning sensation often connected with vertigo (Lane, 2020; May-Benson et al., 2020a). Although similar experiences have been described in the literature as space and motion discomfort (SMD), this construct is more closely associated with dizziness and imbalance and has been linked to both peripheral and central nervous system (CNS) factors (Jacob et al., 1993; Whitney et al., 2018). GrI has been distinguished from other vestibular-based conditions through a connection to the CNS processing of vestibular input, rather than differences in functioning of the peripheral vestibular apparatus (May-Benson et al., 2020a, Potegal et al., 2022). Early descriptions connected GrI to deficiencies in modulating vestibular input received from the otolith organs (Ayres, 1979; Fisher and Bundy, 1989). More recent research has connected GrI to inefficiencies in vestibular velocity storage (VVS), whereby signals from the semi-circular canals are insufficiently amplified, limiting the ability to discriminate vestibular input and accurately determine head movement (Potegal, 2015; Potegal et al., 2022). Deficiencies in the integration of proprioceptive and visual input, which are needed to “make sense” of the movement experience, have also been suggested to be part of the aetiology of GrI (Koomar, 1996; May-Benson et al., 2020a).
To date, there is relatively little research into the prevalence of GrI in adults; however, it is thought to be experienced by between 6% and 18% of adults to some level (May-Benson et al., 2020b). As with other vestibular-based difficulties, anxiety is thought to be a frequently associated experience, with a moderate correlation (r = 0.335) between GrI and anxiety identified in a sample of 1832 adolescents and adults (May-Benson et al., 2016). Strong autonomic nervous system responses have also been suggested to be apparent in fight, flight, and freeze responses (Matson et al. 2025). The presence of GrI in adults has been suggested to be often missed or misattributed, with fear responses to movement and functional difficulties being related instead solely to mental health difficulties or a phobia (Ayres, 2005; Coelho and Balaban, 2015; Matson et al., 2025). Occupational therapists have suggested that this lack of awareness can lead to increased frustration, a sense of mistrust in their own bodies, withdrawal from others due to attempts to hide the impact, and strained relationships with health professionals who may misjudge behaviours (Matson et al., 2025).
Supporting individuals to understand the functional challenges related to sensory processing differences such as GrI can help to reduce self-judgement (Forsberg et al., 2024; Matson et al., 2025; Miller et al., 2023; Williamson and Ennals, 2020). Sensory processing differences in adults are thought to have often been present since childhood but unacknowledged. As a result, by adulthood, occupational participation may have been significantly altered, and avoidance strategies are likely to be much more prevalent (Miller et al., 2023; Pfeiffer, 2020). Consequently, it may be much more difficult to identify these experiences in adults and provide context to their responses. The potential significance of a more limited understanding suggests why it is particularly important to gain insight into the perceptions of adults themselves who experience GrI. While there are previous studies that have sought the perspective of occupational therapists on the experience and presentation of GrI (Matson et al., 2025; Potegal et al., 2018), there are no studies to date that have directly investigated the perspectives of these individuals themselves. Therefore, this study aimed to consider the question “What are the lived experiences of adults with gravitational insecurity?”
Method
Interpretative phenomenological analysis (IPA) was used within this study to facilitate an in-depth consideration of the experience and perception of those interviewed (Smith and Osborn, 2007). IPA views the analysis process as a double hermeneutic where the participants are making sense of their own experience, but the researcher is also making sense of the participants doing so (Smith and Nizza, 2022). Since knowledge of GrI is likely to be more limited, an approach where researchers are more active in the interpretative process was considered particularly pertinent (Matson et al., 2025; Potegal et al., 2022). All study materials, including the study protocol, recruitment materials, participant information sheet, consent form, and interview guide, were developed and reviewed using Patient and Public Involvement (PPI) focus groups consisting of two experts by experience and two clinicians with advanced training in sensory processing. Ethical approval was granted by University of Liverpool IPH-REC, reference 14333.
Participants were recruited through purposive sampling with adverts for the study placed on relevant social media groups and distributed via Sensory Integration Education’s online call for research participants and mailing list. Potential participants were invited to contact the lead researcher if they identified with the indicators of GrI included on the advert, following which they were sent the participant information sheet and link to an online consent form. These indicators represented frequently discussed participation challenges in the GrI literature, such as anxiety related to using escalators or lifts and crossing bridges, and were agreed by the PPI group. Participation was limited to adults aged 18–50 with self-reported experience of gravitational insecurity. Prevalence of vestibular-related disorders significantly increases over the age of 65, with shifts in vestibular sensitivity beginning as early as age 40 (Wagner et al., 2021). An upper age limit of 50 years of age was agreed with the PPI group as a balance between reducing the risk of this as a confounding factor, but without overly excluding potential participants. Those with comorbid conditions or symptomology that have a strong vestibular component, such as vertigo, labyrinthitis, and Meniere’s disease, were also excluded. Comorbidity of anxiety was not an exclusion criterion as the potential for this to co-occur is acknowledged in the literature and has not been an exclusion criterion in GrI studies to date (Potegal et al., 2022; Potegal, 2025). However, to reduce the potential impact of this as a confounding variable, the interview schedule supported detailed reflection on both specific movement experiences as well as the range of situations in which GrI occurred for the participant.
As a first step, participants were asked to complete a self-assessment tool, the Adult/Adolescent Sensory History (ASH) (May-Benson, 2015). This was considered as a necessary step, due to the current limited awareness of GrI, both to determine the likelihood of a participant experiencing GrI, and to support initial self-reflection on experiences. Participants were invited to participate in a semi-structured interview completed via MS teams if they scored within the mild or definite range in the GrI subsection of the ASH. This allowed for participation from a broad geographical area, increasing the potential to obtain a sufficient sample on an emerging area of knowledge. Consent was revisited verbally prior to the commencement of the interview. Following the interview, participants were provided with a debrief form and a £20 voucher as a thank you for participating in the study. Where the ASH results suggested a participant did not experience GrI, reflected by a score within the typical range, a debrief form was provided thanking them for their interest in the study but advising they would not be invited for an interview. Out of seven potential participants screened using the ASH, only one scored within the typical range.
All six participants were female, within the age range specified for the study, and resided within the United Kingdom or Ireland. Small sample sizes are common within IPA studies to support increased focus on depth of understanding and increased consideration of the individual experience (Pietkiewicz and Smith, 2014). ASH total scores and scores for GrI are provided for each participant in Table 1 below as contextual data. These are in the form of z scores that reflect standard deviation from the typical mean (May-Benson, 2015). For each area on the ASH, participants can score within the typical (above −1.0), mild (between −1.0 and −2.0), or severe (−2.0 or lower) range. As this study is concerned with lived experience rather than correlations of different factors to GrI, further demographics, such as a participant’s specific age or ethnicity, are not reported.
Participant information.
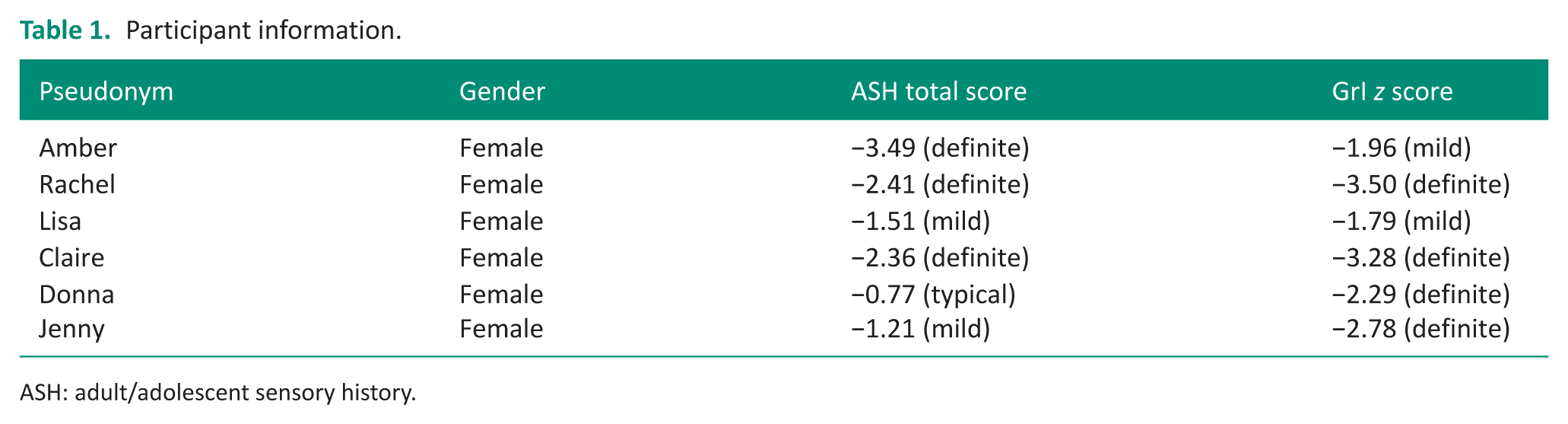
ASH: adult/adolescent sensory history.
Interviews were completed by two researchers following an interview schedule, with additional prompts to support further exploration as needed. Questions were developed based upon the existing literature about GrI, as well as ideas and feedback from the PPI focus group. Initial questions asked participants to reflect on how they initially became aware of their experience of GrI and noted day-to-day experiences. This progressed towards reflection on specific movement experiences, the impact on their well-being, and the responses of those around them.
Data collection took place between March and June 2025. Interviews lasted between 34 and 52 minutes and were transcribed verbatim using the transcription feature within MS Teams, with one member of the research team correcting and verifying the transcripts. Any identifying details were also removed at this point.
Data analysis
Data analysis was completed by the lead researcher (RM) following the stages of IPA analysis as outlined by Pietkiewicz and Smith (2014), where each transcript is analysed individually prior to the identification of shared or overarching themes, which are known as Group Experiential Themes (GETs). To develop the required level of familiarity with the data, (RM) re-read the transcripts prior to noting early observations and reflections on the language used, the participant’s context, and reflexive comments they made during the interview (Smith and Osborn 2007). Emerging themes were identified from these initial notes to ensure they retain a strong connection to the participant’s account. Personal experiential themes (PETs) were then identified from the initial transcript and shared with the co-researcher (KF) for their reflections. Each transcript was analysed in turn, with the PETs from each transcript informing the identification of overall GETs intended to capture convergence and divergence in the experience of GrI.
Trustworthiness
Both researchers are occupational therapists and advanced sensory integration practitioners who have worked clinically with individuals identified as experiencing GrI. Following each interview, immediate reflections were noted to support later analysis and identify potential influencing factors on the researcher’s interpretation. All stages were documented to support transparency within the process. Quotations are used within the analysis to support the researcher’s interpretations and ensure these interpretations remain rooted in the experience of the participants (Nizza et al., 2021).
Findings
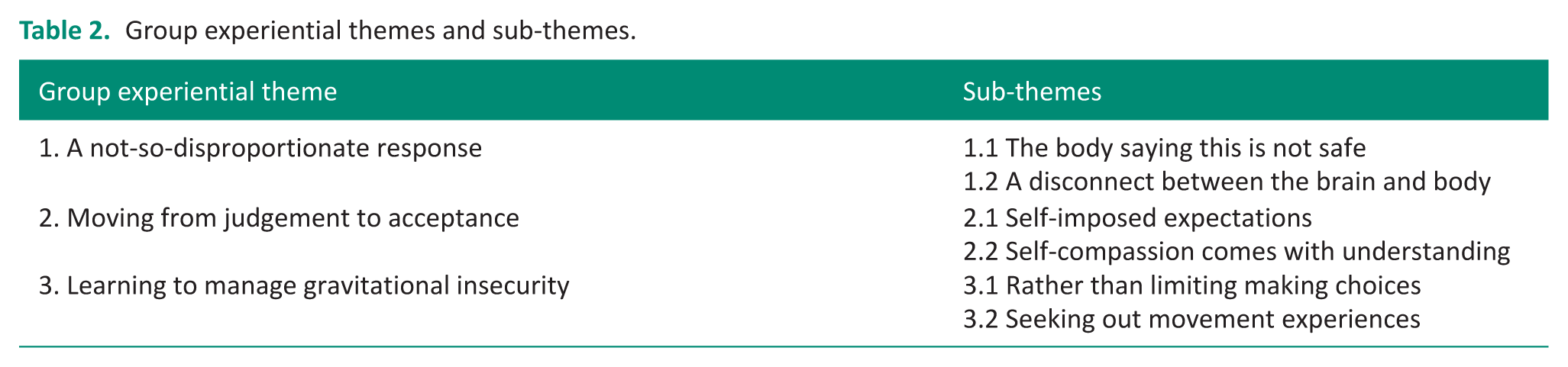
Three Group Experiential Themes (GETs), each featuring two sub-themes, were identified as shown in Table 2.
Group experiential themes and sub-themes.
A not-so-disproportionate response
This GET captures the participants’ experience of innate safety responses that may appear irrational to those around them. These responses were described as defying any logic or attempts at reasoning.
The body saying this is not safe
Five out of six participants described strong autonomic responses to movement, such as becoming immobilised, tightening of the chest, and altered breathing. All five participants refer to the impact of GrI on their sense of safety. Jenny suggests these responses are automatic and outside of their control: you don’t have a choice. You don’t, you know, you literally can’t move
Claire echoes this experience of immobilisation when discussing moving across changeable surfaces around an airport: you feel like you’re walking to your death, like every fibre in your body is saying don’t move. This isn’t safe
For Amber, the sense of threat is so significant that these responses are even activated when reflecting on movement experiences, she states, “even as I talk about it . . . my shoulders are shrugging up and my chest is tightening.”
A disconnect between the brain and body
All participants reflect on difficulties challenging their responses to movement, and unsuccessful attempts to rationalise the level of threat or “push through” the experience. Amber describes this as: a kind of disconnect between the narrative that I had in my head and what my body was telling me
Knowing there may not be any significant danger in a situation did not enable her to challenge these autonomic responses. Similarly, Donna reflects on her attempts to “tease out the logic” but states that “it [GrI responses] kind of defies” logic or reasoning. Lisa discusses thinking she had gained a sense of control over her responses to GrI until an experience where the chair was tilted back at the dentist. She states: I thought I was over that kind of past the, past, that point. And so that was a surprise. Like, oh no, that’s still there
Despite the sense that GrI responses may appear illogical, Rachel counters the idea of such responses as disproportionate. She advocates that the brain’s reaction is proportionate to the bodily experience: Actually it, the fear does fit the sensation. You know the sensation you're having and the way your body’s interpreting it, the fear does fit.
Moving from judgement to acceptance
This GET reflects the transition from self-judgement to self-compassion described by participants in the context of first becoming aware of GrI and gaining a rationale for their difficulties with movement
Self-imposed expectations
All participants describe varying levels of self-judgement and frustration in relation to their difficulties, often seeing GrI as being something they should have overcome or “grown out of” (Donna). These expectations were evident in comparison of themselves to others, who may appear more able, and could have a significant impact on their self-concept. Claire states: I always thought, well, how can I do that as easily as that person? Or why does this not bother them? So, I spent quite a lot of time beating myself up and thinking, um, I wasn’t good enough
Jenny reflects on how this led to a sense of othering, seeing herself as less competent than those around her when unable to join in with a high ropes activity: you compare yourself and you’re like I should be able. I should be up there doing that . . . definitely call yourself weak
In the absence of a clear explanation or rationale for why certain activities or experiences were more problematic, participants often describe themselves using negative terms such as “sensitive” (Rachel) and “stupid” (Lisa), reflective of internalised judgements that occurred in the absence of an explanation.
Self-compassion comes with understanding
When reflecting on how they first became aware that they experienced GrI, all participants described a sense of relief and acceptance at having an explanation. For Amber, this added insight enabled her to shift away from her self-judgement at avoiding certain activities: it’s like, aw God, like there are just so many reasons for me to not want to go to a hairdresser, and that’s OK
Lisa emphasises this is a particularly significant factor for adults, who she states will have more “baggage” than children. She highlights a key shift in mindset on becoming aware of GrI towards: that kind of self-acceptance part and the self-awareness part that oh, I’m not a problem.
Once participants had a reason for why certain activities held barriers, they were able to be kinder towards themselves and realise that as Claire states, “you don’t have to view yourself in that negative light.”
Learning to manage gravitational insecurity
This GET considers the strategies and responses participants had employed to manage or regulate their response to movement
Rather than limiting making choices
All participants describe strategies involving planning or prioritisation as being key in their experience of GrI. This included proactive avoidance of environments or situations that present too significant a challenge, with participants altering factors such as the route they might take or their method of travel. Donna discusses how she would arrange to meet in familiar places and plan her route to avoid challenges such as escalators and minimise the impact of GrI: I probably plan as well in advance, so I won’t have to . . . I’m not going to have to encounter that [GrI]
For Rachel, it was more about remembering that activities involving difficult movement experiences would require her to reduce her level of activity afterwards: It’s just me being mindful of recognising I might need recovery time or I might need to reduce distractions afterwards.
A shared experience was that GrI requires a need to prioritise. However, Amber reflects that rather than “limiting” she viewed this as “making choices” both to preserve her own well-being, and conserve energy for activities that were a priority. Similarly, Jenny describes a realisation that she had to “stop forcing [herself] to do something”.
Seeking out movement experiences
Five participants describe actively seeking out movement experiences, but with this manifesting in different ways for different individuals. Two participants suggest seeking movement to be a strategy they used to regulate after a more passive movement experience, such as travelling on a train or plane. Amber states: I really want to walk. Like so if, if at the end of the movement experience for whatever reason I have to stay still, um, that’s particularly uncomfortable
For some, this appeared to progress further to the active seeking of movement experiences they knew would be challenging to try and overcome their difficulties. Lisa discusses: my kids were doing gymnastics, I thought, right, I’m going to do some of this. Um, but I went in, completely terrified of going backwards, completely terrified of going forwards.
While Rachel also describes physically active hobbies, she states “the exercise I tend to do involves feet on the floor” suggesting a need for more controlled movement experiences. In contrast, Jenny reflects on enjoying a more passive movement experience of travelling in a lift, an activity that can be problematic in GrI. However, like Rachel, it is the element of control that is identified as important: I control it, I get in, I get out, I press the buttons.
A collective aspect of the activities described by the participants is being able to decide when the movement starts and stops, and that this is perhaps a feature in making it more manageable for them.
Discussion and implications
This is the first study to explore the lived experiences of individuals with GrI using a qualitative approach. Previous studies have explored GrI from a clinician’s viewpoint or using quantitative measures. Findings from this study begin to add to the evidence base, insight into how the features and impacts of GrI are perceived by those who experience it. Three GETs were identified from the findings: a not-so-disproportionate response; moving from judgement to acceptance; learning to manage gravitational insecurity.
A key distinguishing factor of GrI identified in the existing literature has been the fear presentation that is seen and described as “disproportionate” to the level of threat in the situation (Fisher and Bundy, 1989; May-Benson et al., 2020b). It is this response that distinguishes GrI from the dizziness or vertigo that may be evident in other vestibular-based conditions (Potegal, 2025). Participants in this study echoed this experience, describing the intensity of these responses that led to autonomic responses such as immobilisation and altered breathing. This echoes the observed autonomic, or freeze responses, reported by occupational therapists working in adult mental health settings in a study by Matson et al. (2025), suggesting such responses are also apparent in the general adult population. A new perspective offered by participants in this study reframes the idea of these responses as disproportionate, suggesting instead that “the fear does fit” (Rachel). While the threat may not be experienced or understood by those around the person, the sensory experience for an individual experiencing GrI is valid, and this is a factor that needs to be acknowledged. Without this acknowledgement, there is a risk of propagating misattributions of GrI responses as behavioural or personality related (Ayres, 2005; Coelho and Balaban, 2015) and increasing self-blame.
While some participants were already aware of their experience of GrI, others only identified this on seeing the study advert and completing the screening assessment. In both circumstances gaining an explanation and reframing for their difficulties was described as a significant factor by participants in this study that helped them move from a negative view of themselves as weak or sensitive to experiencing understandable responses. Participants described a sense of othering that came most strongly from their own self-imposed expectations and comparison to others, rather than the responses of others. Being able to reflect on and identify the impact of GrI in their lives decreased self-blaming, thereby highlighting the centrality of providing information about this sensory difference when working with individuals experiencing GrI. The importance of providing a language to describe experiences when supporting adults with GrI resonates with the existing literature in relation to both GrI specifically, and broader sensory processing differences (Forsberg et al., 2024; Matson et al., 2025; Miller et al., 2023; Williamson and Ennals, 2020).
While anxiety or fear were frequent experiences in response to movement for those with GrI, being able to take control through planning and preparation, or choosing specific sensory experiences, supported self-management. The idea of avoidance or withdrawal as a feature of GrI, as well as broader sensory processing differences in adults, is apparent in the existing literature (Matson et al., 2025; Pfeiffer, 2020; Potegal et al., 2022) However, participant responses in this study reframe this to a focus on taking control and prioritisation. Control has been suggested to be key in the regulation of sensory experiences in previous studies and literature that identify sensory experiences with an increased sense of predictability as easier to tolerate (Harrold et al., 2024; Kandlur et al., 2023; Maclennan et al., 2022).
Strategies used to support self-management have often been framed within sensory processing models using terms such as “sensitivity” and “avoidance” (Dunn, 2001) which, while it provides a system of categorisation to professionals, may risk reinforcing negative self-perspectives. MacLennan et al. (2022) suggest that while avoidance is often viewed as a maladaptive response, it may also be a key strategy for individuals with sensory processing differences. Participant responses in this study further this reframing to the idea of them taking control and “making choices” (Amber) that enable them to engage more fully in the occupations that are of value to them, moving away from a deficit focused view of their differences. Appreciating and identifying these responses is likely to be a key part of empowering those experiencing GrI within the therapeutic relationship. This taking of control also progressed to seeking out movements they found regulating or that would provide them with opportunities to challenge their sensory responses. Ayres (2005) describes this seeking of experiences as a “primal inner drive” that all humans possess to alter their responses and develop a sense of gravitational security. Occupational therapists with training in sensory integration are well placed to enable individuals to meet this “inner drive” through advising and facilitating engagement in valued activities.
Limitations
The authors acknowledge the inherent subjectivity of the approach used and that researcher interpretations within the study may differ from those that would be drawn by other researchers. All study participants identified as female, which, while this makes the sample more homogeneous as is desirable for IPA, leads to other genders not being represented. While a similar prevalence of GrI has been suggested between males and females, severity levels are thought to be significantly higher in females (May-Benson et al., 2016), which could have led to females being more readily able to relate to the indicators of GrI used in the recruitment advert. Another limitation is that as GrI often occurs alongside other sensory processing differences (May-Benson et al., 2016, 2020a), as is evident for the participants in this study with only one scoring in the typical range for overall sensory processing, identifying how much of the experiences described relate to GrI specifically is more of a challenge. In addition to this, while the co-occurrence of anxiety is acknowledged in the GrI literature (Potegal, 2025), this was not an exclusion criterion for this study, and it was not deemed necessary to ask participants to disclose details of any mental health conditions. Both researchers have experience of working in mental health settings with individuals experiencing gravitational insecurity and therefore were able to consider potential confounding factors of this in the analysis.
Conclusion
This study, while small scale, has begun to respond to a gap in the existing evidence base relating to GrI by providing insight into lived experiences and self-perceptions. The strong autonomic responses reported by participants, combined with the difficulties in challenging these responses, support the significant potential impact of GrI on well-being and occupational engagement. There is a need for increased awareness and knowledge of GrI to enable self-management and decrease negative self-perceptions. Occupational therapists have a key role in responding to this through supporting reframing of sensory differences, and enabling the identification of activities that are regulating, as well as those that provide a “just-right” challenge in developing increased gravitational security.
Key findings
Providing information to support self-understanding is key when working with individuals experiencing gravitational insecurity.
Framings of gravitational insecurity as disproportionate, risk negating the bodily experience and suggests the need for a neuro-affirmative definition.
Identification of movement activities at the right level could support self-management and increase feelings of control.
What the study has added
Insight into the lived experiences of adults with gravitational insecurity suggests a potential role for occupational therapists in supporting a positive reframing and increased self-compassion.
Footnotes
Acknowledgements
The authors would like to acknowledge the important role of the PPI group in developing the study materials to be accessible and support insight into the personal experience of GI. Thank you also to Dr Anne-Louise Humphreys for her support in the ethics process, and to the participants who so willingly shared their reflections and experiences.
Ethical considerations
Ethical approval for this study was granted by the IPH-REC, University of Liverpool, ref 14333.
Consent to participate
Informed consent to participate was obtained from participants through an online form and revisited verbally at the commencement of the interviews.
Author contributions
RM conceptualisation of the study, development of study materials, ethics, data collection, analysis, drafting the manuscript. KF development of study materials, data collection, analysis, review of manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding support was received from the Elizabeth Casson Trust pump-priming award to support PPI involvement within this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Patient and public involvement data
During the development, progress, and reporting of the submitted research, Patient and Public Involvement in the research was included at all stages of the research.