
Abstract
Introduction:
Depression and loneliness are common mental health concerns among older adults and are associated with reduced quality of life and daily functioning. Understanding how satisfaction with the residential environment relates to these outcomes may inform approaches to support well-being and aging in place.
Method:
This cross-sectional study analyzed data collected from 89 community-dwelling older adults residing in the southeastern United States. Residential environmental satisfaction (RES), depression, and loneliness were measured using the Residential Environmental Satisfaction Scale, Beck Depression Inventory, and UCLA Loneliness Scale, respectively. Stepwise linear regression analyses examined associations between RES and depression and loneliness, adjusting for age, sex, and education.
Results:
RES and age were significantly associated with both depression and loneliness (p < 0.05). RES explained an additional 7.2% of the variance in depression (p < 0.001) and 11.2% of the variance in loneliness (p = 0.007) beyond demographic factors. Lower RES was associated with higher levels of depressive symptoms and loneliness.
Conclusion:
Perceived satisfaction with one’s home and neighborhood was significantly associated with depression and loneliness among community-dwelling older adults. These findings highlight RES as an important contextual factor to consider when supporting mental well-being and aging in place in later life.
Introduction
The population of older adults is increasing rapidly worldwide, including in the United States, where 58 million individuals aged 65 years or older lived in 2022, and this number is projected to rise substantially over the coming decades (Administration for Community Living, 2024; U.S. Census Bureau, 2020). Older adults already outnumber children in several regions of the country (U.S. Census Bureau, 2025), reflecting a broader global trend toward population aging. The demographic shifts highlight the substantial caregiving burden that may be placed on future generations and underscore the critical importance of developing strategies to support healthy aging and promote aging in place.
Findings from both a longitudinal qualitative study and a systematic review indicate that the home is strongly associated with identity, freedom, autonomy, and community connectedness for older adults (Bolster-Foucault et al., 2024; Gibson et al., 2024). Nearly all older adult participants express a preference to age in place, even when facing physical health challenges or experiencing social and economic disadvantages (Bolster-Foucault et al., 2024; Gibson et al., 2024). Although aging in place offers comfort and familiarity, the risks of social isolation and loneliness – exacerbated by mobility limitations and limited technology literacy – pose significant threats to older adults’ health, particularly among those with disabilities (Donovan and Blazer, 2020; Pollak et al., 2025). Research has shown that, on average, nearly one in three older adults experiences depression or loneliness (Cai et al., 2023; Gerlach et al., 2024), and even among those who remain at home, prevalence rates of loneliness are as high as 25% (one in four; Salari et al., 2025).
Depression and loneliness have been consistently associated with reduced quality of life, impaired daily functioning, poorer physical health outcomes (e.g., cognitive decline, chronic pain, cardiovascular disease), and adverse psychological outcomes (e.g., suicidal ideation, anxiety; Jalali et al., 2024; Salari et al., 2025). To reduce the impact of depression and loneliness among community-dwelling older adults, a variety of strategies have been developed and implemented. Several systematic reviews and meta-analyses have demonstrated that interventions – such as psychotherapy, cognitive behavioral therapy, animal-assisted therapy, music therapy, reminiscence therapy, and exercise – are generally effective in reducing depression and/or loneliness (Elhag et al., 2025; Hoang et al., 2022; Morgado et al., 2024; Patil and Braun, 2024). However, many of these studies involved relatively small samples or reported only small effect sizes (Hoang et al., 2022; Patil and Braun, 2024). More importantly, most interventions have focused narrowly on individual-level factors (e.g., physical activity, self-care education, reminiscence life review, chronic disease self-management) and have largely overlooked environmental and contextual influences.
Initiatives such as Naturally Occurring Retirement Community supportive service programs (Hou and Cao, 2021; Parniak et al., 2022), Village models (Greenfield et al., 2013), and age-friendly community efforts (Hong et al., 2023; Kim et al., 2022) have emerged to promote aging in place and social participation. While these approaches address community-wide supports and environmental conditions, evidence of their effects on mental health outcomes such as depression and loneliness remains mixed and limited (Hong et al., 2023; Parniak et al., 2022). In particular, a recent poll found that the proportion of older adults feeling a lack of companionship remained relatively unchanged, from 33.9% in 2018 to 33.4% in 2024 (Malani et al., 2025). This persistence underscores the limitations of current approaches and highlights the urgent need for additional, potentially innovative strategies.
Residential environmental satisfaction (RES) refers to an individual’s overall contentment with their living environment, encompassing both the physical and social dimensions of the home and neighborhood. It reflects the extent to which the environment supports daily needs, independence, safety, and social connectedness. Prior studies have shown that aspects of the physical environment and dwelling characteristics – such as natural sunlight, ventilation, floor level, and house size – as well as neighborhood features, including familiarity and community security, are significantly associated with depressive symptoms (Chen et al., 2021; Sharifi et al., 2024). RES is also negatively associated with loneliness (Prieto-Flores et al., 2011; Sharifi et al., 2024); for example, poor housing quality (e.g., problems with plumbing or heating) and low neighborhood cohesion have been identified as significant predictors of loneliness (Gan et al., 2022; Lin et al., 2024).
Although previous studies have identified associations between the residential environment and depression and/or loneliness, most of them have focused primarily on physical dimensions or objective housing characteristics rather than on individuals’ self-perceived satisfaction with their living environment. The person–environment–occupation (PEO) model (Law et al., 1996) and the person–environment–occupation–performance (PEOP) model (Baum et al., 2015), both fundamental client-centered frameworks in occupational therapy, posit that well-being emerges from the dynamic interaction among the person, environment, and occupation, thereby influencing participation in meaningful activities. In this context, the residential environment represents a critical component of the environment domain, shaping opportunities for daily engagement, social interaction, and independence. Perceived satisfaction with the residential environment may therefore reflect the degree of person-environment fit and, in turn, influence psychological outcomes such as depression and loneliness. However, despite this theoretical relevance, limited research has examined how subjective residential satisfaction relates to mental health outcomes in older adults, and the association between RES and depression or loneliness has not been well established.
The purpose of this study was to examine the contribution of perceived RES to depression and loneliness among community-dwelling older adults using regression models. The Residential Environmental Satisfaction Scale (RESS) was selected to emphasize subjective evaluations of the dwelling and neighborhood environment, including maintenance, convenience, ambiance, and the quality of neighborhood relationships and cohesion. By investigating RES, this study aims to address a critical gap in the literature and provide evidence that is directly applicable to occupational therapy. The findings may inform innovative, contextually grounded interventions that promote mental well-being and support healthy aging in place for the rapidly growing older adult population.
Methods
Study design
This study was a cross-sectional design with a total of four waves of data collection across four continuous years from 2020 to 2023 with community-dwelling older adults in the United States. Participants were visited at home one time and asked to complete demographic information and outcome assessments.
Participants
Ninety-five community-dwelling older adults were enrolled in the study. Inclusion criteria of the participants were as follows: (a) being 60 years or older, (b) residing at home, and (c) having sufficient cognitive ability to answer the study questions. Participants were recruited using convenience sampling and community-based outreach methods. Recruitment sources included local nonprofit organizations in the Greater Atlanta area in the southeastern U.S. (e.g., independent living communities and Meals on Wheels Atlanta), personal networks of study personnel, and word-of-mouth referrals. Eligible individuals were provided with recruitment flyers (e.g., posted on bulletin boards) or referred directly to the study team. All interested individuals were contacted by the study team, provided with study information, and enrolled after providing written informed consent.
During the strict lockdown period of the COVID-19 pandemic (March–June 2020), participant recruitment and home visits were temporarily suspended. Following this period, home visits gradually resumed only when participants explicitly agreed and felt comfortable, with appropriate safety precautions (e.g., masking). The pace of data collection was affected but fully resumed in 2022.
Procedures
After confirming eligibility, the study team scheduled a home visit with each enrolled participant. During the visit, participants completed demographics (e.g., age, gender, education, and years of residence) and the following outcome measures.
Outcome measures
Residential environmental satisfaction
The RESS is a multidimensional self-report instrument developed to assess residents’ perceived satisfaction with their living environment. It uses a 5-point Likert scale to assess three domains: dwelling satisfaction, internal neighborhood reputation, and residential social climate, with higher scores indicating greater satisfaction (Adriaanse, 2007). Psychometric testing demonstrated strong reliability and construct validity, supporting its use as a robust measure of residential satisfaction (Adriaanse, 2007).
Depression
The Beck Depression Inventory (BDI) is a widely used self-report instrument designed to assess the severity of depressive symptoms in clinical and research settings. It consists of 21 items that capture cognitive, affective, and somatic aspects of depression (Beck et al., 1961). Each item is rated on a 4-point scale, with higher scores indicating greater depression severity. The BDI has demonstrated strong psychometric properties, including high internal consistency and good construct validity across diverse populations (Beck et al., 1988; Wang and Gorenstein, 2013).
Loneliness
The UCLA Loneliness Scale is a self-report instrument designed to assess subjective feelings of loneliness and social isolation. It captures the frequency of perceived social disconnection through 20 items rated on a 4-point Likert scale, with higher scores indicating greater loneliness (Russell, 1996). The scale has demonstrated strong psychometric properties, including high internal consistency, test–retest reliability, and robust convergent and discriminant validity across diverse populations (Russell, 1996; Vassar and Crosby, 2008).
Statistical analysis
Bivariate correlations were conducted to examine associations among demographic characteristics (age, sex, and education), RESS, depression (BDI), and loneliness (UCLA Loneliness Scale). Pearson’s correlations were used for continuous variables. Differences in depression and loneliness by sex were further examined using an independent t-test. One-way analyses of variance (ANOVAs) were also performed to evaluate group differences in depression and loneliness across education levels, categorized into seven groups (some high school, high school diploma, some college, associate’s degree, bachelor’s degree, master’s degree, and doctorate). Post hoc comparisons were conducted using Bonferroni adjustments to control multiple testing.
Stepwise linear regression within blocks was conducted in a theory-guided sequence to examine whether satisfaction with the living environment was associated with older adults’ depression and loneliness. Demographic variables (age, gender, and education) were entered first as a candidate block, given their established associations with depression and perceived loneliness in older adults (Djernes, 2006; Hawkley and Cacioppo, 2007; Ross and Mirowsky, 2006; Wetherell et al., 2001). The RESS score was then added to evaluate its incremental contribution to BDI and UCLA Loneliness Scale scores. Model comparisons were conducted using changes in explained variance (ΔR2) to determine whether the inclusion of RESS significantly improved model fit. Multicollinearity was assessed using variance inflation factors (VIF). A VIF value greater than 5 was considered indicative of potential collinearity.
All statistical analyses were conducted using IBM SPSS Statistics (Version 31.0.0; IBM Corp., 2023), with the significance level set at α = 0.05.
Results
Participants
To ensure participants had sufficient experience to accurately reflect on their living environment satisfaction, we excluded individuals who had lived in their current residence for less than 1 year. Specifically, four participants (M = 5.25, SD = 0.96 months; range 4–6 months) were excluded from the 95 participants recruited. In addition, two participants were excluded as statistical outliers (>3 interquartile ranges). Table 1 presents the characteristics of the final sample of 89 community-dwelling older adults.
Characteristics of participants (n = 89).
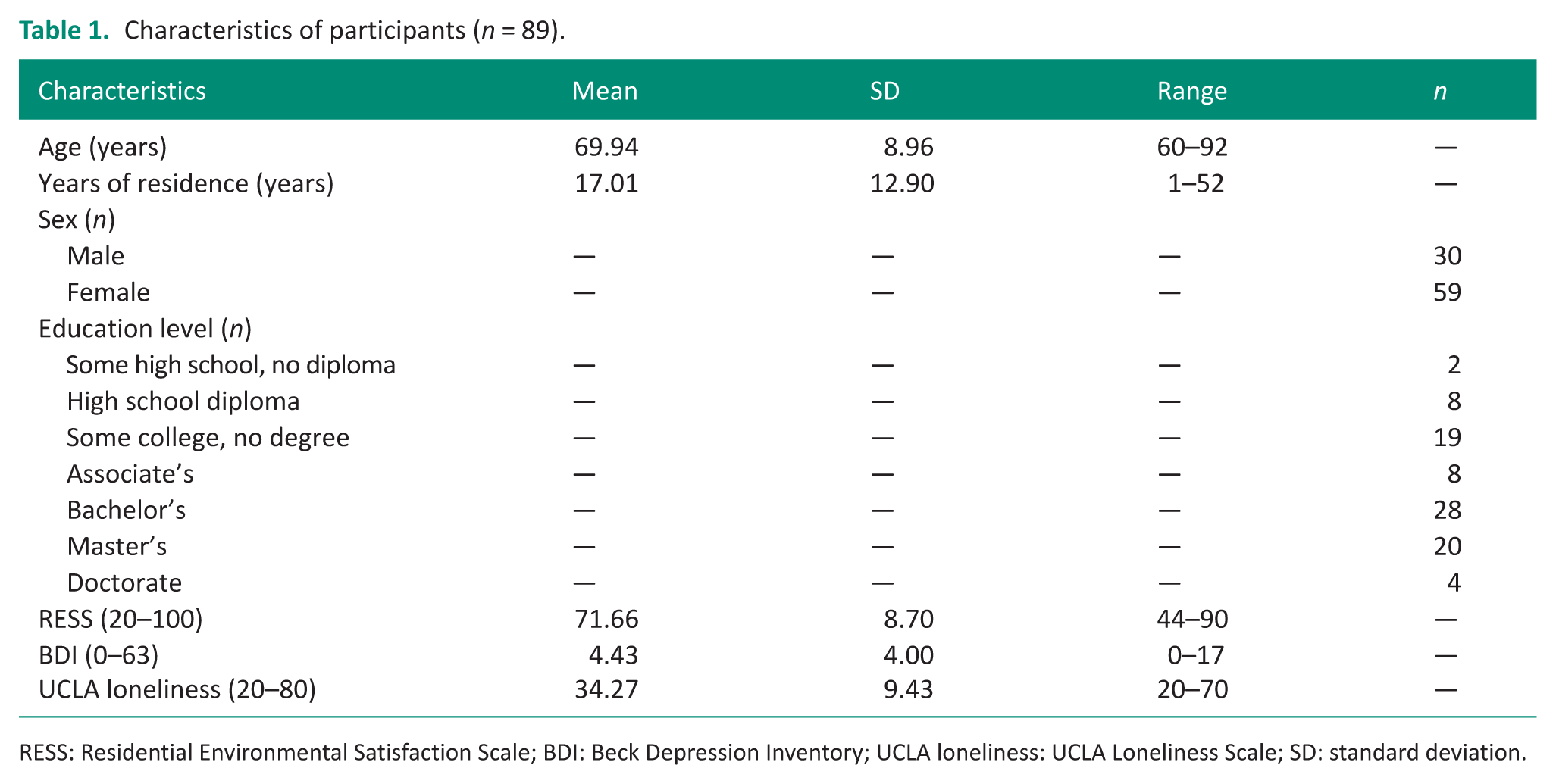
RESS: Residential Environmental Satisfaction Scale; BDI: Beck Depression Inventory; UCLA loneliness: UCLA Loneliness Scale; SD: standard deviation.
Depression
Bivariate correlations
Bivariate correlations are presented in Table 2. Age was positively correlated with BDI scores (r = 0.28, p = 0.007), indicating that older participants reported higher levels of depressive symptoms. Independent t-tests indicated that female participants reported significantly higher BDI scores (M = 5.12, SD = 4.01) than male participants (M = 3.04, SD = 3.66, t = −2.35, p = 0.021). Results of the one-way ANOVA also showed that education level was significantly associated with BDI scores (F6, 82 = 2.58, p = 0.025). Post hoc comparisons using Bonferroni adjustment indicated that individuals with less than a high school diploma reported significantly greater depressive symptoms (M = 14.50, SD = 0.71) than those with a bachelor’s degree (M = 4.32, SD = 3.66, p = 0.009) or a master’s degree (M = 3.95, SD = 4.14, p = 0.009), while no other pairwise comparisons were significant.
Bivariate correlations among study variables (n = 89).
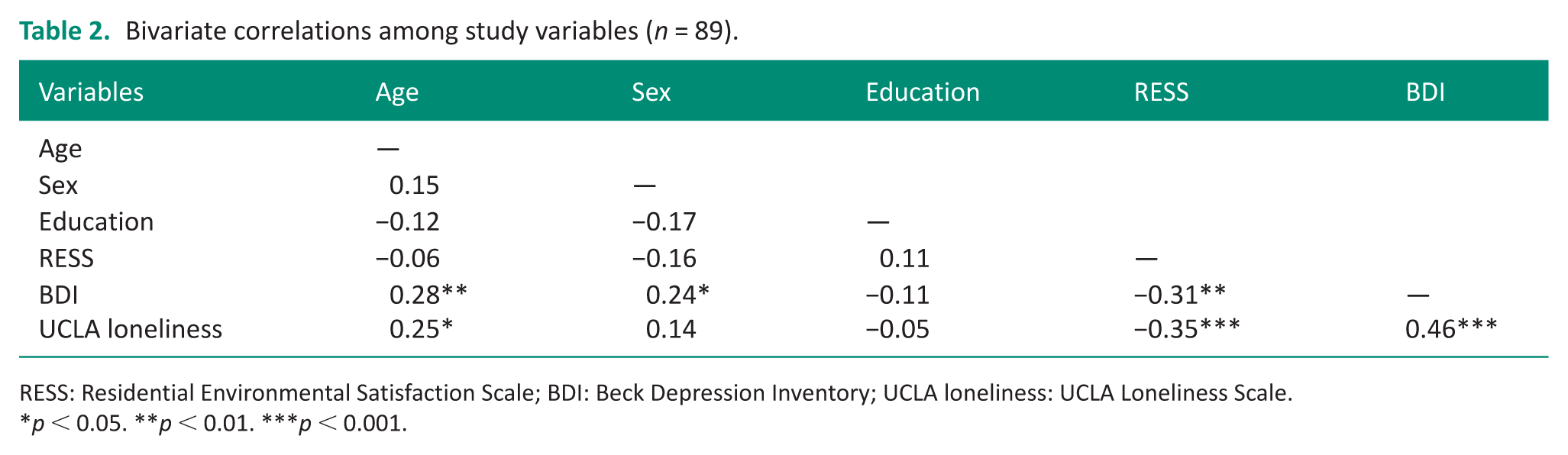
RESS: Residential Environmental Satisfaction Scale; BDI: Beck Depression Inventory; UCLA loneliness: UCLA Loneliness Scale.
p < 0.05. **p < 0.01. ***p < 0.001.
Finally, RESS was negatively correlated with BDI scores (r = −0.31, p = 0.003), such that higher residential satisfaction was associated with fewer depressive symptoms.
Stepwise linear regressions
After entering the demographic variables (age, gender, and education) into the stepwise regression, the initial model retained age as the only variable significantly associated with BDI scores (p = 0.007; Table 3; model 1). This model accounted for 7% of the variance in depressive symptoms (R2 = 0.07), indicating that older age was associated with higher levels of depression. Sex was retained in the subsequent model and was significantly associated with depressive symptoms (p = 0.004; R2 = 0.102; Table 3; model 2). Compared to model 1, model 2 explained an additional 4.1% of the variance following the inclusion of sex (ΔR2 = 0.041, F1,86 = 4.07, p = 0.047).
Stepwise linear regression predicting depression (BDI).
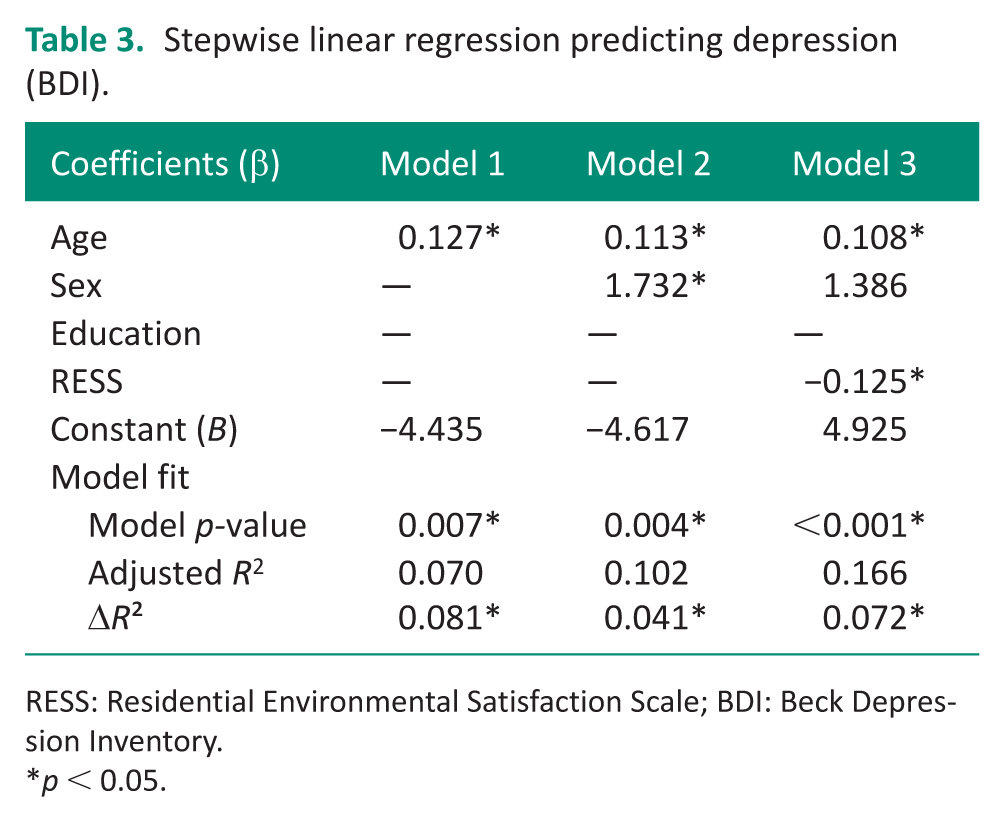
RESS: Residential Environmental Satisfaction Scale; BDI: Beck Depression Inventory.
p < 0.05.
When RESS was added to the model, both age and RESS were significantly associated with BDI scores (p < 0.05; Table 3; model 3), and the model explained 16.6% of the variance (R2 = 0.166). Specifically, older age and lower RES were associated with higher levels of depressive symptoms. Although sex remained in the model, it was no longer significantly associated with depressive symptoms, likely due to shared variance with age and RESS. VIF values for all variables across models ranged from 1.00 to 1.05, indicating no evidence of problematic multicollinearity. Importantly, compared to model 2, model 3 significantly explained an additional 7.2% of the variance (ΔR2 = 0.072, F1,85 = 7.64, p = 0.007), demonstrating that RES contributed uniquely to explaining depressive symptoms and significantly improved model fit.
Loneliness
Bivariate correlations
Age was also positively correlated with UCLA loneliness scores (r = 0.25, p = 0.016; Table 2), indicating that older participants tended to report higher levels of loneliness. Sex (t = −1.32, p = 0.19) and education (F6, 82 = 0.91, p = 0.491) were not significantly associated with UCLA loneliness scores, suggesting no meaningful group differences in loneliness by gender or education. In contrast, RESS was negatively correlated with UCLA loneliness scores (r = −0.35, p < 0.001), indicating that greater residential satisfaction was associated with lower levels of loneliness.
Stepwise linear regressions
After entering the demographic variables (age, sex, and education) into the stepwise regression, the initial model retained age as the only variable significantly associated with UCLA loneliness scores (p = 0.016; Table 4; model 1). This model explained 5.4% of the variance in loneliness (R2 = 0.054), suggesting that older age was associated with greater loneliness.
When RESS was added to the model, both age and RESS were significantly associated with UCLA loneliness scores (p < 0.001; Table 4; model 2), and the model accounted for 15.8% of the variance (R2 = 0.158). Specifically, older age and lower RES were associated with higher loneliness scores. Model comparison indicated that adding RESS significantly improved model fit relative to model 1, accounting for an additional 11.2% of the variance (ΔR2 = 0.112, F1,86 = 11.74, p < 0.001). No evidence of problematic multicollinearity was observed.
Stepwise linear regression predicting loneliness (UCLA loneliness).
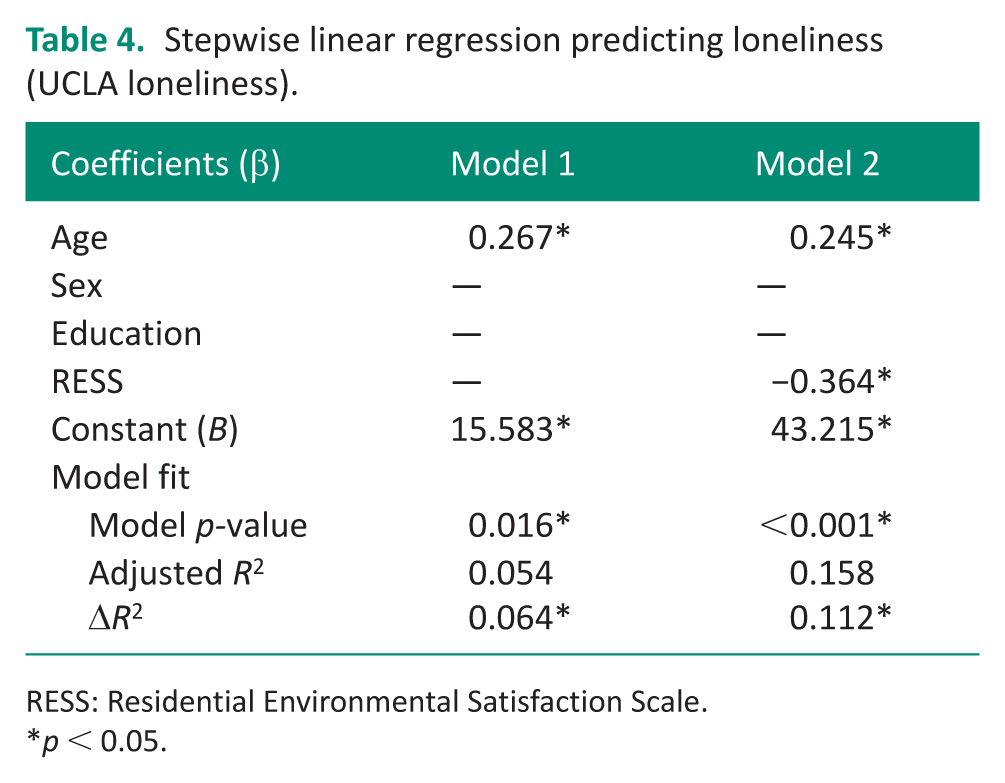
RESS: Residential Environmental Satisfaction Scale.
p < 0.05.
Discussion
This study examined the association between self-perceived satisfaction with the residential environment and depression and loneliness among community-dwelling older adults. Our regression results demonstrated that both age and RES were significantly associated with depressive symptoms and feelings of loneliness. Community dwellers who are older and report lower satisfaction with their residential environment were more likely to experience depression and loneliness. Although sex was initially associated with depressive symptoms, this association was no longer significant after including RES, suggesting a potential interaction between sex and environmental perceptions that warrants further investigation. Most importantly, model comparison tests indicated that RESS explained significant additional variance in depression and loneliness beyond demographic factors (e.g., age) alone.
Our findings align with previous studies associating housing quality and characteristics with depression and loneliness (Chen et al., 2021; Prieto-Flores et al., 2011; Sharifi et al., 2024) and are consistent with research showing associations between neighborhood satisfaction and depressive symptoms or social isolation in older adults (Gan et al., 2022; Lin et al., 2024). We further extended prior work by using the RESS to demonstrate that perceived residential satisfaction, encompassing both home and neighborhood environments, is significantly associated with depression and loneliness. These findings underscore the importance of subjective satisfaction of environmental and contextual factors when examining mental health outcomes in older adults.
Given the cross-sectional design of this study, the directionality of the associations among RES, depressive symptoms, and loneliness cannot be determined. It is possible that lower RES contributes to increased depression and loneliness by limiting engagement and social participation. Conversely, individuals experiencing higher levels of depression or loneliness may perceive their residential environment less favorably due to mood-related biases. These relationships suggest a potentially bidirectional relationship among RES, depression, and loneliness. However, this interpretation should be considered in light of the overall low levels of depressive symptoms and loneliness observed in our sample. Mean BDI and UCLA loneliness scores were 4.43 and 34.27, respectively (Table 1), both well below commonly used clinical cutoffs (BDI ⩾14; UCLA ⩾44), indicating minimal depressive symptoms and loneliness. This suggests that RESS in this community-dwelling sample may primarily reflect environmental perceptions rather than being driven by their emotional state or mood. Nonetheless, longitudinal and experimental studies are needed to better understand these relationships.
In addition, as most participants reported relatively low levels of depression and loneliness, the limited clinical variability, which may reflect a floor effect for the BDI (18 of 89 participants scored 0) and a potential floor effect for the UCLA Loneliness Scale (12 participants scored ⩽24), may have reduced the ability to detect stronger associations and may limit the generalizability of the findings to populations with more severe symptoms. Future studies should include more heterogeneous samples with a broader range of symptom severity, including individuals with moderate to severe depression and loneliness.
On an important note, depression and loneliness are highly correlated, as demonstrated in previous studies (Donovan and Blazer, 2020; Gan et al., 2022; Gerlach et al., 2024; Hawkley and Cacioppo, 2007; Pollak et al., 2025; Prieto-Flores et al., 2011; Salari et al., 2025), as well as our correlation results (r = 0.46, p < 0.001; Table 2). Research has shown that loneliness can predict depression (Luo, 2022; Mann et al., 2022; Wister et al., 2023) and vice versa (Luo, 2022; McHugh Power et al., 2020), suggesting a bidirectional relationship between these two psychological constructs (Chen et al., 2023; Ward et al., 2023). Because the purpose of this study was not to examine how these two factors interact, given the overlap in their underlying structure, we did not include both variables in the same regression model. Instead, we analyzed them separately to highlight the significance of each as a commonly measured key mental health outcome in older adults. This approach allowed us to more clearly identify and address the critical role of RES for each essential health outcome.
RES captures a sense of functionality, attachment, and belonging within the home and neighborhood. Older adults’ perceptions of their living environment may influence their psychological well-being, with supportive environments linked to better outcomes and inadequate or isolating environments associated with greater vulnerability to depression and loneliness. This interpretation is consistent with theoretical frameworks, such as the PEO model (Law et al., 1996) and the PEOP model (Baum et al., 2015), which emphasize that well-being arises from interaction and fit between individuals and their environments. Within these frameworks, RESS can be conceptualized as an indicator of perceived person–environment fit, reflecting both intrinsic perceptions (e.g., security, belonging) and extrinsic factors (e.g., home functions, neighborhood cohesion). Higher RESS may reflect environments that better support engagement in meaningful activities and social participation, which are associated with reduced risk of depression and loneliness. Conversely, lower RESS may indicate environmental barriers that limit participation and increase social isolation, thereby contributing to poorer mental health outcomes. In this way, the associations observed between RESS and both depression (BDI) and loneliness (UCLA) are consistent with the theoretical mechanisms proposed by PEO. Thus, RES represents not only a subjective appraisal of the residential environment but also a potentially modifiable factor contributing to overall well-being for older adults.
In our regression models, RESS significantly explained an additional 7–11% of the variance in depression and loneliness, while the overall R2 values remained modest (16–17%). This finding is consistent with prior research indicating that mental health outcomes in older adults are influenced by a broad constellation of factors operating across individual, social, health, and environmental domains (Blazer, 2003; Fiske et al., 2009). The substantial unexplained variance likely reflects the influence of other unmeasured factors, including social support, physical health status, functional ability, chronic disease burden, life events, socioeconomic conditions (e.g., financial strain), personality traits, and coping resources, all of which may influence mental health and interactions with the residential environment. From this perspective, the observed results suggest that RES represents an important, but not singular, contributor to depression and loneliness within a multifactorial framework. Future studies incorporating additional physical, psychosocial, and contextual variables are needed to further elucidate these multilevel and complex relationships.
Implications for occupational therapy practice
While aging itself cannot be prevented, interventions and strategies can be designed to enhance older adults’ perceived satisfaction with their residential environment, offering a potential modifiable pathway to improve mental health and support aging in place. Integrating RES into clinical practice aligns with the holistic perspective of occupational therapy, which emphasizes the dynamic interaction among individuals, their environments, and their participation in meaningful activities. By exploring how older adults perceive their home and neighborhood environments, occupational therapists (OTs) can be better positioned to identify environmental and contextual factors that influence well-being, including issues related to safety, independence, and social connection. Consideration of RES may complement existing environmental and occupational assessments by providing insight into older adults’ lived experiences of their residential contexts, beyond objective features of the built environment alone. Interventions informed by this perspective may include home modifications that address not only safety and functional independence but also comfort and personal meaning, as well as adaptive and flexible use of home space and strategies to support meaningful activities, social participation, and neighborhood engagement.
Although RES measure shows promise for informing intervention planning and evaluating environmental influences on mental health and participation, their routine use as clinical outcome measures may require further development and validation to ensure feasibility, interpretability, and relevance within everyday occupational therapy practice. Future work is needed to develop, refine, and test such measures for clinical application and to determine how assessments of RES can best be integrated into occupational therapy evaluation and outcome monitoring.
Beyond practice, consideration of RES may also inform housing policy and community design efforts aimed at supporting healthy aging in place and ultimately reducing caregiving demands on future generations. As measures of RES continue to be refined and validated, they may have the potential to inform both research and practice by helping OTs track how perceived environmental changes relate to mental health and participation over time. OTs are uniquely positioned to collaborate with architects and public health professionals to ensure that older adults’ perspectives are meaningfully integrated into community-level decisions that shape residential environments and satisfaction.
Limitations
The present study has several limitations. First, the sample was drawn primarily from the metro-Atlanta area in the United States, and the relatively modest sample size may limit the generalizability of findings to other geographic or cultural contexts. Second, most participants reported depression and loneliness scores within the mild range; therefore, future studies would benefit from including more individuals with moderate to severe symptoms to better capture variability in outcomes. Research using larger and more diverse samples across geographic, cultural, and clinical contexts may further strengthen the understanding of the mechanisms linking RES to mental health. In addition, this study relied solely on quantitative measures and did not capture participants’ in-depth personal experiences or perceptions of their residential environment. Future studies incorporating qualitative approaches may help expand upon our findings and provide a deeper understanding of participants’ lived experiences, as well as better account for factors influencing depression and loneliness that were not fully addressed in this study, such as the COVID-19 pandemic and individual health conditions.
Conclusion
This study demonstrated that satisfaction with residential environment is significantly associated with depression and loneliness among community-dwelling older adults in the United States, even after accounting for demographic factors. Older adults who reported lower satisfaction with their home and neighborhood environments were more likely to experience higher levels of depressive symptoms and social isolation, underscoring the importance of subjective perceptions of residential place in relation to mental health.
Consideration of RES highlights the potential value of addressing both physical and psychological aspects of the residential environment when supporting healthy aging in place. By incorporating older adults’ perceptions of their living environments into assessment and intervention, OTs may address environmental and contextual factors that influence participation and well-being. At a broader level, these findings suggest that RES represents a relevant consideration for community planning and housing policy efforts aimed at improving mental health outcomes in the growing older adult population.
Key findings
Lower residential environmental satisfaction was associated with higher depression and loneliness among older adults.
Residential environmental satisfaction significantly explained additional variance in depression and loneliness beyond demographic factors.
What the study has added
This study highlights residential environmental satisfaction as an important contextual factor associated with depression and loneliness, extending existing evidence beyond objective housing features to include older adults’ subjective environmental experiences.
Footnotes
Ethical considerations
This study was reviewed and approved by the Georgia State University IRB (Approval No.: H18154).
Consent to participate
Written informed consent to participate in the study was obtained from all participants prior to data collection.
Consent for publication
Written informed consent for publication of de-identified study data was obtained from all participants.
Author contributions
YC contributed to protocol development, data analysis, and drafting of the manuscript. AR and CL contributed to participant recruitment, data collection, and data organization. KM contributed to protocol development and obtaining ethical approval. All authors reviewed the manuscript and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by the Georgia State University Brains and Behavior Seed Grant (2022–2023).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Patient and public involvement data
During the development, progress, and reporting of the submitted research, Patient and Public Involvement in the research was not included at any stage of the research.