
Abstract
Introduction:
Individuals with paraplegic spinal cord injury (SCI) experience multiple challenges in daily life participation, significantly impacting their quality of life (QOL). Understanding the determinants of participation and their association with QOL is crucial for guiding rehabilitation strategies in low-resource settings like Pakistan.
Method:
A cross-sectional study of 140 individuals with paraplegic SCI was conducted in rehabilitation centres across Pakistan. Participation was measured using the World Health Organization Disability Assessment Schedule 2.0 (WHODAS-II), environmental barriers with the Craig Hospital Inventory of Environmental Factors–Short Form (CHIEF-SF), and QOL with the WHOQOL-BREF.
Results:
Participants were predominantly male (97.9%), with a mean age of 35 years. The majority sustained traumatic injuries, primarily due to gunshots and motor vehicle accidents. Employment status, supportive environments, and neurological impairment significantly influenced participation. A moderate negative correlation was found between WHODAS-II total scores and WHOQOL-BREF scores (r = −0.586, p < 0.001), indicating that higher levels of disability were associated with lower QOL among individuals with paraplegic SCI.
Conclusion:
Employment status and supportive environments are modifiable factors that can enhance participation, ultimately improving QOL for individuals with paraplegic SCI in Pakistan. Addressing these factors can lead to better rehabilitation outcomes.
Introduction and literature review
Spinal cord injury (SCI) is a significant global health concern, affecting an estimated 250,000–500,000 people annually worldwide, according to the World Health Organization (WHO) (James et al., 2019). In Pakistan, the incidence is among the highest in lower- and middle-income countries, with a large proportion of cases occurring in young adult males due to high-risk behaviours, unsafe working conditions, and violence (Khan et al., 2017). Recent findings further identify falls, road traffic accidents, and firearm-related incidents as leading causes, with many individuals experiencing substantial dependence in activities of daily living (Bibi and Naeem, 2025).
SCI may be classified as traumatic or non-traumatic. Traumatic SCI, resulting from sudden mechanical injury to the spinal cord, is associated with high morbidity and mortality (Jaffar et al., 2022). In Pakistan, traumatic SCI care remains underdeveloped, with limited access to specialised surgical and rehabilitation services and notable gaps in infrastructure and workforce capacity (Ullah et al., 2024). By contrast, non-traumatic SCI arises from conditions such as tuberculosis, tumours, infections, vascular malformations, and degenerative diseases (Ullah et al., 2023). Within this context, paraplegia accounts for approximately 90% of SCI cases, while tetraplegia represents about 10% (Darain et al., 2017). The severity of SCI is determined by neurological impairment, which influences the extent of paralysis, sensory loss, and disability levels below the injury site (Harvey, 2016). The American Spinal Injury Association (ASIA) classifies SCI as either complete or incomplete. A complete SCI results in the total loss of sensory and motor function below the injury level, whereas an incomplete SCI allows for partial preservation of these functions (Craig et al., 2015).
Following hospital discharge, individuals with paraplegic SCI face multiple challenges, including loss of independence, psychological distress, depression, and difficulties with community reintegration (Ekelman et al., 2017). Participation in daily life activities encompassing work, education, social interaction, and recreation is central to rehabilitation and overall well-being (Larsson-Lund and Nyman, 2017). Environmental barriers, such as inaccessible infrastructure, inadequate transportation, and limited social support, further constrain participation (Vessby and Kjellberg, 2010). Occupational therapy interventions, environmental modifications, and assistive technologies are vital for enhancing functional independence and community participation (Kielhofner, 2008).
The WHO defined as an individual’s perception of their position in life within the context of culture, values, goals, and expectations (Ferdiana et al., 2018). Individuals with paraplegic SCI often experience a significant decline in quality of life (QOL) due to physical, psychological, environmental, and social factors. Physical challenges include neurogenic bladder and bowel dysfunction, pressure ulcers, respiratory complications, and cardiovascular risks. Psychological difficulties such as depression, stress, and coping challenges further compromise QOL, while social issues, including relationship strain, isolation, and financial instability, exacerbate these difficulties (Sajid et al., 2020). Environmental barriers, including limited public access and inadequate transportation, add further restrictions to participation and diminish QOL (Saeed et al., 2024).
Despite global recognition of these issues, determinants of daily life participation among individuals with paraplegia remain understudied, particularly in low-resource settings such as Pakistan. A previous study has shown that individuals with paraplegic SCI experience substantial difficulties in social participation, life activities, and mobility, which are associated with reduced QOL (Khanzada et al., 2023). Additionally, limited research has examined the relationship between participation and QOL, particularly in Pakistan (Amsters et al., 2022). As individuals with paraplegic SCI now live longer, they are more likely to experience functional limitations and participation restrictions, which can negatively impact QOL, alongside an increased risk of secondary health conditions related to ageing and psychological distress (Lundström and Dashner, 2023; Mulla et al., 2022). Understanding how participation interacts with environmental, body functions, and contextual factors is essential for guiding rehabilitation strategies, improving community reintegration, and informing interventions to enhance long-term outcomes (Cole et al., 2023; Geyh et al., 2012; Khanzada et al., 2024b). Therefore, this study aimed to identify the determinants of daily activity participation and examine its relationship with QOL among individuals with paraplegic SCI in Pakistan.
Methods
Participants
This cross-sectional study recruited individuals with paraplegic SCI in Pakistan using a purposive sampling technique (Wang and Cheng, 2020). The participants were individuals with traumatic and non-traumatic paraplegic SCI living in the community and receiving follow-up rehabilitation services as outpatients at various rehabilitation centres in Pakistan (Creswell and Clark, 2017). The sample size was determined using G*Power 3.1.9 software, based on an alpha level of 0.05, a power of 0.8, and a medium effect size of 0.15 to identify the determinants of participation, as reported in a previously published study (Faul et al., 2009). A total of 140 participants were required. Participants were included if they had paraplegic SCI affecting the thoracic (T1–T12), lumbar (L1–L5), or sacral (S1–S7) spinal regions. Individuals with secondary medical conditions such as psychiatric illness, cognitive deficits, behavioural issues, or other neurological disorders affecting daily life participation were excluded. Additionally, individuals with communication or comprehension impairments hindering questionnaire completion, as well as those who declined participation, were excluded.
Ethical approval was obtained from the Ethics Committee of Universiti Teknologi MARA, Malaysia (Ref. no: 600-TNCPI (5/1/6)) and the National Bioethics Committee for Research, National Institute of Health, Pakistan (Ref. no: NBC-922/23/1546). Written informed consent was obtained from all participants before the study commenced.
Data collection
Data collection was conducted over 1 year at multiple outpatient rehabilitation centres across Pakistan. Once participants consented, they were initially assessed by medical professionals to determine their neurological level and impairments using the ASIA Impairment Scale, which categorised them from A to E. Participants were then asked to complete a set of questionnaires, which consisted of several measures. The questionnaire took approximately 20–30 minutes to complete. To ensure linguistic and cultural relevance, the assessment tools were translated into Urdu. Permission to translate and use the instruments was obtained from the original authors where required. Preliminary reliability testing was conducted before data collection, and all translated measures demonstrated acceptable internal consistency in the present sample.
Measures
The questionnaire comprised established and reliable outcome measures, divided into four sections to collect demographic data, environmental barriers, daily activity participation, and QOL (Rahman et al., 2023). The first section included socio-demographic data such as age, gender, marital status, education level, employment status, rehabilitation duration, and environmental support. The second section assessed participation in daily activities using the World Health Organization Disability Assessment Schedule 2.0 (WHODAS-II), a 36-item questionnaire covering six domains (cognition, mobility, self-care, getting along with others, life activities, and social participation) rated on a 5-point Likert scale (Irfan et al., 2017). WHODAS-II demonstrated high reliability, with a Cronbach’s alpha of 0.92. The third section utilised the Craig Hospital Inventory of Environmental Factors–Short Form (CHIEF-SF) to evaluate the impact of environmental factors on participation, with participants rating 12 items on a 5-point Likert scale. The total impact score (ranging from 0 to 8) indicated the severity of environmental barriers. The final section comprised the World Health Organization Quality of Life-BREF (WHOQOL-BREF) Scale, which measured QOL across four domains: Physical Health, Psychological Well-being, Social Relationships, and Environmental Health. The 26-item questionnaire used a 5-point Likert scale, with scores ranging from 0 to 100, where higher scores indicated better QOL.
Statistical analysis
Data were analysed using IBM SPSS Statistics version 28. Multiple linear regression was used to identify the determinants (i.e. personal factors, environmental factors, and neurological impairment levels) of participation in daily life activities. A p-value of <0.05 was considered statistically significant. The Pearson correlation coefficient (r) was used to analyse the relationship between participation in daily life activities and QOL domain, assessing how participation in daily activities correlated with physical, psychological, environmental, and social domains of QOL.
Results
Participants description
The study included 140 individuals with paraplegic SCI, primarily young adults in their mid-30s, diagnosed on average approximately 5 years prior (Table 1). Most participants came from middle- and lower-income backgrounds, relying on family support, pensions, zakat (charitable giving), and assistance from relatives for daily survival. Some were independent, engaging in freelancing, small businesses, or government jobs. The majority were male (97.9%), with ages ranging from 21 to 60 years. Most injuries were traumatic (85.7%), resulting from gunshots, road traffic accidents, falls, and industrial mishaps. Non-traumatic cases (14.3%) were mainly due to tumours and transverse myelitis. Injuries predominantly affected the T1–T12 vertebrae (71.5%), followed by L1–L5 (28.5%). Rehabilitation was a key component of recovery, with 72.9% attending comprehensive rehabilitation programmes, while 27.1% received no structured rehabilitation. Follow-up durations ranged from 15 days to 8 years post-injury.
The demographic characteristics information of the individuals with paraplegic SCI.
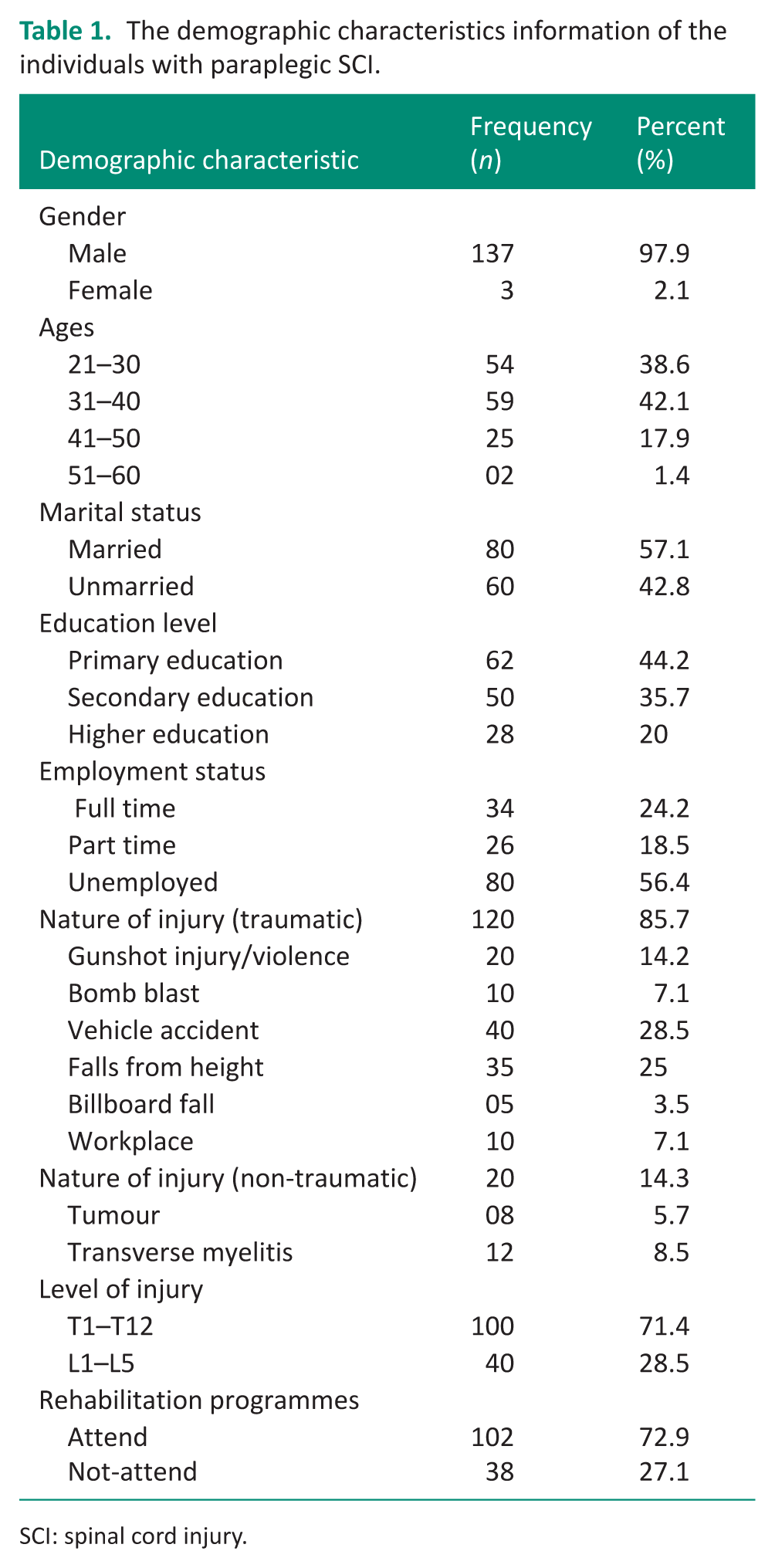
SCI: spinal cord injury.
Environmental barriers measured by CHIEF
Environmental barriers were assessed using the CHIEF-SF. The mean CHIEF-SF total impact score was 1.89 ± 0.34 (median = 2.00) among 140 participants. Most participants reported a score of 2.00 (n = 116, 82.9%), while smaller proportions reported scores of 1.00 (n = 16, 11.4%), 1.50 (n = 4, 2.9%), and 2.50 (n = 4, 2.9%). These findings indicate that environmental barriers were commonly experienced among participants.
Determinants of participation in daily life activities
The multiple regression analysis identified key determinants of participation in daily life activities among individuals with paraplegic SCI living in Pakistan (Table 2). The model demonstrated a good fit (F = 8.90, p < 0.001), indicating a strong collective relationship between the determinants and participation in daily activities. Independent variables included personal factors, environmental factors, and neurological impairment levels, all of which significantly influenced participation. Overall, the model explained 36.7% of the variance in participation, reflecting a moderate predictive ability.
Regression model of key determinants of participation in daily life activities among individuals with paraplegic SCI (N = 140).
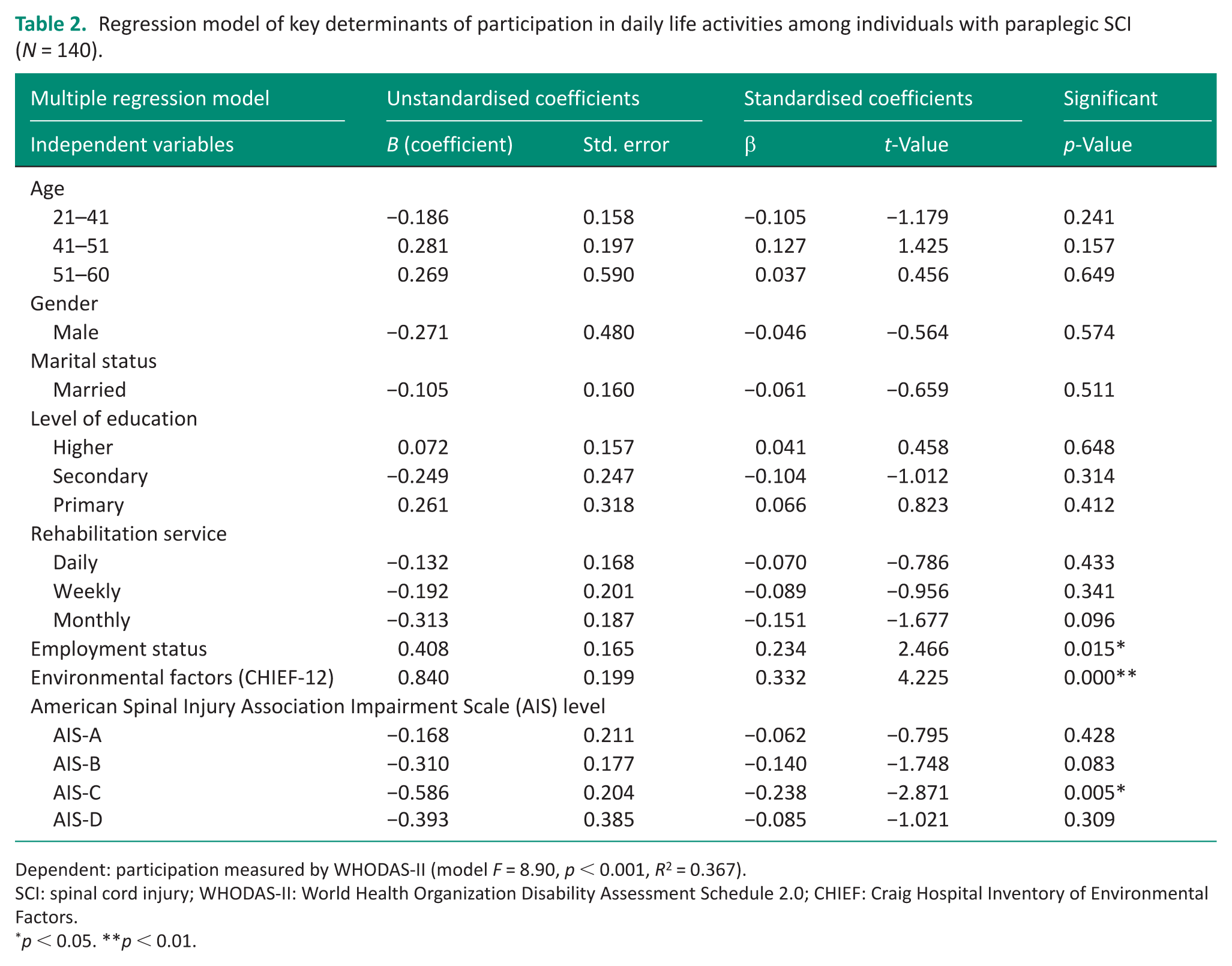
Dependent: participation measured by WHODAS-II (model F = 8.90, p < 0.001, R2 = 0.367).
SCI: spinal cord injury; WHODAS-II: World Health Organization Disability Assessment Schedule 2.0; CHIEF: Craig Hospital Inventory of Environmental Factors.
p < 0.05. **p < 0.01.
Employment status emerged as a significant personal factor. Individuals who were employed reported higher participation levels (β = 0.234, p = 0.015), suggesting that both part-time and full-time work are associated with greater engagement in daily activities. Environmental factors had the strongest influence (β = 0.332, p < 0.001), highlighting the importance of accessibility, assistive devices, and social support in enhancing participation within the community.
Neurological impairment level also contributed significantly to participation. Individuals classified as AIS-C (partial motor function) showed a significant negative association with participation (β = −0.238, p = 0.005), indicating that moderate motor impairments are linked to reduced participation. By contrast, AIS-A and AIS-B impairment levels were not significantly associated with participation (β = −0.062 and β = −0.140, respectively).
Relationships between daily activity participation subscales and QOL domains
The findings on the relationships between participation in daily activities and QOL showed a moderate, negative correlation between the total WHODAS-II score and WHOQOL-BREF scores (r = −0.586, p < 0.001), indicating that greater disability is associated with lower overall QOL among individuals with paraplegic SCI. This study also examined the associations between six subscales of daily life participation and four QOL domains (Figure 1). Physical health, environmental health, and social relationships demonstrated moderate to strong negative correlations with all subscales of daily activity participation (r = −0.346 to −0.742, p < 0.01), suggesting that lower disability in daily activity participation is linked to greater QOL. The strongest correlation was observed between social relationships and social participation (r = −0.742, p < 0.01), reflecting the overlap in constructs measured. By contrast, physical health showed weak or no correlation with most subscales of daily activity participation, except for life activities (r = −0.317, p < 0.01) and social participation (r = −0.410, p < 0.01). No significant correlations were found between physical health and self-care (r = −0.042, p > 0.05) or cognition (r = −0.108, p > 0.05), indicating that these domains may not be substantially associated with physical health in this population.
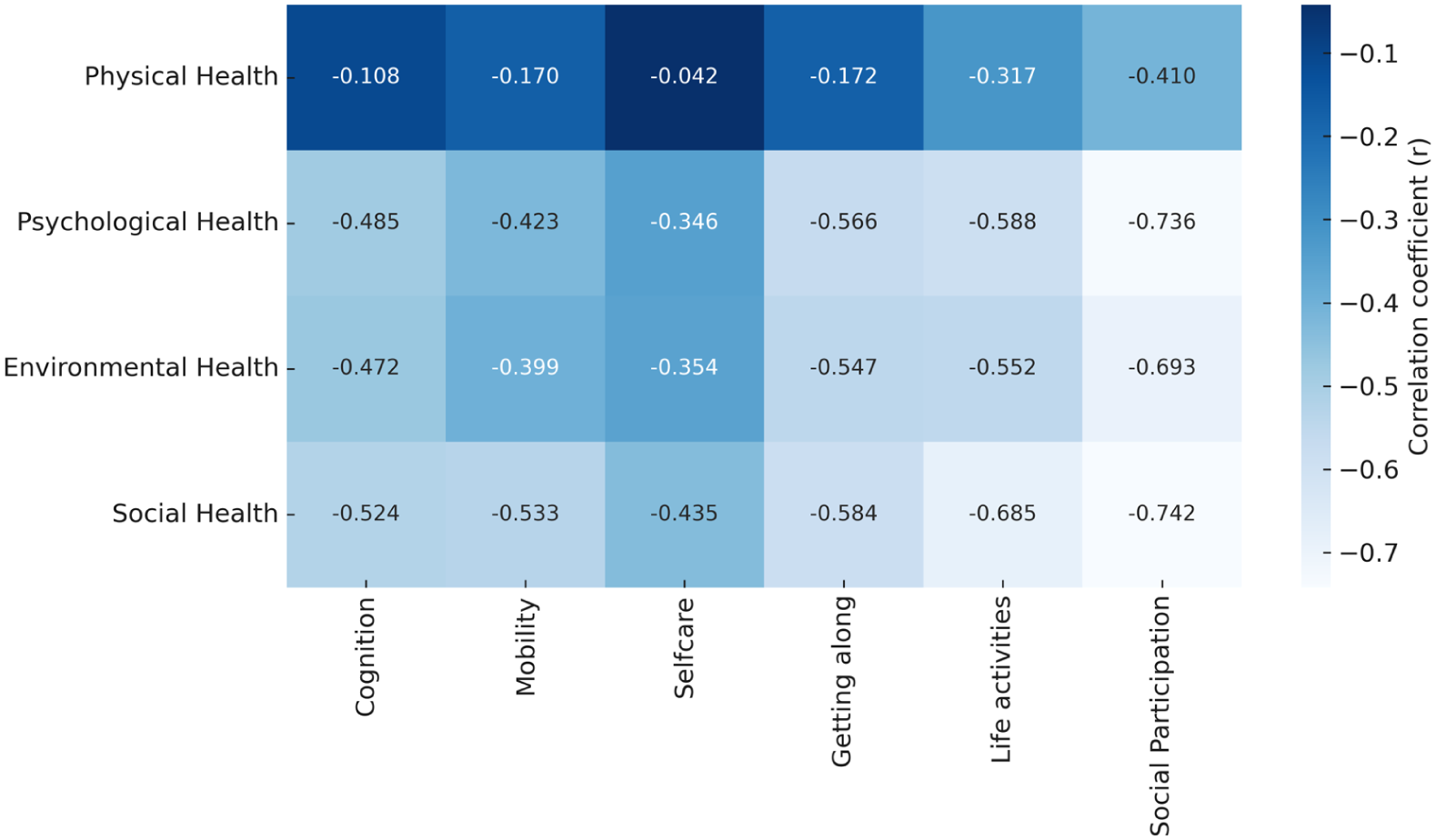
Correlation between participation in daily life activities (WHODAS-II subscales) and QOL (WHOQOL-BREF domains) in individuals with paraplegic SCI (N = 140).
Discussion
This study aimed to identify the determinants of participation in daily life activities and QOL among individuals with paraplegic SCI in Pakistan. Guided by the International Classification of Functioning, Disability, and Health (ICF) model, the study examined personal factors (e.g. age, gender, marital status), environmental factors (CHIEF-12), and impairments of body function/structure (American Spinal Injury Association Impairment Scale level) as determinants of participation. The findings revealed that employment status, environmental support, and neurological impairment level were the most significant determinants. Furthermore, participation in daily activities was closely linked to QOL, with psychological, social, and environmental health demonstrating moderate to strong correlations with all subscales of WHODAS-II. These results provide critical insights for designing effective rehabilitation strategies and developing inclusive social policies for individuals with paraplegic SCI in Pakistan (Ahmed et al., 2018).
Among personal factors, employment status had the greatest impact on participation in daily activities. The regression analysis demonstrated a strong positive association between employment and participation, indicating that individuals who were employed either full time or part time had higher levels of participation than those who were unemployed. This aligns with global studies highlighting how employment fosters independence, enhances social interaction, and improves life satisfaction among individuals with disabilities (Rimmer, 2006). Employment not only provides financial security but also strengthens psychosocial well-being and community integration. However, in Pakistan, individuals with paraplegic SCI encounter significant employment barriers due to limited workplace accessibility, discriminatory hiring practices, and social stigma (Naz et al., 2020). Many individuals rely on family support, pensions, or charitable donations (zakat) for financial stability. Addressing this issue requires policies that promote vocational rehabilitation, self-employment programmes, and microcredit opportunities to empower individuals with SCI economically (Khalid et al., 2022).
Encouraging remote work, freelancing, and entrepreneurship could help individuals with paraplegic SCI overcome mobility challenges and enhance participation in economic activities. Interestingly, other personal factors such as age, gender, marital status, education level, and rehabilitation services did not significantly influence participation in daily activities. This finding contrasts with previous studies that identified education and marital status as key determinants of participation among individuals with disabilities (Mohan and Deb, 2024). In the Pakistani context, however, strong family support systems, cultural expectations, and limited public accessibility may mitigate the impact of these factors. Overall, these results suggest that while personal characteristics shape individual experiences, they are not the primary determinants of participation.
The study identified environmental factors as the strongest determinants of participation, with the highest beta value in the regression model. This finding highlights the critical role of environmental accessibility, social support, and community infrastructure in enabling individuals with paraplegic SCI to participate in daily activities (Khoo et al., 2013). Previous studies have also reported that barriers such as inadequate infrastructure, inaccessible public transport, and the absence of disability-friendly facilities significantly restrict participation (Hussain et al., 2022). In Pakistan, individuals with SCI frequently encounter environmental challenges, including inaccessible buildings, a lack of wheelchair-friendly transportation, and negative societal attitudes. The absence of ramps, elevators, and adapted workspaces limits access to employment and social opportunities. Furthermore, the scarcity of rehabilitation centres and assistive technology resources further hinders participation (Arsh et al., 2019).To address these challenges, policymakers should prioritise universal design principles, disability-inclusive urban planning, and accessible transportation systems. Raising awareness through disability rights campaigns may also help shift societal attitudes and reduce stigma towards individuals with disabilities. In addition, providing government-funded assistive devices such as wheelchairs and mobility aids could significantly enhance independence and participation.
The study found that the neurological impairment level was a significant determinant of participation, with individuals classified as AIS-C showing the lowest participation rates. Interestingly, individuals with complete injuries (AIS-A) demonstrated higher levels of independence compared to those with incomplete injuries (AIS-B, AIS-C, or AIS-D). This finding contrasts with existing literature, which generally reports that less severe impairments are associated with greater participation. A possible explanation is that individuals with complete paraplegia (T1–T12 injuries) often rely on upper-body function, enabling them to develop independent mobility through wheelchair use. By contrast, individuals with incomplete SCI may experience inconsistent mobility, require greater assistance, and frequently encounter complications such as spasticity (Tasiemski et al., 2023). These results highlight the importance of tailored rehabilitation programmes that emphasise upper-body strengthening exercises, mobility training, and adaptive skill development to improve participation among individuals with varying neurological impairment levels of SCI.
This study also explored the relationships between participation in daily living activities and QOL. The findings showed that lower participation was significantly associated with poorer QOL across physical, psychological, social, and environmental domains (Datta et al., 2013; Khanzada et al., 2024a). Psychological and social health were most affected, particularly in relation to difficulties with social participation and interpersonal interactions. These results suggest that when individuals with paraplegic SCI are unable to fully engage in meaningful daily activities, their overall well-being and life satisfaction are compromised. Interestingly, physical health showed weaker associations with some areas of participation, such as cognition and self-care, indicating that these domains may not directly influence physical well-being in this population. Instead, broader aspects such as mobility, life activities, and social roles had a more substantial impact on perceived QOL.
These findings support the biopsychosocial perspective of the ICF model, which integrates body functions and structures, activity limitations, participation restrictions, and environmental factors in understanding disability. They reinforce the idea that QOL is a multidimensional construct shaped not only by physical health but also by social inclusion, psychological resilience, and environmental accessibility. This highlights the need for a holistic, community-centred approach to rehabilitation, where the goal extends beyond physical recovery to enhancing full participation and psychological adjustment after injury (Datta et al., 2013). These findings provide strong evidence for policymakers and rehabilitation professionals to advocate for inclusive and accessible societal structures that allow individuals with disabilities to live fulfilling and meaningful lives.
Strengths and limitations
To our knowledge, this is the first study to explore the determinants of participation in daily life activities and QOL among individuals with paraplegic SCI in Pakistan. Nonetheless, several limitations must be acknowledged. First, the small sample size limits generalisability and may not fully capture the diverse experiences of individuals with SCI across different socioeconomic backgrounds. Second, the sample predominantly comprised male participants (97.9%), restricting the ability to examine gender-related differences in participation and QOL. Third, reliance on self-reported measures may have introduced response bias, as participants’ subjective perceptions could influence their answers. Fourth, the use of translated assessment tools may introduce potential measurement limitations. Although permission to translate and use the measures was obtained where required, and preliminary reliability testing showed acceptable internal consistency for all translated instruments, the Urdu versions used in this study have not yet undergone full formal psychometric validation. Therefore, the findings should be interpreted with caution, particularly regarding cross-cultural measurement equivalence. Finally, the cross-sectional design precludes causal inferences, making it difficult to determine the long-term impact of participation on QOL. Despite these limitations, the study provides important preliminary evidence on the determinants of social participation among individuals with paraplegic SCI in Pakistan, offering direction for improved rehabilitation services and targeted support for this population.
Future research directions
Future research should aim to include larger and more diverse samples, with greater representation of women, individuals from rural areas, and those with different neurological impairment levels of SCI. Longitudinal designs would be particularly valuable for tracking changes in participation and QOL over time and for establishing causal relationships between variables. Exploring cultural attitudes towards disability across different regions of Pakistan may also yield important insights into how social norms influence participation experiences. Furthermore, studies assessing the effectiveness of rehabilitation programmes, assistive technologies, and policy interventions are needed to guide the development of evidence-based strategies that can enhance participation and QOL for individuals with paraplegic SCI.
Conclusion
This study demonstrated that employment status, environmental factors, and neurological impairment level were the strongest determinants of participation in daily life activities among individuals with paraplegic SCI in Pakistan. Participation was also closely linked to QOL, with psychological, environmental, and health factors showing moderate to strong associations across all subscales of the WHODAS-II. These findings highlight the importance of policy reforms, inclusive employment opportunities, accessible infrastructure, and strengthened rehabilitation programmes to enhance participation and QOL for individuals with SCI. Addressing environmental barriers, reducing stigma, and fostering stronger social support networks are essential steps towards creating a more inclusive society for individuals with disabilities.
Key findings
Environmental barriers and employment status significantly influence participation in daily life activities post-SCI.
Participation is moderately associated with psychological, environmental, and social domains of quality of life.
Neurological impairment level (particularly AIS-C) predicts reduced participation compared to complete injuries.
What the study has added
This study provides the first evidence from Pakistan identifying key modifiable determinants of participation and their relationship with quality of life in individuals with paraplegic spinal cord injury.
Footnotes
Ethical considerations
This study was approved by the Ethics Committee of Universiti Teknologi MARA, Malaysia (Ref. no: 600-TNCPI (5/1/6)) and the National Bioethics Committee for Research, National Institute of Health, Pakistan (Ref. no: NBC-922/23/1546).
Consent statement
Written informed consent to participate in this study was obtained from all participants prior to data collection. No identifiable personal data, images, or videos are presented in this manuscript.
Author contributions
FJK conducted the study, reviewed the literature, and led data collection and analysis. MA contributed to the cross-cultural alignment of measures and manuscript editing. MGM and MZAR were involved in protocol development, data interpretation, and critical manuscript review. AZCD supervised the study, facilitated ethical approvals, and provided methodological and reporting guidance. NAMN was responsible for formatting and editing the manuscript. FJK wrote the first draft. All authors reviewed and approved the final version of the manuscript.
Funding
The authors declared no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Patient and public involvement data
During the development, progress, and reporting of the submitted research, Patient and Public Involvement in the research was not included at any stage of the research.
Reporting guidelines
This study was conducted and reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines.