
Abstract
Introduction:
Cardiovascular disease (CVD) frequently compromises independence in activities of daily living (ADL), a core area of everyday occupation. Although resilience supports adaptation to chronic illness, its association with ADL independence in CVD remains unexamined. Given that resilience is multidimensional, this exploratory cross-sectional study examined overall and domain-specific resilience in relation to ADL independence.
Methods:
Thirty-nine adults with CVD were recruited from an outpatient specialized cardiovascular referral center in Shiraz, one of the largest metropolitan cities in southern Iran. Participants completed the Persian Connor–Davidson Resilience Scale, which measures four domains (achievement motivation, self-confidence, tenacity, adaptability), and the Barthel Index assessing ADL independence. Functional independence was dichotomized as independent (Barthel Index >90) or dependent/relatively dependent (⩽90). Mann–Whitney U tests compared overall and domain-specific resilience scores between groups, with effect sizes calculated.
Results:
Higher overall resilience was significantly associated with functional independence. Among the four domains, only self-confidence significantly differentiated independent from dependent participants. Achievement motivation and tenacity showed directional trends favoring independence, whereas adaptability demonstrated weak functional relevance.
Conclusion:
Resilience is domain-specifically associated with ADL independence in CVD, with self-confidence showing the strongest functional relevance. Findings support confidence-targeted occupational therapy strategies (i.e. graded mastery experiences) in cardiac rehabilitation.
Keywords
Introduction
Cardiovascular diseases (CVDs) encompass a group of disorders of the heart and blood vessels, including coronary heart disease, cerebrovascular disease (stroke), peripheral arterial disease, rheumatic and congenital heart diseases, and venous thromboembolic conditions. CVDs remain the leading cause of death worldwide, accounting for an estimated 19.8 million deaths in 2022 (32% of all deaths), primarily because of heart attacks and strokes (World Health Organization, 2025). Projections indicate a substantial future burden, with annual cardiovascular deaths expected to rise from 20.5 million in 2025 to 35.6 million by 2050 (Chong et al., 2025). In Iran, CVD has been the leading cause of mortality for over four decades, accounting for approximately 46% of all deaths and contributing to 20%–23% of the national disease burden (Sarrafzadegan and Mohammmadifard, 2019).
Beyond its impact on mortality, CVD is also a significant contributor to functional decline. Symptom burden—including fatigue, dyspnea, and reduced exercise tolerance—can diminish overall functional capability, impairing the ability to perform everyday tasks (Jurgens et al., 2022). For example, individuals with CVD may exhibit measurable limitations in activities of daily living (ADLs), including mobility, transfers, and self-care, even when clinically stable, as indicated by standardized assessments such as the Barthel Index (Khalandi et al., 2022). These findings underscore functional independence as a clinically meaningful and rehabilitation-relevant outcome for adults living with CVD (Schmucker et al., 2019).
Chronic health challenges, such as CVD, disrupt daily roles and routines, necessitating ongoing adaptive responses—a phenomenon central to occupational therapy perspectives on long-term health conditions (Fields and Smallfield, 2022; Lambdin-Pattavina and Pyatak, 2022). This demand for continuous adaptation highlights the clinical relevance of psychological resilience, which enables individuals to navigate the psychological and functional demands of chronic illness (Sá et al., 2025). Broadly defined, resilience manifests through flexible mental, emotional, and behavioral responses supported by personal beliefs, social resources, and coping strategies (American Psychological Association, 2026). However, from an occupational therapy and occupational science standpoint, resilience is not merely an internal psychological trait; rather, it is closely intertwined with occupation, reflecting how individuals adapt and persist through engagement in everyday activities within specific personal and environmental contexts (Turner et al., 2025). Thus, from this occupation-centered perspective, resilience is not merely inherent in daily activities but is actively fostered through occupational engagement. As Turner et al. (2025) succinctly state, “occupation . . . represents the how of fostering resilience” (p. 16).
Although resilience is increasingly recognized as important in adapting to chronic illness, it remains largely unexplored in adults with CVD. Ghulam et al. (2022) note that investigations examining the relationship between resilience and CVD-related outcomes are still in the early stages of development. Furthermore, a scoping review by Abshire Saylor et al. (2023) characterizes resilience research in cardiovascular populations as emerging and complex, with many unanswered questions. Although findings have not been entirely consistent, the existing literature generally suggests that higher resilience is associated with more favorable health outcomes and fewer adverse disease-related consequences in CVD populations (Ghulam et al., 2022).
Consistent with these observations, higher resilience in adults with CVD has been linked to increased physical activity (Ma, 2023), lower depressive symptoms (Ketcham et al., 2022), reduced death anxiety (Aryafard et al., 2025), and better health-related quality of life (Huang et al., 2025) However, a recent systematic review of resilience in adults with CVD did not identify any studies examining its association with independence in ADL, despite reporting associations with quality of life, depression, and adherence to medication and behavioral regimens (Love et al., 2021). Consequently, whether resilience translates into functional independence in everyday activities within this population remains largely unknown.
Evidence from related cardiovascular conditions, particularly stroke, underscores this uncertainty regarding ADL independence. While some studies have reported positive associations between resilience and independence in ADL measured by the Barthel Index (Heltty and Zahalim, 2023), other longitudinal research suggests that resilience assessed shortly after stroke may not predict subsequent ADL recovery (Norvang et al., 2022). These inconsistencies raise important questions about whether resilience translates to activity-based functioning in non-neurological CVD, where evidence is even more limited.
Consistent with the occupational therapy perspective outlined earlier (Turner et al., 2025), examining resilience in relation to ADL performance offers a direct approach to investigating resilience as an occupationally expressed construct. Addressing the gap identified above, the present study explores the associations between overall and domain-specific resilience and functional independence in ADL among adults living with non-neurological CVD.
Theoretical framework
The present study is based on the four-factor structure of resilience validated in the Persian version of the Connor–Davidson Resilience Scale (CD–RISC; Khoshouei, 2009). This structure conceptualizes resilience as a multidimensional construct comprising four domains: achievement motivation, self-confidence, tenacity, and adaptability. Achievement motivation reflects goal-directed effort despite obstacles. Self-confidence represents perceived competence in managing challenges. Tenacity captures persistence in the face of adversity. Adaptability encompasses meaning-based beliefs and behavioral flexibility in response to change.
Each domain can be conceptually linked to occupational performance processes. Self-confidence may influence perceived competence in self-care and mobility tasks; achievement motivation and tenacity may support sustained effort during daily task completion; and adaptability may facilitate adjustment to environmental or bodily changes affecting performance. The Persian four-factor structure is a culturally validated adaptation of the original Connor–Davidson conceptualization (Connor and Davidson, 2003), which identified five domains: personal competence and tenacity; trust in one’s instincts and stress tolerance; acceptance of change and secure relationships; perceived control; and spiritual influences.
This framework facilitates the examination of resilience both as a global adaptive orientation (reflected in the total CD–RISC score) and as distinct but related domains. The present study employs this domain-specific framework to investigate which resilience domains are most strongly associated with functional independence in ADL among adults with non-neurological CVD.
Aims
ADL performance is a core domain of occupational therapy practice and a central functional outcome in cardiovascular rehabilitation (Schmucker et al., 2019). Accordingly, functional independence in ADL was selected as the primary outcome for examining resilience as an occupationally expressed construct. Using the Persian four-factor structure of the CD–RISC, the study pursued three specific aims:
To examine the association between overall resilience and functional independence in ADL.
To determine whether resilience domain scores differ between participants classified as functionally independent (Barthel Index >90) and those classified as dependent or relatively dependent (⩽90).
To descriptively characterize item-level resilience patterns in order to contextualize domain-level findings and to examine how resilience attributes are expressed in this cardiovascular sample.
Although the study was exploratory and not designed to support confirmatory hypothesis testing, the following directional expectations guided the inferential analyses:
H1: Higher overall resilience is associated with greater functional independence in ADL.
H2: Functionally independent participants demonstrate higher scores across resilience domains compared to dependent or relatively dependent participants.
No a priori hypothesis was specified for Aim 3, as the item-level analyses were exploratory and intended to provide descriptive context.
Methods
Design
This study employed a cross-sectional, exploratory design to examine resilience and its domain-specific expressions in adults with CVD. A cross-sectional approach was chosen to provide an initial characterization of resilience profiles and their associations with functional independence. This design is appropriate for a clinical population with limited empirical evidence and aligns with the study’s focus on describing patterns rather than testing causal relationships.
Study setting
The study was conducted in Shiraz, Iran, a major metropolitan area with specialized cardiovascular care services. Participants were recruited from a single cardiovascular care center affiliated with Shiraz University of Medical Sciences, which serves as a regional referral facility for adults with cardiovascular conditions. Recruitment from this center ensured diagnostic consistency and provided access to individuals receiving standardized cardiovascular care and follow-up services.
Participants
The study sample consisted of 39 adults with a documented history of CVD, including myocardial infarction and coronary artery disease, who were receiving outpatient cardiac care. Eligibility criteria included: (1) age 18 years or older, (2) confirmed medical diagnosis of CVD documented in clinical records, (3) medical stability at the time of assessment, and (4) ability to provide informed consent. The inclusion of a broad adult age range was intentional, as CVD affects individuals throughout midlife and older adulthood. Although functional independence and resilience may vary across the lifespan, age was not the primary explanatory variable in this study and was treated as a demographic characteristic of the clinical population. Therefore, participants were analyzed as a single adult cohort.
To minimize confounding factors affecting functional independence, individuals with diagnosed neurological disorders (e.g. stroke and neurodegenerative diseases), severe cognitive or communication impairments that precluded valid self-reporting, acute medical instability at the time of assessment, or psychiatric conditions likely to interfere with questionnaire completion were excluded. These criteria were applied to ensure that variations in ADL performance more accurately reflected cardiovascular status rather than comorbid neurological, psychiatric, or acute medical conditions.
Instruments
Participants were asked to complete two standardized questionnaires in Persian: CD–RISC and the Barthel Index. In addition, they completed a demographic checklist, which provided self-reported information on factors such as age, gender, marital status, educational attainment, and living arrangement. These demographic variables were included because prior research suggests they may influence resilience.
Connor–Davidson Resilience Scale (CD-RISC)
Resilience was assessed using the CD–RISC, a self-report measure originally developed by Connor and Davidson (2003) to evaluate individuals’ capacity to cope with adversity and stress. The CD–RISC consists of 25 items rated on a five-point Likert scale ranging from 0 (totally false) to 4 (always true), yielding total scores from 0 to 100, with higher scores indicating greater resilience.
In the present study, the standardized Persian version of the CD–RISC, validated by Khoshouei (2009) in an Iranian student sample, was employed. Psychometric evaluation of this version supported a four-factor structure—achievement motivation, self-confidence, tenacity, and adaptability—identified through exploratory factor analysis using maximum likelihood extraction with oblique rotation. The scale demonstrated strong internal consistency and temporal stability. Cronbach’s alpha coefficients for the four subscales were 0.83, 0.91, 0.79, and 0.78, respectively, while test–retest reliability coefficients were 0.78, 0.85, 0.88, and 0.81. Collectively, these findings support the reliability and validity of the Persian CD–RISC and justify its use for assessing resilience and its domains within the Iranian cultural context. A systematic review of CD–RISC psychometric properties across clinical populations confirmed its structural validity and reliability, supporting its use in chronic disease research (Sharif-Nia et al., 2024)
The CD–RISC demonstrated excellent internal consistency in the present sample, with a Cronbach’s alpha coefficient of 0.901 for the total scale. At the subscale level, internal consistency coefficients ranged from acceptable to good, with Cronbach’s alpha values of 0.813 for self-confidence, 0.709 for adaptability, 0.702 for tenacity, and 0.628 for achievement motivation.
Barthel Index
Functional independence was assessed using the Barthel Index, a widely used standardized measure of performance in basic ADL, originally developed by Mahoney and Barthel (1965). The Barthel Index comprises 10 items that evaluate independence in core self-care and mobility activities, including feeding, bathing, grooming, dressing, bowel and bladder control, toileting, transfers, mobility, and stair climbing. Each item is scored based on the level of assistance required, with weighted scores summed to produce a total score ranging from 0 to 100, where higher scores indicate greater functional independence.
The Barthel Index has demonstrated strong psychometric properties in Iranian clinical populations with CVD. Khalandi et al. (2022) reported a content validity ratio of 0.98, a content validity index of 0.93, and high internal consistency reliability (Cronbach’s alpha = 0.94) in individuals with cardiovascular conditions. These findings support the use of the Barthel Index as a reliable and valid measure of functional independence in the present study.
Levels of functional independence were categorized using the same cut-score framework reported by Khalandi et al. (2022). In that study, Barthel Index scores of <55 indicated disability, scores of 55–90 indicated relative dependency, and scores of >90 indicated independence. To maintain consistency with this established Iranian classification and to ensure adequate group sizes for statistical analyses, scores in the present study were dichotomized into dependent or relatively dependent (Barthel Index ⩽90) and independent (Barthel Index >90). This categorization facilitated meaningful comparisons of resilience outcomes based on functional independence while preserving alignment with prior cardiovascular research conducted in Iran.
Procedure
This research was approved by the Research Ethics Committees of Shiraz University of Medical Sciences, Shiraz, Iran. Participants were recruited using a consecutive sampling approach over a 1-month period, during which all eligible patients presenting within the data collection timeframe were invited to participate. This strategy was chosen to enhance feasibility within the clinical context, reduce selection bias, and improve the representativeness of the accessible outpatient CVD population. Eligible individuals were approached by two trained research assistants who provided standardized verbal and written explanations of the study objectives and procedures. Written informed consent was obtained from all participants prior to data collection. Although 51 individuals initially participated, 12 were excluded from the final analysis due to incomplete or insufficient questionnaire data, resulting in a final analytical sample of 39 participants.
Data collection was conducted in a designated assessment room within the specialized cardiovascular care center to ensure privacy and minimize distractions. Participants completed a demographic questionnaire, the Persian version of the CD–RISC, and the Barthel Index. The total time required to complete all study measures was approximately 45 minutes, with short rest breaks offered as needed to reduce fatigue. All questionnaires were administered in Persian, and participants were encouraged to seek clarification if any item was unclear.
Data analysis
All statistical analyses were performed using IBM SPSS Version 27 (IBM Corp., Armonk, NY, USA), with a two-tailed significance level set at p < 0.05. Prior to inferential testing, data were screened to assess distributional assumptions. Because CD–RISC scores were not normally distributed and group sizes were unequal, nonparametric methods were employed.
In addition to analyses aligned with the primary study aims, exploratory comparisons were conducted to characterize the distribution of overall resilience across demographic variables. Mann–Whitney U tests were employed to examine differences in total CD–RISC scores across dichotomized demographic categories, including age group, gender, marital status, living arrangement, and educational attainment. These analyses aimed to contextualize resilience patterns within the sample and were not intended to establish causal or predictive relationships. The analyses addressing the primary aims were structured as follows:
Differences in overall resilience by functional independence
Participants were categorized into two functional independence groups based on Barthel Index scores (⩽90 = dependent/relatively dependent; >90 = independent). The Mann–Whitney U test was used to compare total CD–RISC scores between the groups. Effect sizes (r) were calculated by dividing the standardized z statistic by the square root of the total sample size to estimate the magnitude of group differences.
Domain-level differences by functional independence
Separate Mann–Whitney U tests were conducted to compare resilience subscale scores—achievement motivation, self-confidence, tenacity, and adaptability—across functional independence groups. Effect sizes were calculated to quantify the magnitude of group differences within each domain.
Item-level characterization of resilience patterns
Item-level characterization of resilience patterns was conducted descriptively. Means and standard deviations (SDs) were calculated for each individual CD–RISC item. Items were then ranked according to mean scores to identify resilience attributes that were relatively more or less endorsed within the sample. These analyses were exploratory and intended to contextualize domain-level findings rather than to test specific hypotheses.
Although a formal a priori power calculation was not performed due to the exploratory nature of the study and the limited accessible population, sensitivity analysis indicated that the available sample size was sufficient to detect moderate effect sizes (r ≈ 0.30) in Mann–Whitney U tests at α = 0.05. Smaller effects may not have been detectable given the sample distribution.
Results
The study sample consisted of 39 participants (mean age = 50.05 years, SD = 12.5), predominantly women, individuals under 60 years of age, married participants, and those living with family members. Most participants had completed up to secondary education. Functional independence was unevenly distributed, with a larger proportion classified as independent rather than dependent or relatively dependent, reflecting the characteristics of the recruited outpatient population. Exploratory Mann–Whitney U tests indicated no statistically significant differences in total resilience scores across demographic categories, including age group, gender, marital status, living arrangement, and educational attainment (see Table 1). Results addressing the primary study aims are presented below.
Demographic and functional characteristics of participants with CD–RISC mean ranks (N = 39).
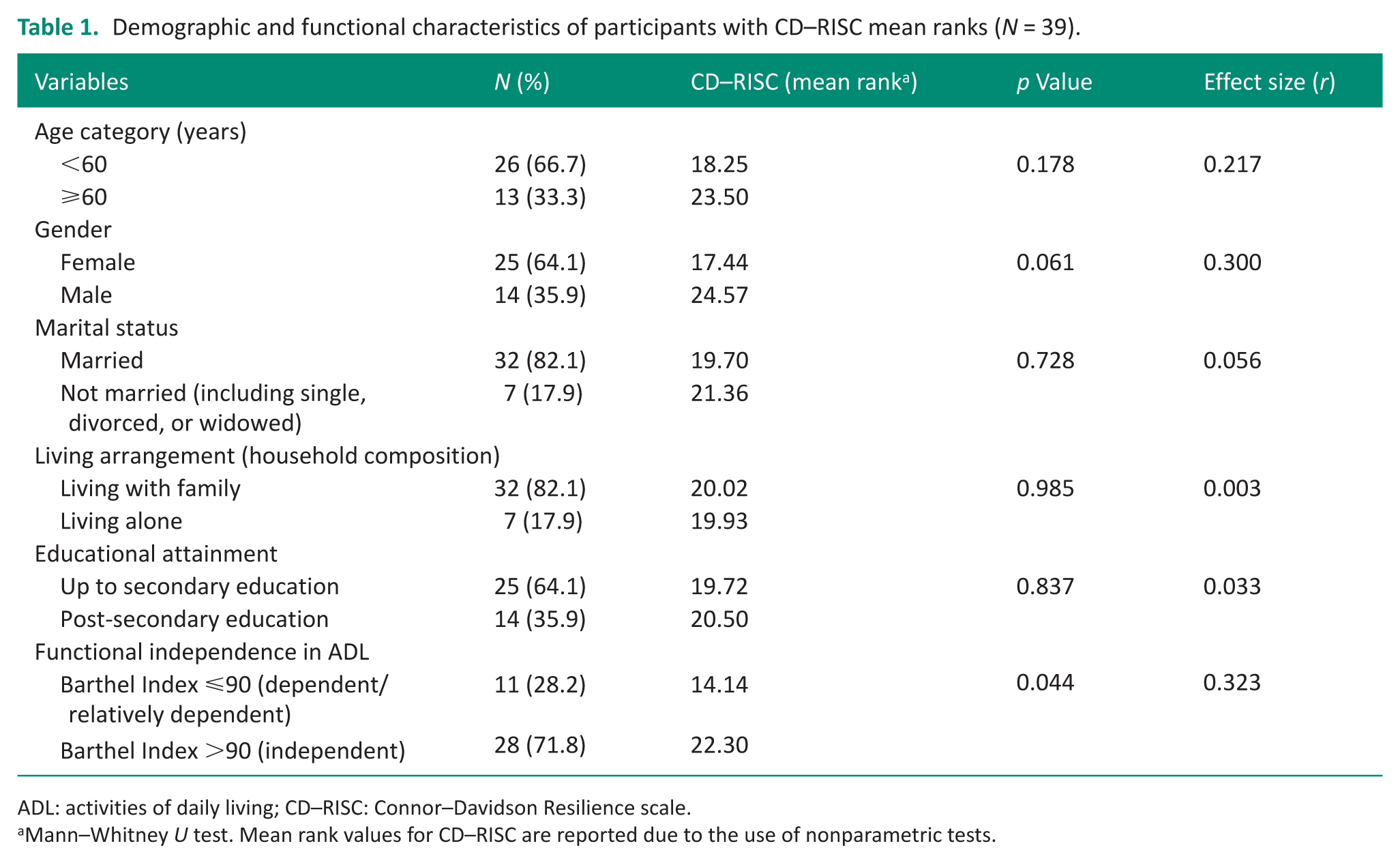
ADL: activities of daily living; CD–RISC: Connor–Davidson Resilience scale.
Mann–Whitney U test. Mean rank values for CD–RISC are reported due to the use of nonparametric tests.
Differences in overall resilience by functional independence
Total resilience scores differed significantly between functional independence groups (see Table 1). Participants classified as independent (Barthel Index >90) demonstrated higher mean resilience ranks compared to those classified as dependent or relatively dependent (Barthel Index ⩽90), with a moderate effect size (r = 0.323). These findings indicate that greater resilience was observed among functionally independent participants.
Domain-level differences by functional independence
Subscale analyses revealed variability in domain-specific group differences (see Table 2). Among the four resilience domains, only self-confidence showed a statistically significant difference between functional independence groups, with a moderate effect size (r = 0.333). Achievement motivation and tenacity exhibited nonsignificant but directionally consistent differences favoring independent participants, accompanied by small to moderate effect sizes. Adaptability demonstrated the smallest effect size and did not differ significantly between groups. These findings suggest differential domain-level relevance to functional independence in ADL.
Subscale-level differences in resilience by functional independence in activities of daily living.
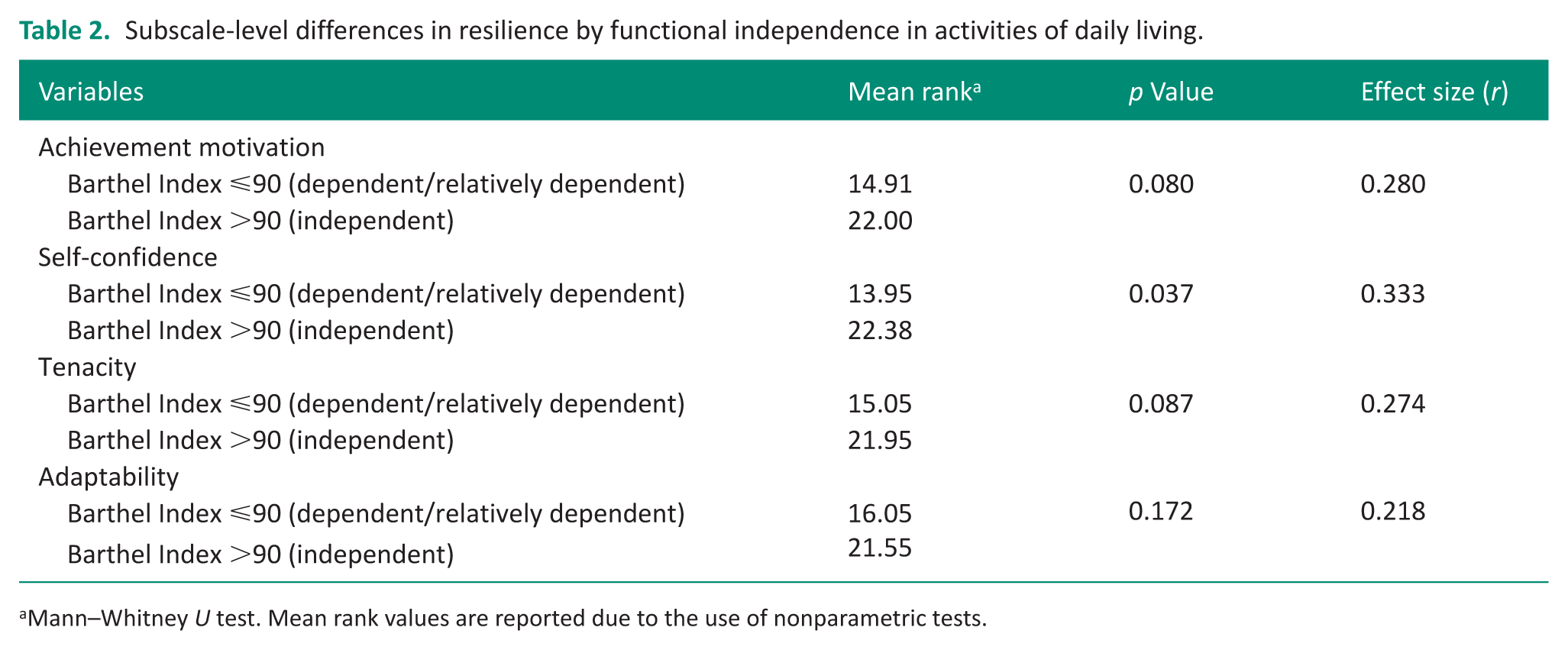
Mann–Whitney U test. Mean rank values are reported due to the use of nonparametric tests.
Item-level resilience patterns
Item-level descriptive statistics were examined to contextualize the domain-level findings (see Table 3). The highest mean scores corresponded to belief-based coping, persistence, and confidence-related attributes. In contrast, items reflecting behavioral and cognitive flexibility under stress were less frequently endorsed. This distribution aligns with the subscale-level findings, particularly the stronger differentiation observed for self-confidence and the comparatively weaker functional differentiation of adaptability.
Item-level descriptive statistics for the Persian CD–RISC, ordered by mean score.
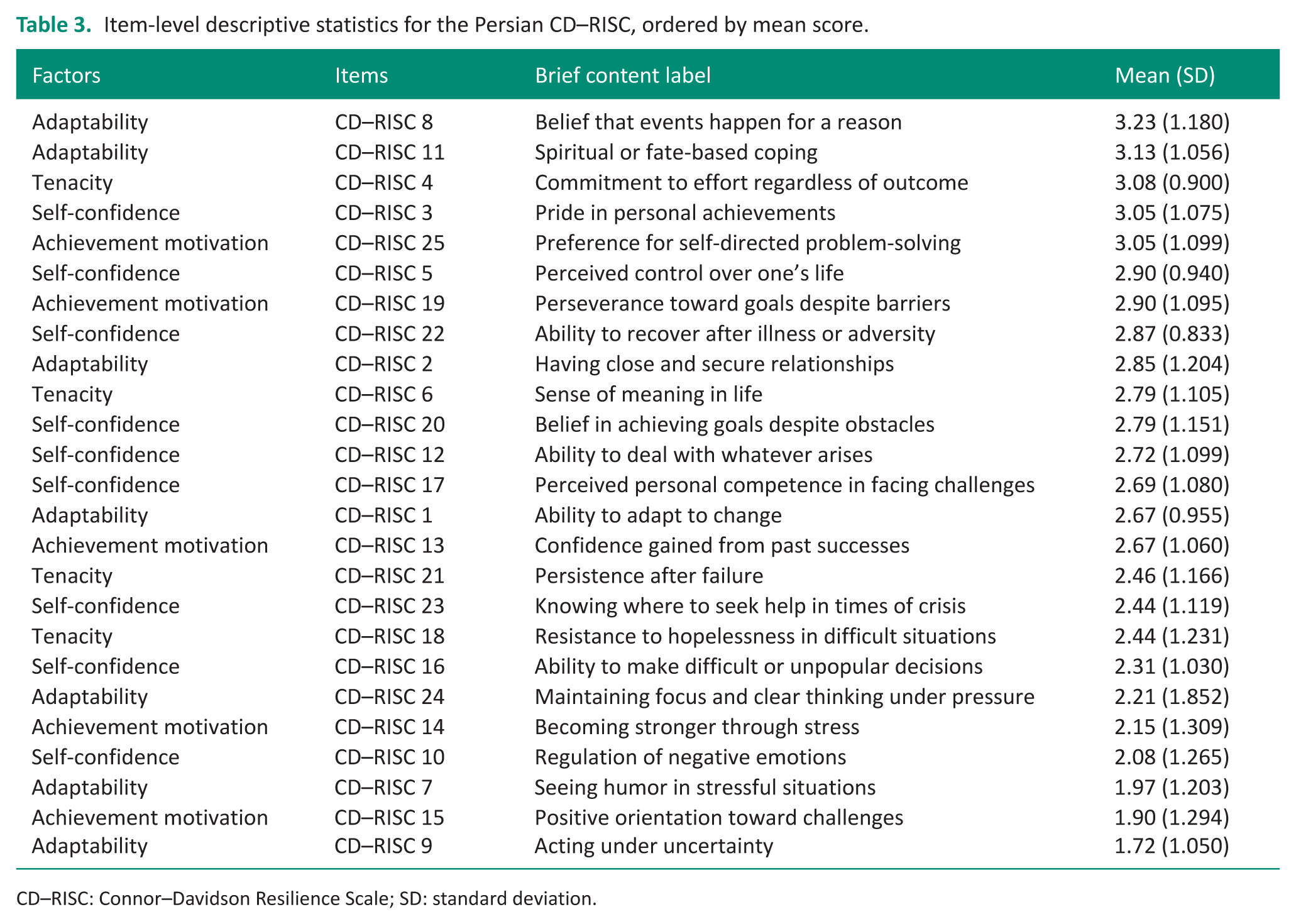
CD–RISC: Connor–Davidson Resilience Scale; SD: standard deviation.
Discussion
This exploratory study examined the association between resilience and functional independence in ADL among adults with CVD using a culturally validated four-factor resilience model. Overall resilience showed a statistically significant association with functional independence, with self-confidence emerging as the only domain that significantly differentiated independent from dependent participants. Achievement motivation and tenacity demonstrated nonsignificant but directionally consistent trends favoring independent participants, whereas adaptability did not meaningfully differentiate functional status. Collectively, these findings suggest that functional independence following CVD may be more closely linked to confidence-based processes embedded in everyday task performance than to broader or more flexible forms of adaptation.
The association between overall resilience and functional independence, though modest, is clinically meaningful. This finding aligns with broader evidence suggesting that resilience may mitigate the adverse effects of CVD-related adversities and stressors on physical health, thereby promoting adaptive behaviors that support everyday functioning (Park et al., 2022). Further support for this interpretation comes from research on physical activity in cardiovascular populations. In adults with heart failure, higher resilience—conceptualized as the effective mobilization of personal and environmental resources to overcome activity-related barriers and maintain participation despite physical limitations—has been associated with greater engagement in physical activity (Ma, 2023). Although physical activity and ADL independence are distinct constructs, both require sustained effort despite functional constraints, underscoring the importance of resilience for functional outcomes in adults with CVD.
The significant association between self-confidence and functional independence observed in this study suggests that confidence-related resilience attributes are closely linked to everyday functioning after CVD. Self-confidence has been identified as a crucial determinant of care-seeking and health-maintenance behaviors during care transitions following cardiac events (Neto et al., 2025). Consistent with evidence from chronic disease populations, higher levels of ADL and self-confidence tend to co-occur (Shi et al., 2025). This interpretation aligns with self-management-oriented occupational therapy approaches, which emphasize the development of patients’ confidence, perceived competence, and sense of agency as foundational to sustained functional independence in individuals with chronic conditions (Fields and Smallfield, 2022).
Beyond self-confidence, achievement motivation and tenacity demonstrated nonsignificant but directionally consistent differences favoring functionally independent participants, with small to moderate effect sizes. Although these differences did not reach statistical significance, the observed effect sizes suggest that persistence-oriented resilience attributes may still play a meaningful role in supporting everyday functioning after CVD. At the item level, participants frequently endorsed statements reflecting sustained effort, perseverance, and commitment to doing one’s best despite difficulty, indicating that these expressions of resilience are salient within this population. Evidence from rehabilitation literature highlights tenacity—defined as persistence and determination—as an essential yet often under-recognized component of effective rehabilitation, particularly in clinical contexts requiring prolonged effort over time (Anderson, 2024). This pattern aligns with conceptual models of psychological endurance, which emphasize that motivation to persist in the face of challenges contributes to sustained goal-directed behavior under conditions of ongoing stress (Biggs et al., 2024). Together with the item-level endorsement patterns observed in this study, these findings suggest that, even in the absence of statistically significant group differences, the convergence of subscale-level trends and item-level endorsements indicates that functional independence may be supported by resilience processes rooted in sustained, goal-directed effort.
In contrast to the self-confidence and persistence-oriented resilience domains, adaptability showed the weakest association with functional independence in ADL. Item-level analyses revealed considerable heterogeneity within this domain: flexibility-oriented attributes were less frequently endorsed, whereas belief- and meaning-oriented items—such as spiritual or fate-based coping—were among the most strongly endorsed resilience attributes. This pattern suggests that adaptability in this population may be expressed primarily through meaning-making frameworks rather than behavioral flexibility. Consistent with evidence that meaning-based resources, including spirituality and religion, can serve as coping mechanisms in chronic illness (Conduah et al., 2025), this pattern may reflect the cultural salience of spiritual and fate-based interpretations of CVD-related adversity within the Iranian context. Although these belief- and meaning-oriented items were highly endorsed and likely support psychological adjustment, they contributed little to functional independence in ADL, helping to explain the weak association of the overall adaptability domain with this outcome.
Conceptual and methodological limitations inherent in cross-sectional designs likely contribute to the weak association observed between adaptability and ADL independence, a pattern that becomes clearer when considering the distinction between meaning-based and flexibility-oriented expressions of adaptability. Flexibility is increasingly recognized as a dynamic, context-dependent aspect of resilience that unfolds through ongoing adjustment to environmental and task demands rather than as a stable trait, requiring longitudinal assessment for accurate measurement (Ringgold and Rohleder, 2025). The relatively lower endorsement of flexibility-oriented adaptability behaviors in this sample may reflect the static nature of cross-sectional assessment. Thus, the weaker association with ADL independence may arise from a mismatch between the dynamic nature of flexibility and the limitations of cross-sectional design, rather than from adaptability being unimportant for functional outcomes following CVD.
Limitations
Several limitations should be considered when interpreting these findings. First, the sample was recruited using a consecutive, single-center outpatient sampling approach, which may introduce selection bias. Individuals receiving outpatient follow-up care are more likely to be medically stable and functionally higher-performing than those in acute or inpatient settings. This recruitment context may have contributed to the predominance of functionally independent participants and limits the generalizability of the findings to more functionally impaired or hospitalized CVD populations.
Second, although including a broad adult age range enhanced the clinical representativeness of the sample, it also introduced heterogeneity. Functional independence and resilience are constructs that may vary across the adult lifespan. The modest sample size and unequal distribution across age categories limited the ability to conduct age-stratified analyses or to examine potential interaction effects between age and functional status. Although no statistically significant age differences in overall resilience were observed in the present sample, the study was not specifically powered to detect developmental effects.
Third, the cross-sectional design precludes causal inferences about the relationship between resilience and functional independence. The observed associations represent concurrent relationships and do not establish a directional influence.
Fourth, resilience was assessed using a self-report measure, which is susceptible to response bias and may not fully capture behavioral or contextually enacted expressions of resilience in everyday activities. Although the Persian version of the CD–RISC demonstrates strong psychometric properties, it was originally validated in a nonclinical student population, which may not fully represent resilience as expressed in adults with CVD.
Finally, functional independence was measured using the Barthel Index, which focuses on basic ADL performance. Instrumental ADL, participation-level outcomes, and broader occupational engagement were not directly assessed, potentially limiting the interpretation of resilience domains—particularly adaptability—that may be more evident at higher levels of functional complexity.
Implications for practice
The significant association between self-confidence and functional independence observed in this study suggests that occupational therapy interventions should explicitly target confidence through graded ADL challenges and mastery experiences (e.g. progressive mobility or self-care tasks with gradually reduced assistance). Furthermore, the four-factor structure of the CD–RISC (achievement motivation, self-confidence, tenacity, and adaptability) can guide domain-specific clinical reasoning. Rather than treating resilience as a unitary construct, therapists may use domain profiles to tailor interventions: goal-setting for low motivation, activity pacing for low tenacity, or problem-solving training for low adaptability. Given that occupational therapy remains underutilized in cardiac care (Lindsey, 2025) and evidence for its effectiveness on ADL outcomes in adults with CVD remains inconclusive (Takeda et al., 2025), resilience-informed strategies represent an occupationally grounded approach consistent with perspectives that view resilience as embedded in engagement in everyday activities (Turner et al., 2025).
Future research
Given the exploratory and cross-sectional nature of this study, future research should utilize longitudinal designs to clarify the directionality of the resilience–function relationship and to examine how resilience domains evolve in tandem with functional recovery or decline following CVD.
Larger, multisite studies would enhance statistical power and improve representativeness across diverse clinical settings, including inpatient populations and individuals with more severe functional impairments. Utilizing sampling strategies that intentionally recruit participants across a wider range of functional limitations would allow for a more precise analysis of domain-specific resilience effects.
Future studies should incorporate age-stratified or lifespan-informed analyses to clarify potential developmental influences on the relationships between resilience and function. Investigating whether specific resilience domains (e.g. self-confidence vs adaptability) differentially predict functional outcomes in midlife compared to older adulthood would enhance both theoretical and clinical understanding.
In addition, incorporating measures of instrumental ADL, social participation, and occupational engagement may provide a more comprehensive understanding of how resilience is enacted in everyday life. Mixed-method or behavioral assessment approaches could further elucidate how resilience processes are expressed beyond self-report measures.
Finally, intervention-based studies are needed to determine whether resilience-informed approaches can improve functional independence and participation outcomes in adults living with CVD.
Conclusion
This exploratory study contributes to the literature on resilience in cardiovascular populations by demonstrating that different domains of resilience are differentially associated with functional independence in ADL. Self-confidence showed the strongest association with functional independence. Achievement motivation and tenacity demonstrated directional trends favoring independence, whereas adaptability showed a weaker association. This reflects heterogeneity within the adaptability domain: high endorsement of meaning-based, belief-oriented items alongside lower endorsement of flexibility-oriented attributes may have contributed to its weaker relationship with ADL. Highlighting these patterns supports the integration of resilience-informed strategies into participation-oriented cardiac rehabilitation to promote functional independence and meaningful engagement in daily life.
Key findings
Higher resilience was significantly associated with ADL independence among adults with CVD
Self-confidence demonstrated the strongest domain-level relationship with ADL independence.
Achievement motivation and tenacity showed directional trends favoring independence, whereas adaptability showed a weak association.
What the study has added?
Using a culturally validated four-factor CD–RISC structure, this study provides novel evidence of domain-specific resilience–ADL associations in non-neurological CVD.
Footnotes
Acknowledgements
We would like to express our gratitude to the participants for their valuable cooperation and to thank Shiraz University of Medical Sciences for their financial support.
Ethical considerations
This research received approval from the Research Ethics Committees of Shiraz School of Rehabilitation Sciences, affiliated with Shiraz University of Medical Sciences, Shiraz, Iran. (approval ID: IR.SUMS.REC.1393.6414).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was financially supported by Shiraz University of Medical Sciences, Shiraz, Iran (grant number: 5047).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the author, Derakhshanrad, S.A., upon reasonable request.