
Abstract
Introduction
All children are dependent on adults for access to a dentist, diet choices and oral health support; but for children in care this responsibility falls to their carers (Ofsted, 2025). Children entering the care system will be offered an Initial Health Assessment (IHA) with an individual health plan which forms part of the child’s overall care plan, and statutory guidance recommends that dental health is included in the content of this (Department for Education and Department of Health and Social Care, 2015). Therefore, with the right education and support, health professionals have a prime opportunity to make long-term improvements to the oral health of these children and young people.
Dental decay is caused when the enamel and dentine of a tooth become softened by acid attack following sugar consumption, and gradually dissolves, leading to the formation of cavities (Oral Health Foundation, 2021). This is a largely preventable disease exacerbated by a combination of high sugar consumption and poor oral hygiene, and as well as distress, pain and infection, there can be negative impacts on eating, sleep, quality of life, speech development, self-esteem, school attendance and performance (Arora et al, 2011; Ramos-Jorge et al, 2014; Sheiham, 2006).
Care-experienced children and those with special educational needs and/or disabilities (SEND) are more vulnerable to poor oral health and, despite having the greatest need, dental practice attendance is poorest in these deprived groups (Welsh Government, 2018).
A project to deliver enhanced oral health promotion at the IHA of children in care attending Brighton General Hospital between April 2024 and June 2024 was undertaken to gather baseline oral health status at entry to care, and to visually examine the teeth and gums alongside providing personalised oral health advice.
The dental project
The project had the following aims:
to determine oral health status by looking in the mouth (lifting the lip); to provide an oral health demonstration of how to clean teeth effectively; to gather information around the external factors impacting oral health.
Method
The sample included children who received an IHA in Brighton and Hove between 1 April 2024 and 30 June 2024 and who were aged between 2–18 years. A total of 13 children met these criteria. Three children were excluded because they were discharged from the service in the weeks following their IHA, and one child would not engage in any follow-up. Patient data was anonymised. Alongside gathering information about the type of placement, level of support and barriers the child might experience, we devised a Likert-type scale that allowed an individual to rate how much they agreed or disagreed with the statements (see below); the five-point scale had ordered response options with numerical values attached, which enabled us to produce quantitative data for comparison and analysis.
Teeth and oral hygiene status (rudimentary inspection of the mouth). Brushes teeth with fluoride toothpaste (appropriate for age). High sugar diet. High sugar drinks. Following oral health promotion advice. Dental registration.
During the IHA (a doctor/nurse joint model), consent was gained from the child/young person to look in their mouth: the dental proforma was completed and each child was provided with a practical demonstration of how to clean their teeth correctly and given a toothbrush, fluoride paste and written oral health promotion literature to take away. A three-month IHA follow up was completed by the same nurse at home, and this provided an opportunity to build on the relationship, reinforce positive oral health messages and for a further practical demonstration. The dental proforma was updated.
Results
Oral health status was measured exclusively using the Likert-type scale-based response model to benchmark, and the variables that we considered to have the most impact on oral health were collected separately; as this was a small project to inform our local practice we did not test for statistical significance. In all nine children and young people, there was a measurable improvement to oral health after three months of being in care (Figure 1):
Total combined scores for all children at IHA and three-month follow-up.
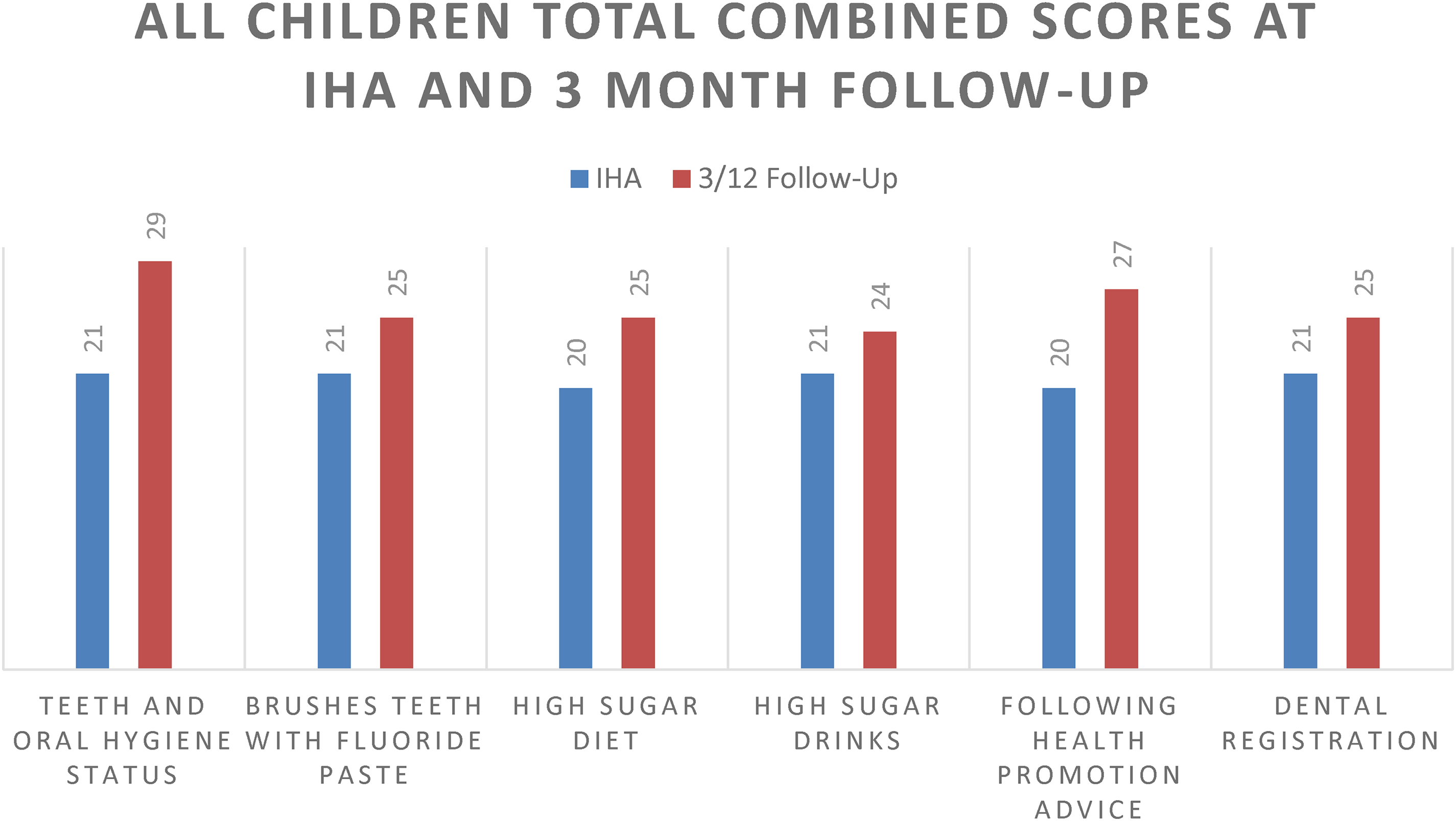
A Radar chart which displays multivariate data stacked at an axis with the same central point was used to compare oral health benchmarking for individual children; however, it was unable to account for the complex variables each experienced, such as type of placement and level of support, or barriers such as language and additional needs (Figure 2).
Oral health benchmarking for child 7.
The data in Figure 2 demonstrates that there was improvement in the areas of teeth and oral health status; brushing teeth with fluoride paste; and following health promotion advice. However, the child continued to consume a high sugar diet with high sugar drinks, and there had been no improvement in the three-month period following the IHA.
Discussion and future work
Although the same nurse completed the follow-up at three months, the nurses reflected that the Likert-type scale within the tool was restrictive, and responses were subjective as the difference between ‘always’, ‘often’, and ‘sometimes’ on a frequency response Likert scale is open to interpretation and not necessarily equal (Sullivan and Artino, 2013); therefore, it was concluded that the information could be captured in the dental section of health assessment paperwork without completing an additional tool, and the updated CoramBAAF paperwork (2025) has prompts for dental registration, a teeth/mouth check, and brushing of teeth with space for free text comments. There are many barriers to improving oral health status for children in care, and dental health is one of several competing priorities they face. However, the children/young people all engaged well with the practical teeth brushing demonstration, and the team felt that the key to improvement was the practical oral health demonstration, which allowed the nurses to deliver oral health promotion messages in a fun way.
Challenges
Many local authorities in England are currently experiencing placement insufficiency causing high rates of placement instability, out of area placements and poor health outcomes (The Children’s Society, 2022). Therefore, it is difficult to build on oral health education completed during the IHA for children who experience multiple moves and multiple carers. Moreover, we found anecdotal evidence of inconsistent compliance with health care plans, in particular for children placed in residential placements or with kinship carers/birth parent(s), where advice is not always followed and dental services not accessed.
Barriers to cover the dental health agenda during the IHA
Children entering the care system often have complex health needs, including undetected mental health issues, developmental delay and missed appointments; therefore, emerging priorities during the IHA (or during subsequent contact) can negatively impact on opportunities to cover the full scope of the dental health agenda (Wilson, 2024), and any engagement difficulties such as language barriers or refusal to participate will have a further negative impact.
Barriers to accessing dental services
The NHS is currently facing a severe NHS dentistry shortage with 97% of new patients unable to access NHS care (British Dental Association, 2024). Children are adversely affected and this is a primary reason for hospital admission. The costs to the NHS of hospital admissions for tooth extractions in children aged 0 to 19 years have been estimated to be £64.3 million for all tooth extractions and £40.7 million for decay-related tooth extractions in the financial year 2022 to 2023 (Gov.Uk, 2024). Therefore, improvements to oral health for children in care will demonstrate a cost saving benefit to the NHS if dental extractions can be prevented.
Long-term improvements to oral health status will only be achieved in conjunction with formal referral pathways for children in care to access timely NHS dental registration. This is not the case in this locality, and being a child in care is not a referral criterion for Special Care Dentistry. However, an Urgent Dental Care and Stabilisation Programme has been commissioned in Sussex which will provide an urgent appointment with an NHS dentist for children in care and care leavers (amongst other identified vulnerable groups), and future work should focus on commissioning pathways for children in care to be prioritised for routine dental treatment, and for Special Care Dentistry to take referrals from this cohort if NHS dental services cannot be accessed.
Recommendations
The project led to the following recommendations:
Health professionals completing statutory health assessments for children in care need annual oral health education, so that they maintain the competencies required to improve oral health status. Foster and kinship carers should be offered regular training, so that they have a better understanding of how to support oral health status. The electronic health record template should be reviewed and a tick box for collecting data on which children/young people have had a practical tooth brushing demonstration should be added. This will enable the identification of children who have received the practical demonstration to aid future audits. The practical tooth brushing demonstration should be expanded to all initial and review health assessments.
There is scope to capture data from a larger sample group at the Review Health Assessment in the future.
In conclusion, although this was a very small sample group, we found that when children and carers are provided with enhanced oral health education combined with a practical demonstration, it is possible to make immediate and positive improvements to oral health.
Footnotes
Author biographies
Health notes are edited by