
Abstract
This longitudinal study examines the reciprocal relationships between self-reported personal and contextual resources, mental health (internalising and externalising symptoms) and wellbeing in adolescents in out-of-home care (OOHC) compared to adolescents living with their biological families (BF). Data from two measurement points (T1, T2) were analysed using path models and multivariate analyses of variance. The results show stabilities of mental health over time in both groups, with wellbeing being less stable for adolescents in OOHC. Comparisons of different models with varying cross-lagged paths showed that the best model fit was found for the mental health-directed model, in which higher personal resources at T1 predicted significantly higher wellbeing scores in both groups at T2. In the OOHC group, higher personal resources at T1 were also associated with lower externalising symptoms at T2. Furthermore, the placement type (OOHC vs BF) proved to be a significant moderator. Adolescents in OOHC reported significantly fewer personal resources and more externalising symptoms. The findings emphasise the preventative importance of personal resources and argue for resource-oriented interventions, especially for at-risk adolescents in OOHC. In the long term, stable, validating care environments could promote the development of personal resources and encourage good mental health.
Plain language summary
This study looked at how young people growing up in foster or adoptive families are doing and compared them to those growing up with their biological parents. The researchers wanted to understand the role of resources in the mental health of adolescents. Resources in this context include strengths that help young people to cope better with challenges. These comprise internal strengths – such as self-confidence or optimism – as well as external support, like having people around who help them, listen to them and make them feel safe. The young people were surveyed twice, six months apart. The study found that adolescents with more resources felt better and had fewer mental health problems, whether they lived in foster/adoptive or biological families. This was especially true for internal strengths: those who reported having many internal strengths at the first time point also reported greater wellbeing six months later. For adolescents living in foster or adoptive families, these strengths were also linked to fewer behavioural problems. Overall, young people in foster or adoptive families reported fewer internal strengths and more behavioural difficulties. This is likely due to challenging experiences earlier in their lives. However, their overall wellbeing was not worse than that of their peers. This suggests that a placement in a supportive environment can make a big difference. The results highlight that it is important not only to support adolescents when they have problems, but also to strengthen their personal resources and support systems – especially for those who have experienced difficulties early in life.
Keywords
Introduction
Out-of-home are (OOHC) represents a central component of the child protection system in Germany. Each year, approximately 70,000 children and adolescents are placed under the care of child and youth services. While some of them return to their original family environment, a significant proportion (around 50%) grow up temporarily or permanently in alternative care arrangements, such as foster families, residential groups or adoptive families (Statistisches Bundesamt, 2024b). In recent years, the number of adoptions has declined in Germany (Statistisches Bundesamt, 2024a), whereas foster care and residential facilities are increasingly utilised (Statistisches Bundesamt, 2024c). The reasons for OOHC are multifaceted and often include neglect, abuse or family instability (Fisher et al., 2023; Vasileva and Petermann, 2017). Such experiences may undermine the ability of children and adolescents living in OOHC to develop healthy psychosocial functioning, leading to higher rates of externalising and internalising symptoms (Fernandez, 2008; Linderkamp et al., 2009). Adolescence represents a sensitive and critical developmental period in this context, characterised by significant physical, cognitive and emotional changes. It is also a time when individuals are highly sensitive to the social and environmental influences that shape their wellbeing and mental health (Steinberg, 2005). For adolescents growing up in OOHC, the challenges they face are often exacerbated by early adversities (Fisher et al., 2023; Vasileva and Petermann, 2017). The extent to which adolescents in OOHC are able to cope with these challenges and achieve positive developmental outcomes depends on the availability and stability of both personal and contextual resources (Gervin et al., 2022; Masten et al., 2009).
Personal resources, including individual strengths such as self-esteem, emotional regulation, optimism and empathy, are crucial factors influencing the mental health and wellbeing of adolescents in OOHC and biological families (BF) (Dunkel et al., 2024). Studies of adolescents growing up in their BF showed that higher levels of personal resources were typically associated with fewer internalising and externalising symptoms and higher levels of wellbeing (Bastiaansen et al., 2005; Kvarme et al., 2009). Longitudinal studies with adolescents in BF showed that low self-esteem was associated with increased internalising (In-Albon et al., 2017; Li et al., 2023; Metsäpelto et al., 2020) and externalising symptoms (Zimmermann et al., 2013). Moreover, high self-control was linked to better mental health outcomes (Tangney et al., 2004). A longitudinal study indicated that adolescents’ self-confidence predicted their wellbeing (Oriol and Miranda, 2024), while other findings suggested that higher wellbeing was associated with subsequent increases in self-esteem among adolescents in BF (Lin and Yi, 2019). Although longitudinal evidence in this context is limited for adolescents in OOHC, cross-sectional findings demonstrated positive associations between higher personal resources and wellbeing among this group (Davidson-Arad and Klein, 2011; Greger et al., 2017). Additionally, personal resources, such as self-confidence and optimism, act as protective factors for mental health of adolescents in OOHC (Costa et al., 2020). However, the development of these resources was often hindered by the traumas associated with early life experiences in adolescents in OOHC (Lin and Yi, 2019).
Contextual resources, including peer group and school integration, parental social and emotional support and authoritative parenting, also play a crucial role in promoting wellbeing and good mental health (Masten et al., 2009; Obsuth et al., 2024). These resources may mitigate the negative effects of early trauma and foster positive psychosocial outcomes. Adolescents in OOHC, however, often face challenges in establishing stable, supportive relationships and environments due to the disruptions and instability associated with foster and adoptive placements (DeLuca et al., 2019; Farineau et al., 2013). In contrast, adolescents in BF frequently benefit from more stable environmental resources, including supportive parental relationships and stable social networks (Petermann and Schmidt, 2006). Studies with adolescents in OOHC showed that fewer contextual resources were associated with poorer mental health (Beeri and Lev-Wiesel, 2012) and lower wellbeing (Albarello et al., 2021). Longitudinal studies revealed that adolescents in BF who experienced poor school integration or peer rejection later exhibited poorer mental health (Felix et al., 2019). Furthermore, a 12-year follow-up study on adolescents living in BF found that peer rejection predicted poorer mental health, whereas strong friendships exhibited higher general self-esteem in adulthood (Bagwell et al., 1998). Likewise, a long-term study showed that poorer mental health, such as increases in internalising symptoms, was also associated with greater peer rejection six months later (Frison et al., 2016). Cross-sectional and longitudinal studies also highlighted positive associations between contextual resources and wellbeing. In particular, school integration (Obsuth et al., 2024), authoritative parenting (Francis et al., 2021) and peer group integration (Hoferichter et al., 2021) were identified as relevant contextual resources with regard to wellbeing. Adolescents in OOHC frequently reported lower levels of school and peer group integration, which were linked to poorer psychosocial outcomes (Benbenishty et al., 2018). However, higher school integration of adolescents in OOHC was associated with fewer internalising and externalising symptoms (Mihalec-Adkins and Cooley, 2020), as well as authoritative or permissive parenting styles (Fuentes et al., 2015). As with personal resources, previous research on adolescents in OOHC often relied on cross-sectional findings.
The present study aimed to investigate the role of personal and contextual resources for mental health and wellbeing longitudinally. More precisely, it examined whether resources act primarily as predictors of internalising and externalising symptoms and wellbeing or whether these mental health outcomes predict resources over time. This was analysed in adolescents in OOHC compared to those raised in BF in two assessments conducted six months apart. It was assumed that there would be stability over time within the individual constructs between the two time points, i.e., that internalising and externalising symptoms, wellbeing, and resources at the first measurement point (T1) would predict the repeated measurement of the corresponding construct at the second measurement point (T2; Hypothesis 1). Furthermore, it was expected that, beyond the stability of internalising and externalising symptoms and wellbeing over time, higher levels of personal and contextual resources at T1 would predict lower levels of internalising and externalising symptoms and higher levels of wellbeing at T2 (Hypothesis 2). Vice versa, it was also expected that lower levels of internalising and externalising symptoms and higher levels of wellbeing at T1 would predict higher levels of resources at T2 (Hypothesis 3). Finally, both directions were analysed simultaneously to examine bidirectional effects. Additionally, the study aimed to examine the extent to which differences exist between adolescents in OOHC and those growing up in their BF regarding both the stability of the relationships and cross-lagged relationships (Exploratory Research Question).
Method
Participants and procedure
The present study was conducted as an online survey between May 2020 and January 2022, with two measurement points at an interval of about half a year (T1 and T2). This interval was chosen primarily for organisational reasons and to minimise the risk of a high dropout rate, which could have occurred with a longer period between assessments. Participants were recruited via multiple channels, including adolescent welfare offices, foster and adoptive family associations across Germany, social media platforms, local newspapers and schools. Families who showed interest in the study contacted the research team to obtain detailed information and register for participation. The initial sample consisted of 183 adolescents aged 11 to 21 years. Due to dropout between the two measurement points, 136 adolescents participated at both T1 and T2. The included and excluded cases did not differ regarding the relevant variables at the first measurement point (all t-values between 0.25 and 0.50, all p > .60), indicating no systematic differences.
The BF group consisted of 76 adolescents (53% female) with a mean age of 14.80 years (SD = 3.38) at T1. Five participants of the OOHC group were excluded from the analysis because they lived in residential care groups, a subgroup that was too small for separate statistical analyses. After this subgroup was excluded, the OOHC group comprised 60 adolescents (52% female), with a mean age of 14.08 years (SD = 2.50) at T1. Participants were, on average, approximately six months older at T2. All participants, along with their legal guardians when applicable, provided informed consent prior to their participation. Upon completing the questionnaires, participants received a 20€ voucher for a store of their choice. The study was approved by the local ethics committee of Bielefeld University (EUB 2019-180) and was funded by the German Federal Ministry of Education and Research (BMBF, Funding code 01KR1806B).
Measures
Mental health
Using the German version of the Youth Self-Report (YSR/11-18R; Döpfner et al., 2014), the adolescents reported on their mental health at both measurement points. This questionnaire was used to assess internalising symptoms (e.g., anxiety and depression), and externalising symptoms (e.g., aggressive and disruptive behaviour). The adolescents indicated on a 3-point Likert scale how often they had recently been affected by these symptoms, ranging from 0 (‘Never’) to 2 (‘Often’). In this study, composite scales for internalising and externalising symptoms were used, based on the sum values of the respective items. Higher scores indicate higher levels of mental health problems. One item relating to suicidality was removed due to ethical concerns, as the online format did not allow for direct contact with participants in the event of a positive response. If more than eight items were missing, no scale value was computed; if fewer than eight items were missing, missing values were replaced using the mean of the available items. In the current sample, the Internalization scale (30 items) achieved an internal consistency Cronbach's αOOHC = .91 and αBF = .93 at T1. At T2, the internal consistencies were very similar with αOOHC = .90 and αBF = .94. The Externalization scale (32 items) achieved αOOHC = .84 and αBF = .86 at T1. At T2, the internal consistencies were αOOHC = .88 and αBF = .88.
Wellbeing
The adolescents’ wellbeing was determined using the KIDSCREEN-27 (The KIDSCREEN Group Europe, 2006) at both measurement points. The self-report questionnaire comprises 27 items with a 5-point response scale ranging from 1 (‘Never’/‘Not at all’) to 5 (‘Always’/‘Very much’). The items cover the five areas of physical wellbeing, psychological wellbeing, autonomy and relationship with parents, peers and social support, and school environment. In this study, the general Wellbeing scale was used by calculating an overall mean value across all items. According to the KIDSCREEN manual, the total mean score can be used only for cases with no more than one missing item per scale. The internal consistencies (Cronbach’s α) for wellbeing were αOOHC = .90 and αBF = .93 at T1. At T2, the internal consistencies for the overall wellbeing scale were αOOHC = .92 and αBF = .95.
Resources
The Questionnaire to Assess Resources of Children and Adolescents (QARCA; Lohaus and Nussbeck, 2016) was used to record the adolescents’ personal and contextual resources at both measurement points. The questionnaire consists of 60 items covering Personal Resources (36 items) and Contextual Resources (24 items). The Personal Resources include empathy and perspective-taking, self-efficacy, self-esteem, sense of coherence, optimism and self-control. The Contextual Resources include parental emotional and social support, authoritative parenting style, integration into the peer group and school integration. All resources were assessed with six items each. The items were answered by the adolescents using a 4-point scale ranging from 1 (‘Not true’) to 4 (‘Often true’). If at least five out of six items answers were available, the participants` scale means were computed for overall personal and contextual resources. At T1 the internal consistencies (Cronbach’s α) in this study were αOOHC = .94 and αBF = .96 for personal resources, αOOHC = .91 and αBF = .95 for contextual resources. At T2 the internal consistencies were αOOHC = .94 and αBF = .97 for personal resources, αOOHC = .92 and αBF = .95 for contextual resources.
Statistical analyses
Statistical analyses were performed using IBM SPSS 29 and Mplus Version 8 (Muthén and Muthén, 1998–2017). Missing data at the scale level were imputed using multiple imputation. The percentage of missing values imputed ranged from 0% to 17%, depending on the scale. Following the guidelines of Asendorpf and colleagues (2014), imputation was carried out with 20 imputed datasets. In addition to family placement (OOHC vs BF) and the scales used to test the study’s hypotheses, adolescents’ gender and age were included as predictor variables for the multiple imputation at the scale level. All analyses were then conducted using a dataset aggregated from the 20 imputed datasets. Using Mahalanobis distances, 14 multivariate outliers were identified. As these cases did not result from incorrect data entry and analyses conducted with and without the outliers yielded similar results, these cases remained in the sample for analyses.
Before the hypotheses were tested, a MANCOVA (Multivariate Analysis of Covariance) was calculated to analyse differences between the OOHC and the BF groups with regard to internalising and externalising symptoms, wellbeing and resources (including age and gender as covariates). Prior to conducting the MANCOVA, the assumptions underlying the MANOVA were considered. Normality was examined using Shapiro-Wilk tests and visual inspection of Q-Q-plots. Although some Shapiro-Wilk tests were significant (p < .05), visual inspection indicated only minor deviations from normality. Given the sample size, the analyses are considered robust against these deviations. The homogeneity of variance between groups was examined for all dependent variables at both measurement points using Levene’s test. Variances were largely homogeneous, except for internalising symptoms at T1 and externalising symptoms at T2, where Levene’s test was significant (p < .05). Therefore, and because of the minor deviations of normality, the robust multivariate statistic Pillai’s Trace, which is considered less sensitive to violations of these assumptions, was used for the interpretation of the effects. The homogeneity of covariance matrices between groups was examined using Box’s M test. The test was not significant (p > .01), indicating that the assumption of equal covariance structures of the dependent variables was met. The relationship between covariates and dependent variables was approximately linear. As shown in Table 1, no problematic multicollinearity was present. Since there were only two measurement points, the assumption of sphericity was automatically met, and a Mauchly test was not required.
Correlations between the study variables for adolescents living in OOHC (n = 60; presented below the diagonal) and for adolescents living in BF (n = 76; presented above the diagonal).
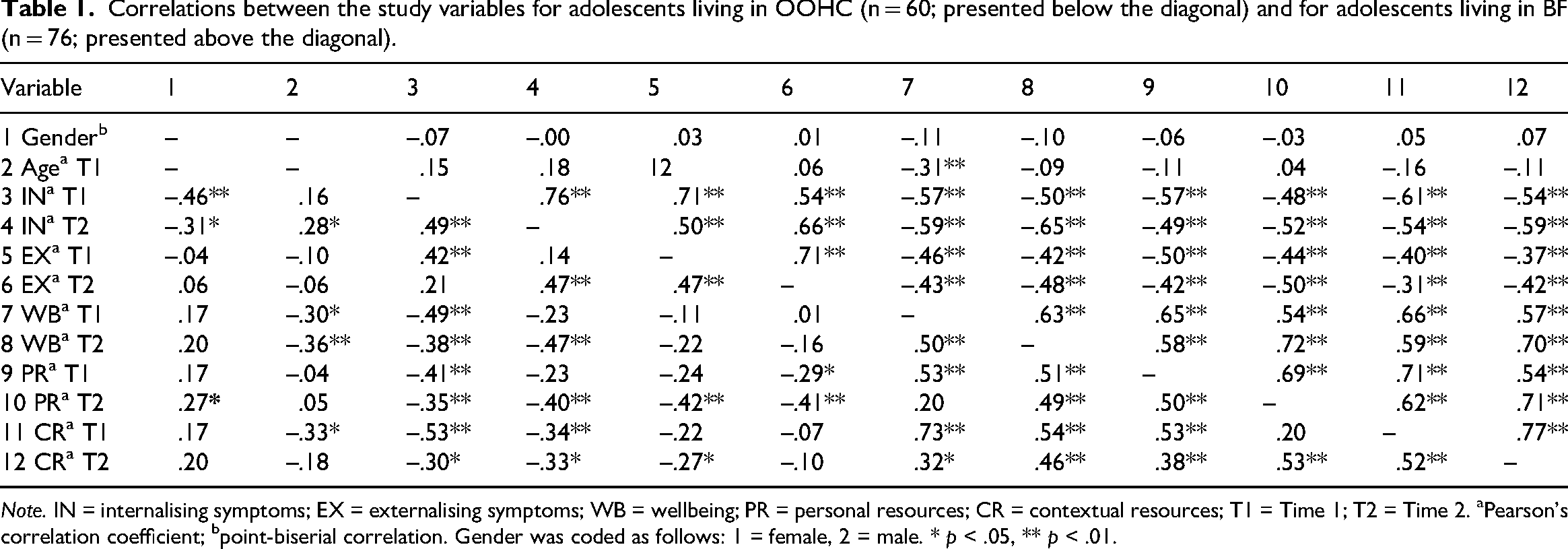
Note. IN = internalising symptoms; EX = externalising symptoms; WB = wellbeing; PR = personal resources; CR = contextual resources; T1 = Time 1; T2 = Time 2. aPearson’s correlation coefficient; bpoint-biserial correlation. Gender was coded as follows: 1 = female, 2 = male. * p < .05, ** p < .01.
To test the hypotheses of this study, Cross-Lagged Panel (CLP) analyses were conducted. CLP models are used to analyse reciprocal relationships between multiple variables longitudinally. They allow for the investigation of directed effects by testing whether one variable at T1 predicts another variable at T2 and vice versa. The CLP models were computed as path models with manifest variables. Given the non-normal distribution of the data, the robust maximum likelihood estimator (MLR) was used. Model fit can be assessed using fit indices such as the Comparative Fit Index (CFI) and the Root Mean Square Error of Approximation (RMSEA). For a good model fit, the CFI should have a value of ≥ .97 and for an acceptable model fit a value of ≥ .95. An RMSEA ≤ .05 indicates a good model fit and an RMSEA > .05, and ≤ .08 an acceptable model fit (Schermelleh-Engel et al., 2003).
In this study, four models were computed to test the hypotheses (Figure 1). To test Hypothesis 1, a baseline autoregressive model was specified (stability model) in which internalising and externalising symptoms, wellbeing, and personal and contextual resources at T1 predicted their corresponding values at T2. To test Hypothesis 2, a CLP model was tested (mental health-directed model), in which resources at T1 were specified as predictors of internalising and externalising symptoms and wellbeing at T2, while accounting for the stability of these constructs over time. For testing Hypothesis 3, another CLP model was estimated (resources-directed model). In this model, in addition to the stability paths, internalising and externalising symptoms as well as wellbeing at T1 predicted resources at T2 to examine whether these variables predicted changes in resources over time. Finally, the reciprocal model combines Models 2 and 3 by incorporating bidirectional cross-lagged paths of resources with internalising and externalising symptoms and wellbeing to test for reciprocal relationships. Across all models, the same variables were included and differences between models were based on variations in the specification of cross-lagged associations. This stepwise approach allows for a systematic investigation of predictive relationships while accounting for stability over time (Newsom, 2023). The comparison of the models is based on goodness-of-fit indices. A commonly used test is the χ2- difference test (Δχ2, Δdf, p-value), which examines whether nested models differ significantly. Since the MLR estimator does not allow for conventional χ2-difference tests, adjustments were made following the guidelines provided by Satorra and Bentler (2010).
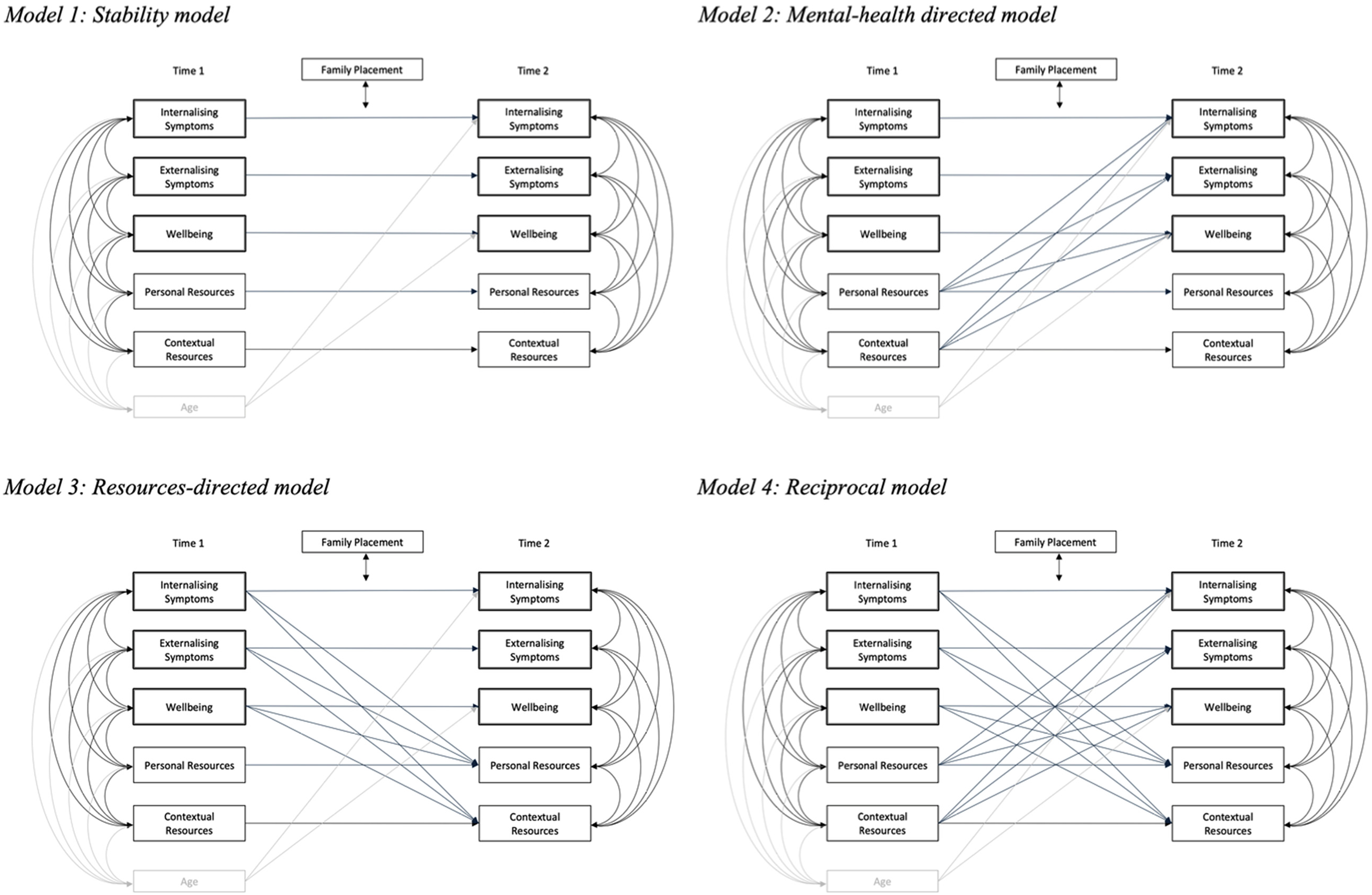
Theoretical path models on the directionality of the links between internalising and externalising symptoms, wellbeing, and resources at Time 1 and Time 2 with family placement as moderator and age as control variable.
Initially, age and gender were included as control variables for the variables that showed significant correlations with age or gender (Table 1). To maintain model parsimony and avoid unnecessary complexity, paths that were not significant in the model were gradually removed. Ultimately, only age remained as a control variable for internalising symptoms and wellbeing.
To test the moderating role of family placement (OOHC vs BF), a Multi-Group Analysis (MGA) was conducted for each of the models described above. Each model was specified in a constrained and an unconstrained version. In the unconstrained model all parameters were allowed to vary freely between groups, whereas in the constrained model certain paths were set equal across groups. If imposing these constraints resulted in a significantly worse model fit, this indicated the presence of potential moderation of the relationships between the variables. If no moderation was found, the analysis proceeded with a Single Group Analysis (SGA). If moderation was detected, Multi-Group Analysis (MGA) with unconstrained models was used for further analyses.
Results
Preliminary analyses
As expected, numerous significant correlations were found between the variables used at both time points (Table 1). These significant correlations serve as the basis for the subsequent analyses. Before conducting the path analyses, a MANCOVA with repeated measures (with age and gender as control variables) was performed to examine whether there were significant differences between the groups (OOHC vs BF) regarding internalising and externalising symptoms, wellbeing and resources.
The MANCOVA revealed a significant multivariate main effect of group, F(5, 128) = 5.09, p < .001, Pillai’s Trace = .166. As univariate analyses showed (Table 2), adolescents living in OOHC reported significantly more externalising symptoms and significantly fewer personal resources in comparison to adolescents living in their BF at both measurement points. The MANCOVA also revealed a significant multivariate main effect of time, F(5, 128) = 2.48, p .035, Pillai’s Trace = .088. There was an overall significant decrease in personal resources between T1 and T2 (Table 2). The interaction effect between time and group was not significant. Regarding the covariates, there was a significant multivariate main effect for gender, F(5, 128) = 2.59, p .029, Pillai’s Trace = .092, and for age, F(5, 128) = 4.20, p .001, Pillai’s Trace = .141. Older adolescents reported significantly more internalising symptoms, worse wellbeing, and fewer contextual resources. Girls reported significantly more internalising symptoms, whereas no significant multivariate main effect for gender was found for wellbeing, externalising symptoms or resources. A post hoc power analysis using G*Power showed for the repeated-measures MANCOVA that the estimated power to detect multivariate effects at a significance level of α = .05 was approximately 0.80–0.85, indicating sufficient power to detect moderate to large effects.
Differences between adolescents in OOHC (n = 60), and BF (n = 76) regarding their mental health and resources (univariate effects) at T1 and T2.
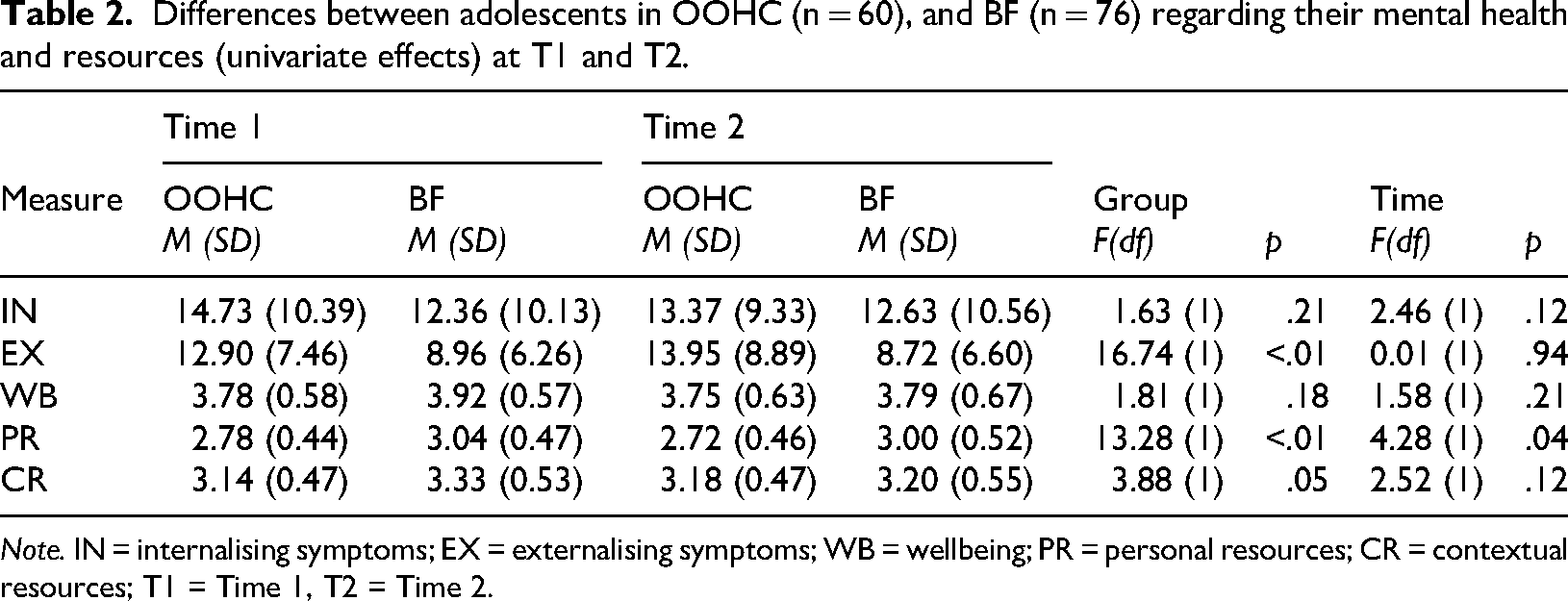
Note. IN = internalising symptoms; EX = externalising symptoms; WB = wellbeing; PR = personal resources; CR = contextual resources; T1 = Time 1, T2 = Time 2.
Main analyses
Moderating role of family placement (Exploratory Research Question)
Unconstrained models were compared to constrained models, and significant differences were found in Models 1, 2 and 3, indicating a moderating effect of family placement (Table 3). Although there was no significant moderation in Model 4, the unconstrained models (free models) had superior fit indices compared to their constrained counterparts (Table 3).
Multi Group Analyses: Comparison of cross-lagged unconstrained and constrained models to test the moderation effect of family placement.
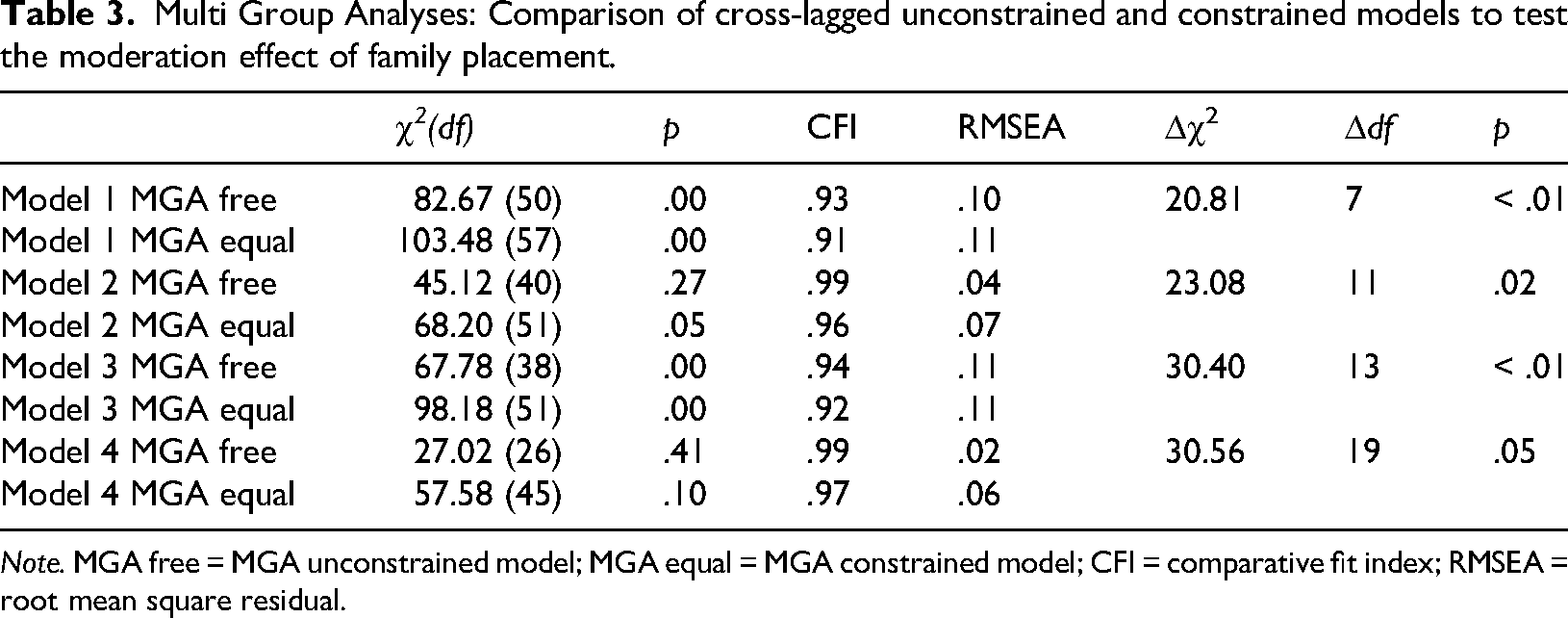
Note. MGA free = MGA unconstrained model; MGA equal = MGA constrained model; CFI = comparative fit index; RMSEA = root mean square residual.
Comparison of cross-lagged models and path coefficients
Subsequent analyses (MGA) focused on the unconstrained models. CLP analyses were conducted to compare the models with different cross-lagged paths (stability model, mental health-directed model, resources-directed model, reciprocal model). As shown in Table 4, the mental health-directed model aligned best with the observed data. It consistently demonstrated a good model fit, χ2(40) = 45.12, p = .27, CFI = .99, RMSEA = .04. In comparison, the stability model exhibited a significantly higher χ2-value (p < .01). The resources-directed model showed a high RMSEA value of .11 and a significant p-value, indicating that it did not fit the data well (Table 4). While the reciprocal model provided a good fit, it was more complex and less economical than the mental health-directed model (Table 4). Therefore, the mental health directed model (Model 2) was selected as the optimal and final path model.
Multi Group Analyses: Comparison of cross-lagged unconstrained models.
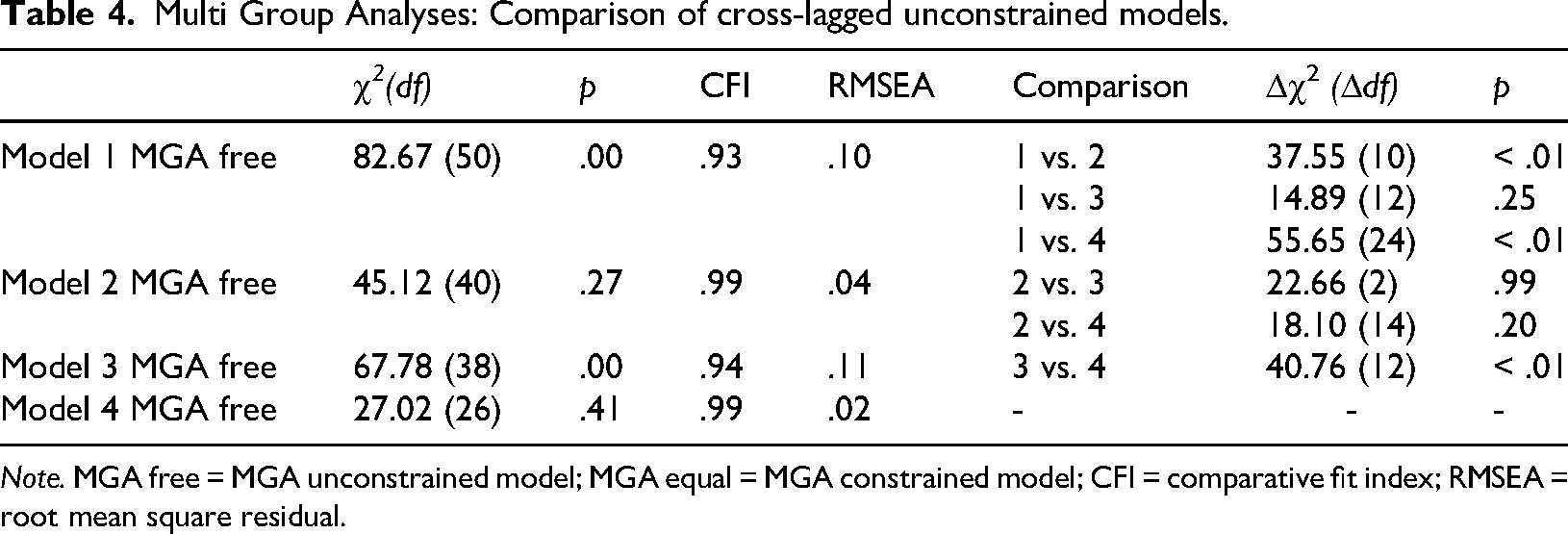
Note. MGA free = MGA unconstrained model; MGA equal = MGA constrained model; CFI = comparative fit index; RMSEA = root mean square residual.
For the cross-lagged panel analyses (Model 2), a post hoc power analysis using G*Power showed that the power to detect individual, moderately large paths from Personal Resources (T1) to Internalising Symptoms, Externalising Symptoms, and Wellbeing (T2) at α = .05 was estimated between 0.88 and 0.89 for path coefficients of β ≈ .25, and 0.96 for β ≈ .30. These results indicate adequate power to detect moderate to large cross-lagged effects.
In the following, the focus is on examining the individual pathways within Model 2 to gain deeper insights into the relationships between resources and mental health outcomes.
In the group of adolescents in OOHC (Figure 2) the autoregressive paths (stability) of internalising and externalising symptoms as well as of personal and contextual resources were significant. In contrast, wellbeing at T1 was not associated with wellbeing at T2 in this group. Regarding the cross-lagged paths, more personal resources at T1 were associated with fewer externalising symptoms at T2 and higher wellbeing at T2. In the BF group (Figure 3), similar associations as in the OOHC group were observed, showing significant autoregressive paths between T1 and T2 for internalising and externalising symptoms, personal resources and contextual resources. Unlike the OOHC group, wellbeing at T1 was significantly associated with wellbeing at T2 in the BF group. Regarding the cross-lagged paths, personal resources at T1, as in the OOHC group, were positively associated with wellbeing at T2, but in contrast to the OOHC group they were not associated with externalising symptoms at T2. Regarding the control variable age, the OOHC group showed that older age was associated with significantly more internalising symptoms and poorer wellbeing; these associations were not found in the BF group.
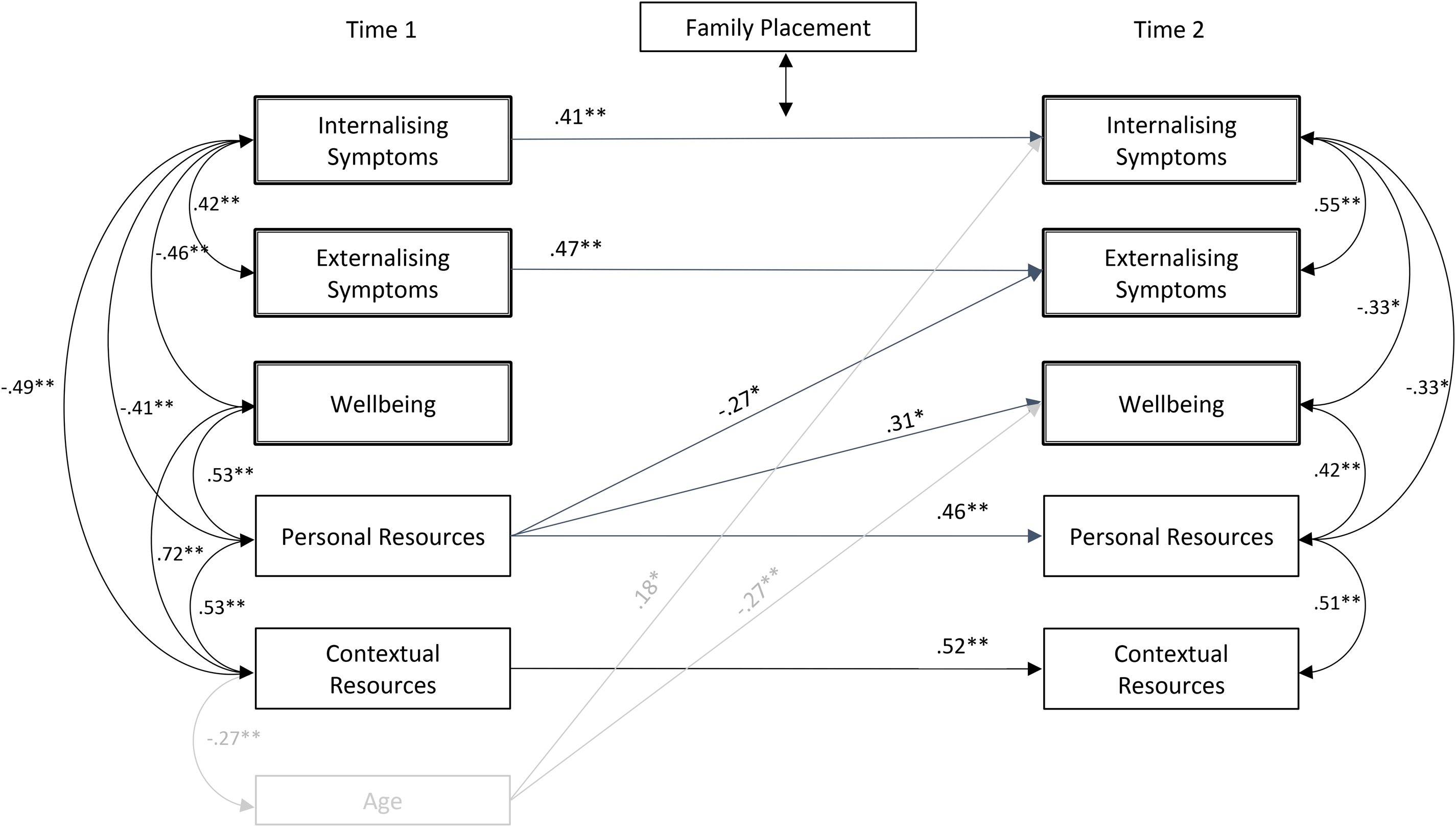
Mental health-directed model of adolescents in Out-of-home care (OOHC) with resources of adolescents at Time 1 as predictors for mental health at Time 2.
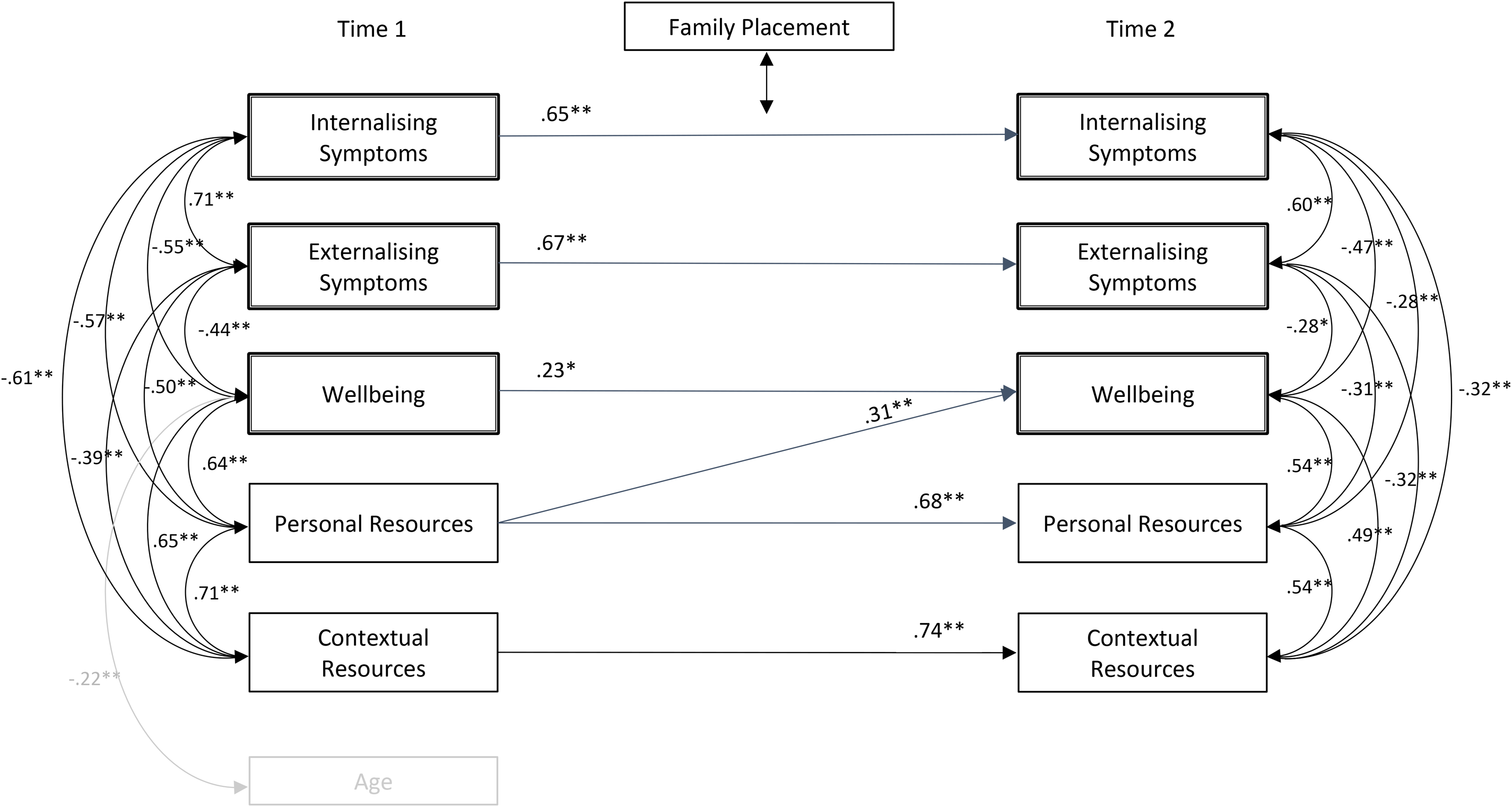
Mental health-directed model of adolescents in Biological Families (BF) with resources of adolescents at Time 1 as predictors for mental health at Time 2.
Discussion
The aim of the study was to investigate the reciprocal influence of personal and contextual resources as well as mental health and wellbeing in adolescents in OOHC and those in birth families over a longitudinal period. The study confirms the stability of internalising and externalising symptoms, wellbeing, and resources over time (Hypothesis 1). However, an exception was observed in the group of adolescents in OOHC: wellbeing at the first measurement point (T1) did not significantly predict wellbeing at the second measurement point (T2). This finding aligns with previous studies suggesting that wellbeing among adolescents in care settings is more volatile due to contextual changes and individual adjustment processes (Goemans et al., 2015). These findings can also be interpreted in light of the theory of latent vulnerability (McCrory et al., 2022; McCrory et al., 2017). Adolescents in OOHC often have histories of early adversity, which may have induced latent vulnerability through altered stress and reward processing. Such latent vulnerabilities may contribute to the observed instability in wellbeing, despite improvements in the current care environment. At the same time, the development of personal resources within OOHC may mitigate some of this risk, thus highlighting the dynamic interplay between early adversity, current context and individual adaption. In addition to the challenges posed by these processes, positive changes may also occur within OOHC, especially when stability and supportive structures are present (Goemans et al., 2015; Pecora et al., 2006). Consequently, both negative and positive developments may occur, which may explain the observed lack of stability in wellbeing within this group. Nonetheless, no significant differences in mean values were found between the groups, indicating that although adolescents in OOHC may experience greater individual fluctuations, on average they do not report lower wellbeing than their peers living with their BF.
The mental health-directed model – whereby greater resources at T1 predict lower internalising and externalising symptoms and higher wellbeing at T2 – proved to be the best-fitting model (Hypothesis 2). Personal resources played a pivotal role: in both groups, higher personal resources were associated with greater subsequent wellbeing, thereby showing a pattern consistent with prior research on the protective function of resources (Masten and Barnes, 2018). Interestingly, personal resources did not significantly predict internalising symptoms in either group. One possible explanation is that internalising symptoms, such as anxiety or depression, may be more deeply rooted in individual emotional histories or shaped by relational dynamics that were not captured by the resource measures used. Alternatively, the relatively short time span between T1 and T2 may not have been sufficient to observe meaningful changes in these more entrenched symptoms. In the OOHC group, higher personal resources were also associated with fewer externalising symptoms. Previous research has similarly emphasised the role of personal resources in fostering wellbeing and reducing problematic behaviours, especially in at-risk adolescents (Bastiaansen et al., 2005; Luthar and Eisenberg, 2017). These findings align with resilience theories, which emphasise the role of internal assets – such as self-efficacy, optimism and self-regulation – as protective factors that buffer against adversity (Masten and Barnes, 2018). In this context, personal resources function as key mechanisms that promote adaptation and psychological wellbeing, particularly for youth facing chronic stress or early adversity, such as those in OOHC.
In contrast, Hypothesis 3, which assumed that higher wellbeing and lower symptoms at T1 would predict greater resources at T2, was not supported. The corresponding model showed a poor fit, suggesting that resources are more likely to be stable, predisposing protective factors rather than outcomes influenced significantly by symptom trajectories (e.g., Alvord and Grados, 2005; Masten and Barnes, 2018).
Regarding the Exploratory Research Question, results indicated that placement type moderated the observed effects. In this context, it is worth revisiting the development and characteristics of the variables relevant to this model. Personal resources typically develop in early childhood (Hohm et al., 2017). When basic needs for secure relationships, recognition, appreciation, significance, autonomy and the inviolability of personal boundaries are met (Sachse, 2015), adaptive development of personal resources, such as empathy and perspective-taking, self-efficacy, self-esteem, sense of coherence, optimism and self-regulation, can occur (Hohm et al., 2017). However, adolescents in OOHC often have histories marked by invalidation of these basic needs (Vasileva and Petermann, 2018), which hampers the development of personal resources, resulting in lower levels of such resources during adolescence (Dunkel et al., 2024). This finding is reflected in the mean comparisons of the present study, which show that adolescents in OOHC report significantly fewer personal resources. Nonetheless, placement in OOHC puts these adolescents in a different environment, where – at least conceptually – greater validation should be possible (Saarnik, 2021). One indicator that this is often the case is the absence of significant mean differences in wellbeing, internalising symptoms and contextual resources in this study. At the same time, adolescents in OOHC reported significantly more externalising symptoms. Just like personal resources, emotion regulation strategies also develop during early childhood, and it can be assumed that invalidating environments foster less adaptive co-regulation and more maladaptive modelling (Bandura, 1976; Schore, 2001; Ulrich and Petermann, 2017). Thus, early traumatic experiences – which are common among adolescents in OOHC – likely impair the development of personal resources and emotion regulation competencies, resulting in more externalising symptoms (Engler et al., 2022). However, since these adolescents are no longer in their original, potentially invalidating environments at the time of assessment, it can also be assumed that the development of resources in OOHC settings is more dynamic, influenced by additional factors such as placement stability, the quality of caregiver relationships and access to supportive interventions (Leathers et al., 2019; Nuñez et al., 2022). The observed mean differences, together with established developmental psychology research, help explain why placement type moderated the effects. Despite this moderation, both groups showed similar patterns – for example, personal resources consistently predicted wellbeing. However, the significant group differences suggest that adolescents in OOHC face more substantial challenges and stressors. This implies that while similar developmental processes may be occurring, they do so under different initial conditions and with differing levels of support (Greeno et al., 2019; Vasileva and Petermann, 2017). As such, the unique circumstances and needs of youth in care should be more thoroughly integrated into intervention designs (Goemans et al., 2015).
Strengths, limitations and future directions
The present study has several strengths, including its focus on adolescents in OOHC, a population group that has received little attention in previous research. Another strength is the longitudinal study design, but to gain a more comprehensive understanding, future research should follow the adolescents over a longer time period, especially during the care leaving phase. It would also be preferable to include a larger sample so that young people in OOHC who grow up in residential groups can also be included. It should also be noted that the study is based on self-reports and therefore involves a certain degree of perception bias, which might have increased associations between our variables. It would therefore be desirable to include proxy reports in addition to self-reports in future studies. In addition, the relatively short and potentially variable time interval between T1 and T2 should be considered a limitation of the study.
Conclusion
The final model supports developmental and resilience theories that conceptualise resources as predisposing protective factors (Masten et al., 2009). Personal resources serve as a preventative factor in relation to externalising symptoms and wellbeing. This implies that interventions aimed at strengthening resources may be more effective in the long term than those focusing solely on symptom reduction (Alvord and Grados, 2005). This is especially relevant given that research on adolescents in foster care often adheres to a deficit-oriented paradigm (Gypen et al., 2017). Similarly, the healthcare system typically emphasises symptom treatment over prevention. Of course, treating symptoms remains important – particularly in light of the high prevalence (and stability) of mental disorders (Engler et al., 2022; Fernandez, 2008; Linderkamp et al., 2009) – but resource-oriented approaches may show additional and sustainable effects, in particular in this vulnerable population (Nuñez et al., 2022). As the results of this study show, such interventions should specifically target the development of personal resources.
To translate these findings into policy and practice, preventative programmes that strengthen resources should be implemented early and integrated into care plans for adolescents in OOHC. Evidence-based measures may include mentoring programmes to provide stable and supportive social relationships, socio-emotional competence training to foster resources, as well as resilience-focused cognitive-behavioural programmes to teach effective coping strategies for stress and adversity. Furthermore, policies should aim to enhance placement stability and the quality of caregiver relationships, as these contextual factors support the development of personal resources. Of particular importance is early support for foster parents, not only when they actively seek help. For example, afternoon programmes could be offered in which children experience opportunities to exercise self-efficacy while foster parents simultaneously receive guidance, exchange and relief. Similarly, school support for adolescents should begin early, with a focus not only on academic achievement, but also on participation, social integration and the development of resources. This could include programmes that actively engage adolescents in extracurricular activities, sport clubs or other school-based and community opportunities, where they can experience self-efficacy, social skills and a sense of belonging. Beyond symptom-focused treatment, such resource-oriented approaches can offer sustainable benefits and help prevent mental health problems in this vulnerable population (Masten and Barnes, 2018; Nuñez et al., 2022).
Footnotes
Ethical considerations and consent to participate
Informed written consent was obtained from all participants included in the study and the study was approved by the local ethics committee (EUB 2019-180).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received funding from the Federal Ministry of Education and Research (BMBF, funding code 01KR1806B).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The authors are willing to share their data and research materials with other researchers. The material will be available upon request.