
Abstract
Tubeless microlaryngoscopy optimises surgical access but typically relies on total intravenous anaesthesia, commonly using propofol and remifentanil infusions. We present a difficult airway case where an unrecognised drug error during programming of an infusion pump resulted in unexpected apnoea. Open airway surgery proceeded with the use of a prophylactic cannula cricothyroidotomy using a Rapid-O2® insufflation device to provide rescue oxygenation. Furthermore, cricothyroid membrane identification failed with digital palpation but was successful with ultrasonography. While the latter is currently not considered the standard of care for preparing for front-of-neck access in a time-critical ‘can’t intubate, can’t oxygenate’ scenario, in our case it proved helpful.
Keywords
Introduction
Tubeless microlaryngoscopy optimises surgical access. Maintenance of oxygenation options includes SponTaneous Respiration using IntraVEnous anaesthesia and Hi-flow nasal oxygen (STRIVE Hi), 1 where anaesthesia is commonly achieved via propofol and remifentanil infusions. We describe a case of an unrecognised drug error leading to unintended apnoea and discuss the subsequent use of front-of-neck access (FONA) ultrasonography and prophylactic cricothyroidotomy. Consent from the patient was obtained to publish this case report and accompanying image.
Case report
A 61-year-old male was scheduled for day case tubeless microlaryngoscopy for biopsy of a vocal fold lesion. His medical history included tonsillar cancer for which he had been treated with chemoradiotherapy the year before.
Airway examination revealed a mouth opening of two fingerbreadths, Mallampati Class 4, thyromental distance of three fingerbreadths, normal neck extension, an indurated submental area secondary to radiotherapy and a palpable cricothyroid membrane. We set up STRIVE Hi for tubeless microlaryngoscopy as follows. 1 Monitoring (oxygen saturation (SpO2), non-invasive blood pressure and electrocardiogram) was established, and an intravenous cannula inserted. Facemask pre-oxygenation with end-tidal carbon dioxide monitoring was commenced, whilst OptiflowTM nasal cannulae (Fisher & Paykel, New Zealand) were placed on the patient’s forehead ready for high-flow nasal per-oxygenation. Intravenous midazolam 1 mg was administered and target controlled infusions of remifentanil (set at effect site concentration (Ce) 2.0 ng/ml) and propofol (Ce 1.5 µg/ml) commenced. The latter was increased to 1.8 µg/ml and, unexpectedly, the patient became apnoeic. The remifentanil infusion was decreased to Ce 1.5 ng/ml and jaw thrust applied, but the patient remained apnoeic. Facemask ventilation was difficult, requiring two hands and an oropharyngeal airway. The OptiflowTM nasal cannulae were lowered into the nostrils and high-flow nasal oxygenation (HFNO) commenced at 70 l/min. Videolaryngoscopy revealed only posterior arytenoids. As the patient remained well oxygenated with apnoeic HFNO, surgery was commenced. A Lindholm laryngoscope was inserted but a poor view was obtained. An anterior commissure laryngoscope was inserted which revealed a swollen epiglottis and supraglottic oedema (changes consistent with radiotherapy). Four percent lignocaine was sprayed onto the supraglottis, which resulted in laryngospasm and desaturation (SpO2 68%). A ‘call for help’ was made and a second senior anaesthetist quickly arrived, by which time the laryngospasm had resolved and the SpO2 had increased to 92%.
Due to the difficult airway (post-radiotherapy airway, indurated submental area, difficult facemask ventilation, difficult videolaryngoscopy and difficult suspension laryngoscopy), a discussion was carried out with the senior otolaryngologist whether to wake up the patient or continue with surgery, as both options had the potential for loss of airway control and hypoxia. We also discussed tracheal intubation via a bougie inserted through the suspension laryngoscope, and kept this only ‘on standby’ as an in situ tracheal tube would impede surgical access.
A decision to proceed with surgery was made and we performed a ‘prophylactic’ cannula cricothyroidotomy ready for oxygen insufflation via a Rapid-O2® device (Meditech Systems Ltd, Dorset, UK) (see Figure 1).2 –5 After digital palpation of the patient’s anterior neck, a cricothyroidotomy with a 14 gauge InsyteTM cannula (Becton Dickinson UK Ltd, Oxford, UK) was attempted as described by Heard. 3 However, correct placement was not obtained as indicated by a ‘negative aspiration’ of air into the saline-filled syringe connected to the needle/cannula unit.3,5 Continued apnoeic HFNO resulted in a SpO2 of 99%. A second cricothyroidotomy attempt also resulted in a negative aspiration. A nearby ultrasound machine was quickly retrieved and was used to easily identify the cricothyroid membrane. Subsequent cannula cricothyroidotomy was successful as indicated by a ‘positive aspiration’; the point of insertion was to the left of the two previous attempts (see Figure 2). Jet oxygenation via the Rapid-O2® was not performed as the patient remained well oxygenated. Equipment for an emergency tracheostomy was also set up.
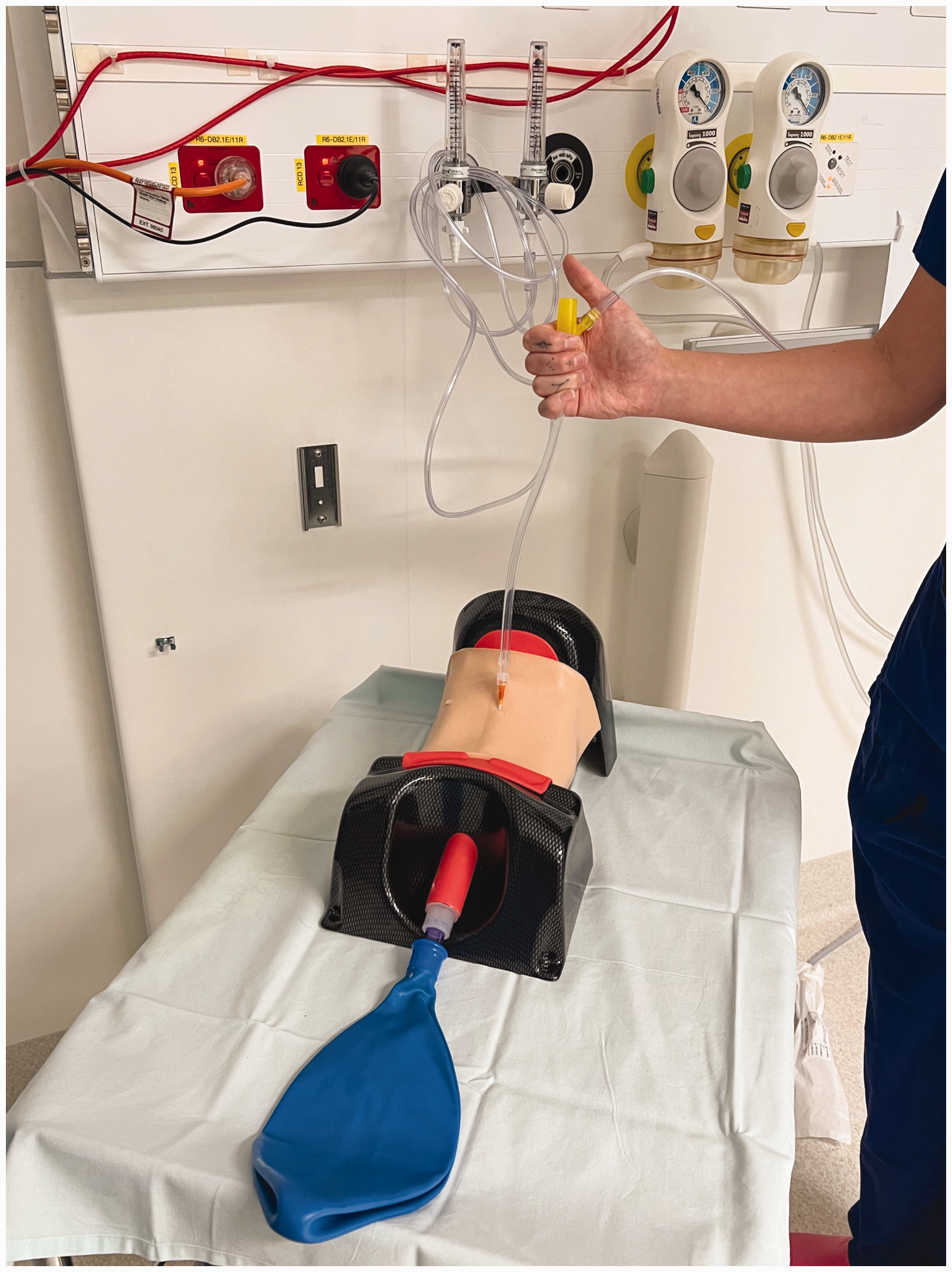
Rapid-O2® oxygen insufflation device connected proximally to oxygen supply (15 l/min) and distally to the cannula cricothyroidotomy in a neck manikin.
Cannula inserted through the cricothyroid membrane.
Surgery resumed, but soon after, despite apnoeic HFNO, the patient became hypoxic (SpO2 88%). A 4-s jet via the Rapid-O2® insufflator, connected to an oxygen supply of 15 l/min, was administered (delivering 1 l of oxygen).3,5 After 20 s, the SpO2 rose to 99%, where it remained throughout the surgery. The latter included microlaryngoscopy and biopsy, and debridement of the vocal fold lesion.
During this time, another senior anaesthetist came in and noticed that the remifentanil infusion pump was incorrectly set up using a propofol target controlled infusion programme. During the prior 15 min, the calculated administered total dose of remifentanil was five times higher than intended (approximately 500 µg instead of 100 µg). 6 The remifentanil infusion was stopped, and spontaneous ventilation returned after approximately 5 min, whereupon the remifentanil infusion was restarted at 3 ml/h. The propofol infusion was up-titrated to a Ce of 4.0 µg/ml to maintain an adequate depth of anaesthesia.
At the end of surgery, the patient was woken up with the cricothyroidotomy cannula in situ. The patient was transferred to the postoperative care unit, where the cannula was removed. After full operative recovery, and with no adverse airway complications noted, the patient was discharged home later that evening.
Discussion
This case represents an unrecognised drug error that led to unintended apnoea, airway collapse and a prophylactic cannula cricothyroidotomy. Despite decreasing the remifentanil infusion, we failed to notice our drug error. Two factors may have contributed to this. First, we made a cognitive error of premature closure 7 by assuming the patient was sensitive to the anaesthetic agents. Second, the ability of HFNO to provide initial effective apnoeic oxygenation may have encouraged our decision to proceed with surgery. Both factors may have prevented us from looking at alternative causes of the unexpected apnoea.
Medication errors are common in anaesthetic practice. In one study, 37% of opioid dose errors involved remifentanil being infused in a wrong concentration or via an incorrectly programmed syringe pump. 8 One contributing factor in our case was the senior anaesthetist being distracted by discussing the case with the junior anaesthetist whilst setting up the infusion pumps. This case emphasises that vigilance is required for all drug administrations, but that particular close attention may be required for patients with a lower margin for error, such as those with a known compromised airway. The episode of laryngospasm may have been prevented had we used apnoeic HFNO (using neuromuscular blocking agents) from the outset. However, in our institution, for open airway surgery we routinely use STRIVE Hi, which is associated with a lower rate of increase in end-tidal carbon dioxide and can be used for longer periods in obese patients. 1
Our airway management may be considered suboptimal as we did not perform FONA ultrasonography pre-emptively in a patient with a difficult airway. Our reliance on digital palpation of the cricothyroid membrane was falsely reassuring. In our case, failure to correctly identify the cricothyroid membrane may have been due to the post-radiotherapy changes of the neck and the time pressure associated with a deteriorating airway.
Pre-emptive (before induction of anaesthesia) ultrasonographic identification of the cricothyroid membrane is recommended, especially in patients with poorly defined neck anatomy. 9 However, ultrasonographic identification of the cricothyroid membrane is not currently recommended during a time-critical ‘can’t intubate, can’t oxygenate’ (CICO) scenario. However, emergency FONA has been performed in non-CICO scenarios when oxygenation can be maintained.10 –12 These were reported in the Fourth National Audit Project (62% of surgical tracheostomies, including several taking over an hour to complete); 10 a Danish Anaesthesia Database study (30% of cases); 11 and in an update from the Airway App (33% of cases). 12 Such cases may allow time for cricothyroid membrane ultrasonography if ultrasound equipment is immediately available and the anaesthetist is trained in performing it.
The advantages and disadvantages of the two main FONA techniques (cannula versus scalpel cricothyroidotomy) have been well described. 13 We would like to add what we consider further advantages of cannula cricothyroidotomy. First, it can be performed in the awake patient as a ‘prophylactic’ technique for subsequent percutaneous oxygenation insufflation (if needed) for difficult airway management. 5 Second, training opportunities for cannula cricothyroidotomy can be obtained by translaryngeal injection for airway topicalisation for awake intubation. 14 In our institution, we teach both FONA techniques as various emergency FONA scenarios may benefit from one technique over the other.
We may be criticised for the number of cannula cricothyroidotomy attempts. However, they were performed by an anaesthetist with considerable experience in awake prophylactic cannula cricothyroidotomy, several emergency FONA cases and routine translaryngeal injection for awake intubation.
The Rapid-O2® device was successfully used for percutaneous oxygenation insufflation after hypoxia developed despite the use of apnoeic HFNO. Its technical and non-technical advantages, and risks, are described elsewhere.4,5
In summary, we present a case where distraction led to an unrecognised drug error. Maintaining a high level of vigilance, especially in patients with a known compromised airway, may help reduce such errors. We recommend that anaesthetists should be trained in both cannula and surgical cricothyroidotomy. This case indicates that cricothyroid membrane identification by digital palpation may be falsely reassuring, so pre-emptive ultrasonographic identification should be considered in cases of difficult or altered neck anatomy. In our case, ultrasonography was also helpful in performing prophylactic cannula cricothyroidotomy, which eventually allowed us to maintain oxygenation using Rapid-O2® oxygen insufflation. We recommend that ultrasound equipment is made readily available for this purpose if required.
Footnotes
Author Contribution(s)
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.