
Abstract
This study aimed to characterise specialist palliative care service involvement within the intensive care unit (ICU) and subsequently in post-ICU hospital wards, and compare current ICU referral practices with those suggested by an internationally utilised ICU palliative care referral tool. This was a retrospective cohort study, carried out at a large university-associated ICU in Melbourne, Australia, and was conducted on adult patients aged at least 18 years admitted to ICU between July 2019 and July 2023. The study included 11,449 ICU admission episodes relating to 10,171 patients. The overall ICU mortality for all patients was 9% in ICU with a further 4.3% post-ICU. Within non-survivors, specialist palliative care involvement was uncommon for patients who died in ICU (78/1035, 7.5%), but substantial (287/488, 59%) for those ICU patients who died on a hospital ward after ICU discharge. Compared with ICU patients who did not have an identified palliative care referral, ICU patients with palliative care input averaged longer ICU stays with shorter hospital stays post-ICU discharge. The referral tool showed low sensitivity (39%) when compared with observed current ICU palliative care referral practice. Clinical staff within the ICU provided the majority of palliative care for ICU patients, with a palliative care consultative service taking a proportionally much greater role in post-ICU hospital wards. The selected criteria appeared inadequate for use as an effective referral tool. Future research may explore the quality of palliative care provided by ICU staff and specialist palliative care staff, and the role of decision support tools, so as to provide optimal care for critically ill patients approaching the end of life.
Introduction
Outcomes of patients admitted to Australasian intensive care units (ICUs) have improved over recent years with a decline in the standardised mortality ratio from 2008 to 2020. 1 There was some reversal in this improvement from 2021, which may be related to the consequences of pandemic-related changes in service delivery. 2 It is recognised that Australasian patients admitted to ICU who survive to discharge have a worse long-term survival than the general population. 3 Furthermore, patients with a life-limiting illness account for almost a quarter of Australasian ICU admissions, require prolonged ICU and hospital care and have high mortality in subsequent years. 4
Whilst the long-term survival is characterised, 3 there are limited descriptions on patients’ mortality in hospital after ICU discharge. In Australasian data, it is recognised that those with life-limiting illnesses have an 11% ICU mortality and 17% hospital mortality. 5 However, the in-hospital mortality rate of the entire population of ICU admissions is not well characterised. There are limited descriptions of the in-hospital trajectory of patients post-ICU discharge in small international studies across different healthcare settings.6 –8
Palliative care is an essential component of comprehensive care for some critically ill patients. 9 Critical care clinicians integrate many aspects of palliative care into their routine practice including, but not limited to, symptom management, communicating prognostication and establishing appropriate treatment limitations. Initiating referral to specialist palliative care services can vary depending on the anticipated illness trajectory. 10 Identifying that a patient is approaching the end-of-life is critical to allow collaborative decision-making in keeping with an individual’s goals and wishes. 11 However, identifying those who are at the end-of-life, and those who may benefit from specialist palliative care input can be challenging. 12 Internationally there is some use of protocolised ICU/palliative care referral tools.13 –15 Furthermore, the use of palliative care triggers (referral tools) in Australia has been advocated for by both state governments 16 and the Australian Commission on Safety and Quality in Health Care 17 as essential elements of safe and high quality end-of-life care. However, the use of formal palliative care referral tools is not considered standard practice in Australasian ICUs.
The aims of this study were threefold. First, to describe the epidemiology of post-ICU mortality in a large Australian tertiary metropolitan hospital over a four-year period. Second, to describe the involvement of specialist palliative care services with patients who have been admitted to ICU, and their outcomes. Third, to conduct a preliminary comparison of an internationally used ICU palliative care referral tool 14 compared with observed ICU practice. Whilst there are a number of proposed ICU-based palliative care referral tools that have been published, we selected the Hua tool. 14 This tool was designed to identify patients with serious illness who have a high risk of dying14,18 and relies on physiological/demographic data rather than incorporating other domains such as frailty/performance state or severe physical/emotional/spiritual symptom control, which were unavailable in our retrospective dataset.12,13,15,19 This trigger tool screens patients based off five variables: post-cardiac arrest, intracerebral haemorrhage (requiring ventilation), stage IV malignancy, multi-organ failure and ICU admission following >10 days of consecutive inpatient hospital stay. 14
Methods
Setting, design and population
This single-centre retrospective cohort study was performed at The Royal Melbourne Hospital ICU (a 42-bed university-affiliated tertiary department). In addition to general and specialist medical and surgical services, it provides a state-wide trauma service, as well as haematology, oncology, bone marrow and renal transplant services. The ICU accepts approximately 3000 adult admissions per year.
All patients admitted to The Royal Melbourne Hospital (RMH) ICU between 5 July 2019 and 5 July 2023 were considered eligible. This time window corresponded with the first four years of use of an electronic medical records system (EPIC, Verona, WI, USA). To simplify the data analysis where multiple ICU admissions occurred during the same hospital admission, only the first is considered. Where patients have been admitted to the ICU numerous times across different episodes of care, each episode is considered a new episode. Small repeat counts of ICU admission will minimise any errors associated with this data simplification.
We excluded patients who were discharged directly from the ICU to hospitals outside The Royal Melbourne Hospital. These patients were excluded because of logistical challenges associated with cross-campus data access.
Data source
As part of The Australian and New Zealand Intensive Care Society Adult Patient Database, 20 the RMH ICU collects demographic and physiological data pertaining to all ICU admissions. The RMH Palliative Care Service has two datasets. One contains information about all patients reviewed by the palliative care department in a consultative capacity. The second dataset contains information regarding all patients who are admitted to RMH Palliative Care and Supportive Care Unit (PCU), a 12-bed specialist unit which provides care for patients requiring symptom management, complex pain management, end-of-life care and community palliative care discharge planning. A patient was considered as referred to specialist palliative services if an EPIC consult was requested during the period of ICU admission or if the patient was discharged directly from ICU to PCU.
Referral tools
The use of formal palliative care referral tools may not be considered standard practice in Australasian healthcare settings. However, delayed identification of dying and late initiation of palliative care may be associated with high use of non-beneficial interventions and investigations in the last 48 h of life. 21 Therefore, there is a movement towards a priori criteria for palliative care consultation. 22
In the absence of locally developed tools, we selected an American referral tool14,15 to apply to this ICU population. This tool was developed based off retrospective analysis of patients to establish systematic screening tools for palliative care consultation in the ICU. This tool has the advantage of being clinically derived (based off ICD-10 codes and admission diagnosis) and objective, so allows for data-driven protocolisation of palliative care consultation in the ICU. The use of electronic medical records (EMR)-embedded palliative care trigger tools has been found to be acceptable and desirable within a multicentre multidisciplinary American ICU context. 23
Statistical analysis
The four-year extracts from the palliative care and ICU databases were received separately in spreadsheet form in Excel 2019, version 16.78 (Microsoft, Redmond, WA, USA). These two datasets were then merged using the Stata, version 18 (College Station, TX, USA) using the rangejoin function according to unique patient identifier, date of birth and hospital admission dates. All subsequent analyses were also performed using Stata.
To assess the integrity of the merge, we manually confirmed the accuracy of dates of admission, occurrence (and dates) of palliative care and death in the clinical notes of 60 patients who died in hospital. These consisted of 30 from those who died in hospital but were not identified on the palliative care databases and 30 from the palliative care database. We also ensured that dates/times of hospital admission, ICU admission, ICU discharge/death and hospital discharge/death occurred in a logical sequential manner on all admissions.
Data on patient characteristics are summarised with descriptive statistics. Continuous data are presented as mean (standard deviation) or median (interquartile range) (IQR), as appropriate. Categorical and count data are summarised as numbers within categories and associated proportions.
To examine the performance of the referral tool compared with clinician-guided referral, sensitivity and specificity analyses were conducted. The Mann–Whitney U test was used in comparisons between non-parametric continuous variables.
Ethical considerations
Ethics approval was granted by the RMH Office for Research & Governance under the low risk/quality assurance pathway (QA2023075). As such, the need for informed consent was waived.
Results
Details of patients, baseline demographics and outcomes
Over the four-year study period, there were 11,449 ICU admissions involving 10,171 individual patients with hospital survival outcomes known for all except 29 episodes. Overall, 11% of admissions were repeat observations of individuals, with very few (0.8%) patients having more than three admissions (Supplemental material). The clinical conditions treated ranged widely across adult medical and surgical specialties. The majority of these included admission episodes (65.8%) were associated with a principal non-operative rather than operative diagnosis.
As expected, patient demographics as well as illness severity and diagnostic groupings varied substantially according to patient hospital survival relative to the cohorts of patients who died either in ICU or in hospital after their ICU admission (Table 1).
Admission characteristics overall and for categories of intensive care unit and hospital survival.
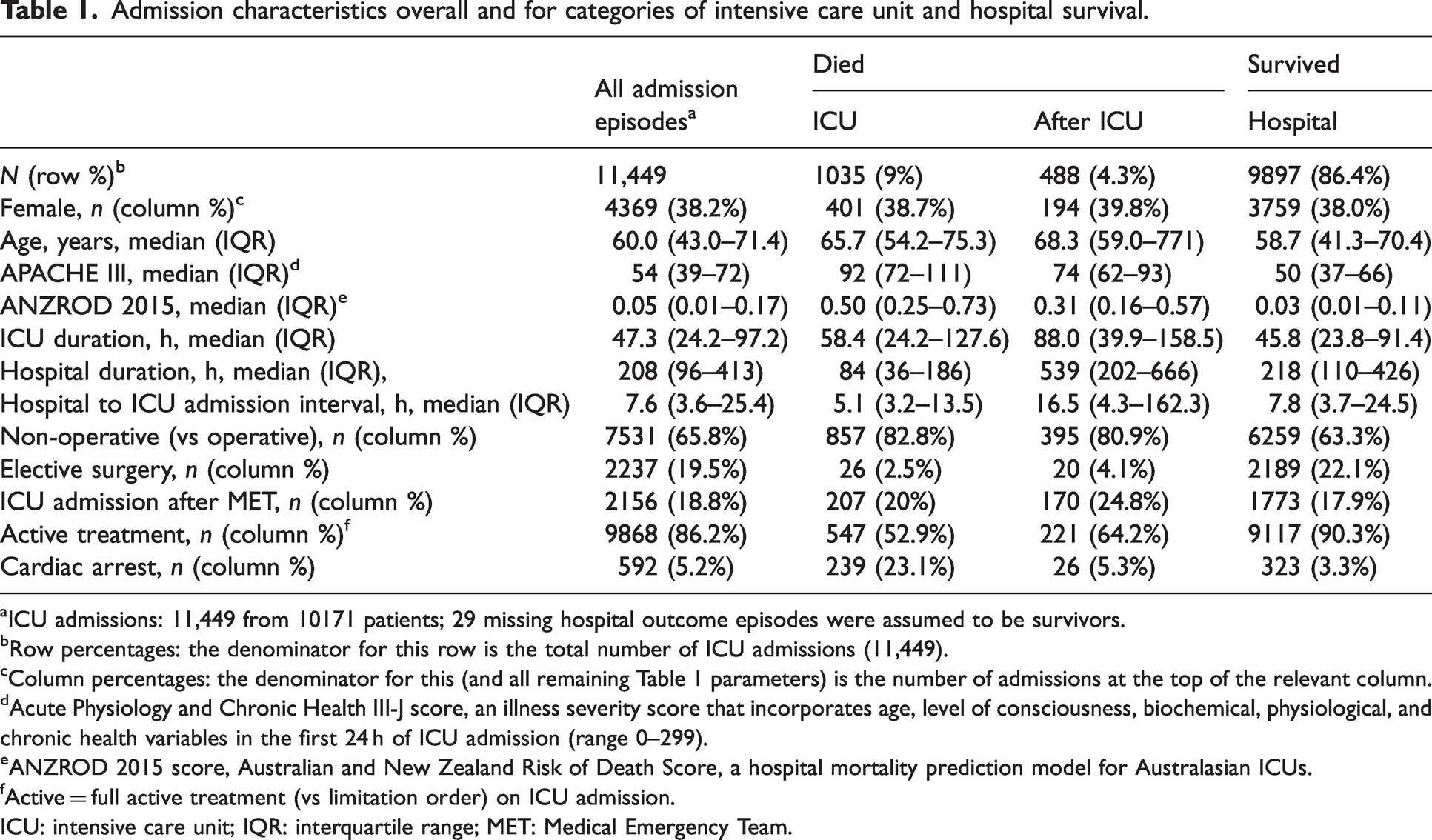
ICU admissions: 11,449 from 10171 patients; 29 missing hospital outcome episodes were assumed to be survivors.
Row percentages: the denominator for this row is the total number of ICU admissions (11,449).
Column percentages: the denominator for this (and all remaining Table 1 parameters) is the number of admissions at the top of the relevant column.
Acute Physiology and Chronic Health III-J score, an illness severity score that incorporates age, level of consciousness, biochemical, physiological, and chronic health variables in the first 24 h of ICU admission (range 0–299).
ANZROD 2015 score, Australian and New Zealand Risk of Death Score, a hospital mortality prediction model for Australasian ICUs.
Active = full active treatment (vs limitation order) on ICU admission.
ICU: intensive care unit; IQR: interquartile range; MET: Medical Emergency Team.
Patients who did not survive their ICU admission episode had on average higher Acute Physiology and Chronic Health Evaluation (APACHE III)/Australian and New Zealand Risk of Death scores. Likewise, ICU survivors who died subsequently on the ward also tended to be older with a greater ICU/hospital length of stay. Non-operative admissions and admissions that followed Medical Emergency Team (MET) responses were associated with higher death rates, both in ICU and subsequently on the ward. Notable diagnostic subgroups included cardiac arrests, which accounted for 23% of ICU deaths (Table 1), in contrast to ICU admission episodes linked to immunosuppressive diseases or their therapy, where these ICU patients more commonly died subsequently on the ward (Supplemental material).
Specialist palliative care involvement
Of the 1035 deaths that occurred in ICU, only a minority (7.5%) had evidence of input from specialist palliative care services (Table 2). ICU non-survivors who received such input tended to be older with longer ICU admission durations. End-of-life ICU admission episodes with palliative care input more commonly followed MET events rather than cardiac arrest events and were more commonly associated with patients receiving non-invasive than invasive ventilation (Supplemental material, Table S3).
Intensive care unit patient characteristics based on location of death and palliative care input.
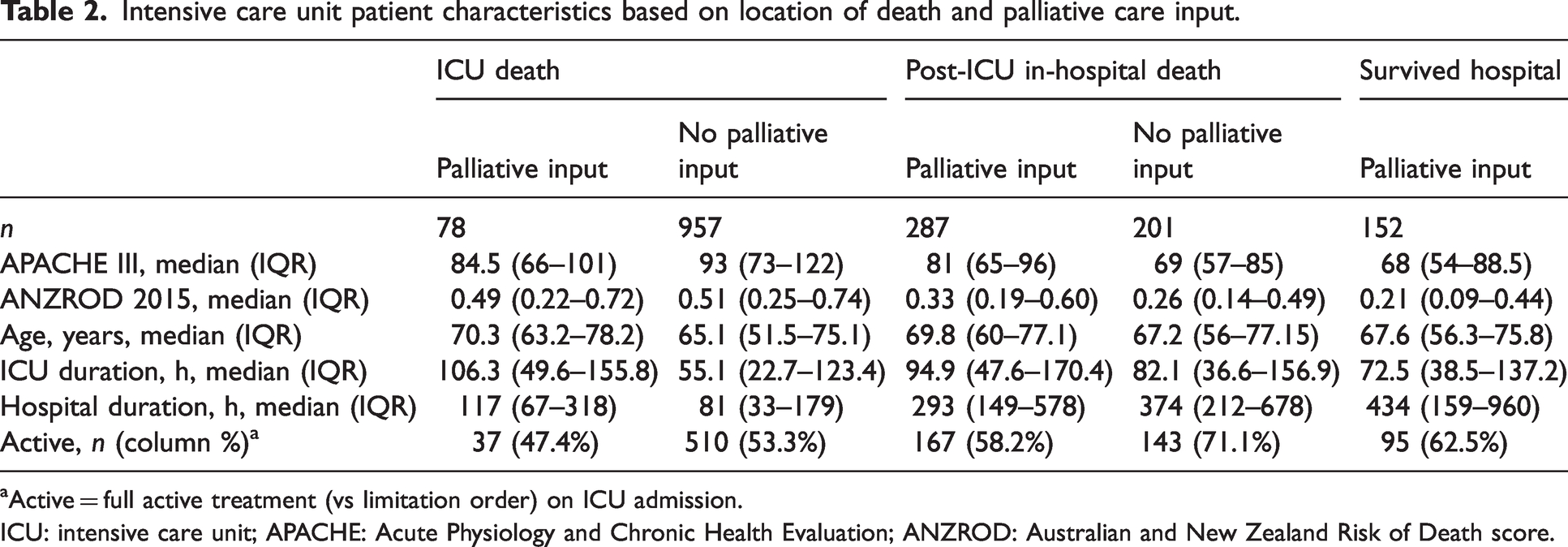
Active = full active treatment (vs limitation order) on ICU admission.
ICU: intensive care unit; APACHE: Acute Physiology and Chronic Health Evaluation; ANZROD: Australian and New Zealand Risk of Death score.
In contrast there was a much higher involvement of specialist palliative care services (59%) in those who died on the ward after being discharged from ICU. Within the overall ward death cohort, those who received specialist palliative care had on average higher severity of illness scores and a reduced hospital length of stay.
Not all patient episodes associated with identified specialist palliative care input were followed by death. While survival to hospital discharge occurred in 29% of cases with palliative care contact (152/517), only 42 such cases were discharged home, with the remainder moving to nursing homes or other health facilities. Across the cohort of patients who had specialist palliative care input, these survivors tended to have a lower illness severity score and yet a prolonged hospital length of stay.
Sensitivity and specificity of palliative referral tools
Using local clinician-guided referral to palliative care as the gold standard, we analysed the Hua referral tool to look at sensitivity, specificity and predictive values. In the absence of a well-validated objective indicator for palliative care referral, day-to-day clinician judgement was chosen as a practical and pragmatic gold standard for comparison of the tool.
Application of the referral tool shows a relatively high specificity (81.9%) for current ICU–specialist palliative care interactions. However, it shows a low sensitivity (39.3%), suggesting that it might miss a number of patients whom clinicians would have referred for specialist palliative input.
Timing of palliative care input
We analysed timing between palliative care referral and death for the 365 admissions (3.2%) that resulted in death with palliative input. Time from ICU admission to palliative care referral had a median of 151.7 (IQR 68.4–301.5) h. This was significantly shorter (P < 0.001) in those who had a treatment limitation order present at the time of admission (median 87.6, IQR 34.4–178.0 h).
The time between palliative care referral and death had a median of 21.3 h (20.1 h in those with a treatment limitation, P = 0.99).
Discussion
Summary of major findings
This is a large retrospective study of 11,449 ICU admissions examining the important but incompletely characterised use of palliative care services. Of these patients, 9% died within the ICU and a further 4% died during the same hospital admission following discharge from ICU.
Those who died on the ward were less unwell based on physiological scores than those who died in ICU. There are noticeable differences in patient characteristics as well, with those who died following cardiac arrest having higher representation in ICU deaths. Those who died in ICU or on the ward had a longer ICU length of stay than those who survived to discharge. Hospital length of stay was shortest for those who died in ICU and longest in those who died in the ward when compared with hospital survivors.
Only 7.5% of those who died in ICU received specialist palliative care input, compared with 58.8% of those who died on the ward. Those who did receive palliative care had a longer ICU length of stay. However, we cannot establish a causal link and this may represent differing clinical characteristics between the two groups. Of those who died on the ward after an ICU admission, individuals who received palliative care had a shorter hospital length of stay than those who did not receive palliative care. Again, we cannot draw strong conclusions but it may be related to the reduced burden of unnecessary interventions seen in other studies.24 –26
There was a relatively short period between referral to palliative care and death, with a median of 21.3 h. This combination of low frequency of palliative care input and short duration of input may represent a delayed recognition of dying/unmet need of palliative expertise.
This study also compared clinical practice in palliative care referral to an internationally used EMR-embedded referral tool. This tool had low sensitivity (39.3%) when compared with clinician-guided referral, suggesting that it does not align well with clinical judgement. This likely reflects the complex multifactorial decision-making process employed in end-of-life care which may be hard to capture from demographic and physiological data.
Comparison with previous studies
The mortality rate is in keeping with other Australasian ICU datasets.2,5 However, substantially fewer patients (7.5%) in this cohort received specialist palliative care compared with the Australian average for all people who died in hospital—63%. 27 Without more granular data it is difficult to ascertain whether this discrepancy represents an unmet palliative care need or indicates confidence and competence in delivering end-of-life care from critical care staff.
There is a paucity of data on the optimal model of delivery and the most appropriate outcome measures for integration of palliative care into ICU populations, with insufficient published data to examine how palliative care utilisation varies across local and international ICUs. Almost all available studies are from North America with differing interventions and variable (seldom overlapping) outcome measures, which limits their generalisability . 28
Study limitations
This is a single-centre retrospective study with the limitations inherent to this design. The nature of the data does not explain the care provided to these patients: excellent ‘non-specialist’ palliative care may be provided, but we cannot assess this. Symptom severity data would also enable us to assess other referral tools. 29 The rollout of EPIC may have been associated with inaccurate data collection: there were some months with no recorded palliative care consultations. Whilst we manually checked a large number of patient episodes and found the data consistent, we cannot rule out some inaccuracy in data collection. Finally, palliative care encompasses complex symptom and psychosocial care for those with life-limiting illnesses. There may be many who did not die but still could benefit from palliative care supports such as outpatient/community palliative care input: particularly survivors with chronic illnesses, long-term palliative needs, or psychosocial burden. These patients may not be well identified by a mortality-based tool which utilises demographic/physiological data such as the one used in this study.
Another potential limitation of this study is that we used admission episodes rather than individual patients. We elected to use patient episodes rather than individual patients as, in our experience, ICU palliative care decisions are based more on the acute clinical situation rather than an individual’s ‘unchanging’ characteristics over time (although these will overlap).
Finally, the pandemic period creates potential for confounders. The impact on Australia’s health system was less severe than comparable countries 30 and critical care systems in Melbourne were not overwhelmed. 31 Furthermore, our data do not show changing specialist palliative care involvement across fluctuations of COVID-19 presentations (Supplemental material).
Implications for clinicians and policy makers
A large percentage of end-of-life care in this cohort rests with ICU staff. As such, we need to be confident in the ability of ICU clinicians to identify and address those with palliative care needs.32 –35 Alongside this we need to clarify the optimal structure for specialist palliative care involvement in ICU, which may include symptom management (particularly in more intricate/persistent issues), continuity of care post-ICU or psychosocial/spiritual support for patients (and families) as well as support for ICU clinicians. 36
Areas for future research
Further studies may involve examining what interventions/therapy are provided as part of end-of-life care, symptom severity scores for those who die in ICU or a prospective trial of specialist palliative care involvement based on physical, emotional or spiritual symptoms rather than physiological/demographic scores. Without more granular analysis of patient admissions, we cannot assess the quality of care provided or identify factors that ICU clinicians use to involve palliative care. Palliative care interventions have been shown to improve quality of life, manage symptoms and reduce healthcare costs in hospitalised patients.37,38 It would be useful to examine whether some of these findings can be replicated in the ICU context, but to do this we need a more complete understanding of the nature of end-of-life care provided in Australasian ICUs.
Conclusions
This retrospective cohort study offers a comprehensive analysis of end-of-life care and palliative care integration within a large ICU population over a four-year period. The study observed that 9% of patients died in the ICU, while an additional 4.3% died in hospital post-ICU discharge. Only a small fraction (7.5%) of those who died in ICU received specialist palliative care input, in stark contrast to the higher involvement (59%) for those who died on the ward post-ICU discharge.
The study assessed the Hua palliative care referral tool on this dataset, finding it to have low sensitivity (39.3%) and inadequate performance for use as referral criteria.
Future research may focus on more granular data about how end-of-life care is provided within the ICU and how these care needs are addressed for different patient populations.
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X251334659 - Supplemental material for A four-year retrospective study of palliative care involvement with Australian intensive care patients
Supplemental material, sj-pdf-1-aic-10.1177_0310057X251334659 for A four-year retrospective study of palliative care involvement with Australian intensive care patients by Mark P Collins, Patrick Steele, Lewis Hackenberger, Christopher MacIsaac and Jeffrey Presneill in Anaesthesia and Intensive Care
Footnotes
Author Contribution(s)
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.