
Abstract

We write in follow-up to our recently published article ‘Evaluation of opioid prescribing for surgical patients discharged from three metropolitan hospitals between 2012 and 2020’ 1 (the original study), in which we described a gradual reduction in opioid initiation and supplied quantities at surgical discharge. Since publication, we have updated our analysis using data from 2024 to compare against our previously published 2012–2020 data, aiming to assess whether trends in opioid prescribing had been sustained. Intermediate years (2021–2023) were not included, as the intent was to examine longer-term change rather than conduct a year-by-year analysis. This updated evaluation is timely given the release of the Australian Commission on Safety and Quality in Health Care’s Opioid Analgesic Stewardship Clinical Care Standard, 2 increasing attention to persistent opioid use following hospitalisation, 3 and recent evidence showing substantial variability in opioid prescribing practices across Australian hospitals.4,5 Here, we present the new 2024 data and reflect on how opioid stewardship efforts may be influencing current practice.
The original study reviewed 117,989 surgical patient encounters from three metropolitan public hospitals within the same health network between 2012 and 2020, averaging 13,109 patient encounters per year. In 2024, this number was 15,260. The study identified a downward trend in opioid use at discharge, from 79% of patients in 2012 to 68% in 2020. 1 This decline has continued, with only 58% of patients discharged on opioids in 2024. Similarly, the use of modified-release opioids, which peaked at 20.6% in 2017, declined to 5.4% in 2020 and dropped further to 3.3% in 2024. These trends reflect broader national efforts to reduce unnecessary opioid exposure following surgery, as supported by Australian guidance advocating for judicious, short-duration opioid prescribing post-discharge. 2
We have also revisited the original oral morphine equivalent daily dose (OME or OMEDD) analysis using statistical process control (SPC) techniques. Commonly applied in quality improvement, SPC techniques offer valuable insights when examining observational data over time, and specifically the identification of special cause variation. Unlike random variation, which is inherent to most systems, special cause variation describes variation that is unexpected based on historical data and is likely the result of fundamental changes in the underlying system. This updated analysis demonstrates that the reduction in OME identified in our original study, from an average of 130.7 mg in 2012 to 66.8 mg in 2020, was sustained through to December 2024, with an average of 65.3 mg in 2024 (Figure 1). Furthermore, the presence of special cause variation immediately prior to the introduction of voluntary real-time prescription monitoring, rather than afterwards, supports our speculation that the statistically significant reduction in OME observed in the original study may have been driven by other factors, such as anticipation or increased awareness of the upcoming change.
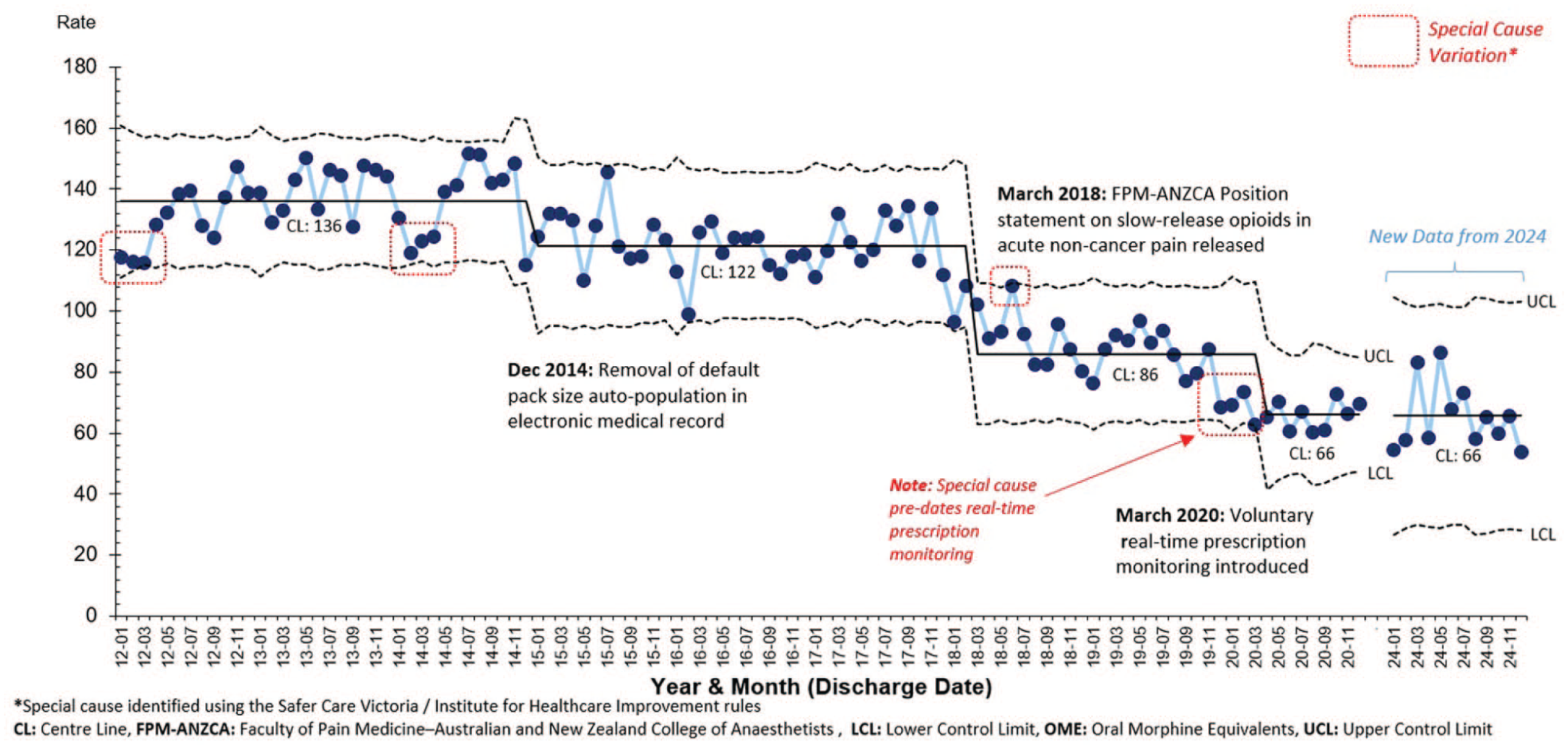
Monthly opioid prescribing rate on discharge: surgical patients (OME per patient encounter, U′ chart) N = 132,197.
This sustained reduction in OME is particularly notable given several intervening factors between the original study period and the updated data that might have been expected to increase OME. One such factor is the shift away from modified-release opioids, which has likely resulted in greater prescribing of short-acting opioids. In addition, there has been an increased use of higher OME opioids such as tapentadol (rising from 9.5% in 2020 to 13% in 2024) and buprenorphine (from 0% to 2%). Conversely, prescribing of lower OME opioids has declined, including tramadol (from 4.5% to 2.3%) and codeine (from 3.4% to 2.5%). Oxycodone remains the most commonly prescribed opioid, accounting for 77% of opioid discharges in 2020 and 78% in 2024. The growing preference for tapentadol and buprenorphine may reflect attempts to balance analgesic efficacy with perceived safety, although the evidence base for long-term superiority remains limited. 6
The original paper also examined oxycodone prescribing patterns, particularly the effect of removing the default pack size of 20 tablets from electronic systems. This change was associated with a reduction in the proportion of patients receiving a full box from 79% to 32%, and this has dropped further to 11.7% in 2024. This aligns in part with the Australian Commission on Safety and Quality in Health Care’s ‘Opioid analgesic stewardship in acute pain clinical care standard’, which recommends tailoring discharge quantities to the patient’s analgesic needs over the 24 hours prior to discharge. 2 However, in 2024, 58% of patients were prescribed exactly 10 tablets—equivalent to half a standard box. This pattern suggests that, although the prescribing software no longer auto-populates a quantity, prescribers may be relying on self-imposed defaults. While this behaviour has contributed to reduced overall prescribing and represents a positive step in addressing oversupply, it may not reflect a truly individualised approach. These findings highlight the enduring influence of prescribing habits and underscore the need for ongoing education and targeted system-level interventions.
These updated findings demonstrate that progress in opioid stewardship at surgical discharge has largely been sustained at the hospital network, with continued reductions in opioid initiation, modified-release formulations, and default pack prescribing. However, the observed increase in average discharge OME and signs of new default prescribing behaviours suggest that further improvements are possible. Ongoing efforts should focus on embedding truly patient-centred prescribing practices, supported by education, clinical decision support, and audit-feedback mechanisms. Future research should examine the relationship between prescribing patterns and patient-reported outcomes, including pain control and opioid-related harms, to ensure stewardship initiatives continue to align with safe and effective care.
Footnotes
Author contributions
Declaration of conflicting interests
The authors have no conflicts of interest to declare.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.