
Abstract

Keywords
Surgical antibiotic prophylaxis is the leading reason for antimicrobial use in Australian hospitals, 1 with cefazolin the most recommended. The national guideline, Therapeutic Guidelines: Antibiotic, identifies cefazolin as the first-line prophylactic agent for the majority of procedures. 2 Reflecting its dominance, cefazolin accounted for 75.9% of all operating theatre antibiotic usage in 2021. 3
Recent research has focussed on inappropriate prescribing of antibiotics, particularly concerning the timing of initial administration and total duration of the antibiotic course. 3 There is, however, scant research on the observation of actual push administration practices in operating theatres. Specifically, the time to inject cefazolin completely in awake or consciously sedated patients has received minimal attention. While the product information recommends injection over 3–5 minutes, 4 the rationale for this timeframe is not specified. Furthermore, adherence to this guideline remains unknown, especially during anaesthesia induction when multiple priorities compete for attention.
The length of time to inject cefazolin is clinically important. Administering it rapidly pre-incision may lead to adverse reactions such as pain, nausea or vomiting. 4 However, the exact incidence of these reactions and their relationship to the speed of cefazolin injection is unknown. 5 Administering it too slowly, whether intentionally or unintentionally, may risk incomplete dosing at incision time, potentially resulting in suboptimal plasma and tissue concentrations.
We conducted a preliminary direct observational study of the length of cefazolin injection time in operating theatres across two hospitals. Our primary aim was to quantify the total administration time and assess adherence to the manufacturer’s recommendations. A secondary aim was to record any adverse reactions.
South Eastern Sydney Local Health District Ethics Office determined this study did not pose significant ethical risks and that a formal ethics review was unnecessary.
This study took place in the operating theatres of two Sydney metropolitan hospitals: Prince of Wales Hospital (POW), a 450-bed tertiary hospital, and Sydney Hospital and Sydney Eye Hospital (SSEH) a quaternary referral hospital for hand and ophthalmic surgery. To minimise alterations to usual practice, only limited disclosure was provided; staff were informed of an antibiotic audit but not of its focus.
Inclusion criteria were patients undergoing surgery awake or under conscious sedation who received intravenous cefazolin as the sole antibiotic. Exclusion criteria were those who did not receive cefazolin or were administered additional antibiotics.
A convenience sample of 60 patients was observed over the 5 months to September 2024. Cases selected to be observed were based on the availability of four observers (one specialist, two fellows and one registrar). One observer was assigned to each case. At POW, operations from all specialities were observed except for cardiothoracic surgery. At SSEH, only hand surgery was observed, as intravenous cefazolin was rarely used in ophthalmic operations.
Observers recorded the start and end times of cefazolin injection and any associated adverse reactions. We assessed the patient as experiencing pain if they either reported pain spontaneously without questioning or exhibited behavioural signs such as facial grimacing or arm withdrawal. Basic demographics (age, sex), surgery type, and sedation medications were also noted. Data analysis was performed using Microsoft Excel (Microsoft, Redmond, WA) using simple descriptive statistics.
We observed a total of 60 cases: 21 at POW and 39 at SSEH (Table 1 and Figure 1). The median injection time overall was 81 (interquartile range (IQR) 56 to 120) seconds. The shortest injection took 15 seconds and the longest 672 seconds. The median was 74 (IQR 37 to 84) seconds at POW and 90 (IQR 59 to 120) seconds at SSEH.
Time to inject cefazolin preoperatively by hospital.
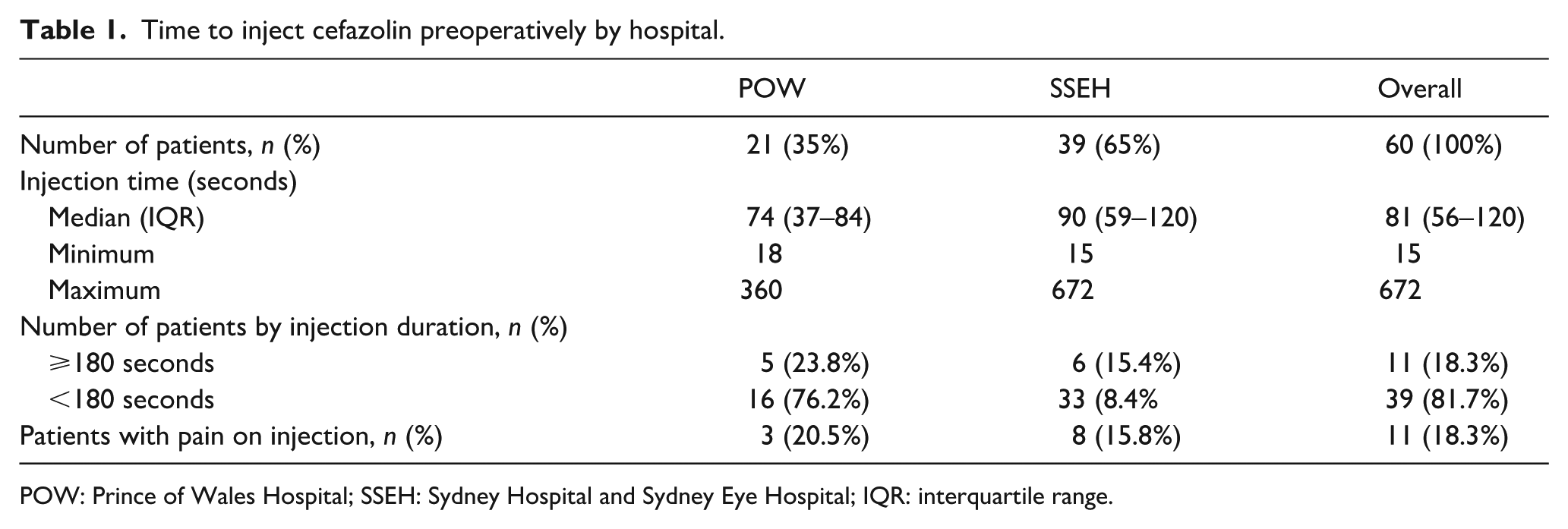
POW: Prince of Wales Hospital; SSEH: Sydney Hospital and Sydney Eye Hospital; IQR: interquartile range.
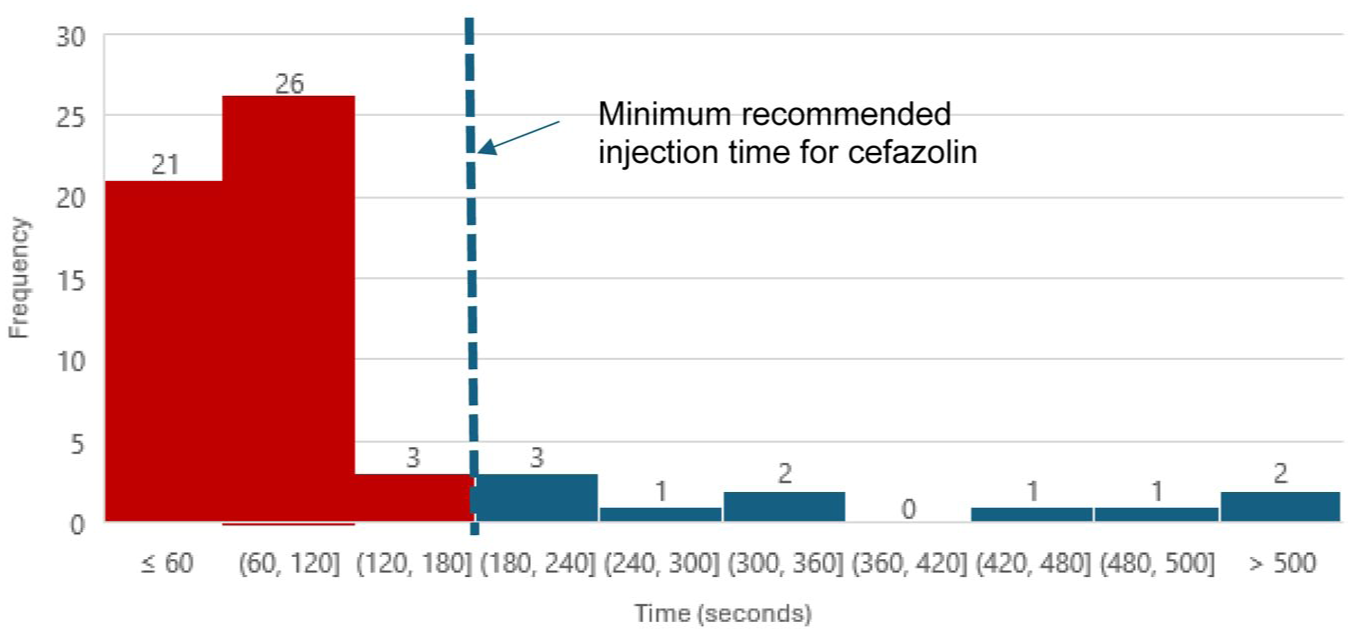
Time to inject cefazolin (seconds) preoperatively by frequency.
Adherence to the manufacturer’s recommended injection time of at least 180 seconds was observed in 18.3% of cases (11 patients). Non-adherence was noted in 81.7% of cases (39 patients), with 76.2% at POW and 84.6% at SSEH.
The only adverse reaction was pain at the injection site, seen in 18.3% of patients (11 patients). The incidence was similar across the two hospitals, occurring in 20.5% of patients at POW and 15.8% at SSEH.
The Therapeutic Guidelines: Antibiotic 2 recommend that cefazolin be administered within 60 minutes prior to surgical incision, and re-dosed every 4 hours intraoperatively. Manufacturers recommend direct injection over 3–5 minutes after dilution with at least 10 ml of a compatible fluid, 4 or as intermittent or continuous injections.
In practice, however, we observed that cefazolin was frequently given at rates much faster than the manufacturer’s guidelines. While patients under general anaesthesia may not experience side effects associated with a rapid intravenous push, the same cannot be said about conscious patients. Pain, nausea, and vomiting are important patient-centric events that can meaningfully impact the patient experience. 6 It is not known whether rapid administration increases the likelihood of these side effects, although anecdotal evidence suggests it may.
From an adverse reaction standpoint, nearly 20% of all patients experienced pain during injection. Notably, all cases of pain occurred when injections were completed in less than 180 seconds, while no pain was observed in patients whose injection took longer than 180 seconds. However, due to the small sample size, it is not possible to draw conclusions regarding this association. No other side effects such as nausea, vomiting or phlebitis were observed. Although pain on injection may be regarded as a ‘minor’ side effect, it is an important patient-centred outcome.
There are several limitations to this study. First, limited disclosure was provided to clinicians, which may have modified their usual practices. Although the antibiotic study was known, details about its focus were not disclosed. Audits are common in these two hospitals, but typically focusing on type and duration, rather than the injection itself. Given the low adherence to the recommended administration rate despite clinicians being aware of the study, real-world adherence may be even lower. Second, the studied group consisted of only 60 patients, limiting the generalisability of the findings. Third, case selection was opportunistic due to the varied availability of observers, possibly introducing bias.
In conclusion, we found low adherence with the recommended cefazolin injection rate across both hospitals along with a notable incidence of pain during injection. Future larger-scale studies could offer greater insight into adherence with the recommended rate of cefazolin push in awake or consciously sedated patients. Additionally, the relationship between the time to complete injection and the incidence of pain at injection site could be further explored.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.