
Abstract
Propofol-based total intravenous anaesthesia (TIVA) is being increasingly used for maintenance of general anaesthesia due to benefits over volatile anaesthetic-based anaesthesia. An ongoing concern with the use of TIVA is the increased incidence of unintended awareness. The bispectral index (BIS) monitor has been proven to reduce the risk of awareness in relaxant general anaesthesia; however, it does not directly measure or ensure adequate anaesthesia delivery. Volatile anaesthetic delivery is confirmed by end-tidal gas monitoring; however, there is no comparable monitoring in TIVA. Recent research has thus focused on the development of technologies supporting the real-time monitoring of propofol levels, which could allow TIVA to operate with the same direct feedback that end-tidal monitoring provides for the volatile anaesthetics. It would not replace pharmacodynamic effect monitoring such as BIS, as inter-patient variability in anaesthesia doses required for an adequate depth of anaesthesia remains. It could, however, complement it, allowing TIVA to operate with the same level of real-time monitoring, and overall risk of awareness, as volatiles. There are currently no technologies for this in use in the clinical setting. This review provides an overview of the various propofol measuring technologies that have been or are being developed, as well as some of the key ongoing attempts at applying these technologies in clinical settings. We discuss challenges that have impeded the implementation of promising innovations, and outline future directions for making real-time propofol monitoring a clinical reality.
Introduction
Propofol, a potent intravenous anaesthetic, is widely used for the induction of anaesthesia. Additionally, propofol-based total intravenous anaesthesia (TIVA) is seeing increasing use in the maintenance of general anaesthesia. This is largely driven by the smooth, clear-headed recovery that propofol produces, the drug’s antiemetic properties, and its ability to preserve cerebral autoregulation,1–4 among other benefits including reduced postoperative pain, 5 and additional proposed benefits such as reduced postoperative delirium in older patients and improved survival in cancer patients.5–10 An ongoing concern with the use of TIVA is the increased incidence of unintended awareness. The 5th National Audit Project (NAP5) on accidental awareness during general anaesthesia in the United Kingdom found that TIVA in any method of administration was over-represented in cases of awareness; TIVA with neuromuscular blockade conferring an almost four-fold risk. 11 Awareness is still a very rare event during any general anaesthetic, 11 but the increased relative risk with TIVA has stimulated the search for better monitoring alternatives that could diminish this risk.
A key advancement in anaesthetic depth monitoring, the bispectral index (BIS), has been shown to reduce the risk of awareness in high-risk cases under relaxant general anaesthesia. 12 The BIS measures the depth of anaesthesia, a surrogate for drug effect, providing anaesthetists with a simple numerical guide to aid in appropriate doses of anaesthesia. 12 It should be noted, however, that BIS does not directly measure or ensure adequate anaesthetic delivery. Volatile anaesthetic delivery is confirmed by end-tidal gas monitoring, ensuring the patient is receiving the desired anaesthetic dose. In contrast, while using TIVA, there is no comparable method for direct confirmation of propofol delivery.
The potential failure to identify unintentional cessation of propofol delivery remains a key risk factor for awareness during TIVA, particularly when using neuromuscular blockade. There remains the potential for cannula failure, with lack of visualisation or access to cannulae during certain surgeries prohibiting direct visualisation and identification of failed drug delivery. Target-controlled infusion (TCI) malfunction is also a critical and under-recognised contributor to TIVA delivery failure. 13 Complexities create numerous potential error pathways, including the choice between multiple pharmacokinetic models, the choice between plasma and effect-site targeting, searching in drug libraries, and patient factor inputs. 13 Line management also adds an element of complexity including the potential for occlusions, disconnections and wrong-line routing. 13 While mitigating practices exist such as standardised programming and human factor strategies, including pre-induction TCI checklists, the ability to monitor drug concentrations in real time would be more directly effective in detecting delivery failure. An additional consideration is that TCI pumps are based on population data, and do not account for inter-individual differences or physiological intra-individual dynamics. 14 This type of monitoring device would not replace pharmacodynamic effect monitoring such as BIS, as inter-patient variability in anaesthesia doses required for an adequate depth of anaesthesia remains. It could, however, complement it, allowing TIVA to operate with the same level of monitoring as inhalational anaesthesia.
Recent research effort has focused on the development of technologies supporting real-time plasma propofol concentration monitoring. This review provides an overview of some of the key investigational propofol-measuring technologies, as well as some of the key ongoing attempts at applying these technologies to the clinical setting. There are currently no technologies in use in the clinical setting. We discuss the technologies, mechanisms and challenges that have impeded the implementation of promising innovations, and outline future directions for making real-time propofol monitoring a clinical reality.
An ideal propofol monitoring device
To be of benefit in the administration of TIVA, a propofol monitoring device would need to provide anaesthetists with pharmacokinetic feedback similar to the accurate, real-time data that end-tidal gas monitoring provides for volatile anaesthetics. Such a technology should be able to detect rapidly when there are inadequate propofol levels due to either insufficient dosing or the failure of propofol delivery. This would allow anaesthetists to titrate infusion rates to the desired concentration, or act quickly to reinstate adequate propofol delivery, thereby diminishing awareness risk. A device would, of course, also need to be able to be easily and practically incorporated into existing anaesthetic practice and equipment.
We therefore propose the following key factors that would be required of a clinically acceptable propofol monitoring device:
Rapid and continuous data provided
High sensitivity and specificity for propofol
Small in size, point of care and automated measurement
Validated in humans.
Materials and methods
We conducted a literature search using Medline (Ovid), Web of Science, and Google Scholar for English language articles between 2005 and 2025 on propofol monitoring technologies. Search terms included combinations of propofol, monitoring, biosensor, TIVA, real-time, continuous, analyser and awareness. We identified relevant publications including bench research studies, device validation trials, review articles, and pertinent conference proceedings or industry reports. Additional information on commercial devices and company histories was gathered from regulatory filings and press releases.
Technologies under investigation
Chromatography
The current gold standard for quantifying propofol is high-performance liquid chromatography (HPLC) analysis of blood. 15 As this requires sample collection, laborious sample preparation, and slow, cumbersome, bench-top analysis, its turnaround times are in the order of tens of minutes to hours, 15 rendering it unable to provide real-time information. Likewise, gas or liquid chromatography combined with mass spectrometry (GC-MS or LC-MS) offers sensitive propofol detection for research and forensic purposes,16–18 but these instruments are expensive, not point of care and too slow to return clinically actionable information. 15 Thus, while these laboratory-based assays are useful for pharmacokinetic studies and forensics, they fall far short of meeting the needs of anaesthetists for immediate feedback in the operating theatre. 15
Mass spectrometry
An alternative approach to HPLC has been to leverage modern mass spectrometry (MS) in a more portable fashion.15,19 One novel strategy, employing ‘paper spray ionisation’, has achieved near real-time propofol measurement. 19 In this, a tiny, 10 µl sample of whole blood taken at the bedside is mixed with an internal standard and a solvent on a paper substrate. 19 A high voltage applied to the paper creates a spray of charged droplets, which are fed into a mass spectrometer. The authors showed that a single analysis could be completed in about 2 minutes. 19 In their paper, they tested the method on three surgical patients, with intermittent, 10 µl blood samples being drawn and analysed throughout the propofol infusions. 19 The resulting measurements achieved were reportedly successful in measuring the propofol concentrations in these patients, with this proof-of-concept strategy showing the theoretical feasibility of ‘continuous’ monitoring by rapid serial sampling and analysis. 19 The limitation, of course, is the need for a mass spectrometer at the bedside. While smaller spectrometers are under development, they are far from being commonplace in operating theatres, and the requirement to collect a sample, mix and then insert it into a device makes the likelihood of automation with this strategy low. Nonetheless, this study could serve as a reference method to validate other sensors.
Colorimetric assays
The Gibbs reaction, in which 2,6-dichloroquinone-4-chlorimide reacts with phenolic compounds to produce a coloured product, provides a ready, optical means of measuring propofol.20–22 A difficulty in employing this reaction in real-time propofol monitoring, however, is that the chemical reaction must constitute part of a multi-step assay. To circumvent this difficulty, Hong et al. created a microfluidic chip supporting the rapid, autonomous measurement of plasma propofol. 21 To do so, the chip system performed sampling, mixing, and detection on a small disposable cartridge, potentially enabling integration into a bedside monitor. 21 The microfluidic chip incorporated propofol sensors and photodetectors to measure propofol optically, reporting results within 60 seconds. However, the device failed when challenged with whole blood due to the strong optical absorption of this sample matrix. 21
The most prominent attempt at a commercial propofol monitor, the Pelorus series developed by Sphere Medical (Cambridge, UK), also utilised the Gibbs reaction as part of an automated assay. 22 The two models, Pelorus 1000 and its successor Pelorus 1500, both received Conformité Européenne (CE) marking between 2010 and 2012 as in vitro diagnostic devices, and were described as the world’s first commercially available devices for propofol concentration monitoring in blood.23,24 Validation studies demonstrated their accuracy both in vitro and even in animal models, with the quantification range spanning clinically relevant plasma propofol concentrations. 22 Despite these promising results, however, the Pelorus never achieved widespread clinical adoption. We suspect the issue was due to the fact that the device requires intermittent sampling and has a time lag of 5 minutes, which limit its clinical benefit.
Electrochemical approaches
Electrochemical sensing, which generates an electrical signal in response to the presence of a target molecule, has been intensively studied for propofol monitoring for several reasons: it can be fast, sensitive, continuous, and devices can be very small.15,25 Propofol, being a phenolic compound, is electroactive: it can be oxidised at certain electrode surfaces, yielding a measurable current proportional to concentration. 25 However, a well-documented challenge has hindered direct electrochemical propofol sensors: electrode fouling. 25 When propofol is oxidised electrochemically, it forms reactive by-products that polymerise into an insulating film on the electrode surface. 25 Within minutes, this by-product passivates the electrode, causing the sensor to lose sensitivity. 25 Various techniques have been trialled to circumvent this issue, including utilising membranes to coat electrodes, as well as cyclic electrode cleaning to strip the fouling layer. None of these approaches, however, have yet led to real world sensor examples.26,27 Despite this, several techniques to avoid electrode fouling seem to show promise. One approach is to utilise enzymes to oxidise propofol, avoiding direct oxidisation at the electrode surface thereby preventing film deposition. 28 The sensor responds to changes in propofol concentrations within one minute and has good sensitivity and specificity for propofol. 28 While only tested in vitro, this represents a potentially useful technique that could be used for continuous real-time monitoring; the challenge being to integrate such a biosensor with human blood or plasma and demonstrate stability of the enzymatic component in vivo. 28
Hong et al., 21 who developed the above microfluidic chip, utilised electrochemical propofol sensors to develop their chip further. The on-chip biosensors were based on the conduction of molecularly imprinted polymers that employ label-free electrical detection techniques. 29 The proposed disposable microfluidic biochip showed good selectivity for propofol over structurally similar compounds in spiked human plasma samples, producing a measurement in just 25 seconds. 29 Despite these promising results, after 2016 there have been no further publications from this team on a commercial product, and the device has not, to our knowledge, undergone clinical trials. A hypothesis on why this technique has not advanced to a prototype device could be related to transitioning from controlled laboratory tests to real world use in human blood, with the potential for cells and proteins in whole blood to cause fouling of microchannels or sensors.
A more recent approach to compensate for electrode fouling has been the use of machine learning. 30 In 2021 the École Polytechnique Fédérale de Lausanne (EPFL), a Swiss federal research institute, together with the Swiss Lausanne University Hospital and the Polytechnic University of Turin unveiled a syringe-shaped, electrochemical ‘smart portable pen’ device supporting continuous propofol measurements. 30 The device’s needle contains tiny electrodes that sample blood (either through an arterial line or periodically from a vein) and transmit data to a central unit in the syringe body. 30 Rather than physically cleaning the electrodes, the team applied machine learning algorithms to model and correct the drift caused by fouling. 30 By training the system on how the propofol signal decays over time, they could computationally adjust the readings to reflect true concentrations. 30 The device displays propofol concentrations every 30 seconds, but has only been reported to monitor continuously for a maximum of 10 minutes, which would need to increase substantially to be clinically useful. 30 The smart sensor syringe has been validated in human serum samples, however, with the next steps planned for in vivo trials in surgical patients. 30 It remains to be seen whether the machine learning compensation is robust across different patients and clinical conditions (where fouling dynamics might differ), but this strategy to mitigate fouling without manual intervention is promising.
Finally, in yet another approach researchers are exploring advanced nanomaterials to improve electrochemical propofol sensors. A microcatheter developed by Kafley et al. 31 utilises nanomaterials to provide continuous propofol monitoring with a high sensitivity and stability. The microcatheter format is intended to sample directly from an artery or vein for real-time monitoring. 31 While still in an early stage, such developments indicate that the field is actively progressing toward practical continuous sensors.
Each iteration—from membrane coatings to periodic cleaning, enzyme catalysis, machine learning correction, and nanomaterials—addresses a piece of the puzzle in achieving a reliable, continuous propofol sensor. None of these electrochemical systems have yet been tested in a clinical trial on humans, but they form the technical foundation for future devices.
Photoacoustic detection in breath
Early studies into correlating exhaled propofol concentrations to plasma propofol levels utilising mass spectrometry were found to be too weak to be of clinically useful predictive value.32,33 However, there are studies that show that propofol concentrations in breath could correlate with brain concentrations.34,35 Mass spectrometry is unsuitable for point-of-care measurement, but recently a novel photoacoustic detector to monitor propofol in exhaled breath has been studied. 36 A photoacoustic sensor quantifies exhaled propofol via sound waves emitted by propofol when molecules are excited by the light of a specific wavelength and frequency. This sensor accurately measured propofol exhalate from 10 healthy anaesthetised patients. They also found that there was an alignment between changes in propofol breath gas and changes in the processed electroencephalogram (EEG). 36 However, there are still significant challenges to overcome with this method before it could be of clinically useful value. Other components of exhaled breath such as varying fractions of oxygen, acetone, water and volatile anaesthetics, can influence acoustic detection. For example, the sensor is unable to measure propofol concentrations in the presence of sevoflurane, which would be a major limitation of any photoacoustic sensor. A lack of specific breath reference values for adequate anaesthesia also remains a current open research question. Additionally, the influence of cardiovascular and respiratory disease on propofol in breath gas is unknown. Another issue raised with the technology is the potential for propofol to stick to plastic surfaces such as the inside of endotracheal tubes, as well as leak out through insufficiently tight connections, causing issues with detection. The technology, although potentially promising, remains a long way from being incorporated usefully into clinical practice, with questions remaining on the achievability of measuring propofol in breath under clinical conditions.
Summary of technologies under investigation
In summary, numerous technological avenues have been pursued, but unfortunately, none of these are ready for clinical use. Notably, validation in human subjects has been achieved only for a subset of these—Pelorus (briefly, in clinical evaluations), 22 the paper-spray mass spectrometry method (in three patients) 19 and photoacoustic detection (in 10 patients), 36 with none of these achieving the necessary requirements needed to support widespread clinical adoption (see Figure 1).
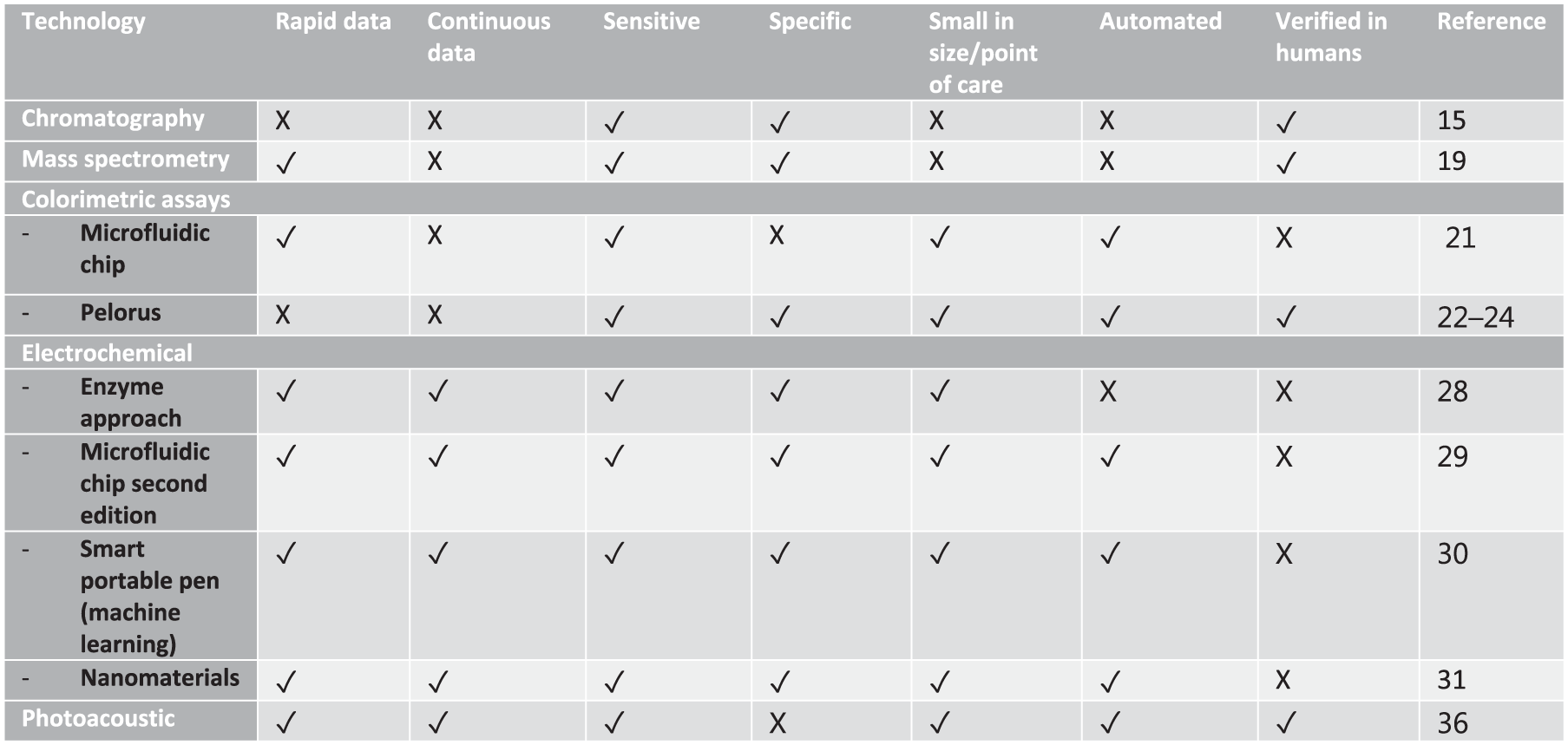
Technological methods assessed for monitoring of propofol levels.
Challenges of device development and implementation
Developing an accurate, real-time propofol monitor for anaesthetic use has proved difficult. Several challenges explain why the development and implementation of technologies has not translated into a clinically applicable device.
Conclusion
A successful, real-time propofol monitoring technology has the potential to provide anaesthetists with confirmation that propofol is being delivered to the patient as desired, allowing TIVA to operate with the same direct feedback that end-tidal concentration monitoring provides for the volatile anaesthetics. It would not replace BIS or other processed EEG technologies, but could complement them, allowing TIVA to operate with the same level of monitoring, and overall risk of awareness, as volatile anaesthetics. There are currently no technologies in use in the clinical setting. Any successful, real-time propofol monitoring technology will need to surmount considerable hurdles to conveniently and accurately provide continuous, clinically relevant measurements of propofol concentrations that can be easily integrated into existing practice. No technologies developed in the past 20 years have been clinically successful; however, they have yielded valuable lessons and incremental progress, setting the stage for future innovation.
Footnotes
Author contributions
Declaration
This manuscript is an honest, accurate and transparent account of this topic, and to the authors’ knowledge, no important aspects have been omitted.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: KWP consults for and owns equity in Nutromics Pty. Ltd., a company developing electrochemical biosensors supporting the real-time monitoring of in vivo drug, metabolite, and biomarker concentrations. The other authors have no conflict of interest to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.