
Abstract
Pre-anaesthesia fasting guidelines typically recommend a six-hour fast for solids and a two-hour fast for clear liquids. Jelly is a fruit-flavoured gelatin dessert that exists as a viscoelastic semi-solid mass when refrigerated but melts back into its liquid form once ingested; therefore, it is not obvious to which category it should belong. We used ultrasound to investigate gastric emptying following ingestion of jelly in a pilot study of 10 fasted healthy adult volunteers. First, a baseline scan was performed to confirm their estimated gastric volume was less than 2.3 ml/kg (the 95th centile for a fasted population). Subjects then ate 400 g of jelly and underwent repeated scans every 10 minutes until their estimated gastric volume had returned to baseline. Median (interquartile range) estimated gastric volume was 0 (0–0.6) ml/kg at baseline, peaked at 3.1 (2.7–4.3) ml/kg 10 minutes post-ingestion and had decreased to 0 (0–0.9) ml/kg by two hours. It took a median (interquartile range) of 70 (47.5–80.0) minutes for estimated gastric volume to fall below 2.3 ml/kg, and 110 (110–130) minutes before it had returned to baseline. These data suggest that, for serving sizes up to 400 grams of jelly there might be no justification for mandating a six-hour fast prior to anaesthesia.
Introduction
Pulmonary aspiration of gastric contents is a rare but serious complication of anaesthesia. 1 Inadequate fasting prior to anaesthesia has been identified as a potentially modifiable risk factor for aspiration. 2 The European Society of Anaesthesiology and Intensive Care (ESAIC) and the American Society of Anesthesiologists (ASA) have both produced guidelines recommending a two-hour fast for clear liquids and a six-hour fast for solids prior to elective surgery.3,4 The ASA guidelines recommend additional fasting time (e.g. eight or more hours) for fried foods, fatty foods or meats. 4
When surgeons, gastroenterologists and dieticians use the term ‘clear liquid’ they are referring to a specific diet given to patients who are preparing for a procedure (e.g. colonoscopy) or incrementally reintroducing oral intake after surgery. 5 Jelly plays an important role in this diet due to its palatability and high caloric density. The list of acceptable clear liquids according to the ESAIC and ASA includes water, pulp-free juice, clear tea and black coffee. Neither list specifically includes or excludes jelly (or its North American equivalent Jell-O), so there is no recommendation as to whether the fasting time for jelly should be two hours or six hours.
There is one professional body that does specifically mention jelly however. The Australian and New Zealand College of Anaesthetists (ANZCA) excludes jelly from its list of acceptable clear liquids prior to anaesthesia on the basis that ‘there are many alternative liquids including just water that have more established risk-benefit profiles’.6,7 A curious anomaly therefore exists in Australia and New Zealand where a hospital inpatient may eat jelly as part of a clear liquid lunch only to have their afternoon procedure cancelled because eating jelly violates ANZCA’s fasting recommendations.
Jelly is made by dissolving sugar (a carbohydrate), gelatin (a protein derived from bovine collagen), flavourings and colouring agents in hot water. When the mixture is refrigerated, it forms a viscoelastic semi-solid mass as the forces favouring its aggregated state (hydrogen bonds) overcome the forces favouring its amorphous state (configurational entropy). 8 Because the melting point of bovine gelatin is lower than that of normal body temperature, 9 jelly melts back into its liquid form once it has been ingested.
There are two reasons for recommending a longer fasting time for solids than for liquids, and both pertain to the risk of aspiration. First, liquids empty from the stomach into the duodenum much faster than solids 10 ; second, aspiration of solids can cause death within minutes from asphyxia whereas aspiration of gastric fluid can result in acid aspiration syndrome. 11 Fasting recommendations for jelly should take into account its physical state following ingestion as well as its gastric emptying time. We therefore performed an observational pilot study whose primary aim was to establish a protocol for assessing and describing the gastric emptying of jelly.
Methods
Ten healthy adult volunteer staff members were recruited from our anaesthetic department. Ethical approval was obtained from our local Human Research Ethics Committee (HREC/2023/MNHA/101360), and all subjects provided written informed consent. Each subject agreed to fast overnight in accordance with ANZCA recommendations, 6 undergo a gastric ultrasound examination to estimate their baseline (fasted) gastric volume, consume 400 grams of jelly (66 kcal per 100 g, 1.6% bovine gelatin) and undergo serial gastric ultrasound examinations every 10 minutes until their estimated gastric volume had returned to baseline.
The study was conducted in March and April 2024. All gastric ultrasound examinations were performed by the same investigator (FM), who had prior experience with over 400 scans. Scans followed a standard clinical algorithm for qualitative and quantitative assessment. 12 Subjects were first positioned supine, and a low-frequency (5–2 MHz) curvilinear probe (C60xp, X-Porte, Fujifilm Sonosite, Inc, Bothell, WA, USA) was used to identify the gastric antrum in a parasagittal plane between the left lobe of the liver anteriorly and the long axis of the aorta posteriorly. Subjects were then turned into the right lateral decubitus position and the cross-sectional area of the gastric antrum was measured.
A subject’s stomach was deemed to be ‘empty’ (i.e. Grade 0) if no solids and no fluid could be visualised in either the supine or right lateral decubitus position. If fluid or solid gastric contents was visualised, the appearance of the contents was noted, and the cross-sectional area (CSA) of the gastric antrum was measured in the right lateral decubitus position. A quantitative estimate of the total volume of gastric fluid (‘gastric volume’) was then calculated using a validated mathematical prediction model 13 :

When the stomach was empty (Grade 0), we assigned a gastric volume of ‘0 ml’. In reality, such stomachs contain a trivial amount of fluid (3–13 ml) 14 ; however, we considered it more logical to round down to zero rather than round up by applying the formula to an antrum that was visibly empty. If clear fluid was visualised in the right lateral decubitus position but not supine (i.e. Grade 1), the subject was considered ‘low risk’ if their estimated gastric volume was less than 1.5 ml/kg, and ‘high risk’ if it was greater than 1.5 ml/kg.
This threshold of 1.5 ml/kg was the upper limit of what was considered ‘normal’ and ‘safe’ in fasted patients at the time our study was conceived. 12 After our study commenced, however, further data emerged suggesting that the upper limit of ‘normal’ (i.e. the 95th centile for a fasted population) should be revised up to 2.3 ml/kg when gastric volume is estimated using ultrasound (as opposed to directly measured via nasogastric suctioning). 15 This did not influence eligibility for our study because all subjects had an estimated gastric volume at baseline of less than 1.5 ml/kg.
Subjects were excluded if they were unable or unwilling to undergo an overnight fast, were pregnant, did not consume animal products (jelly contains bovine collagen), had an estimated gastric volume in excess of 2.3 ml/kg on baseline gastric ultrasound examination, had undergone previous gastric surgery, had a medical condition associated with impaired gastric emptying (e.g. gastroparesis), were taking medications known to affect gastric secretions (e.g. proton pump inhibitors) or gastric emptying (e.g. incretin analogues) or had a body mass index greater than 40 kg/m2.
Baseline gastric ultrasound examination was performed at approximately 0800 hours, with subjects ingesting four 100-g tubs of jelly over the following five minutes. The jelly was sourced from our hospital’s Department of Nutrition and Dietetics, and was identical to what inpatients on a clear liquid diet would receive at our hospital (although inpatients typically only receive one standard serving size of 100 g of jelly per meal). The larger serving size of 400 g was used because the maximum volume of clear liquid recommended by ANZCA is 400 ml two hours prior to anaesthesia. 6 Subjects underwent gastric ultrasound examinations every 10 minutes, repeated until their estimated gastric volume had returned to baseline. On each occasion, three measurements of cross-sectional area were made, and the mean (average) was used when calculating the estimated gastric volume.
We were unaware of any previously published data on the gastric emptying of jelly, so we were unable to perform any statistical power calculations. For this pilot study, a sample size of 10 was chosen because it is similar to what has been used in comparable studies. 16 The primary outcome was a description of gastric volume from the time of jelly ingestion until it had returned to pre-ingestion baseline. Secondary outcomes were time until gastric volume fell below 2.3 ml/kg and time until gastric volume returned to baseline.
Subject characteristics were described by number (percentage) if categorical or median (interquartile range [IQR] [range]) for continuous characteristics. Gastric volume two hours post-ingestion was described as a median with the IQR and range—both in absolute terms (millilitres) and scaled by body weight (millilitres per kilogram). Kaplan–Meier cumulative risk function plots of gastric volume returning to 2.3 ml/kg and subject baseline levels were produced using the survival and ggsurvfit packages.17,18 Subjects were considered to have had the event at a time-point only if subsequent time-points remained below 2.3 ml/kg or baseline respectively. Post hoc comparison of gastric volume two hours post-ingestion versus baseline was performed using a Wilcoxon signed rank test. All analyses were performed using R Statistical package version 4.3.1 (R Foundation for Statistical Computing, Vienna, Austria).
Results
All 10 subjects met eligibility criteria; their demographics and baseline gastric ultrasound assessments are summarised in Table 1. Six subjects had an ‘empty’ stomach (Grade 0) at baseline and so were assigned a baseline gastric volume of 0 millilitres (0 ml/kg). The remaining four subjects were assessed as being at ‘low risk’ of aspiration. Specifically, clear fluid was seen in the right lateral decubitus position but not supine (Grade 1), and their baseline estimated gastric volumes were 28 ml (0.3 ml/kg), 44 ml (0.6 ml/kg), 60 ml (1.1 ml/kg) and 65 ml (1.1 ml/kg).
Demographics and baseline gastric ultrasound assessment. a
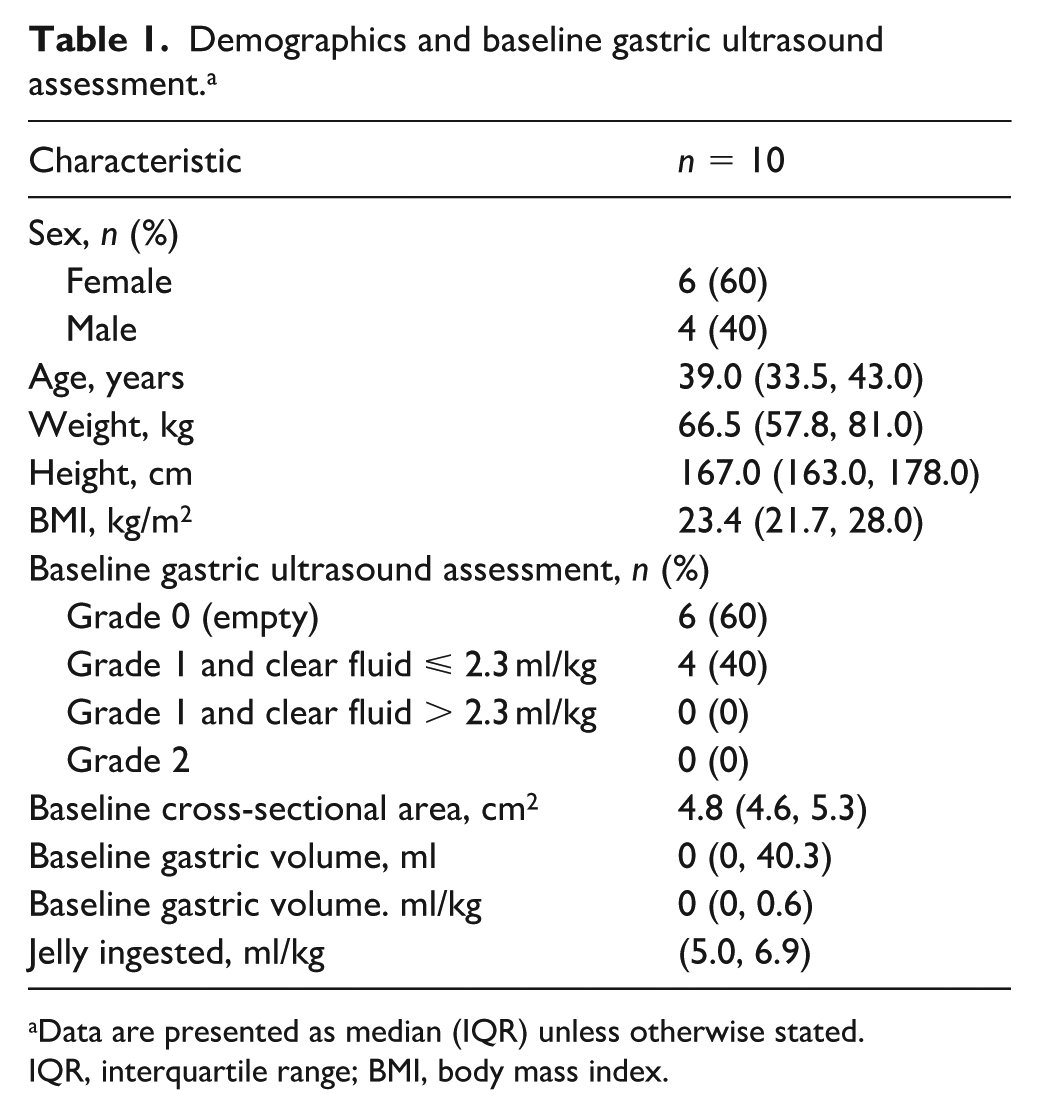
Data are presented as median (IQR) unless otherwise stated.
IQR, interquartile range; BMI, body mass index.
In all 10 subjects, the first ultrasound examination 10 minutes post-ingestion showed a full stomach with multiple hyperechoic foci suspended in anechoic fluid (Figure 1(a)). This is similar to the ‘starry night’ appearance seen after ingestion of effervescent water. 19 No evidence of solid gastric contents was seen in any of the 10 subjects. The sonographic appearance seemed to change from ‘starry night’ to ‘clear fluid’ (Figure 1(b)) after a median (IQR [range]) of 30 (30–47.5 [20–70]) minutes.
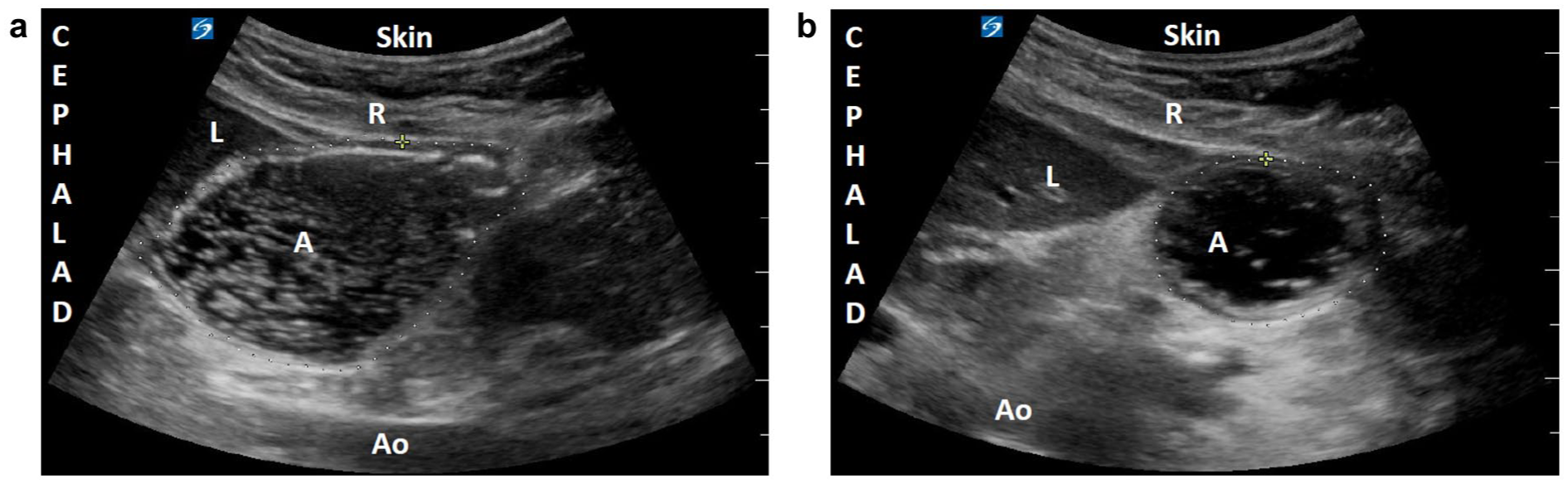
(a) ‘Starry night’ appearance (punctate hyperechoic foci) 10 minutes post-ingestion before jelly has melted. (b) Liquefied jelly solution (anechoic fluid) one hour post-ingestion after jelly has melted. A, antrum; Ao, aorta; L, liver, R, rectus abdominis muscle.
Each of the 10 subjects ingested 400 grams of jelly, which, when scaled to body weight, would have resulted in an initial median (IQR [range]) gastric volume of 6.0 (5.0–6.9 [3.3–7.4]) ml/kg. At the first ultrasound examination 10 minutes later, the median (IQR [range]) estimated gastric volume based on the observed antral cross-sectional area was 233 (196–260 [179–366]) ml. When scaled to body weight, estimated gastric volume increased from a median (IQR [range]) of 0 (0–0.6 [0–1.1]) ml/kg at baseline to a peak of 3.1 (2.7–4.3 [1.8–5.3]) ml/kg 10 minutes post-ingestion before subsequently decreasing (Figure 2).
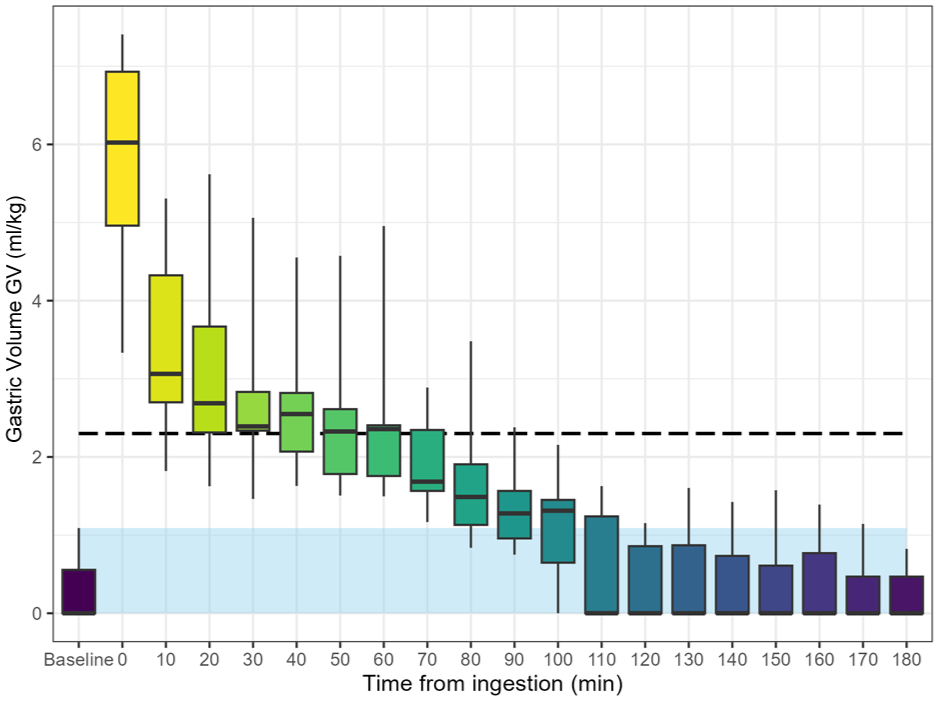
Estimated GV versus time. The dashed line represents the 95th centile for a fasted population and the shaded region represents baseline GV. Boxplots at each time point display the median, first and third quartiles, and range. GV, gastric volume.
Two hours post-ingestion, the median (IQR [range]) estimated gastric volume had decreased to 0 (0–60 [0–101]) ml, or 0 (0–0.9 [0–1.2]) ml/kg when scaled to body weight. The median (range) difference between estimated gastric volume at two hours versus baseline was 0 (–0.3 to 0.8) ml/kg which was not statistically significant (Wilcoxon signed rank test (V=5), P=0.50).
Subject-level variability in the change in estimated gastric volume was noted (Figure 3). In two subjects, the estimated gastric volume was higher at two hours compared with baseline (Subject 2: 0.8 ml/kg versus 0 ml/kg; Subject 3: 1.2 ml/kg versus 0.6 ml/kg); whereas in another two subjects it was lower at the two-hour mark (Subject 9: 0.9 ml/kg versus 1.1 ml/kg; Subject 10: 0 ml/kg versus 0.3 ml/kg). There was no difference in the remaining six subjects, with the most common finding being an ‘empty’ stomach at both baseline and two hours post-ingestion. All subjects had an estimated gastric volume well below the ‘at risk’ threshold of 2.3 ml/kg after two hours.
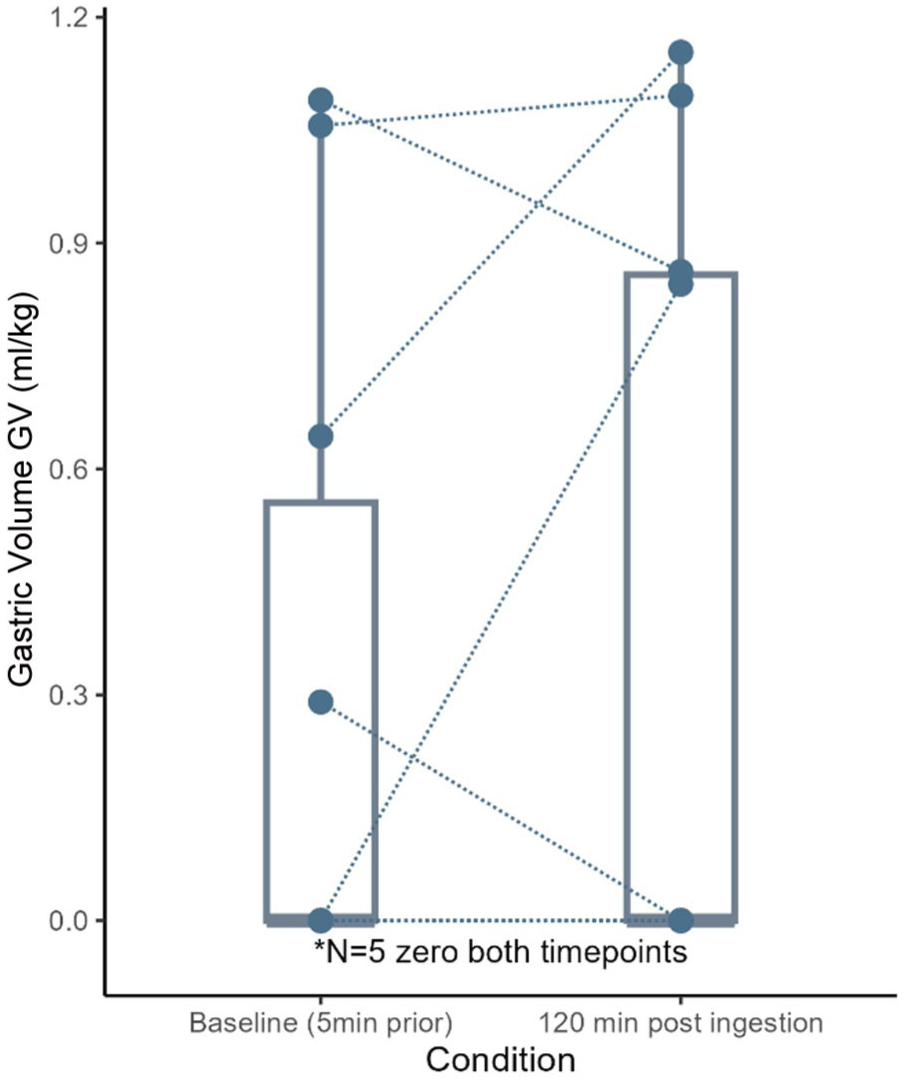
Estimated GV two hours post-ingestion versus baseline. GV, gastric volume.
The median (IQR [range]) time until estimated gastric volume fell below 2.3 ml/kg was 70 (47.5–80.0 [30–100]) minutes (Figure 4). This means that, from 100 minutes post-ingestion onwards, no subject assessed with gastric ultrasound according to a standard clinical algorithm would have been deemed to be at ‘high risk’ of aspiration when using the threshold of 2.3 ml/kg (the 95th centile for a fasted population).12,15
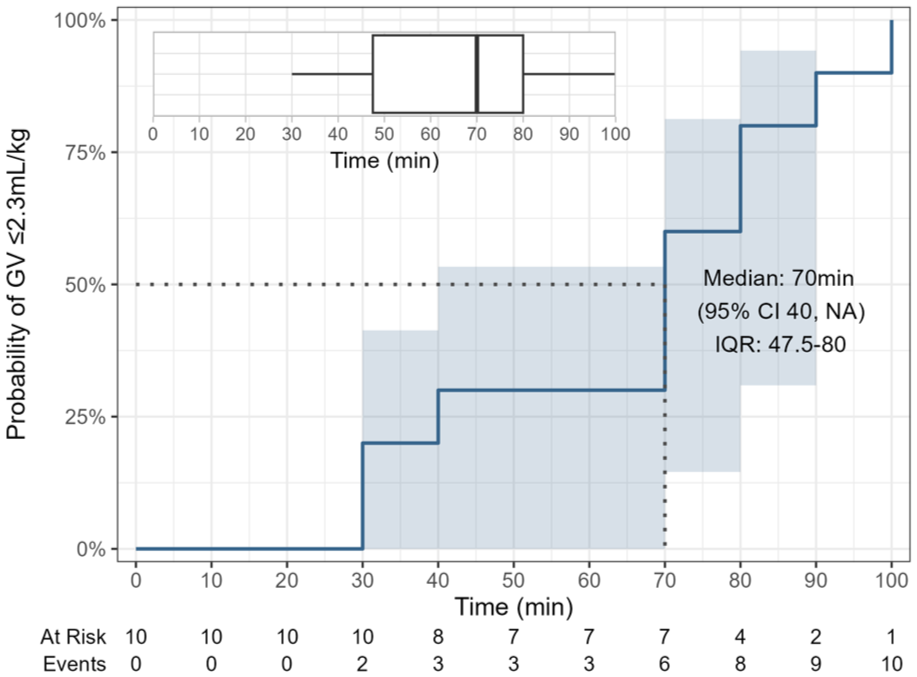
Kaplan–Meier cumulative risk function plot for showing probability of estimated GV being less than 2.3 ml/kg. Dotted line indicates median time before estimated GV falls below 2.3 ml/kg. Risk table displays the number of subjects whose estimated GV remains above 2.3 ml/kg. Inset boxplot displays the median, first and third quartile, and range. GV, gastric volume; CI, confidence interval; IQR, interquartile range.
The median (IQR [range]) time until estimated gastric volume had returned to baseline was 110 (110–130 [100–180]) minutes (Figure 5). There were two outliers whose estimated gastric volume remained above baseline until well into the third hour. Subject 2 had an estimated gastric volume of 0 ml at baseline, 101 ml (0.8 ml/kg) at two hours and did not return to baseline until 170 minutes post-ingestion. Subject 3 had an estimated gastric volume of 44 ml (0.6 ml/kg) at baseline, 80 ml (1.2 ml/kg) at two hours and did not return to baseline until 180 minutes post-ingestion.
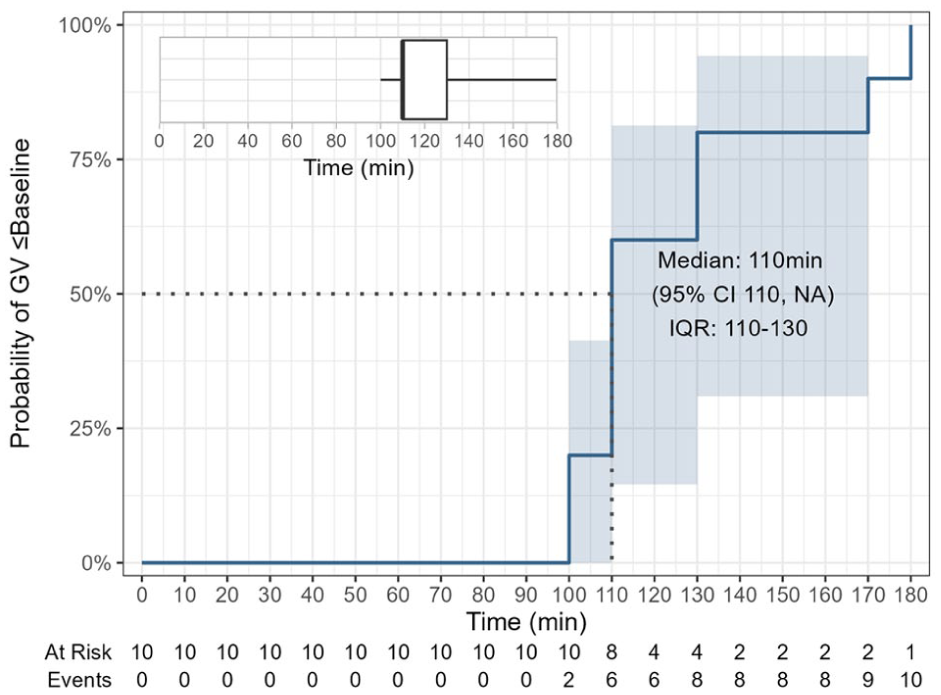
Kaplan–Meier cumulative risk function plot for showing probability that estimated GV has returned to baseline. Dotted line indicates median time before estimated GV returns to baseline. Risk table displays the number of subjects whose estimated GV remains above baseline. Inset boxplot displays the median, first and third quartile, and range. GV, gastric volume; CI, confidence interval; IQR, interquartile range.
Discussion
Our study provides a detailed description of gastric emptying following ingestion of a large serving of jelly in healthy adult volunteers. Two hours after ingestion of 400 g of gelatin-based jelly, none of our 10 subjects were found to have gastric volumes or contents that would be considered ‘at-risk’ for sequelae of aspiration examined using a standard clinical algorithm for gastric ultrasound assessment. 12 Specifically, by two hours post-ingestion all of the jelly had melted back into its liquid form; and all subjects had an estimated gastric volume well below the ‘at risk’ threshold of 2.3 ml/kg (the 95th centile for a fasted population), 15 and below the original ‘at risk’ threshold of 1.5 ml/kg (a more conservative and widely accepted benchmark) 12 ; the median (range) estimated gastric volume of our subjects was similar to what it had been at baseline prior to ingestion (however, our study would not have been powered to detect a difference unless that difference was very large).
The small sample size does limit our ability to make conclusive statements; however, there are larger studies on this topic. A 2024 study by Correia et al. comparing 100 ml of water with 100 ml of jelly in 25 healthy adults found that the estimated gastric volume two hours post-ingestion of jelly was no higher than for water. 20 Theirs was an interventional study comparing gastric volume between groups at a set point in time, whereas ours is a smaller observational study with a more detailed description of gastric volume over a more extended period of time. Our study used a larger quantity of jelly (400 g versus 100 g), and evaluated gastric volume every 10 minutes until it had returned to baseline, whereas theirs took a single measurement at two hours. When considered together, the data from these two studies suggest that two hours may be a reasonable fasting time following a standard serving size of jelly.
We demonstrated a definite change in the sonographic appearance of jelly in the first hour post-ingestion. It is unclear whether the punctate hyperechoic foci in Figure 1(a) are semi-solid jelly particles suspended in liquefied jelly, or entrained air bubbles trapped within the semi-solid jelly. Regardless, the observation that they disappear within the first hour confirms that jelly melts back into its liquid form well before the two-hour mark.
We observed two outlier subjects whose estimated gastric volume remained above baseline (but below 2.3 ml/kg) until well into the third hour—a finding that has also been observed in a similar study on high-calorie clear liquids. 21 This suggests that a longer fast (e.g. three hours or more) may reduce gastric volume more than a two-hour fast in at least some people, some of the time. When this hypothesis was tested in a randomised study, however, no difference was found in mean gastric volume two hours post-ingestion of a carbohydrate drink compared with 12 hours post-ingestion. 22
It is worth exploring why the presence of a modest volume of clear fluid, such as 100 ml at the two-hour mark in Subject 2, does not necessarily imply that a patient is ‘at risk’ of aspiration. For aspiration to occur, there must not only be a large volume of gastric fluid in the stomach, but also a failure of the lower oesophageal sphincter, regurgitation of gastric contents and failure of the patient (and anaesthetist) to prevent the gastric contents from entering the respiratory tract. 23 Clearly there is a positive correlation between gastric volume and aspiration risk, but the relationship is non-linear and multifactorial.
The threshold gastric volume at which a patient’s risk of aspiration starts to increase has been a source of debate for decades.24,25 Early efforts to define this threshold focused on the question: ‘What volume causes harm if aspirated (in animal models)?’ 26 The resultant cut-offs proved impractically low because healthy fasted human patients routinely exceed them.27,28 The guiding question therefore shifted to: ‘What volume (measured using nasogastric suctioning) is normal in a fasted population?’. Thus 1.5 ml/kg emerged as a widely accepted benchmark and was adopted into gastric ultrasound risk-stratification algorithms. 29
Although gastric ultrasound does have a very high inter-rater and intra-rater reliability, 30 it is not a precise measurement of gastric volume. The formula for calculating gastric volume overestimates by a factor of two the actual volume as measured via gastroscopy. 14 This may explain how the upper limit of normal can be 1.5 ml/kg when measured directly but 2.3 ml/kg when estimated using ultrasound. This is not a contradiction, it simply reflects two different modalities for observing the same physiological phenomenon. We used the 2.3 ml/kg threshold because our endpoints were based on ultrasound observations, not direct measurements.
The rationale for pre-anaesthesia fasting is to allow enough time for a patient’s gastric contents to empty into the duodenum and therefore reduce the likelihood of aspiration. The rate of gastric emptying is determined by the physical characteristics and caloric density of the ingested food. 10 For example, Okabe et al. demonstrated that high-calorie clear liquids empty more slowly than low-calorie clear liquids, 16 and that milk (which contains fat and protein) empties at a rate similar to carbohydrate-containing clear liquids (which contain no fat or protein) provided the caloric content is equivalent.
The ASA published a modular update to their Practice Guidelines in 2023 that specifically addresses the topic of carbohydrate-containing clear liquids. 31 This document does not differentiate clear liquids based on their caloric density; however, it does suggest that protein-containing clear liquids do not appear to delay gastric emptying, and may result in less hunger compared with non-caloric or carbohydrate-containing clear liquids. If one wishes to simply maintain hydration and allay thirst during a short pre-operative fast, then water (or cordial) is preferable to jelly. For extended fasts, however, jelly may have an advantage due to its palatability, high energy content and greater potential to promote satiety.
Our study does have some limitations. First, our results may not be generalisable to the broader population, or to other brands of jelly. Brands that do not use bovine gelatin as a thickener (e.g. premade ‘ready-to-eat’ jelly or vegan jelly) may have a higher melting point, which could result in slower gastric emptying. Secondly, our comparison of estimated gastric volume at two hours versus baseline was conducted post hoc on a small sample size. It is possible that an adequately powered (larger) study may find a higher gastric volume at two hours versus baseline; however, even such a finding would not necessarily indicate a higher aspiration risk if the estimated gastric volume at two hours was less than 2.3 ml/kg.
We often observed increases in estimated gastric volume from one measurement to the next, despite all subjects exhibiting a downward trend. This is not surprising when one considers how estimated gastric volume is calculated. Antral cross-sectional area is measured from serosa to serosa, 13 which means the calculated gastric volume depends on how much fluid is seen within the lumen as well as the full thickness of the gastric wall. Changes in the shape and size of the muscular wall will produce fluctuations in the calculated gastric volume. This is most evident during the third hour (data shown in Figure 2), a time point at which only two subjects were still contributing data points and both of their stomachs were almost back to baseline.
Should professional bodies such as the ESAIC, ASA and ANZCA include jelly on the list of acceptable clear liquids that they recommend patients ingest up until two hours prior to surgery? Data from our small pilot study are insufficient to either support or dismiss existing fasting guidelines. However, the current ANZCA recommendation to fast for six hours after jelly is not supported by any published evidence, neither is there a clear rationale for why jelly should be excluded from the clear liquids category. To date, only two studies (ours, and the study by Correia et al.) have investigated this question directly and both suggest that aspiration risk is no longer elevated two hours after jelly ingestion. 20 Given the uncertainty, a cautious clinician faced with anaesthetising a patient two hours after eating jelly may insist on a longer fast (e.g. three hours), or perform gastric ultrasound to help stratify aspiration risk, but mandating a six-hour fast seems unjustifiably conservative.
Footnotes
Acknowledgements
We wish to thank Fujifilm Sonosite, Inc for the loan of their X-Porte ultrasound machine and probe used in this study.
Author Contributions
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.