
Abstract
Neck rescue encompasses a variety of techniques and terms used to describe direct access to the trachea to allow delivery of oxygen into the airway, typically in the context of a ‘can’t intubate, can’t oxygenate’ (CICO) scenario. Anaesthetists rely on CICO simulation exercises to obtain competency in neck rescue using commercially available plastic airway models. Recently, innovations in three-dimensional (3D)-printed airway models and ‘symbiotic culture of bacteria and yeast’ (SCOBY) skins have been trialled for CICO training. We undertook a study to compare the fidelity of a 3D-printed airway model and SCOBY skin model with a commercially available plastic and foam model (Crico-Trainer ‘Frova’, VBM-Medizintechnik GmbH, Sulz am Neckar, Germany) trialled by 27 volunteer anaesthesia specialists and trainees. Study participants performed neck rescue on all model variants and provided structured feedback. The 3D-printed model with SCOBY skin was found to have the highest fidelity for neck rescue training and was the model preferred by most participants. Model fidelity, environmental impact, and ethical considerations were rated as important or very important by participants. Further studies are needed to confirm these findings in other hospital settings.
Keywords
Introduction
Neck rescue encompasses a variety of techniques and terms used to describe direct access to the trachea in order to entrain oxygen into the airway, including emergency front-of-neck access (eFONA), cricothyroidotomy, tracheostomy, percutaneous emergency oxygenation and others. 1 Neck rescue is performed in the context of a ‘can’t intubate, can’t oxygenate’ (CICO) scenario, where an anaesthetist has been unable to achieve patient oxygenation using routine airway interventions such as bag-mask ventilation, or insertion of a supraglottic airway device or tracheal tube. Can’t intubate, can’t oxygenate events are estimated to occur in approximately one in 3000 patients in the operating room and as a result anaesthetists rely on simulation training exercises to achieve competency in performing neck rescue techniques. 2
Neck rescue simulation has been shown to increase technical proficiency and reduce time to oxygenation in benchtop and animal studies. 3 Commercially available models comprise a rigid plastic scaffold (Figure 1, left) that represents the cartilaginous and bony airway structures, covered with synthetic materials designed to mimic the subcutaneous tissues and skin of the anterior neck. 4 While commercially available neck rescue simulation models have demonstrated efficacy for neck rescue skills acquisition in a simulation environment, 5 our prior studies have reported the feasibility of using three-dimensional (3D)-printed airway models for neck rescue simulation in both anatomically normal airways and in acute airway pathologies.6,7 These models have been shown to be cost-effective and anatomically accurate.6–8 While porcine skin has been used to achieve a more realistic representation of human skin, 9 we have recently described the use of a biological skin produced by symbiotic culture of bacteria and yeast (SCOBY) for neck rescue simulation. 10
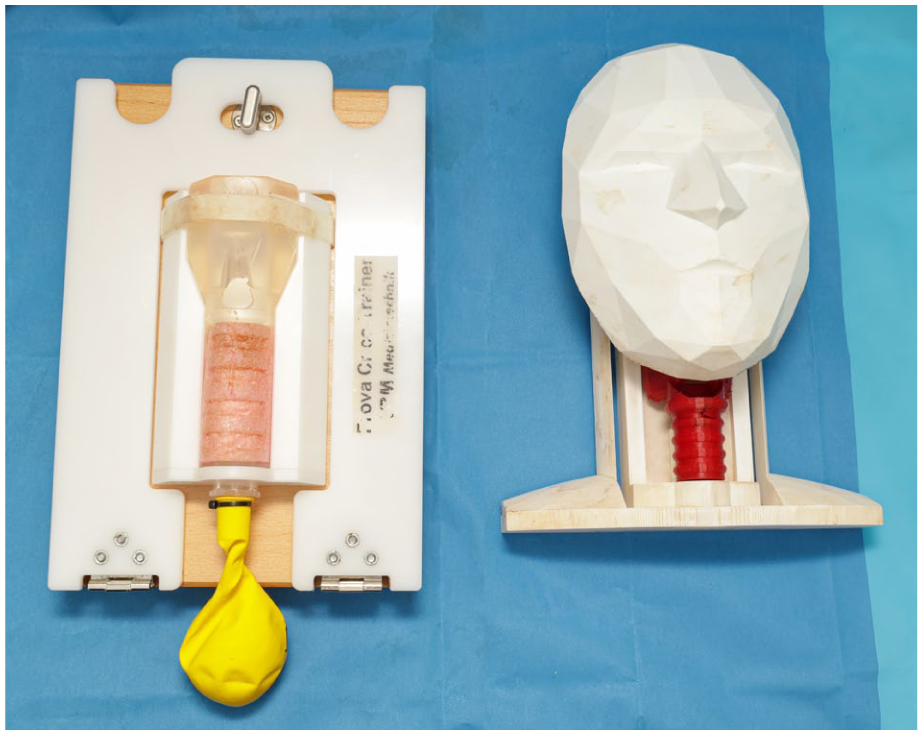
Crico-Trainer trachea (left), 3D-printed trachea (right). 11
However, there have been no direct comparisons of the fidelity (likeness to human tissues), and user satisfaction of custom 3D-printed models to commercially available models for the purposes of neck rescue simulation, nor of commercially available synthetic skin tissue to artificial skin produced by SCOBY. Accordingly, we designed a study to investigate the relative fidelity of two novel components of a neck rescue model: a commercially available versus a 3D-printed airway, and SCOBY skin compared with a commercially available synthetic skin. We hypothesised that simulation participants would report the highest neck rescue scenario fidelity with the combination of a 3D-printed airway and SCOBY skin model.
Methods
Potentially eligible participants were recruited from a single large tertiary hospital in New Zealand. Anaesthesia specialists and trainees were invited to participate. Anaesthesia doctors of senior house officer grade or below and medical students were excluded. Anaesthetists were provided with electronic study information by email one week prior to the study workshop. Study information included a link to standardised 5-minute videos of neck rescue concepts (Supplemental Appendix 1). Ethics review was undertaken by the University of Otago Wellington School of Medicine and approval for the study was granted (project number 24/0427, approved 30 September 2024).
Participants were randomly assigned by drawing numbered cards to one of four groups and invited to perform neck rescue sequentially on each of the four models: (a) Crico-Trainer trachea with synthetic skin; (b) Crico-Trainer trachea with SCOBY skin (Figure 2, left and Figure 3, left); (c) 3D-printed trachea with synthetic skin; and (d) 3D-printed trachea with SCOBY skin (Figure 2, right and Figure 3, right). In keeping with the Vortex approach, 12 participants chose their preferred technique for cricothyroidotomy (cannula or scalpel-bougie) and used that same technique at each of the four stations.
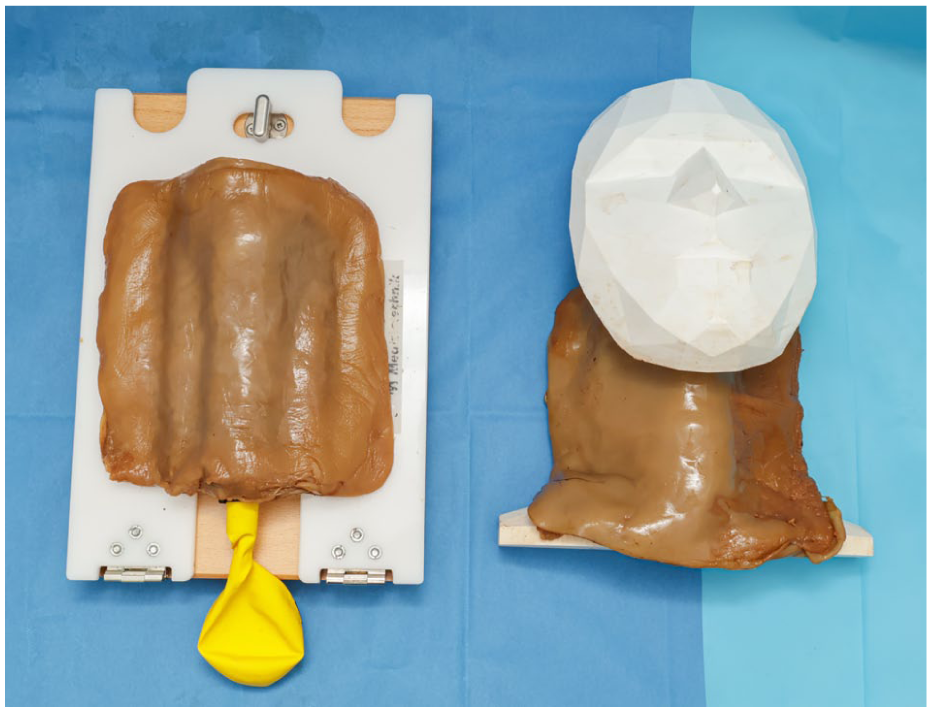
Crico-Trainer trachea with SCOBY skin (left), 3D-printed trachea with SCOBY skin (right).
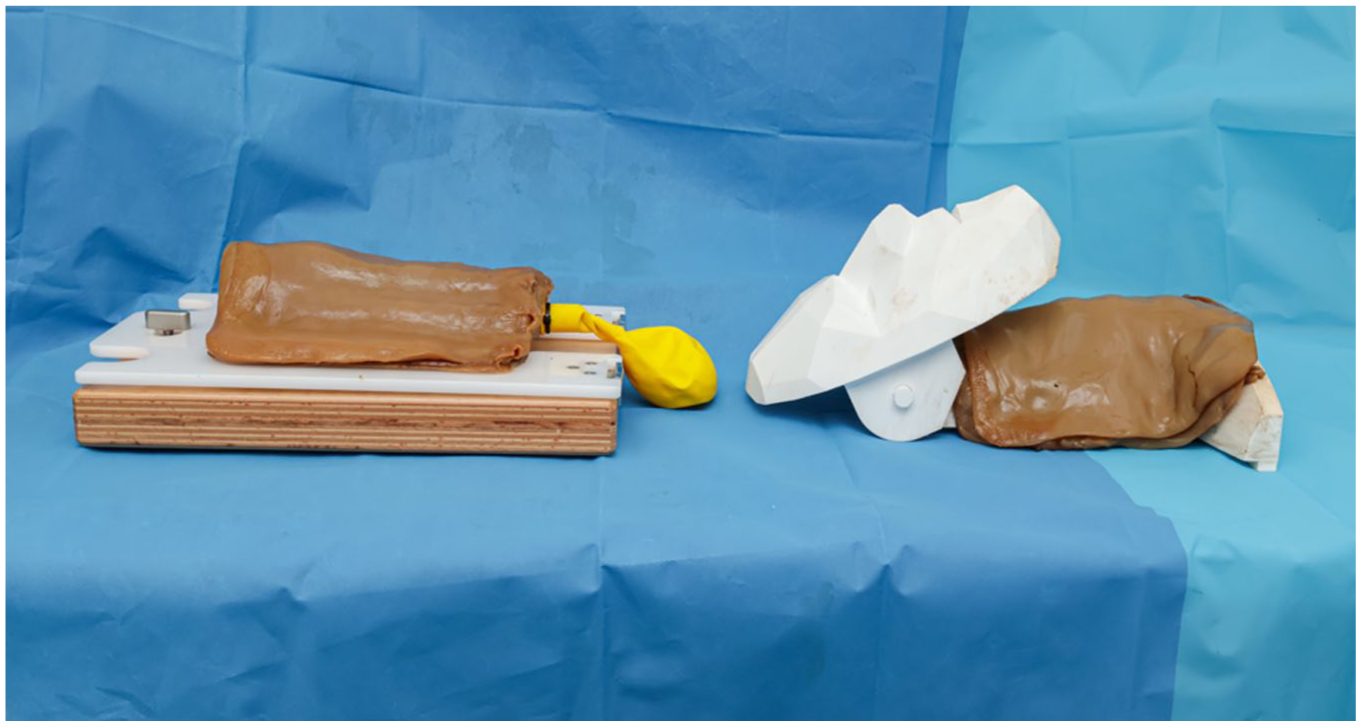
Crico-Trainer trachea with SCOBY skin (left), 3D-printed trachea with SCOBY skin (right).
Participants were supervised by instructors during simulation with all models, but no direct feedback was given on technique. At the completion of the workshop the participants were asked to complete anonymous feedback on the simulator combinations that were used. The questionnaire is attached as Supplemental Appendix 2.
Results
A total of 27 anaesthesia doctors participated in the study, 14 specialist anaesthetists and 13 anaesthesia training registrars.
Two of the 27 participants (7%) reported that they had been involved in neck rescue on a patient in an emergency clinical setting. Thirteen (48%) had performed neck rescue on a live animal or cadaver for training.
When asked about the usefulness of each model specifically for rehearsing neck rescue, the combination of a 3D-printed model airway with SCOBY skin was rated as useful by more participants than any other model combination. Overall, 26 of 27 (96%) respondents indicated they either ‘strongly agree’ (19 of 27) or ‘agree’ (seven of 27) that the model combination of the 3D-printed airway with SCOBY skin was a useful tool. (Figure 4).
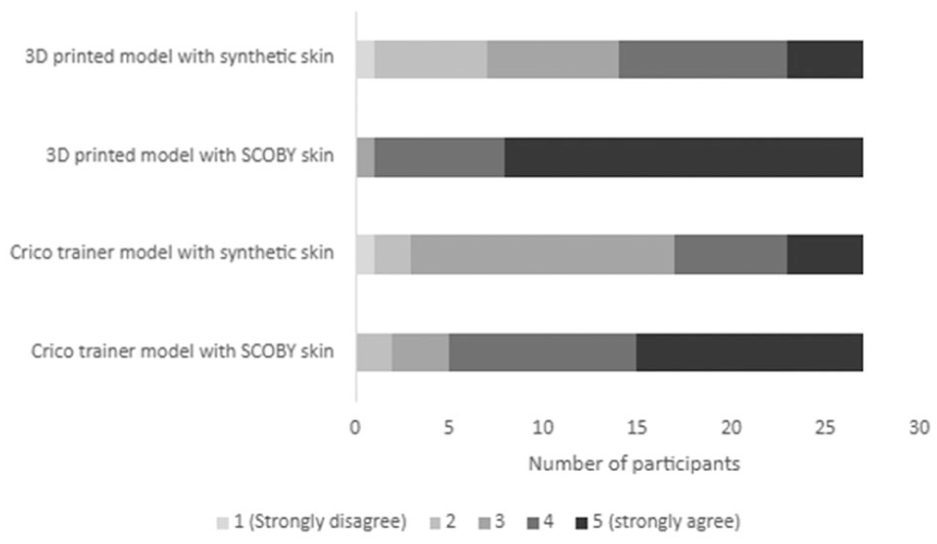
Participant responses regarding the usefulness of model combinations in practising neck rescue.
Sixty-seven percent of respondents found the 3D-printed model with SCOBY skin to resemble most closely the clinical reality of cutting through skin, with 22% finding the Crico-Trainer with SCOBY skin to be more realistic. Synthetic skin was found to be less realistic, with 7% finding this combined with the Crico-Trainer to be most realistic, and 4% preferring the 3D-printed model with synthetic skin.
Of those who had previously performed neck rescue on a live animal or cadaver, 77% (10 of 13) preferred the 3D-printed model with SCOBY skin overall. Fifteen percent (two of 13) preferred the Crico-Trainer with SCOBY skin and 8% (one of 13) preferred the 3D-printed model with synthetic skin.
In terms of comparison with human anatomy, 81% found the 3D-printed model with SCOBY skin to be most realistic. Eleven percent found the Crico-Trainer model with SCOBY skin to be most realistic, followed by 4% each for the 3D-printed model with synthetic skin and Crico-Trainer with synthetic skin.
Respondents were asked which model was their preferred choice overall. The majority (78%) preferred the 3D-printed model with SCOBY skin. The second most preferred (15%) was the Crico-Trainer model with SCOBY skin. Both the 3D-printed model with synthetic skin and Crico-Trainer with synthetic skin were preferred by 4% (Figure 5).
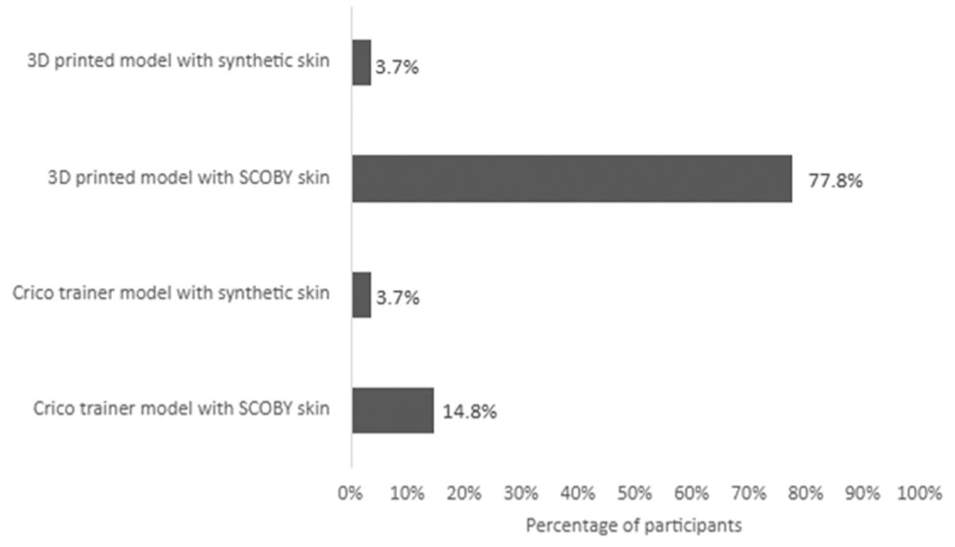
Participant preferences for model combinations.
The 3D-printed model with SCOBY skin was the preferred model combination for training in neck rescue skills, regardless of the preferred participant-reported neck rescue technique. It was preferred by 75% of those whose preferred technique was cannula cricothyroidotomy, and by 79% of those whose preferred technique was scalpel-bougie cricothyroidotomy.
Respondents were also asked about the importance of specific factors that contributed to which model they chose as their overall preference. Model fidelity was felt to be the most important factor, with 74% of respondents indicating that this was ‘very important’. Environmental impact and ethical considerations were each determined to be ‘very important’ for 33% of those taking part. Cost was the least important consideration, with 3.7% thinking this was ‘very important’, and 22.2% responding that this was ‘not important’ (Figure 6).
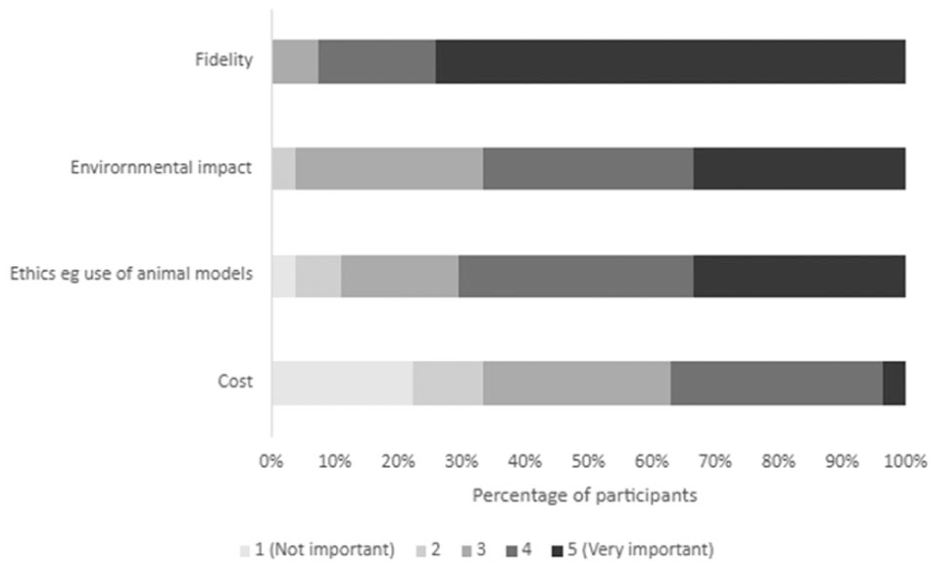
Weight of importance of specific factors contributing to participants overall preferred model combination.
Participants were asked to provide free-text feedback about other factors that determined the overall preference for specific model combinations. Common themes included the texture of the skin, the mobility of the skin, similarity to normal human anatomy, general realism, and environmental factors.
In terms of texture, participants responded that ‘SCOBY skin texture is more realistic’ in comparison with synthetic skin, ‘slightly slimy feeling on the surface close to real life with a sweaty patient or blood’ and ‘SCOBY gives a more tactile experience which resembles human skin’.
The mobility of the model and skin was also commented on as being an important factor. Comments included that the ‘SCOBY moves more, slippery, more difficult, closer to real life’ and ‘mobility of the SCOBY much more similar to skin than foam’.
Anatomical considerations included that ‘the 3D-printed model chin makes for a more realistic angle of approach’ and ‘the Crico-Trainer is very easy to access the airway; too easy as the CM membrane is too wide’.
Further examples of quotes and themes can be found in Supplemental Appendix 3.
Discussion
This study obtained feedback from practising anaesthesia specialists and training registrars on the fidelity and overall realism of a SCOBY skin and 3D-printed trachea model compared with a commercially available Crico-Trainer with synthetic skin. The majority of participants showed a strong preference for the models using a SCOBY skin compared with synthetic skin, and more respondents preferred the 3D-printed trachea than the Crico-Trainer model.
Prior research conducted by our research group has demonstrated a feasible method for the safe production, storage, and reuse of SCOBY in large quantities, providing an example of an environmentally friendly and cost-effective neck rescue model for medical simulation. 9
There are several limitations to our study. Firstly, the small sample size of anaesthetists from a single institution limits the generalisability of the study findings. The 3D-printed trachea with SCOBY skin model should therefore be trialled and evaluated across a wider range of anaesthetists and hospitals prior to widespread use in simulation practice. Additionally, while the distribution of anaesthesia specialists and training registrars was balanced and represented a range of clinical experience, few participants had previously performed neck rescue in a real clinical setting. Therefore, despite most participants rating this model as closely resembling that of human anatomy, this is largely based on perception rather than in vivo experience. Future studies evaluating neck rescue models might include head and neck surgeons experienced in front-of-neck and tracheal surgery in order to overcome this limitation. A limitation of the models themselves includes the inability to emulate bleeding, an inevitable complication that would be seen in a real clinical setting. Furthermore, participants did not perform neck rescue on models with impalpable anatomy, nor on paediatric models. This may present additional areas for further model development and research, particularly given the increasing prevalence of obesity in the surgical population.
The SCOBY skin and synthetic skin vary in their thickness. The synthetic skin was used as specified, with a single layer placed over the tracheal models, whereas the SCOBY models used multiple layers of SCOBY to represent skin and soft tissue. While this may be viewed as a limitation of the study, we submit that the ability to layer the SCOBY to represent skin and soft tissues in both simulated palpable and non-palpable front-of-neck anatomy represents an added benefit of the SCOBY models. Furthermore, the SCOBY is cheap to produce, meaning that there are minimal cost implications to this approach.
The dimensions of the cricothyroid membrane differ between the Crico-Trainer model (width 15 mm × height 17 mm) and the 3D-printed model (width 25 mm × height 17 mm). While the 3D-printed model is based on human anatomy, the width of the cricothyroid membrane could be reviewed in future models to improve real-life fidelity further. Nevertheless, despite the Crico-Trainer model having a narrower cricothyroid membrane than the 3D-printed model, some participants perceived the opposite to be true. This may be explained by the lack of an anatomical head and mandible on the Crico-Trainer model, allowing easier neck access compared with the 3D-printed model, and creating the perception of easier access to the cricothyroid membrane overall. The absence of an anatomical head and neck on the Crico-Trainer may also explain the difference in user perception between the clinical reality of cutting through skin with the 3D-printed model and the Crico-Trainer model when both are used with SCOBY skin.
Conclusion
Neck rescue simulation training is crucial in preparing anaesthetists for the rare, but life-threatening CICO situation. Improving the fidelity of airway models for skill acquisition and maintenance is likely to increase technical proficiency and success rates for neck rescue. The 3D-printed model airway with SCOBY skin is a useful, high-fidelity, and cost-effective tool for neck rescue simulation training, with minimal adverse environmental impact that is rated favourably by anaesthesia specialists and training registrars compared with a commercially available neck rescue training model.
Supplemental Material
sj-docx-1-aic-10.1177_0310057X261443357 – Supplemental material for Evaluation of novel materials for front-of-neck access simulations
Supplemental material, sj-docx-1-aic-10.1177_0310057X261443357 for Evaluation of novel materials for front-of-neck access simulations by Monica E Mullally, Laura J Bond, Raja R Palepu, Jeremy S Young and Daniel R Frei in Anaesthesia and Intensive Care
Footnotes
Author contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.