
Abstract
Leaks from nitrous oxide (N2O) infrastructure have been identified as a significant contributor to the greenhouse gas emissions of healthcare facilities. Recent studies in Australia and in the United Kingdom have found at least half (and often more than 70%) of the N2O supplied to many healthcare facilities leaks from medical pipelines and associated infrastructure before clinical administration. To assist in addressing this issue, the University of Melbourne, in collaboration with the Interim Australian Centre for Disease Control and the Australian Government’s Department of Health and Aged Care, published Detecting and reducing nitrous oxide leaks in healthcare facilities – a practical guide (the ‘Guide’) in 2024. This article summarises the Guide and best practice approaches for detection and reduction of N2O leaks in healthcare facilities across Australia. It is intended to assist clinicians and facility managers to identify appropriate methods to test for N2O leaks, make an informed choice about the most appropriate way to supply N2O to a facility and reduce waste from N2O leaks in their healthcare facility.
Introduction
Nitrous oxide (N2O), a gas used for labour analgesia, sedation and dentistry, and as an adjunct in general anaesthesia, is a significant contributor to health system greenhouse gas emissions, accounting for around 20% of the direct (scope 1) emissions of the Australian health system. 1 In Australian healthcare facilities N2O is often supplied from a central store of cylinders and delivered through a network of rigid pipelines to areas of a facility for administration. Pipeline supply can also be present in non-clinical areas of healthcare facilities for legacy reasons as facilities are renovated or upgraded.
Leaks in N2O piping infrastructure have been identified as a significant contributor to the greenhouse gas emission footprint of anaesthetic gas use in healthcare and are financially wasteful. Recent studies in Australia and in the United Kingdom have found at least half (and often more than 70%) of the N2O supplied to healthcare facilities leaks from infrastructure before clinical administration.2–9 Given that N2O is both colourless and odourless, leaks need to be actively detected.
International interest in addressing N2O leaks gained momentum in 2021, when an audit of 16 hospitals in the Lothian National Health Service revealed that waste via leaks accounted for over 95% of N2O procured.4,10 Further audits at 38 sites in Scotland demonstrated that 83–100% of purchased N2O was lost via infrastructure leaks.4,5 Numerous healthcare facilities in Scotland have subsequently decided to decommission their piped supply of N2O. 4 There is growing international recognition of the imperative to reduce waste from N2O leaks and an increasing body of opinion, most recently in a joint statement published by the Australian and New Zealand College of Anaesthetists, the Australian Society of Anaesthetists and the New Zealand Society of Anaesthetists, that piped N2O does not have a place in a sustainable high-quality health system.11–15
The Australian Government committed to reducing emissions from medical N2O in the 2023 National Health and Climate Strategy, which sets out a whole-of-government plan for addressing the health and wellbeing impacts of climate change, whilst also mitigating the contribution of the health system to climate change through the generation of greenhouse gas emissions in care delivery. 1 Action 4.13 of the Strategy commits to working to improve patient care, protect health care staff and reduce greenhouse gas emissions from N2O, by:
(a) Reducing waste from N2O leaks;
(b) Dealing with venting, the practice of releasing unused N2O when cylinders are returned for refill;
(c) Educating on appropriate use.
Background methodology
As part of the work to implement the National Health and Climate Strategy, in 2024 the Australian Government Department of Health and Aged Care worked with the University of Melbourne to publish a practical guide to detecting and reducing N2O leaks in healthcare facilities. 16 This article summarises key recommendations from the Guide as well as recent Australian progress and cases studies.
Australian Standards
Australian Standard 2896:2021 (AS 2896:2021) sets out procedures for installation and testing of non-flammable medical gas pipeline systems. 17 AS 2896:2021 informs the Australasian Health Facility Guidelines, which act as an overarching guide describing all required elements and relevant standards that should be adhered to in the construction and maintenance of healthcare facilities.
Under AS 2896:2021, monitoring and maintenance of medical gas pipeline systems is limited to visual checks, pressure gauge checks and the ‘soapy water bubble test’ (4.13.5). The last, which involves spraying detergent onto N2O pipes and valves to search for leaks identified as bubbles, provides only a rudimentary indication of the presence of leaks in specific locations and does not test the system in its entirety or allow for the size of any given leak (i.e. the volume of N2O being leaked) to be accurately determined.
Australian healthcare facilities that have passed the AS 2896:2021 maintenance standards have subsequently been shown to have major leaks when applying alternative testing methods for N2O leaks.6–8 This might reflect that the Australian Standards currently do not require regular ongoing leak testing of the entirety of the rigid pipeline network after commissioning (except for a requirement to pressure test after major modifications or prolonged downtime). It might also reflect that the Australian Standards currently do not provide specific guidance on the use of more accurate and comprehensive leak testing methodologies than the ‘soapy water bubble test’. 17
The additional methods described in the Guide and this article can significantly improve the sensitivity by which N2O leaks are detected as part of an ongoing maintenance regime.
In recognition of the new understanding of N2O leakage from medical pipelines, the Australasian Health Facility Guidelines (AHFGs) were updated in 2024. The guidelines now state that reticulated N2O and associated scavenge outlets are not mandatory for a healthcare service, and that point-of-care cylinders can meet clinical requirements for the majority of healthcare facilities. In addition, the new AHFGs require that consideration be given to both measurement and monitoring of N2O usage, and the management of N2O leakage. 18
Potential sources of leaks
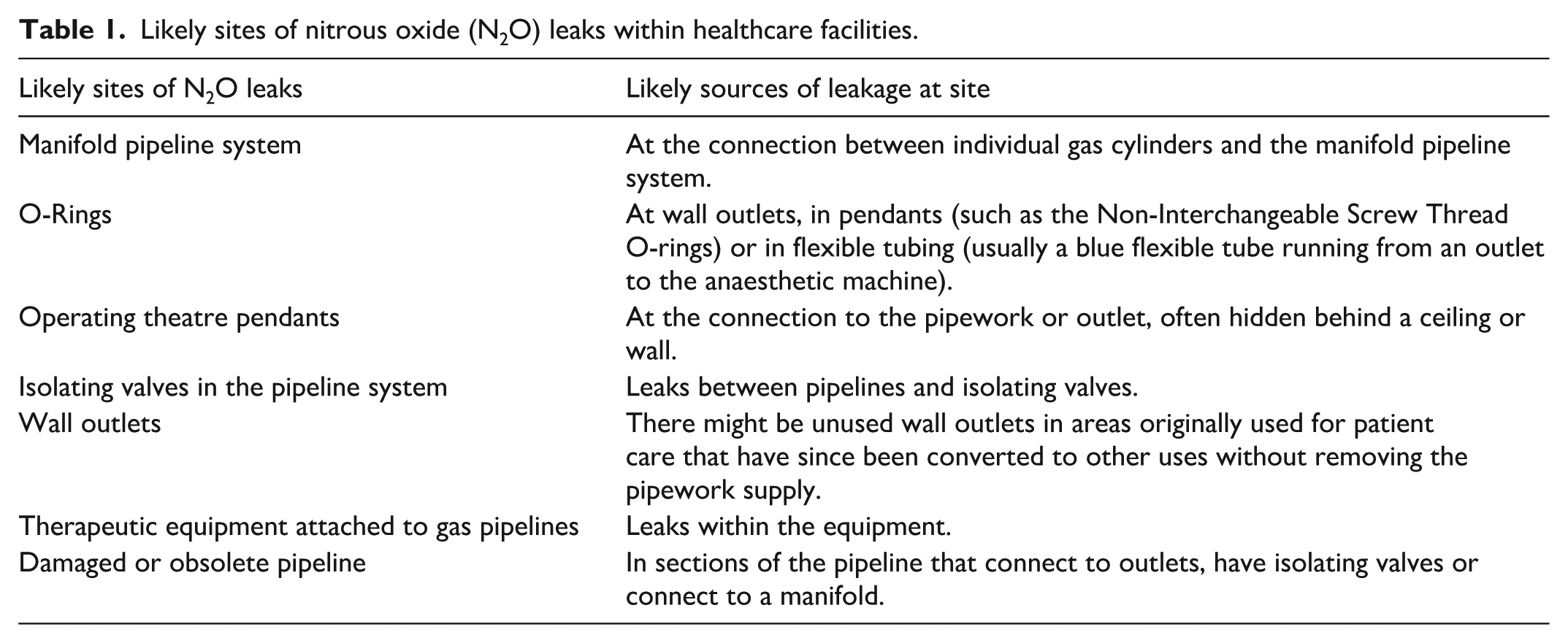
Leaks can occur along the N2O infrastructure of healthcare facilities (Table 1) with increasing facility age and inadequate maintenance schedules likely to increase the risk of leaks. While leaks from the manifold-pipeline system (the central pipe fitting which connects multiple gas cylinders to their points of use throughout the healthcare facility) appear to be more common, leaks can occur at other locations, including at wall outlets or at the point of clinical administration, such as N2O cylinders left open when attached to an anaesthetic machine.
Likely sites of nitrous oxide (N2O) leaks within healthcare facilities.
Detecting N2O leaks in a healthcare facility
The following initial steps are recommended in advance of attempting to detect leaks, to obtain an overview of the existing N2O infrastructure and history of supply:
1. Engage with the healthcare facility engineering department and/or facility manager to obtain a servicing schedule for the N2O pipeline and an up-to-date pipeline infrastructure map to help identify each outlet.
2. Clarify whether the healthcare facility engineering department does the servicing or whether they outsource this work to an external contractor. If external, confirm that the contracted servicing agency adequately tests for leaks, and identify the testing method(s) being used.
3. Obtain N2O purchasing data from the healthcare facility or directly from the supply company with as much detail as possible, such as cylinder size and weight and volume of N2O.
While it is necessary to have purchasing data only for the Discrepancy Method (described below), displaying purchasing data graphically by amount of N2O purchased over time (e.g. per month or year) can help identify the likelihood of leaks from changes in purchasing patterns (adjusting for any trends or cycles in clinical administration).
When detecting N2O leaks in healthcare facilities, it is essential to take a multidisciplinary approach by engaging a wide range of staff members throughout the process, including representatives from engineering and infrastructure, bioengineering, pharmacy, administration, procurement, anaesthesia, midwifery and obstetrics, paediatrics, emergency services, clinical governance, sustainability, safety and quality and others.
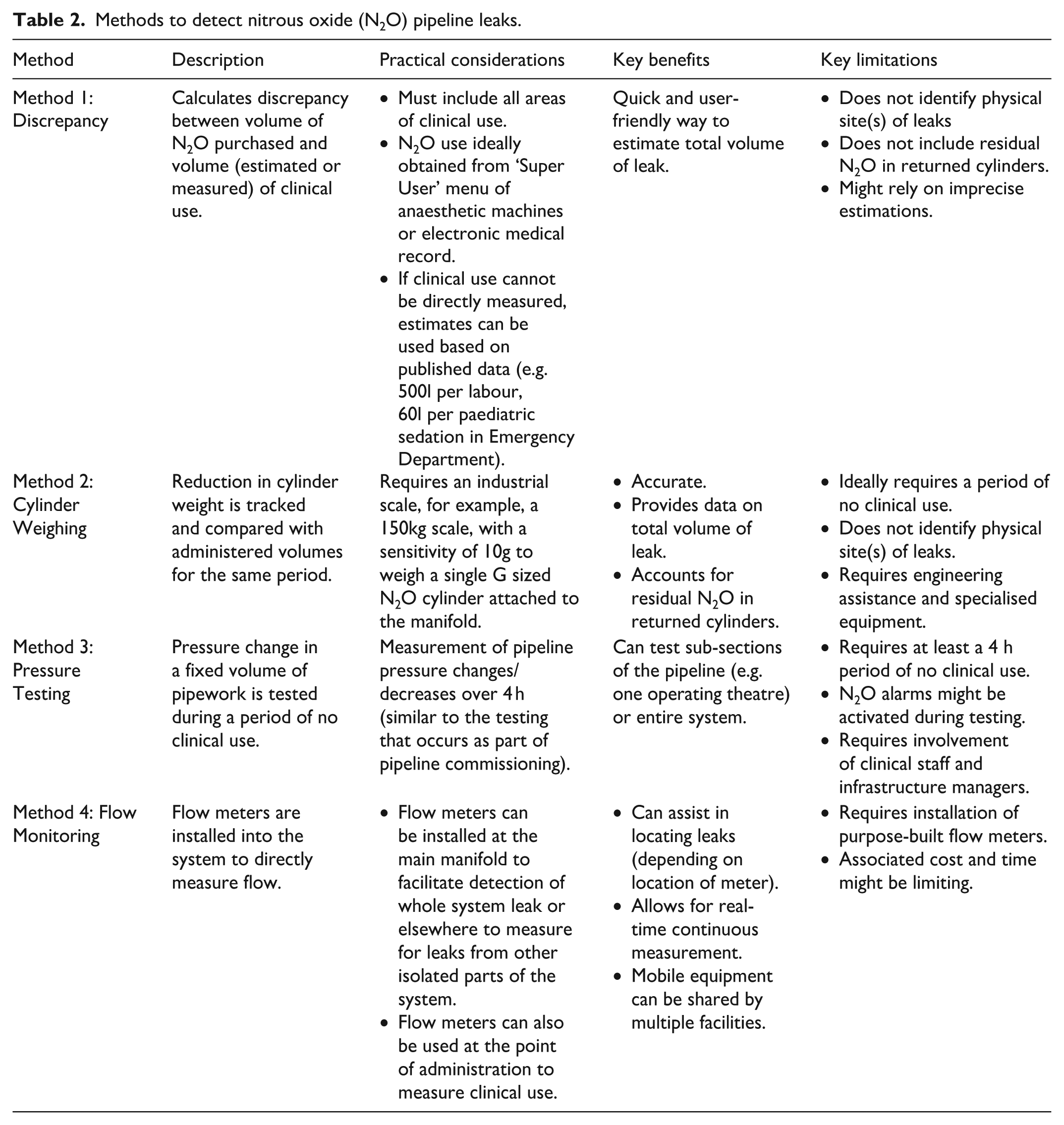
Four methods to detect N2O pipeline leaks have been described in the literature. These methods are summarised below and in Table 2 with further detailed descriptions found in the 2024 Guide. 16
Methods to detect nitrous oxide (N2O) pipeline leaks.
Discrepancy Method
The Discrepancy Method was developed by the Nitrous Oxide Project in the United Kingdom. 4 It calculates the difference between purchased amounts and clinically administered amounts of N2O, with discrepancy indicating a leak. It is a relatively quick and user-friendly method to indicate whether a leak is present.
Clinical administration amounts may be obtained by interrogating anaesthesia workstations. If this is not possible then estimations of clinical use, whilst likely less precise, have been used in the literature. 19 Discrepancies greater than 15% might indicate the existence of a leak (or multiple leaks) in the N2O delivery infrastructure.
Other limitations of this method are that the resulting leak estimates do not take into account residual N2O in manifold cylinders when they are returned to the gas suppliers, and that physical site(s) of leaks are not identifiable without a subsequent leak site detection process.
Cylinder Weighing Method
The Cylinder Weighing Method was developed at the Alfred Hospital, Melbourne, in 2022. 8 It detects N2O leaks via two similar methods: (a) weighing a manifold cylinder supplying N2O to determine depletion during a period when no N2O is administered, for example, overnight; or (b) weighing a manifold cylinder over a set time period when N2O is being administered and calculating the discrepancy between measured (via weight) cylinder depletion and N2O administration data.
This method relies on the fact that a regulator at the manifold maintains a constant pressure in the N2O pipeline network, hence any leak will lead to cylinder depletion and reduction in weight. An industrial scale, for example a 150 kg scale with a sensitivity of 10 g, is required to weigh a single N2O cylinder attached to the manifold.
Like the Discrepancy Method, this method provides information on leaks across a facility rather than identifying the physical site(s) of leaks. However, unlike the Discrepancy Method it does not include residual N2O contained in cylinders in the leak estimates.
This method is ideally undertaken during a period of no N2O clinical administration, which might be difficult in healthcare settings where continuous access to N2O supply is required.
Pressure Testing Method
The Pressure Testing Method detects N2O leaks by measuring the pressure decrease in a fixed volume system during a period of no clinical administration, at constant temperature. During the test, the N2O supply is disconnected or isolated from the gas pipeline. Close consultation with clinical staff and infrastructure managers is required to plan and implement this testing method, as there is the potential for activation of low pressure N2O alarms. This method might need to be conducted out of hours, during a period of no clinical use for piped N2O, which might not be possible in healthcare settings where continuous access to N2O supply is required.
This method is based on a protocol developed in 2023 by the Green Theatres Project at the Fiona Stanley and Fremantle Hospitals in Western Australia. The full protocol is available on the website of the Green Theatres Project. 20
Using this method, individual departments or areas can be checked for leaks (e.g. checking one operating theatre at a time), or the entire N2O delivery system can be checked as a system.
The suggested testing time is at least 4 h for each location being examined. An anaesthetic machine with a digital readout of N2O pipeline pressure can be used to measure the system pressure during the test.
Flow Monitoring Method
The Flow Monitoring Method utilises purpose-built flow meters to assist in detecting both N2O leaks and/or the amount of N2O that is clinically administered (where anaesthetic machine records are not available). This method was developed by Wong and coauthors at Sunshine Hospital, Melbourne and subsequently adapted and implemented at the Sydney Children’s Hospital Network and the Royal Women’s Hospital, Melbourne.19,21
The flow monitoring method can be used to measure flow at any point, from the supply of nitrous oxide at the manifold, to a clinical delivery device connected to a wall outlet at the point of care. Coriolis flow meters are used to directly measure N2O flow rates, with high accuracy, either for the entire facility or for isolated areas. 22
By installing a purpose-built flow meter at the point of the N2O supply infrastructure (e.g. at the central cylinder manifold) N2O supply can be measured, which might reflect supply more accurately than procurement data.
Clinical administration of N2O can also be measured by installing a purpose-built flow meter at the point of N2O clinical administration (i.e. wall outlets). The use of a threaded stainless steel sleeve enables the leakproof attachment of the N2O flow meter to N2O piping. Data obtained are used to accurately assess supply and clinical administration, and leaks can then be calculated using the Discrepancy Method.
The Flow Monitoring Method can be used to provide real-time, continuous measurement and, depending on the location of the flow meter, can also be used to locate leaks. It also has the potential to provide high-precision leak estimates (depending on the sensitivity of the flow meter). Given that the equipment is mobile, a single flow meter can be used across multiple facilities. Alternatively, permanent installation of leak detection equipment can be considered, to assist subsequent identification of leaks in real time.
Recommended next steps
Once a healthcare facility has identified the presence of a leak, using one of the four methods described, it is recommended to undertake a cost–benefit analysis to determine the best approach for a facility to reduce waste from N2O leakage. This could include:
Complete decommissioning of existing N2O pipelines;
Minimising N2O pipelines to supply only areas with a high-volume need (e.g. birthing suites);
Use of portable cylinders to supply N2O at the point of care where possible;
Avoiding installation of new N2O pipelines;
Avoiding the use of N2O where there is no impact on patient care.
As part of any cost–benefit analysis, consideration should be given to how to incorporate the environmental cost of greenhouse gas emissions into the analysis as well as the cost of routine testing and servicing. These costs should be communicated clearly to all staff who procure, store and use N2O. The preferences of health practitioners and user groups most likely to require continued use of N2O—such as maternity staff and patients—should also be considered before implementing any major changes to N2O infrastructure.
In considering next steps, it is important to collaborate closely with engineering staff, facility management teams, and anaesthetic and other departments that administer N2O, to ensure clear roles and responsibilities for testing and reporting. Regular testing (every 3–6 months) will help detect new N2O leaks, allow for alternative leak detection methods to be tried and compared if needed and enable a better understanding of N2O use over time. Consultation and collaboration with the wider health workforce will also be important, including identifying cases of unnecessary or low-value use of N2O and education on appropriate use.
If zones in the healthcare facility are identified where no (or negligible amounts of) N2O is administered, consider whether the isolation valve for that zone could be switched off, effectively isolating these areas from the rest of the N2O infrastructure.
Healthcare organisations should also consider an organisational policy that outlines the recommended uses of N2O administration across their facilities. This could include appropriate indicators and a governance framework for monitoring and overseeing N2O use. To further drive changes in N2O administration patterns, the organisational policy would ideally encompass training of health practitioners, and implementation of sustainable procurement policies and reporting frameworks. Combining a whole-of-organisation approach of this kind with appropriate change communication and health workforce training would support tangible and sustained reductions in N2O administration while maintaining the quality and safety of care delivery.
Decommissioning pipelines
Where N2O supply is required, healthcare facilities should consider moving away from piped N2O and instead supplying N2O via cylinders at the point of clinical administration. This would enable decommissioning of the entire N2O pipeline infrastructure and the associated financial and environmental benefits.
Hospitals in the United States and the United Kingdom that have decommissioned their N2O pipelines and moved to point-of-care cylinders have achieved large reductions in their N2O purchasing and greenhouse gas emissions as a result.4,23
Before decommissioning N2O pipeline infrastructure, facilities should consider:
Existing anaesthetic machines might not have a yoke for N2O cylinders to connect to. In these cases a point-of-care cylinder on a mobile cart, fitted with a regulator and hosing with Sleeve Indexed Bayonet, can be used, or the machines can be retrofitted with a yoke. When purchasing new anaesthetic machines, models with a yoke for N2O cylinders should be sought if N2O is expected to be required;
Appropriate storage, access, and monitoring of use of portable N2O cylinders, in compliance with the applicable standards and guidelines;
Practicalities of transporting N2O cylinders to the point of clinical administration;
Advantages to patients, who may be able to move around the room more freely when administered N2O via a cylinder;
Development of a new protocol for portable cylinder ordering.
Last, healthcare facilities are encouraged to explore avenues to minimise residual N2O amounts in cylinders returned to suppliers, and to advocate to suppliers for solutions to address and avoid greenhouse gas emissions from venting—the practice of releasing unused N2O when cylinders are returned for refill.
Recent progress
Since publication of the Guide in 2024, a number of Australian hospitals have decommissioned their piped N2O infrastructure and moved to portable supply of N2O. 24 Hospitals with large birthing suites and paediatric hospitals face additional challenges in moving to portable N2O supply. While examples of major obstetric hospitals successfully decommissioning are awaited, The Children’s Hospital at Westmead moved to cylinder based supply of N2O in December 2025.
Conclusion
Evidence suggests that the current Australian Standards for maintenance of N2O infrastructure and pipelines in healthcare facilities are inadequate to detect leaks, and that as a result millions of litres of N2O, and unnecessary greenhouse gas emissions, are currently leaking from healthcare facility infrastructure before clinical administration. Detailed guidance was developed and is presented in the Guide to detect and reduce leaks from N2O in healthcare facilities, alongside case studies of hospitals from across Australia who have successfully applied these methodologies and implemented improvements. Acting to reduce N2O infrastructure leaks represents an important opportunity for healthcare facilities to substantially reduce their greenhouse gas emissions and associated financial costs with no impact on patient care—and a significant opportunity for the health system to show leadership in responding to the threat of climate change.
Footnotes
Author contributions
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.