
Abstract
Arterial catheters are commonly inserted for intraoperative monitoring but are known to cause complications. We analysed all cases of arterial catheter complications and incidents related to arterial line monitoring reported to webAIRS. Anaesthetists voluntarily reported cases between 2009 and 2023. Included incidents met keyword search criteria and involved the insertion and presence of an arterial catheter, covering complications relating to the accuracy of arterial blood pressure readings, equipment or monitoring malfunction or human error related to equipment usage. Our aim was to promote awareness of both common and rare complications of arterial lines. Of the 10,518 incidents, 53 incidents met criteria, with 54 events described. Twenty-seven (50%) incidents were related to equipment failure, 17 (31%) compromised flow, five (9%) nerve injury, two (4%) medication error, one (2%) injury to skin, one (2%) infection and one (2%) inability to place an arterial catheter. The most common equipment problem was related to inappropriate transducer height causing inaccurate readings. No harm occurred in 16 (29.5%) of the patients, mild harm in 25 (46%), moderate harm in 10 (18.5%), severe harm in two (4%) and death in one (2%). Clinician vigilance is critical in the preparation, insertion and monitoring of arterial catheters, to allow the detection of problems and prevention of patient harm.
Keywords
Introduction
Arterial catheters are regularly inserted for continuous haemodynamic monitoring and arterial blood sampling in the perioperative and critical care setting. Arterial catheterisation is generally safe and well tolerated by patients. 1 However, the consequences of complications can range from no harm to severe harm.2,3 Temporary occlusion of blood flow, infection, haematoma and injury to surrounding structures are known complications of arterial catheter placement. 2 The need for placement of arterial catheters should be carefully weighed between clinical benefit and risk of complications. 3
A systematic review of 78 studies and 19,615 arterial catheterisations by Scheer et al 3 reported serious complication rates of less than 1% at all sites. Thrombotic occlusion was the most common complication at all sites, with radial and dorsalis pedis arteries most prone to thrombosis. The rate of temporary occlusion at radial arterial catheters was as high as 20% while the rate of occlusion at femoral arterial catheters was approximately 1.5%. 3 Human error and severe harm might also occur in relation to the pressurised intravenous fluids that are connected to intra-arterial catheters for pressure monitoring. 3 Nerve injury might occur due to direct trauma from needle insertion. 4
We analysed all cases of arterial catheter complications and incidents related to arterial line monitoring that were reported to the web-based anaesthetic incident reporting system (webAIRS) between 9 October 2009 and 23 May 2023.
Methods
WebAIRS is a self-reporting web-based anaesthetic incident reporting system from the Australian and New Zealand Tripartite Data Committee (ANZTADC). This voluntary and de-identified reporting system is used to collect, analyse and disseminate data on anaesthetic incidents related to the safety and quality of anaesthesia in Australia and New Zealand. These clinical incidents range from difficult cases, near misses and workload issues, to serious cases of patient harm and death. Denominator data are not provided by all registered hospitals and the voluntary nature of reporting of numerator data precludes analysis of frequency of outcomes and absolute risk calculations. Previous publications have described the process of data collection, management and analysis of webAIRS data and this is presented again here.5–7 Detailed information regarding the data entered and the incident reporting process can be found on the webAIRS website. 8
The de-identified data follows the National Health and Medical Research Council recommendations for quality assurance data, and the webAIRS data management process has undergone ethical assessment (HREC/11/QRBW/311; HREC/12/NEPEAN/18; MEC/09/17/EXP).
The study assessed all incidents related to complications arising from arterial catheter placement and monitoring reported via webAIRS, from the database’s inception on 9 October 2009 to 23 May 2023. An administration officer or data analyst from ANZTADC removes duplicate, test or empty records as part of the routine data cleaning process. The narratives relating to the incidents in the cleaned database were searched for the term/fragments ‘arterial’ or ‘art’ and contained the term/fragments ‘line, catheter’, or whether it was recorded that an arterial catheter had been inserted in the monitoring section of the incident report. These reports were read by VMT, VAE and MDC and screened according to inclusion and exclusion criteria agreed upon by all the authors.
The inclusion criteria were: insertion and presence of an arterial catheter, inaccuracies in invasive blood pressure readings, equipment or monitoring malfunction, human error related to use of equipment, potential or actual clinical injury, ischaemia, or pain caused by the arterial line system. Incidents were excluded if they were related to the inadvertent catheterisation of an artery when venous cannulation was intended, when the incident was not directly related to the arterial catheter, or if the incident was related to a pulmonary arterial catheter. Severity of patient complications was classified according to the Agency for Healthcare Research and Quality Harm Scale V1.2 definitions. 9 Severity was classified as: no harm, mild harm, moderate harm, severe harm, death.
In an iterative process, VMT read the narrative entry of each incident, applying categorisation which was agreed upon with VAE and MDC. The categorisation of incidents was refined as review of the narratives proceeded. Each incident was able to be assigned to more than one category where multiple events occurred. The final overarching categories included: equipment failure, compromised flow, nerve injury, medication error, injury to skin, infection, and inability to place arterial catheter. Compromised flow resulted in clinically diagnosed hypoperfusion, detected via either a dampened arterial trace or clinical signs in the distal limb. The ability to draw conclusions was limited to the information provided in the narrative by the entering clinician. The frequency with which each category was reported was identified using Structured Query Language (SQL) of the initial categorisation and presented as number (percentage) of the total number of arterial catheter reports. We calculated the proportion of overall incidents in each category, with the numerator, the number of incidents meeting inclusion criteria, and the denominator, the overall number of incidents in the webAIRS database, at the time of arterial catheter incident selection. Some incidents included in this analysis are likely to have been included in previous webAIRS publications.5–7
Procedure characteristics included: the urgency of the case (elective or emergency), the time of day of the incident (08:00–18:00 h, 18:00–22:00 h, 22:00-07:59 h). Patient characteristics included: age in years, body mass index (BMI) according to the World Health Organization classification, and the American Society of Anesthesiologists physical status (ASA PS) score of 1–5. 10 Clinician characteristics included: seniority of the clinician making the entry (specialist anaesthetist, post-Fellowship anaesthetist, trainee or other).
Results
A total of 10,518 clinical incidents were reported to webAIRS from October 2009 to May 2023. Applying the search terms resulted in 264 incidents and, of those, 53 incidents met inclusion and exclusion criteria (see Figure 1). One incident had two different arterial catheter complications, resulting in 54 total events. Of the final 53 incidents, 33 (62.3%) were elective cases and 19 (35.8%) were emergency cases, with one case unspecified (1.9%). Forty-three (81.1%) arterial catheterisations were performed by specialist anaesthetists, one (1.9%) was performed by a post-Fellowship anaesthetist, five (9.4%) were performed by trainees and four (7.6%) were not specified or ‘other’. Forty-one (77.4%) cases occurred between the hours of 08:00 and 18:00 with 41 (77.4%) clinicians on duty for less than 10 hours. Of the patients cared for, 27 (50.9%) were male, 24 (45.3%) were in the age category 60–79 years and two were aged under 17 years. Ten (18.9%) had a BMI >30 kg/m2 (with 10 BMI missing). Thirty-six (67.9%) of the patients had an ASA PS score >3 (with one not specified).
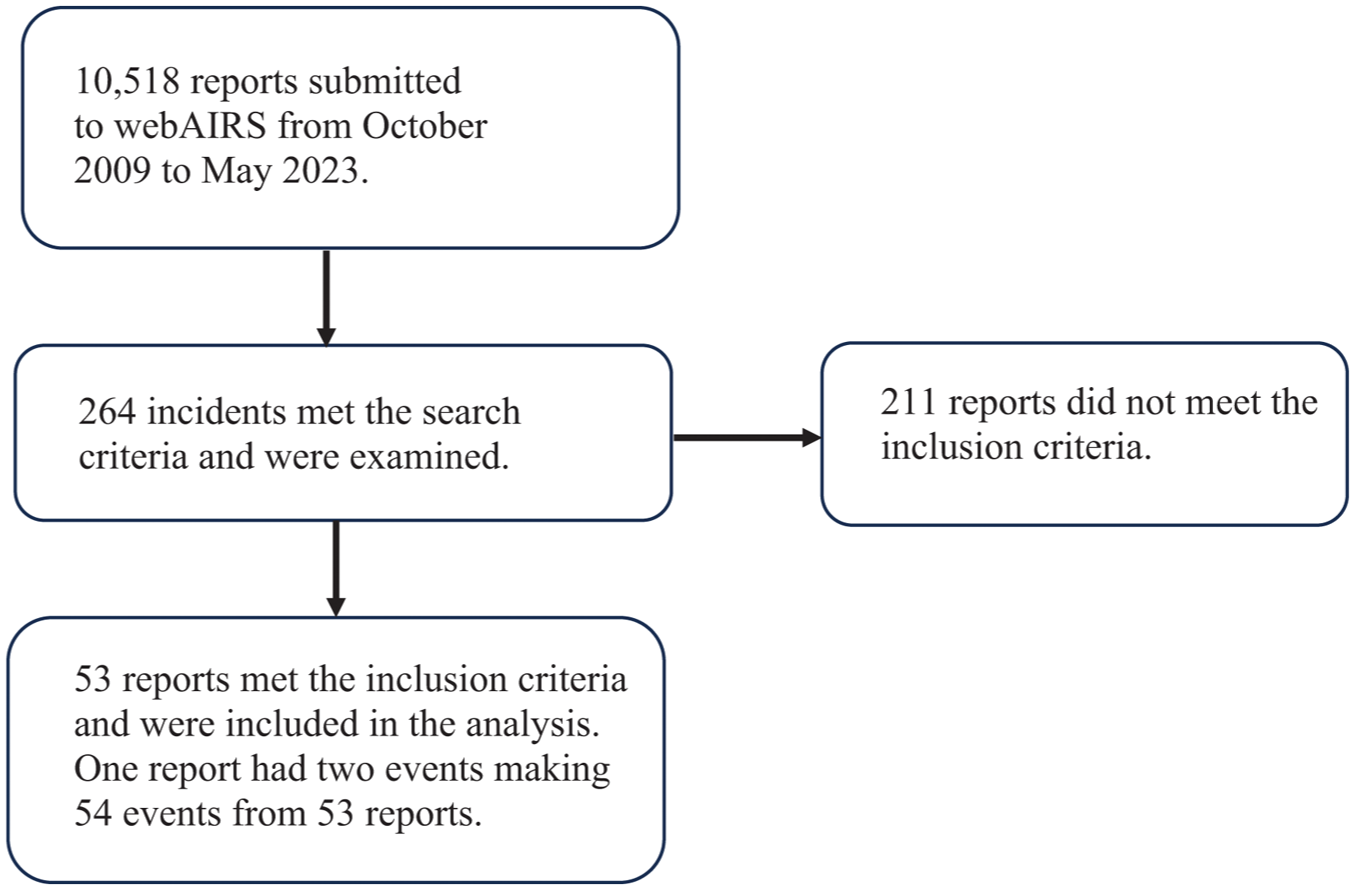
Flow diagram to identify webAIRS incident reports involving arterial catheters.
Table 1 shows the overarching categorisation of incidents. The largest category was equipment failure, with 27 (50%) incidents detailed in Table 2. Four incidents reported issues involving the guidewire and three incidents involved the catheter itself. In four incidents, parts of, or the entirety of the guidewire or catheter were retained in the artery and three incidents required vascular intervention (Table 2). Air was found within the arterial line tubing in two of the cases, one of which was associated with an air embolism that resulted in the patient having a severe stroke and death.
Categorisation of 54 events reported to webAIRS related to intra-arterial catheterisation.
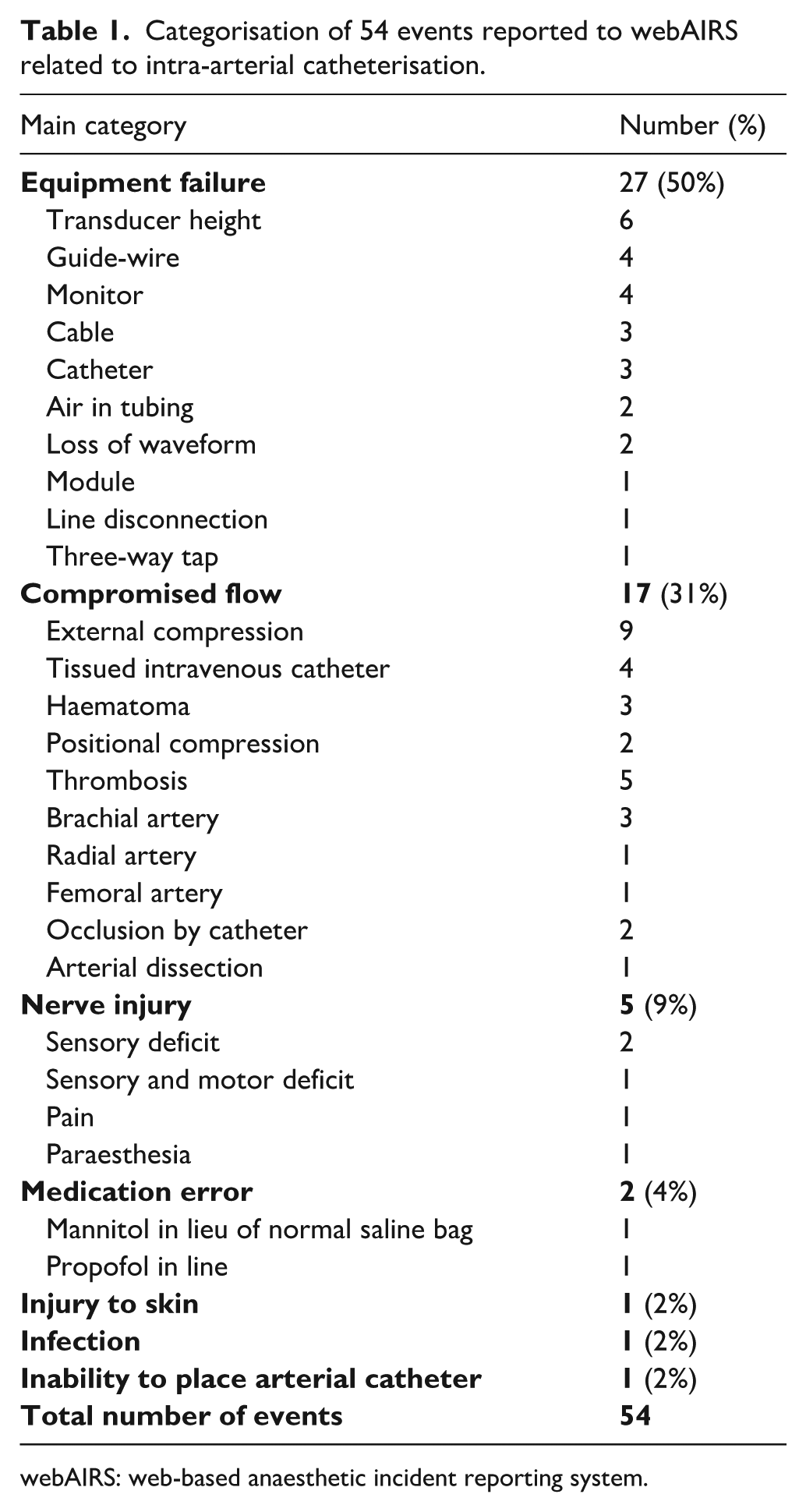
webAIRS: web-based anaesthetic incident reporting system.
Equipment failure events reported.
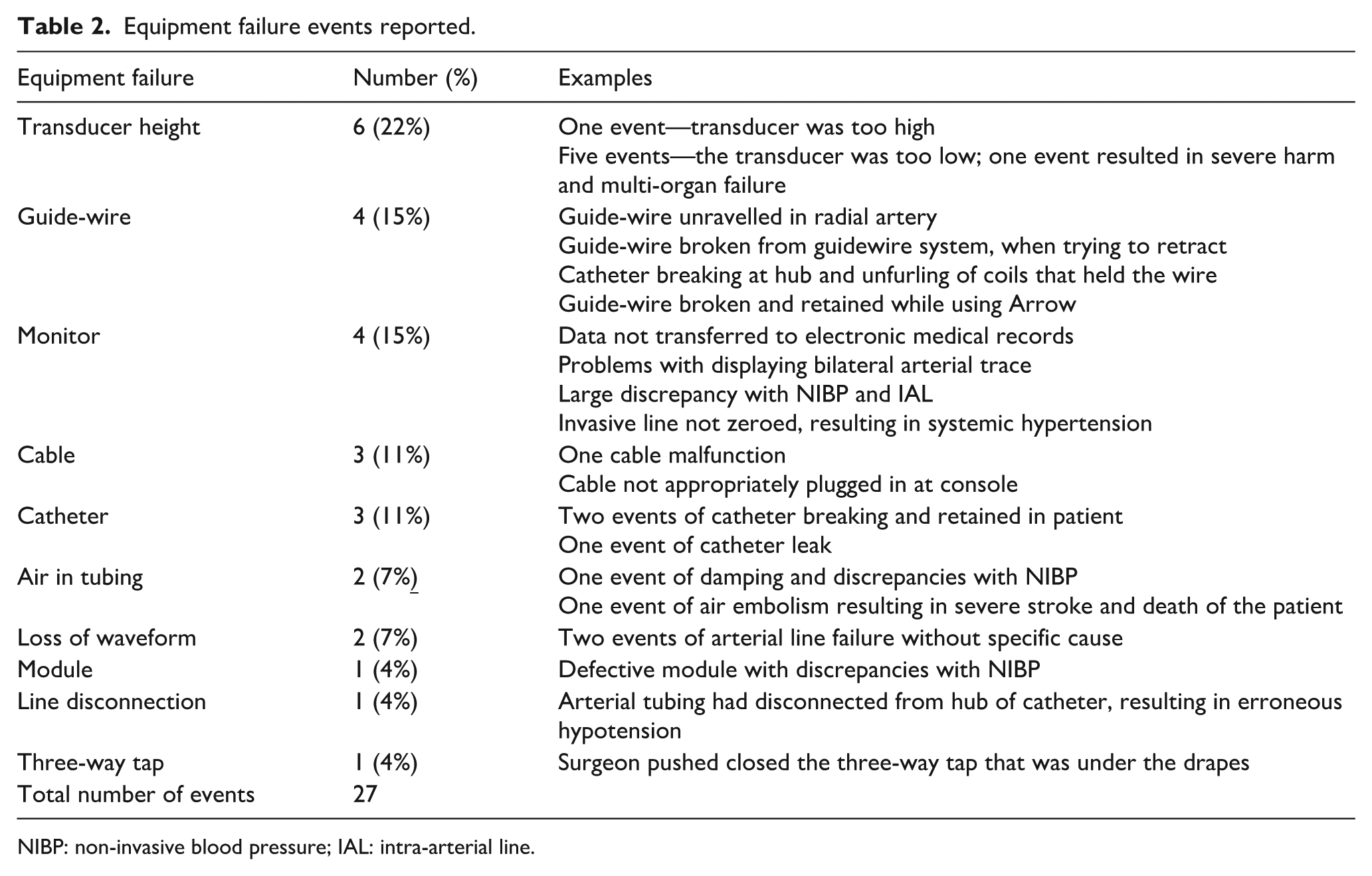
NIBP: non-invasive blood pressure; IAL: intra-arterial line.
The second largest main category was ‘Compromised flow’, with 17 (31%) incidents (Table 3). All cases within this category resulted in some degree of harm to the patient, ranging from mild harm to moderate harm. External compression (n = 9, 53%) accounted for the greatest number of reported cases, four of which were due to compression of the artery from fluid extravasation from a neighbouring intravenous line. In three cases, external compression was caused by haematoma, while two cases were caused by changes in positioning during surgery. All cases of external compression were associated with a dampened or impaired arterial trace, and/or signs of hypoperfusion. An arterial catheter in situ might have contributed to the restriction in blood flow. Two cases of compromised flow were caused by occlusion of the arterial catheter. Nerve injury accounted for five of the complications: two cases of postoperative sensory deficit, one case of both sensory deficit and motor weakness, one case of pain and one case of paraesthesia.
Compromised flow events reported.
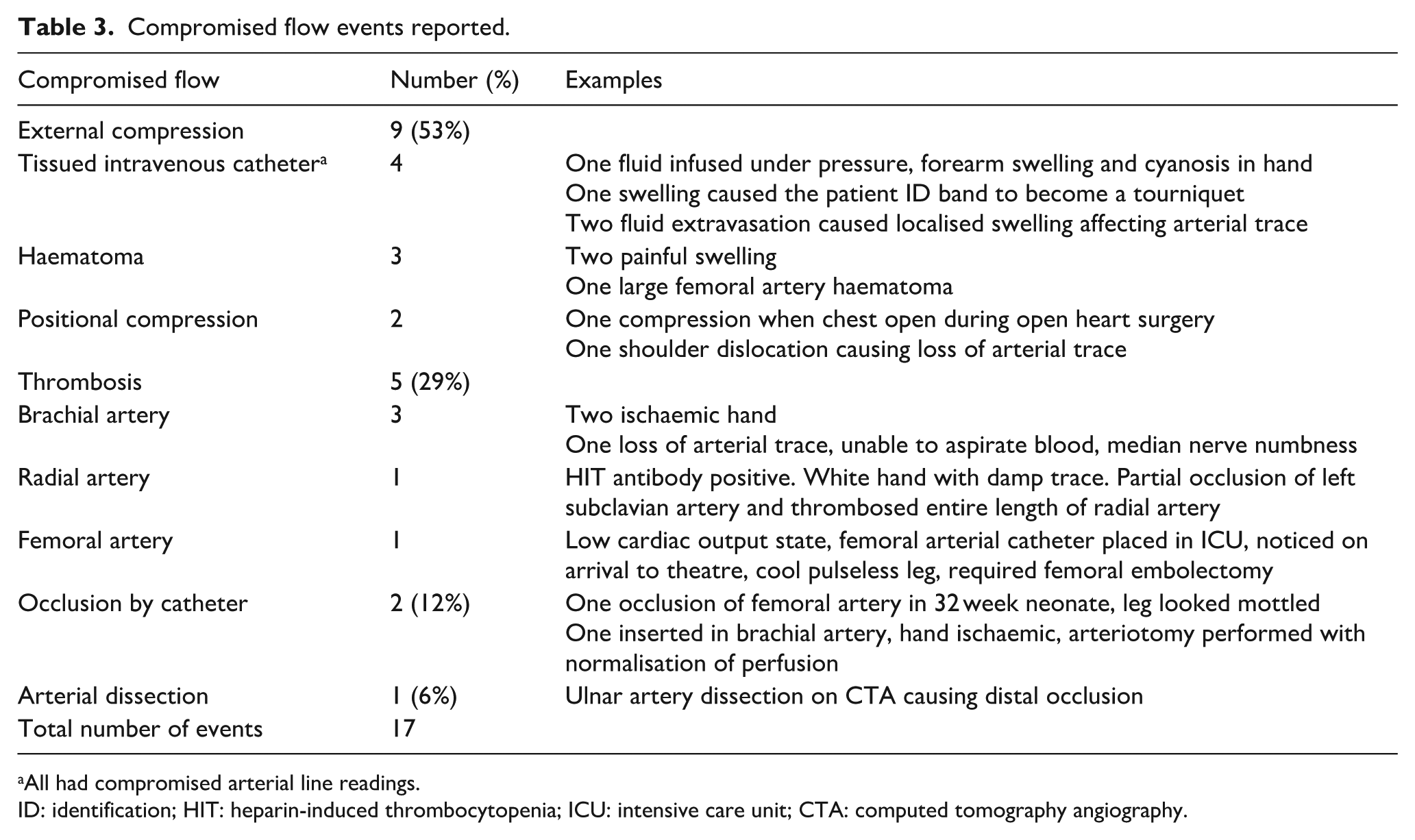
All had compromised arterial line readings.
ID: identification; HIT: heparin-induced thrombocytopenia; ICU: intensive care unit; CTA: computed tomography angiography.
There were two cases which involved medication error. In one, a 500 ml bag of mannitol was erroneously used in lieu of a 500 ml normal saline bag. In another case, propofol was inadvertently found to have been injected into the arterial line tubing. Neither case resulted in patient harm. There was one report of skin injury from peeling of the superficial layer of skin at the time of dressing removal. There was one report of infection that required a flexor tendon sheath exploration and intravenous antibiotics, and one event where the anaesthetist was unable to place an arterial catheter pre-induction and the patient suffered a post-induction arrest. The majority of events (75%) caused no harm (16, 29.5%) or mild harm (25, 46%) to the patient. Twenty-five percent of events had moderate harm (10, 18.5%), severe harm (2, 4%) or death (1, 2%).
Discussion
We report 54 perioperative events among 53 incidents reported to webAIRS involving arterial catheters, with the majority of events resulting in no harm or mild harm to the patient. There were two cases where the patient was subject to severe harm and one event where the arterial line complication was closely associated with the death of a patient. The reported incidents were more likely to occur in ASA PS >3 patients, reflecting the increased need for arterial catheter insertion in this higher risk patient group. Despite the widespread use of arterial catheters in the perioperative and intensive care unit settings, complications from arterial catheters accounted for only 0.5% of all incidents reported to webAIRS. In contrast to the existing literature, we report cases restricted to perioperative care specific to Australia and New Zealand, and in the context of modern equipment and practice.11–14
While many previous publications have focused on arterial catheterisation causing direct injury to the patient, 15 we describe equipment problems as the most frequent incident related to arterial catheters reported to webAIRS. Most of the equipment issues resulted in an inability to correctly produce a reliable blood pressure reading. The most common issue was transducer misplacement, resulting in erroneous blood pressure readings. Most cases of transducer misplacement resulted in no harm to the patient. However, one incident of transducer height error led to severe harm from unrecognised prolonged hypotension resulting in multi-organ failure in an unwell and high-risk patient. Other issues identified included the inability to appropriately document blood pressure readings onto patient records. Equipment failure without direct harm can still distract the anaesthetist from other clinical priorities. Vigilance in checking transducer location and correlation with non-invasive blood pressure measurement is recommended to identify misleading measurements.
Guide-wire complications accounted for the second most common category of equipment failure. There are a range of products and techniques available for inserting arterial catheters. Since the 1970s, publications reporting arterial catheter complications have described surgical arterial cutdown, 11 catheter-over-needle12–14,16 and the use of a guide-wire (Seldinger technique). 17 Catheter insertion kits that have an integrated wire are available. 18 While use of an integrated wire system is increasingly popular, two patients in our cohort had a part of the wire retained and one patient required surgical intervention. Clinicians should be aware of the risk of retained wire and potential intimal damage by the wire itself.
One incident related to arterial line mismanagement resulted in a fatal outcome for the patient. The incident describes a retrograde arterial air embolus that caused a stroke in the intensive care unit (ICU). The patient was sitting upright in a chair while a staff member was troubleshooting the arterial line, and the patient experienced sudden onset dysarthria, hemiparesis and facial droop. It was noted that the pressure bag was empty, and air was present in the arterial line tubing. Computed tomography of the brain showed reduced perfusion. Hyperbaric treatment was instituted, but further deterioration occurred due to haemorrhagic conversion. The patient concurrently suffered from further complications and passed away despite medical and surgical management. Experimentally, it has been shown that 2 ml of air injected into the radial artery can result in a retrograde passage into the vertebral system and the brain. 19 Manual flushing with >1 ml/s produces a retrograde flow into the proximal axillary artery. In the upright position, gas can travel upwards from the aortic arch into the brain-supplying arteries, resulting in fatal air embolism. 19
Compromised distal tissue perfusion is a feared complication of arterial catheterisation, with published case reports of severe harm.1,3 A study in the Australian context identified extensive arterial thrombus using duplex ultrasound in 15% of patients with short-term perioperative arterial catheterisation. 1 Despite thrombi with a mean length of 9.6 cm, there were minimal reported symptoms, and no medical or surgical intervention was required. 1 Catheterisation of brachial arteries is generally not recommended owing to the risk of median nerve injury and the absence of collateral flow, with consequent risk of ischaemia of the forearm and hand.20–22 Out of the five cases of thrombosis, three involved thrombosis of the brachial artery. All three cases were catheterised in the brachial artery after failed access to the radial artery and had either clinically detectable ischaemia or altered sensation to the distal limb. There was also one incident that reported partial occlusion of the left subclavian artery and thrombosis in the entire length of the radial artery on vascular ultrasound after catheterisation of the radial artery. Staff noticed a white hand and damped arterial trace. The patient was heparin-induced thrombocytopenia antibody positive and was treated with bivalirudin and then warfarin. A week later ultrasound showed normal flow in the subclavian and radial arteries. Physical access to and direct visual observation of arterial catheters is frequently prevented by patient positioning and opaque surgical drapes. Our results highlight that a damped or unreliable invasive blood pressure waveform requires further investigation to allow early detection and prevention of potential patient harm.
The biggest risk factor for thrombosis from arterial catheterisation relates to the proportion of the arterial lumen taken up by the catheter. 3 The more space occupied, the higher the risk of thrombosis. Other risk factors include: the patient being female (likely owing to narrower arteries), low cardiac output states, multiple catheterisations, the catheter being in situ for more than 72 h and haematoma at the site of puncture. 3 It is important to note that thrombosis can occur following the removal of the arterial catheter. 3
Spencer et al 23 proposed the Safe Insertion of Arterial Catheters protocol, applying a systematic approach to arterial catheterisation, with a focus on improving insertion practices, reducing complications and increasing patient safety. The protocol recommends consistent use of ultrasound-guided arterial catheter insertions to optimise the choice of insertion location and the actual catheterisation. 23 Ultrasound-guided insertions might help reduce some of the risk factors of thrombosis noted above, such as reducing repeated puncture and haematoma.
In our review, we report one case of drug error where mannitol was used instead of the intended 0.9% normal saline as the arterial line flush solution. No harm to the patient was reported; however, various case reports have documented detrimental consequences of misidentified arterial line flush fluids. In 2008, the UK National Patient Safety Agency issued a Rapid Response Report concerning problems with infusions and sampling from arterial lines. 24 They conducted a literature search up to 2008 which identified 84 incidents where there were misidentifications of arterial line infusions, two of which resulted in death. The use of glucose 5% fluid instead of 0.9% normal saline consisted of the majority of the misidentifications; however, they reported 21 different types of fluids that were substituted. One of the deaths was a result of severe hypoglycaemia and neuroglycopenic brain injury from insulin being titrated to samples taken from the arterial line containing 5% glucose infusion bag instead of 0.9% saline.24,25 A further contributing factor to note is that the fluid is placed inside an opaque or semi-opaque pressure sleeve that conceals the identifying label of the fluid. 25 We encourage workflows that include double-checking of all fluids and medications administered to patients, for healthcare workers who manage arterial line preparation and monitoring. 24
Despite the widespread use of arterial catheters in the perioperative and ICU settings, adverse events from arterial cannulations have a low frequency of occurrence. 2 Complications from arterial catheters account for 0.5% of all incidents reported to webAIRS. Despite these low numbers, our study illustrates some rare adverse events from arterial catheters that can cause severe harm and even death to our patients. We hope to highlight these events to bring awareness, as well as encourage clinicians to remain vigilant during insertion and management of arterial catheters.
Limitations
Incident monitoring is a qualitative research technique particularly useful when problems are complex and multifactorial in causation. WebAIRS is an anonymous incident monitoring database where the information gathered does not provide a numerator or denominator and no inference of incidence can be made from these data. Selected contributing factors represent the subjective opinion of the reporter and relevant details reported are at the discretion of the reporter. We have limited information regarding the type of arterial catheter used or whether ultrasound was used to aid insertion. Further complications of arterial lines occurring post-discharge or late in ICU might not be identified by the managing anaesthetist.
Conclusion
We have described a series of complications of arterial catheterisation which occurred in the perioperative period. Anaesthetists can learn from the experiences of their peers that are well documented in this voluntary reporting system. Equipment problems were commonly reported. Clinician vigilance is critical in the preparation, insertion and monitoring of arterial catheters, to allow the detection of problems and prevention of patient harm.
Footnotes
Acknowledgements
The authors would like to thank ANZTADC for managing the collection, data cleaning and provision of the de-identified data which were used for analysis in this article. We also thank all the reporters who have shared their experience of events that have occurred during anaesthesia by submitting incident reports using the webAIRS incident reporting system.
Author contributions
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: ANZTADC is the Australian and New Zealand Tripartite Anaesthetic Data Committee, which is funded by the New Zealand Society of Anaesthetists, the Australian Society of Anaesthetists and the Australian and New Zealand College of Anaesthetists. ANZTADC funds and manages the webAIRS website and database. Otherwise, the authors above do not have any conflicts of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.