
Abstract
Electronic medical records (eMRs) could support perioperative outcomes registries, but the completeness of routinely collected data remains uncertain. This study evaluated the availability of perioperative data within a large Australian hospital eMR against the Perioperative Clinical Outcomes Registry Extended (PCOREx) dataset. A retrospective audit of all elective inpatient procedures involving anaesthetists at Westmead Hospital (Sydney, New South Wales) in June 2022 was performed. Records were reviewed in Cerner® PowerChart (Cerner Corporation, Kansas City, MO, USA) and completeness was defined as the presence of PCOREx variables across Baseline Risk, Intraoperative Risk, Process of Care, In-Hospital Outcomes and Post-Discharge Outcomes. A total of 405 patients met inclusion criteria. Overall completeness was 63%; excluding post-discharge variables, inpatient completeness was 77.5%. Demographic, procedural and intraoperative physiological data—mostly structured or automatically captured—were consistently recorded (>90%). Comorbidities, frailty indices, intraoperative temperature, and fluid balance were less complete (<50%). Post-discharge outcomes were recorded in only 7.9% of patients, limited to those who re-presented to hospital. Missingness reflected both structural gaps (absence of fields, siloed intensive care unit systems) and clinical behaviour (selective documentation, variable pathology ordering). While routine eMR data capture many perioperative variables, significant gaps remain, particularly for post-discharge outcomes and selectively documented fields. Mapping completeness within the Clinical Adoption Meta Model framework highlights barriers at system and clinical levels. Standardised data capture, linkage with external databases, and improved interoperability are needed to realise the potential of eMRs for perioperative outcomes registries.
Keywords
Introduction
As more and more inpatient medical record data become primarily electronic, a multitude of opportunities are becoming available for both retrospective and prospective research. Studies that use existing clinical data on a large scale are becoming much more feasible and can contribute to evidence-based medical practice as well as improve patient outcomes locally. In fact, the data now routinely collected in clinical practice may be leveraged to provide quality and standardised data to populate multi-hospital registries. To that end, the Perioperative Clinical Outcomes Registry (PCORE) initiated by the Australian and New Zealand College of Anaesthetists (ANZCA)1,2 is a national clinical quality registry in perioperative medicine. This can be expanded upon to include postoperative outcome data and thus form a more extensive registry that can potentially be used for research purposes.
At the institutional level, the electronic medical record (eMR) represents a primary vehicle for capturing perioperative data across all stages of the patient journey and for the generation of a hospital-specific local registry.
The overall goals of such a registry are:
(a) Provision of a reliable repository of data for use in both retrospective and prospective clinical research;
(b) Facilitating departmental-level Quality Assurance and Improvement projects;
(c) Generating data to provide individualised feedback to anaesthesia staff;
(d) Contribution to the national PCORE database.
Despite this potential, practical challenges remain. Reilly et al 3 conducted a survey of ANZCA Clinical Trials Network hospitals to gauge the potential use of perioperative medical record data in such research and quality assurance purposes. The survey generated 42 responses, representing six public hospitals across Australia. Between 19% and 85% of the predefined perioperative PCORE data domains were recorded electronically; however, the ability of the anaesthetic departments to export this data and leverage it for research and auditing purposes in an efficient way was as low as 13%. This highlights not only issues of accessibility but also heterogeneity of data types distributed across disparate systems with limited interoperability, for example free text versus structured fields, and ward-based versus intensive care unit (ICU) platforms. These challenges underscore the need to evaluate the completeness and accessibility of perioperative eMR data before it can reliably support registry development.
It is important to note that the term ‘completeness’ requires a formal definition. eMR data differ substantially from research data in terms of methods of collection, storage and structure; and it is also contextual, meaning that a record can be judged to be complete or incomplete depending upon the context in which the information therein was collected and its intended use. 4 There have been a number of studies looking at both the degree of completeness of eMR systems and, more broadly, nationally-based Electronic Health Records (EHRs) in the literature, all of which have specific definitions of data completeness.4–10 Weiskopf et al 4 specifically define four types of completeness:
Documentation completeness. The extent to which a medical record captures all clinical observations generated during a patient encounter.
Breadth completeness. The degree to which a record encompasses the full spectrum of data domains required to support secondary applications, such as clinical research, quality assurance or registry development.
Density completeness. The sufficiency of repeated data entries for a given clinical parameter over time, enabling longitudinal assessment and monitoring.
Predictive completeness. The adequacy of information contained within a record to support predictive modelling and the anticipation of future clinical events.
For the purpose of the current study, completeness was defined as the presence or absence of data from a predefined registry dataset encompassing routinely collected perioperative demographic and outcomes data. In alignment with the breadth completeness definition, as utilised in the studies of Wurster et al,9,10 this study aimed to evaluate the extent to which routinely collected eMR data fulfil the requirements of a standardised data collection framework in perioperative care. It was hypothesised that completeness would vary by category, with higher levels for automatically generated data (e.g. vital signs in the electronic anaesthetic record) compared with manually entered fields (e.g. free-text notes).
Method
This was a retrospective evaluation of completeness of a predefined set of perioperative data (PCORE Extended (PCOREx) dataset; Table 1) within the eMR of Westmead Hospital, which is a large teaching hospital and trauma centre in Western Sydney, New South Wales, Australia. Records from eligible elective inpatients during the month of June 2022 were accessed manually to serve as a representative snapshot of the eMR. The month of June was selected to be a reasonable sample as by this time the hospital had returned to a full complement of elective surgical caseload after restrictions imposed by the COVID-19 pandemic. The eMR system utilised was Cerner® PowerChart (Cerner Corporation, Kansas City, MO, USA), with the SurgiNet Anesthesia module used for perioperative charting.
Data overview for the Perioperative Clinical Outcomes Registry Extended dataset.
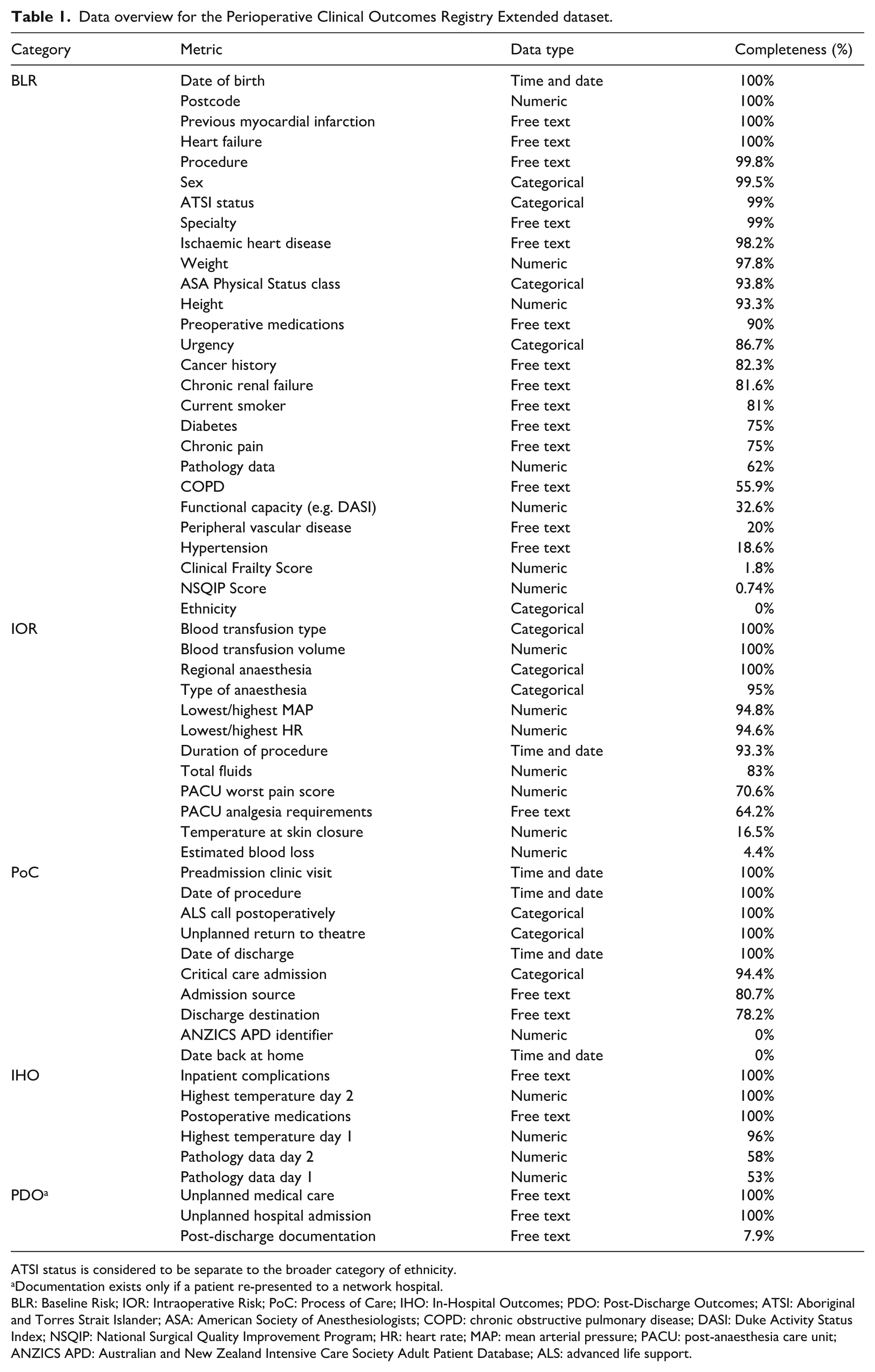
ATSI status is considered to be separate to the broader category of ethnicity.
Documentation exists only if a patient re-presented to a network hospital.
BLR: Baseline Risk; IOR: Intraoperative Risk; PoC: Process of Care; IHO: In-Hospital Outcomes; PDO: Post-Discharge Outcomes; ATSI: Aboriginal and Torres Strait Islander; ASA: American Society of Anesthesiologists; COPD: chronic obstructive pulmonary disease; DASI: Duke Activity Status Index; NSQIP: National Surgical Quality Improvement Program; HR: heart rate; MAP: mean arterial pressure; PACU: post-anaesthesia care unit; ANZICS APD: Australian and New Zealand Intensive Care Society Adult Patient Database; ALS: advanced life support.
Inclusion and exclusion criteria
All adult patients (⩾16 years) who had undergone an elective inpatient (i.e. with a planned overnight hospital admission) procedure with the involvement of an anaesthetist, including all non-cardiac surgery, and interventional endoscopic, neuroradiological, vascular and cardiology procedures, were eligible for inclusion. Patients who had undergone cardiac surgery, any other operation combined with cardiac surgery, or transplant surgery were excluded. These criteria are identical to the inclusion and exclusion criteria used for PCORE. 11
Defining data categories and types
Data outlined below were queried to determine whether the target information was available in the eMR, following the methodology of Wurster et al. 9 Additional data, such as number of days of admission at the time the snapshot was taken, were also collected and compared with the dates of any procedures. Partial, inconsistent or conflicting entries were classified as incomplete, reflecting the anticipated impact such data would have on registry reliability.
The data that were collected can be defined within the following categories: Baseline Risk (BLR); Intraoperative Risk (IOR); Process of Care (PoC); In-Hospital Outcomes (IHO); Post-Discharge Outcomes (PDO).
For each of the above categories of data, a multitude of data types were generally available. These may broadly be classified as structured and non-structured. For the present purpose, information on the type of data storage was also collected:
Time and date data;
Numeric data (e.g. patient vital signs, height, weight, biochemical pathology results, etc) (structured);
Categorical data (e.g. gender, yes/no data, American Society of Anesthesiologists Physical Status class, etc) (structured);
Free text/string data (non-structured).
The rationale for classifying data types was to facilitate identification of which pieces of data were more likely to be omitted from a patient’s medical record and might lead to some insights as to the reasons behind such an omission.
Definition of completeness
For the purposes of the present investigation, the term ‘completeness’ was directly related to the presence or absence of the items outlined in the PCOREx dataset (Table 1).
Data collection
The eMR for each of the eligible patients was manually accessed and interrogated for the requisite data in Table 1. All study data were collected and managed using a custom-built REDCap (Research Electronic Data Capture) data collection tool hosted at The University of Sydney.12,13
Data analysis
Results are presented as the proportion (%) of patients with complete data for each variable in the PCOREx dataset. Furthermore, the locations in the eMR of available information (for patients where this information was present) are also presented as a proportion. Within the Cerner eMR, the locations were defined to be: Anaesthesia Documentation, Clinical Documentation, Results Summary and the Medication Admission Record (MAR). No further statistical comparisons were made.
Ethics and dissemination
Ethical approval, including a waiver of individual patient consent, was sought and granted for this study from the Western Sydney Local Health District Human Research Ethics Committee (approval number QA-2207-01).
Results
A total of 405 patients were identified to meet the above outlined inclusion criteria in the designated period. For all 405 patients, access to their eMR was available, and data collection could be completed in all of these patients. The following data categories are hence presented: BLR, IOR, PoC, IHO, PDO, Overall, Data Types.
BLR and IOR
Completeness of BLR data showed considerable variation (Table 1). Demographic variables and key cardiac history were consistently recorded, with near-complete data across these fields. Procedural details and basic anthropometric measures were also captured at high rates. Figure 1 highlights the primary sources of BLR information within the eMR. The Anaesthetic Documentation, encompassing the preoperative assessment and anaesthetic record, served as the primary source of information. If the target information was absent, other areas of the eMR were examined in a sequential manner. Comorbidity-related fields demonstrated more variability, with several conditions and perioperative assessments recorded less consistently. Functional measures, frailty indices and structured risk assessment tools had the lowest levels of completion, with some fields rarely documented.
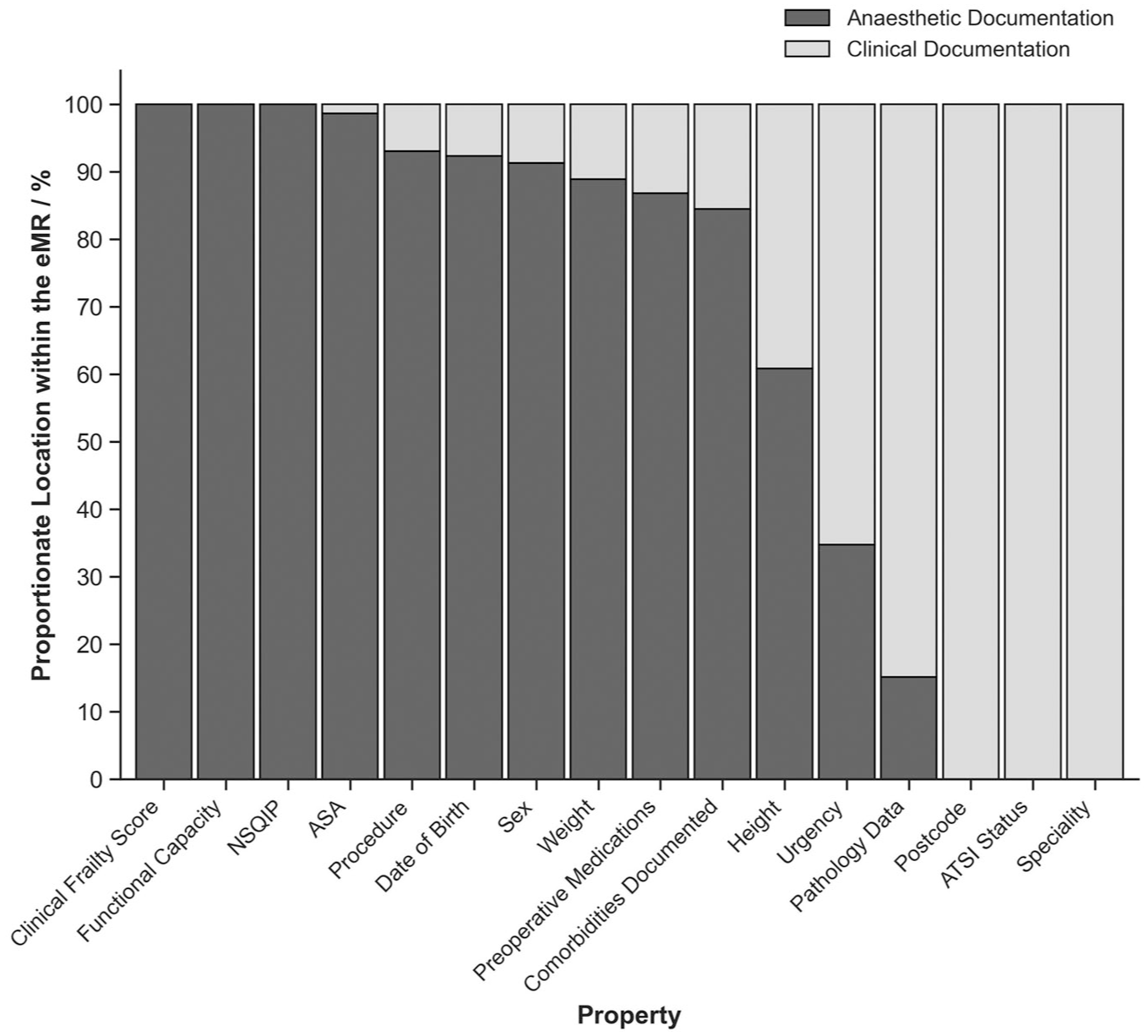
Location within the electronic medical record for the Baseline Risk data.
Within the IOR category, data completeness was highest for transfusion variables and anaesthetic techniques, which were consistently recorded across all cases (Table 1). Physiological measures and procedural details such as blood pressure, heart rate and duration of procedure were also captured at high levels. In comparison, fluid balance and post-anaesthesia care unit (PACU) observations were less consistently documented. Variables related to perioperative blood loss and temperature monitoring had the lowest completeness, with very limited data available.
PoC
Of the 405 patients, just over half (50.1%) attended the Pre-admission Clinic ahead of their elective surgery. Of these patients, 100% had their visit documented within the Anaesthetic Preoperative Assessment. The degrees of completeness of the various elements within the PoC category are displayed in Table 1. The distribution of locations within the eMR where each of the properties of the PoC dataset were recorded is presented in Figure 2. It must be noted that at the time of data acquisition, two of the 405 patients had not yet been discharged from the hospital following their surgery. Therefore, the percentage completeness of any discharge-related data within this category reflects a total of 403 patients.
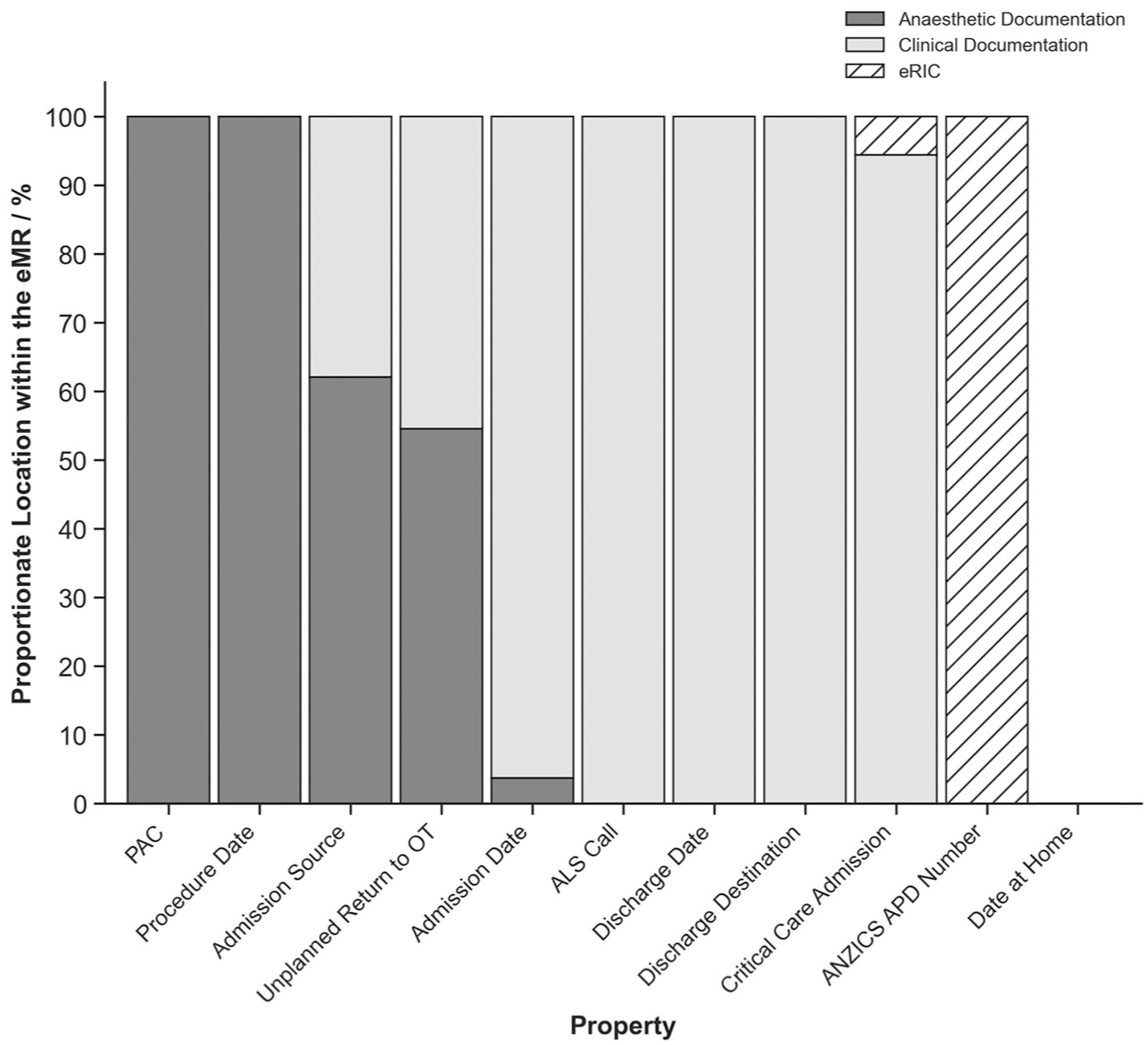
Locations of the Process of Care Data within the electronic medical record.
The Australian and New Zealand Intensive Care Society Adult Patient Database (ANZICS APD) Number is not part of the hospital’s eMR system, as it belongs to a separate database. The eMR in this study refers to data within the Cerner PowerChart, while patients admitted to the ICU had their clinical data entered into a different system called the Electronic Record for Intensive Care (eRIC, iMDSoft MetaVision, Tel Aviv, Israel), which has limited connectivity to the broader Cerner-based eMR. ICU patients had their ANZICS APD Number recorded with 100% completeness within eRIC.
IHO
Sixty-six (16%) patients included in this study experienced at least one inpatient complication, details of which were included within the clinical documentation with 100% completeness. The degree of completeness within this dataset is shown in Table 1.
With regard to temperature measurements, of the patients who were admitted for only one day, 92% had their Day 1 Temperature recorded. One hundred percent of patients who were admitted for more than one day had their Day 1 Temperature recorded. Of the patients who were admitted for only one day, 31% had recorded Day 1 Pathology data, whereas 74% of the patients who were admitted for more than one day had this information within their record.
PDO
Among the 403 individuals who were discharged from hospital, 32 (7.9%) were documented as having some form of post-discharge complication. Five (1.2%) had an unplanned review by a general practitioner (and subsequent re-presentation to the emergency department); 24 (5.6%) re-presented to the emergency department directly, 22 (5.5%) of whom were re-admitted to hospital. A further three (0.7%) patients experienced a complication documented and managed in a hospital-based outpatient clinic. At the time of data acquisition for this study, two patients remained as inpatients; therefore, documented PDO was present, with a 7.9% completion rate. However, those few patients had 100% completeness for the target metrics (Table 1). Post-discharge data were collected only if a patient re-presented to hospital or a hospital-based outpatient clinic.
Overall completeness
Across all categories for the PCOREx dataset, the Overall completeness was determined to be 63%. Given that current clinical documentation is not designed to collect post-discharge data routinely, if this category is omitted, the observed completeness rate for the remaining inpatient collected data was 77.5%. The individual breakdown of Overall completeness for each category is shown in Figure 3. Likewise, the Overall completeness for each data type is presented in Figure 4.
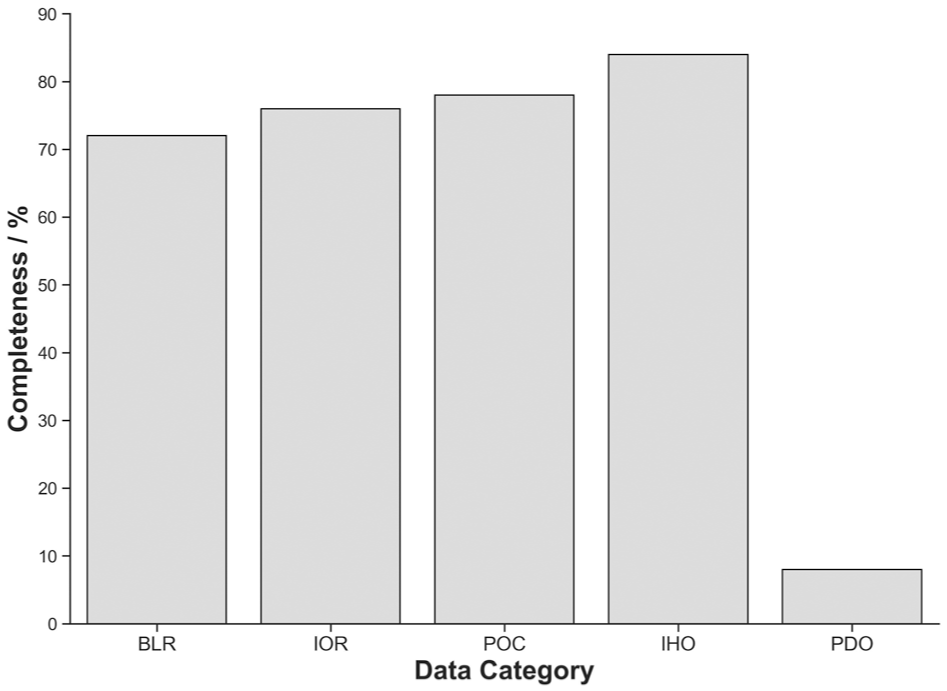
Overall completeness of the Perioperative Clinical Outcomes Registry Extended data categories.
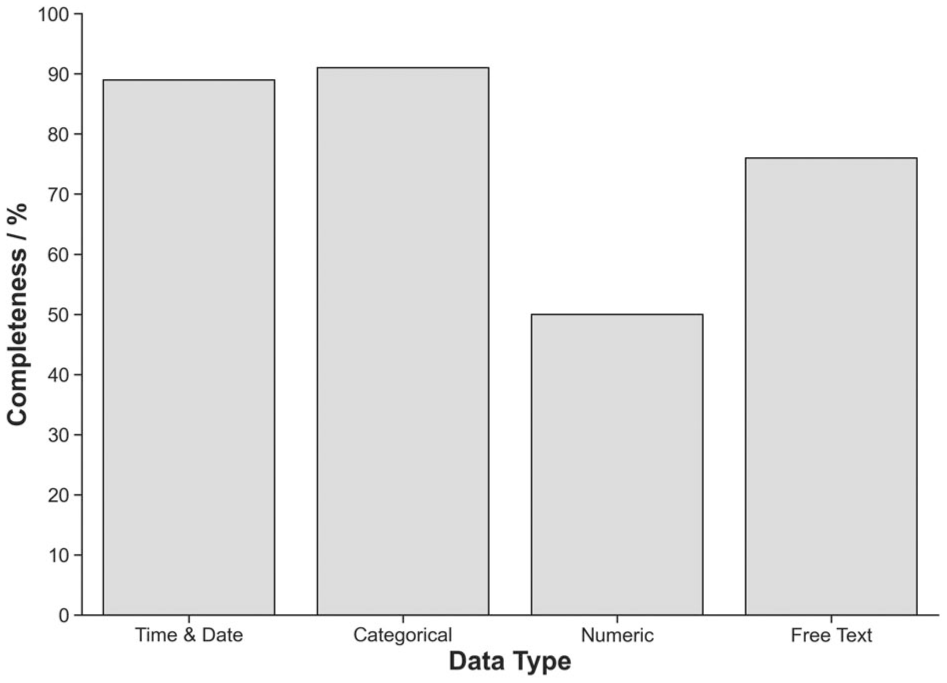
Completeness of Perioperative Clinical Outcomes Registry Extended data by data type.
Discussion
In this single-centre evaluation of perioperative data availability in the eMR, the overall degree of completeness across the inpatient component of the PCOREx data registry was 77.5%. The completeness of PDO was significantly lower (7.9%). These findings highlight the challenges of using routine clinical care data within a hospital’s eMR system as source data to populate a clinical outcomes registry. Where a formalised and dedicated registry has well-defined target data and an independent data-entry process, real world clinical data are considerably more heterogeneous. This heterogeneity is present in terms not only of data availability, but also of varied formatting. 14
This study examined whether existing eMR data can meet the requirements of a proposed standardised registry framework such as PCOREx. At the time of sampling in June 2022, local documentation practices had stabilised following the initial disruptions of the COVID-19 pandemic, and the PCOREx framework was already established. Since then, no major developments have occurred in the eMR system, and it is anticipated that a repeat sampling in 2025 would produce similar findings. Wurster et al. 10 noted that the COVID-19 pandemic acted as both a limiting and confounding factor in their observed differences between paper-based and electronic records. In contrast, our study was conducted entirely within a stable eMR environment, where the pandemic did not alter the underlying system or documentation practices. As such, COVID-19 had no influence on the degree of completeness observed in our results.
It is important to make a distinction between the completeness of data and the quality of data. The former attests to the availability of the target data whereas the latter refers to the overall utility and fitness of data for its intended use. While data completeness is considered to be a dimension of data quality, the considerably larger scope of data quality was not the focus of the present study. Quality and accuracy of the available data might pose a separate challenge for use of routine care clinical data for research purposes. The results of this study compare well with the broad ranging degree of completeness (25–91%) presented in previous similar studies.4–10,15 This further illustrates the influence of the definition of completeness utilised and the precise secondary use case of the clinical data.
Despite these limitations, clinical data systems have been used for secondary purposes in improving perioperative outcomes, in particular in the United States and some Scandinavian countries.16–23 Therefore, if clinical data that already exist are to be leveraged for further (and broader) utility, an appreciation of the degree of data completeness is warranted. Furthermore, existing data entry mechanisms should not expand to further increase the burden of electronic clinical documentation for the sake of contriving a platform for registry generation.24,25 However, adapting current systems where possible to better serve this purpose seems more feasible.
In our study, variables with a high level of completeness for the most part included process data and data with (semi-)automated capture (mainly those recorded as part of the electronic anaesthesia record). For the data that were less complete, the reasons for incompleteness varied. Many variables are collected only ‘by indication’, such as frailty and National Surgical Quality Improvement Program scores, which are typically recorded in high-risk patients. Most notably, the absence of 38% of preoperative pathology data and the low level of completeness of postoperative pathology data likely stem from clinical rationalisation; this is further reflected in the overall low completion rate of numeric data types.
On closer inspection, the variables with the lowest completeness can be grouped into themes of missingness. 26 To interpret these systematically, we drew on the Clinical Adoption Meta Model (CAMM), which describes four inter-related stages of digital adoption: availability, system use, clinical behaviour and outcomes. 27 Mapping our findings to the CAMM highlights that incompleteness was rarely random, but reflected barriers at different levels of adoption. Some gaps arose from availability issues, where certain variables were never designed into the eMR (e.g. ‘ethnicity’, ‘date back at home’). Others stemmed from system use, where siloed data flows or manual processes limited routine capture (e.g. pathology, PACU pain scores). Finally, much of the missingness reflected clinical behaviour, where documentation was selective, conditional or rationalised (e.g. frailty scores, intraoperative temperature, comorbidity detail). Similar results were observed by Wurster et al. 10 A thematic summary of these patterns, with their alignment to CAMM dimensions, is presented in Table 2.
Themes of missingness in perioperative data.
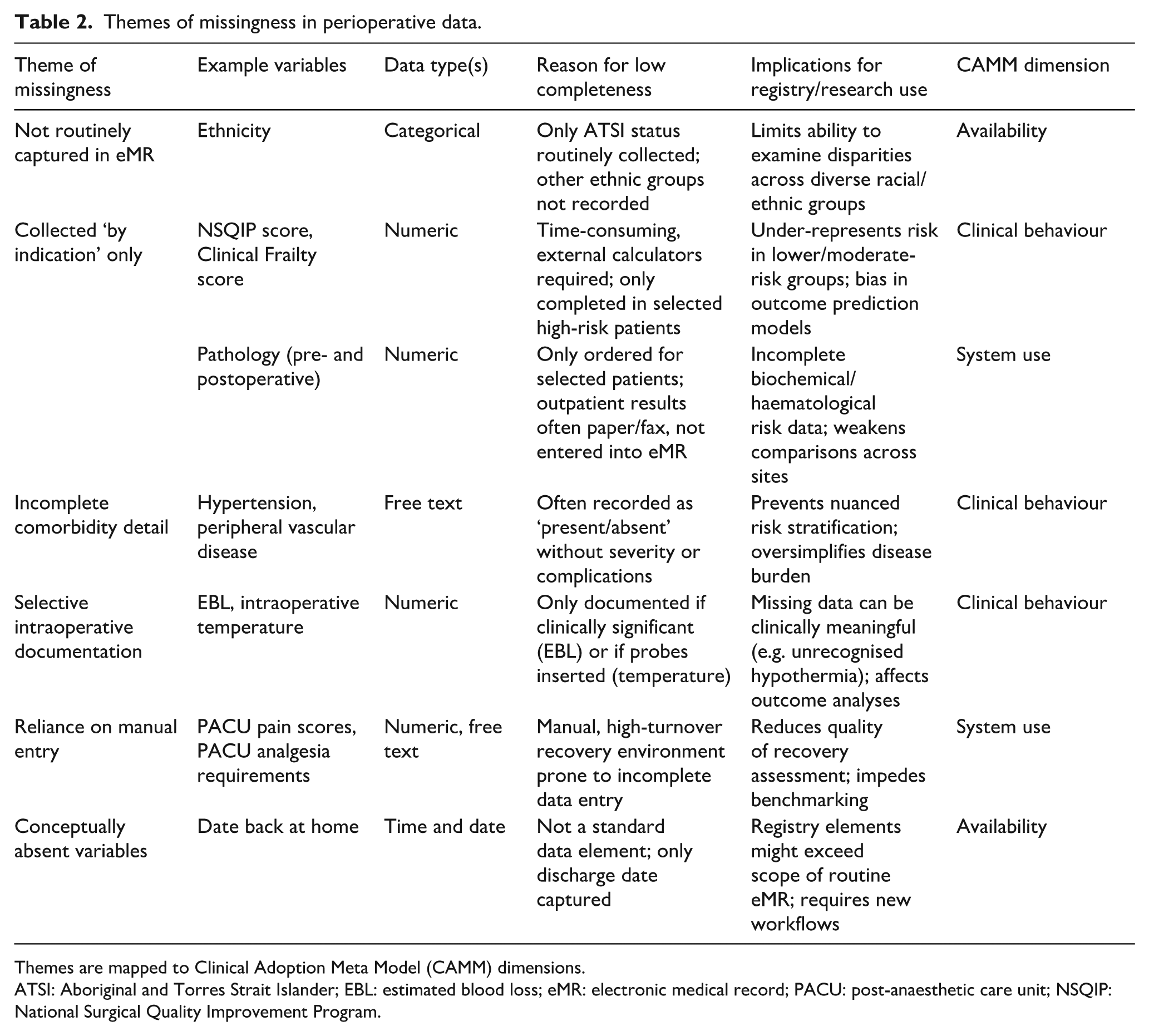
Themes are mapped to Clinical Adoption Meta Model (CAMM) dimensions.
ATSI: Aboriginal and Torres Strait Islander; EBL: estimated blood loss; eMR: electronic medical record; PACU: post-anaesthetic care unit; NSQIP: National Surgical Quality Improvement Program.
We therefore demonstrate that mapping data completeness within an eMR against the CAMM framework provides a systematic way to identify both structural and behavioural drivers of missingness. By linking these findings to the requirements of PCOREx, we show how gaps in data availability and consistency translate into practical limitations for registry adoption. Importantly, the approach outlined here is transferable: other centres can apply the same framework to interrogate their own eMRs, anticipate points of data loss and plan targeted solutions such as modular data linkage, general practice integration or national EHR interoperability.
Importantly, this study highlights the tension between electronic data extraction, which relies on structured, machine-readable fields and manual abstraction, which is accurate but resource-intensive and difficult to scale. Several challenges limit the completeness and reliability of eMR data for perioperative outcomes. Missing intraoperative metrics, such as temperature, often reflect omitted measurements rather than technological failures, while estimated blood loss—consistently the least complete metric—is frequently left unrecorded owing to its perceived clinical insignificance. The continued use of paper forms scanned into the eMR in non-machine-readable formats further complicates digital registry processes and introduces administrative delays. In addition, inconsistent data-entry practices, including duplicate or variably formatted information scattered across eMR sections, affect metrics such as Worst Pain Score and medication records. While advances in natural language processing, optical character recognition and machine learning offer potential to extract information from free-text fields, their integration into eMR systems is severely limited by data security, privacy, and computational and regulatory requirements.28–32 These constraints restrict the use of automated extraction tools and reinforce the continued reliance on robust, structured data capture as the most reliable and scalable approach for perioperative registry generation.
The configuration of Cerner PowerChart and SurgiNet at the study hospital must be acknowledged as a limitation. While hospitals within the same State Government clinical network share an identical configuration, other hospitals in the state—although also using PowerChart—might not implement the anaesthesia module, and hospitals in other states might employ entirely different eMR systems. This variability in system architecture, interoperability and local workflows constrains the generalisability of our findings. For registry purposes, the development of a nationwide standardised data collection tool that can interface with diverse eMR platforms would likely improve the robustness and comparability of registry data.
In the absence of a robust and nationwide EHR, the eMR at present captures only inpatient documentation. PDO is therefore visible only if patients re-present to hospital or attend a hospital-based outpatient clinic, creating a systematic bias towards sicker patients and underestimating outcomes occurring in the community. This limitation reflects a broader structural gap in availability within the CAMM framework, where the relevant data fields are not routinely collected in the eMR. Emerging technologies such as smart-device platforms, 33 or automated follow-up systems such as DayCOR34,35 (a patient-reported outcome survey system designed for day hospitals and anaesthetists) offer partial solutions, although these are dependent upon sustained patient engagement and, at present, remain largely separate from hospital systems. Whether such data streams can be integrated automatically into eMRs at scale is not yet established. However, with other existing databases, such as the ANZICS APD, which is well-recognised for its high-quality data, 36 an opportunity exists for modular data-linking to expand upon and improve the utility of PCOREx.37,38 In parallel, integration of general practice documentation—whether via nationally accessible EHR platforms or through structured data-sharing with local hospital-based eMRs—offers an additional, complementary avenue to capture long-term outcomes. Future registry design will therefore need to balance the technical feasibility of such linkages with governance, privacy and workflow considerations in order to deliver a sustainable model of comprehensive outcome capture.
This study highlights a critical limitation of using real world patient data for registry-based studies in perioperative patients. Real patient data can be incomplete when compared with registry requirements, as what is required for a complete registry is not always necessary for individual patient care. This must be kept in mind when designing a research question that is to take leverage of such data. However, when certain data points are considered critical for quality assurance or benchmarking, mandating such information to be entered into the clinical patient record could be considered.
In conclusion, eMR data for perioperative outcomes registries are constrained by incomplete documentation, non-standardised practices and limited interoperability, reflecting their design for clinical care rather than research. As noted by Wurster et al, 15 documentation practices often shift with eMR adoption; our study extends the work of Reilly et al 3 by moving from perceptions of feasibility to empirical evidence of real world completeness. By directly assessing data availability within a large institution, we show how these limitations create practical barriers to registry adoption while outlining a transferable framework that other centres can use to anticipate data gaps and plan targeted solutions.
Footnotes
Author Contributions
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.