
Abstract
Background
New daily persistent headache (NDPH) is a primary headache disorder that often presents in adolescence. Presently, there is no effective treatment for NDPH and a paucity of clinical trials exploring therapeutic options. In this study, we explored the relative benefit of currently used treatments to help inform future trials and clinical decision-making.
Methods
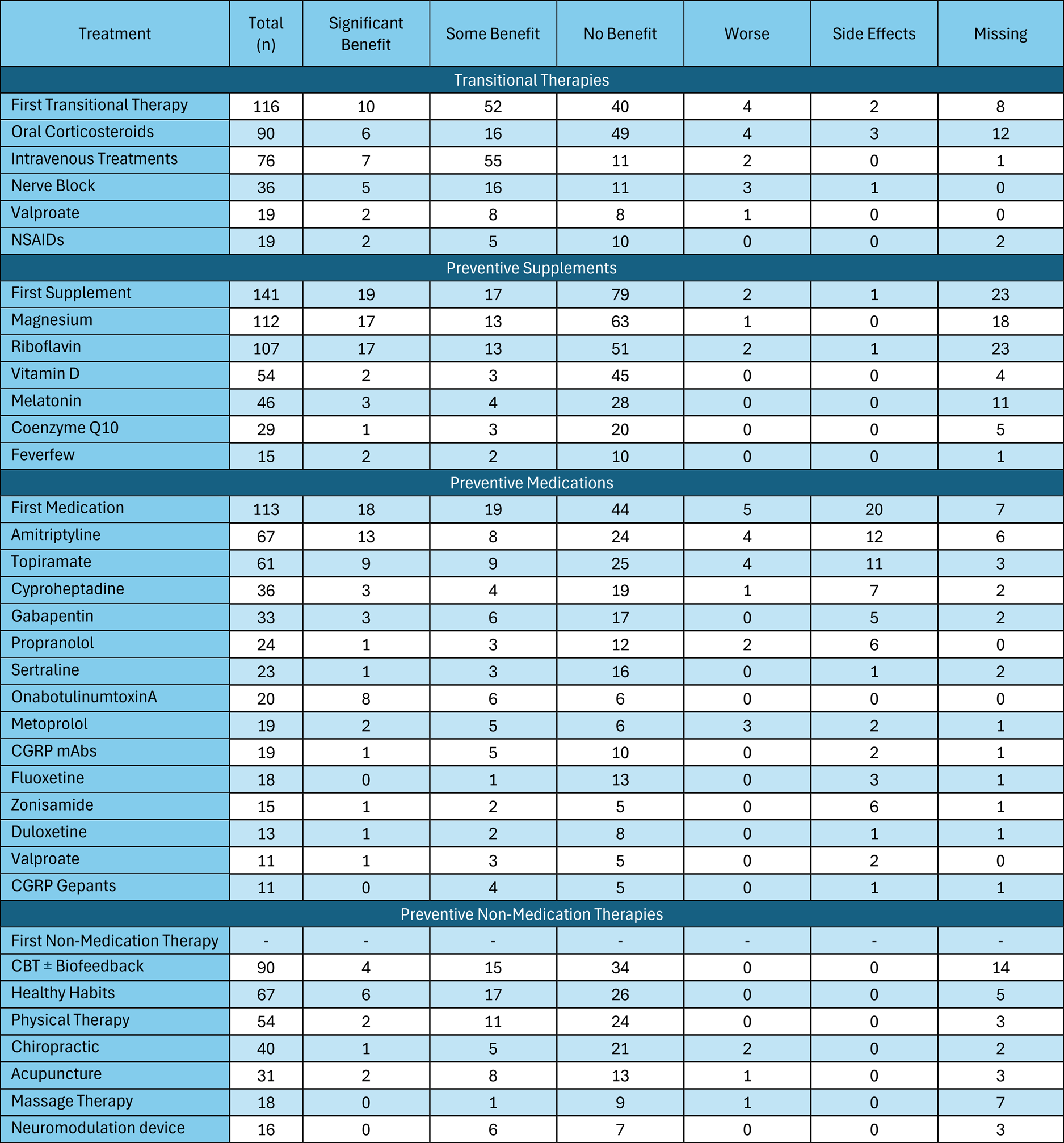
In this retrospective chart review study, patients aged 5–17 years with abrupt onset continuous headache and headache duration of at least one month (constituting NDPH or probable NDPH) were identified based on responses to a Headache Questionnaire in child neurology clinic and confirmed with chart review. We included all treatments (transitional therapy, preventive supplement, preventive medication and preventive non-medication therapy) started during continuous headache until both break in continuous headache and sustained improvement in headache were achieved. For treatments tried by at least 10 patients and for the first treatment tried in each category, we calculated proportions of any documented benefit, including “Significant” (≥30% improvement lasting ≥4 weeks) and “Some improvement” (all other improvement) and proportions of negative outcome (those with worsened headaches or side effects warranting discontinuation), as well as median time to treatment. We used multivariable regression modeling to examine for factors associated with headache outcomes. Treatments may have overlapped.
Results
Of the 165 patients, the largest proportion of patients experienced benefit with the first transitional therapy (62/108; 57%), which was usually intravenous medications ± oral corticosteroids. The first supplement tried, usually riboflavin ± magnesium, offered benefit in (36/118; 31%), with few negative outcomes (3/118; 3%). The first prescription preventive tried, usually amitriptyline or topiramate, offered similar benefit (37/106; 35%) as the first supplement, but with more negative outcomes (25/106; 24%). Despite being tried after oral preventives, onabotulinumtoxinA injections offered benefit to the largest proportion of patients (14/20; 70%) without negative outcomes (0%). Overall, the time to first therapy was weeks to months into continuous headache: shortest for transitional therapies (median = 49 days, interquartile range = 17–92 days), and longest for non-medication therapies (median = 144 days, interquartile range = 61–381 days). Increased time to any first treatment was associated with decreased odds of headache improvement at one-year follow-up (odds ratio = 0.823, 95% confidence interval = 0.715–0.946, p = 0.006).
Conclusions
Children and adolescents with new onset continuous headache experience treatment delays which are associated with worse outcomes. Clinicians should consider use of transitional therapies in combination with preventive treatments as early as possible. Prospective natural history studies and trials are needed to improve treatment outcomes for pediatric patients with NDPH.
Introduction
New daily persistent headache (NDPH) is a primary headache disorder characterized by its abrupt onset and chronic, unremitting nature. The International Classification of Headache Disorders, 3rd edition (ICHD-3), describes NDPH as a headache with a “distinct and clearly remembered onset” that becomes continuous within 24 hours of onset, has been present for at least three months, and is not better attributed to another primary or secondary headache disorder. 1 Little is currently understood about the risk factors or pathophysiology underlying this relatively rare and enigmatic headache disorder.2–4 NDPH presents more frequently in children and adolescents than adults. 5 The continuous headache in NDPH often persists for months to years, and treatments may be ineffective in breaking the continuous pain.6,7 As such, NDPH is associated with high levels of disability and significant reduction in quality of life.8,9
There is little clinical guidance available for treating NDPH, and there are currently no approved treatments for NDPH. A common recommendation is that clinicians treat NDPH based on the predominant headache phenotype that the patient presents with, but there is currently no evidence for the use of one treatment over another.2,3,10 The objective of this retrospective study was to determine the relative benefit of treatments and timing of treatments tried by pediatric patients with new onset continuous headache to contribute to future studies exploring treatment trials for NDPH.
Methods
Design
This study was a retrospective, chart-review study of a cohort of children and adolescents who were seen in tertiary pediatric neurology clinic at the Children's Hospital of Philadelphia (CHOP). This is the second manuscript from these data, with demographics and clinical outcomes published previously. 11
Ethical conisderations
Headache questionnaire data were collected clinically and extracted from the electronic health record into the CHOP Headache Registry with approval from the CHOP institutional review board (IRB), with a waiver of the requirement for informed consent.
Inclusion criteria
These have been reported in detail previously. 11 To summarize: this study included 5–17-year-olds who presented to child neurology clinic with abrupt onset headache of at least one month duration, without prior escalation of headache frequency or preceding head injury. All patients completed the CHOP Headache Questionnaire, which is offered to all patients who present with chief complaint of headache. 12 All responses that were thought to represent NDPH or probable NDPH were then reviewed by a fellowship-trained pediatric headache specialist (CLS). Cases with definite or possible secondary causes of headache were excluded from the analysis. Every patient was assessed by clinical and fundoscopic examination, and the majority additionally received brain imaging and laboratory studies as part of clinical care. We included patients with headache duration of one to three months (probable NDPH), as well as those with a duration of three months or more (NDPH) at time of first neurology visit, as previous analysis revealed that there was no difference in outcomes between these patient groups. This deviation from the ICHD-3 definition of NDPH is further elaborated in previous work. 11
Data collection
A standardized data form for this study was developed in a secure REDCap (Research Electronics Data Capture) database.
13
Data collected from each patient chart included the following:
11
Headache treatments tried at any point during continuous headache, falling into four broad categories: transitional therapies, preventive medications, preventive supplements and preventive non-medication therapies. A full list of included treatments and details of certain therapy regimens is provided in the Supplementary material. Transitional therapies refer to treatments used for severe headaches that are unusually prolonged (e.g. a course of corticosteroids)
14
and may act as a “transition” between acute and preventive therapies, as well as treatments used for severe exacerbation of headache. Preventive medications and supplements include any that were prescribed or recommended for the purpose of long-term headache treatment, regardless of whether that medication would typically be considered a migraine preventive. Non-medication therapies include any non-pharmacologic treatment recommended or prescribed for the treatment of the continuous headache. Date of initiation of each treatment and of first treatment tried within a treatment category. Start dates were not always available in medical records for non-medication therapies; hence, only the date of the first treatment within this category was recorded. Headache response to each treatment, including the first treatment within each category, scored on a six-part scale: Significant benefit, Some benefit, No benefit, Worsened, Discontinued due to side effects, Missing. “Significant benefit” was defined as four or more weeks of ≥30% improvement in severity, frequency and/or disability.15,16 “Some benefit” was recorded if some degree of improvement in these areas or other quality of life was observed, but did not meet criteria for “Significant benefit”, or if a treatment was continued for three months or more without recorded benefit or worsening as it was assumed continued therapy implied benefit. “No benefit” was recorded if no improvement in headache was observed, and “Worsened” was recorded if clear worsening of headache was documented. If a treatment was initiated prior to the headache becoming continuous, it was included in the analysis only if it was maintained as a preventive therapy during the continuous headache. Treatments often overlapped with one another, and if multiple treatments were concurrent at the time of headache improvement, each treatment received a score of at least “Some benefit” unless clear distinctions were made between the treatments’ outcomes in patient records. Non-medication therapies were not included in the analysis of the first treatment tried within a treatment category due to imprecise start dates for this category, as many were done outside the clinic. Any recorded break in continuous headache, defined as “0/10 headache pain for >24 hours and subjective benefit for at least one week.” A transition to episodic or daily non-continuous headache is also considered to be a break. Individual patient outcomes at one year from onset of continuous headache and at time of last follow-up, including whether headache had transitioned to non-continuous and if there was any headache improvement. If the last follow-up occurred sooner than one year from onset of continuous headache, the last follow-up visit was carried forward as the one-year outcome. Based on the timing of case ascertainment and follow-up data collection, all youth had the possibility of at least one year of follow-up data. Total number of onabotulinumtoxinA treatment cycles, the first cycle with any benefit, the first cycle with Significant benefit, and the number of concurrent preventive therapies during the first cycle with any benefit for all patients who received onabotulinumtoxinA injections.
Statistical analysis
There was no a priori power calculation. The sample size was determined based on the number of patients who met inclusion criteria. Values are rounded to the degree of precision with which they were measured. If a continuous variable was not normally distributed, medians and interquartile ranges are reported. Analyses were done in Stata, version 17 (StataCorp, College Station, TX, USA) and Excel 2024 (Microsoft Corp., Redmond, WA, USA). Figures were created in R (R, version 2024.04.2) 17 using packages ggplot2 18 and ggvenn. 19
Primary analysis: individual treatment outcomes
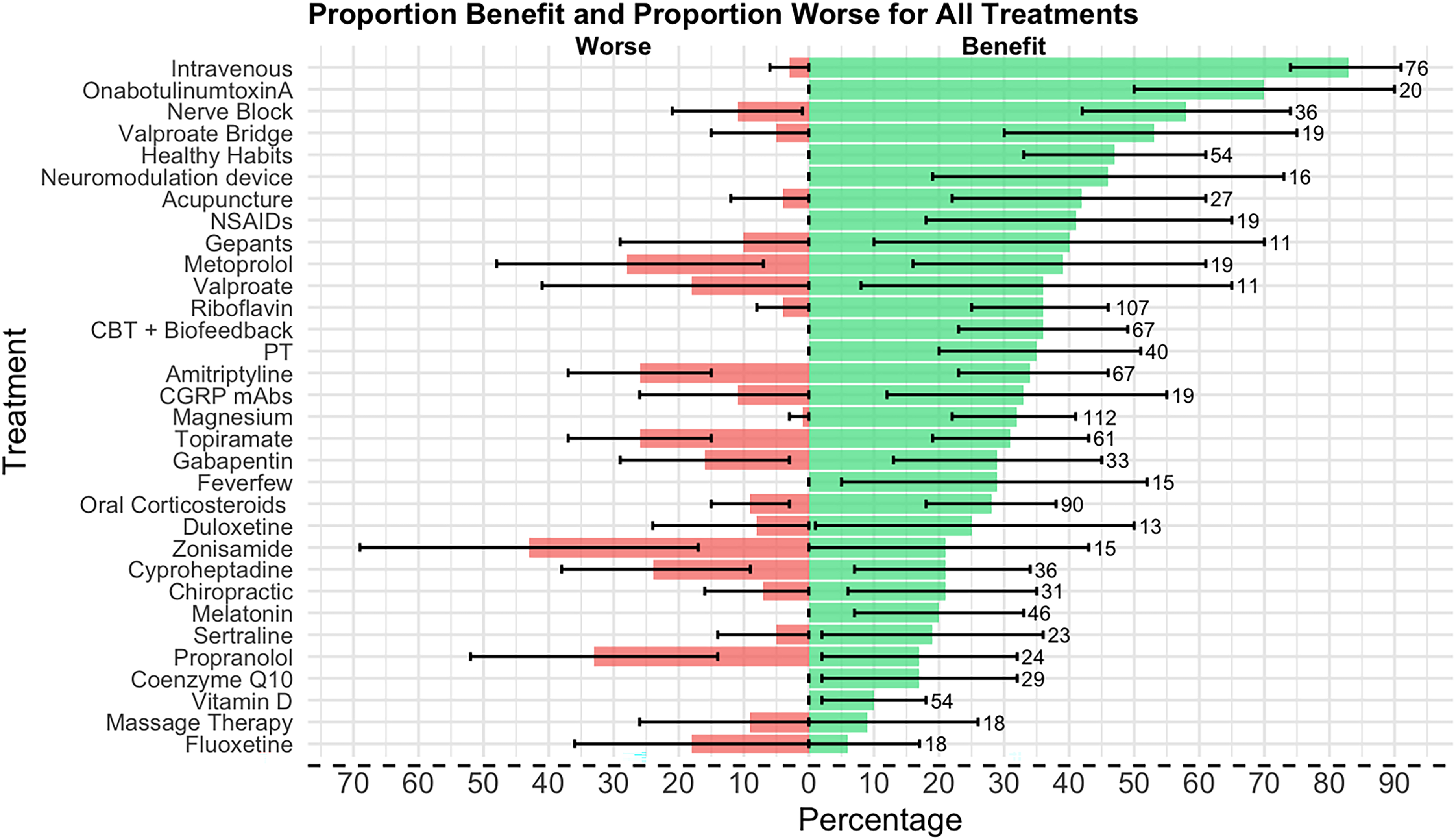
For each treatment, the proportion of patients who received any benefit (defined as “Significant” or “Some benefit”) was calculated as proportion with benefit, and the proportion of patients with negative outcomes while on a treatment (defined as “Worsened” or “Discontinued due to side effects”) was calculated as proportion worse. These calculations excluded patients who tried a therapy without recorded follow-up (defined as “missing”). Confidence intervals (CIs) for each proportion were calculated with 95% confidence. The median time to each therapy from onset of continuous headache was calculated with interquartile ranges between the first and third quartiles. Only treatments that were tried by at least 10 patients were included in the analysis for individual therapies.
Secondary analysis: outcome of first treatment within treatment category
Treatments initiated for another diagnosis prior to the onset of continuous headache were excluded from this analysis. Patients were often started on multiple therapies within the same category simultaneously. In these cases, we included only the treatment that demonstrated the most benefit in our analysis of first treatment benefit and of the rates of first treatment within each category. For example, if a patient was initiated on oral corticosteroids and intravenous (IV) treatments on the same date, the transitional therapy with greater observed benefit was included for this analysis. This analysis by category did not exclude treatments that were tried by at least 10 patients.
Analysis of outcomes vs. time to treatment initiation
Treatment outcome
We performed univariable logistic regression to examine the relationship between time to treatment initiation and the benefit of the first treatment within each category for which time to treatment initiation was available (i.e. transitional therapy, preventive supplement, preventive medication) as well as the first treatment from any category.
Patient outcome
In addition, we explored whether time to treatment for these categories and the non-medication category were associated with odds of any headache improvement at time of last follow-up and at one-year from onset of continuous headache. We also examined odds of a patient transitioning to non-continuous headache at last follow-up, as well as odds of transition to non-continuous headache within 6 months of initial visit. This model made use of previously published patient outcome data. 11
For the univariable models where time to treatment was significantly associated with the treatment or patient outcome, we then ran multivariable models. The full models included all covariates which had a significant association with the outcome (p < 0.1) and backwards elimination was used. Here we present the adjusted odds ratio (OR) with 95% CI for the time to first treatment of any category and for each individual treatment category where there remained a significant association. We also summarize the covariates which had a significant association with outcomes across at least two models.
Missing data
Those with missing data were excluded in the main regression analyses, and in sensitivity analyses those with missing data were alternately grouped with those who improved and did not improve.
Results
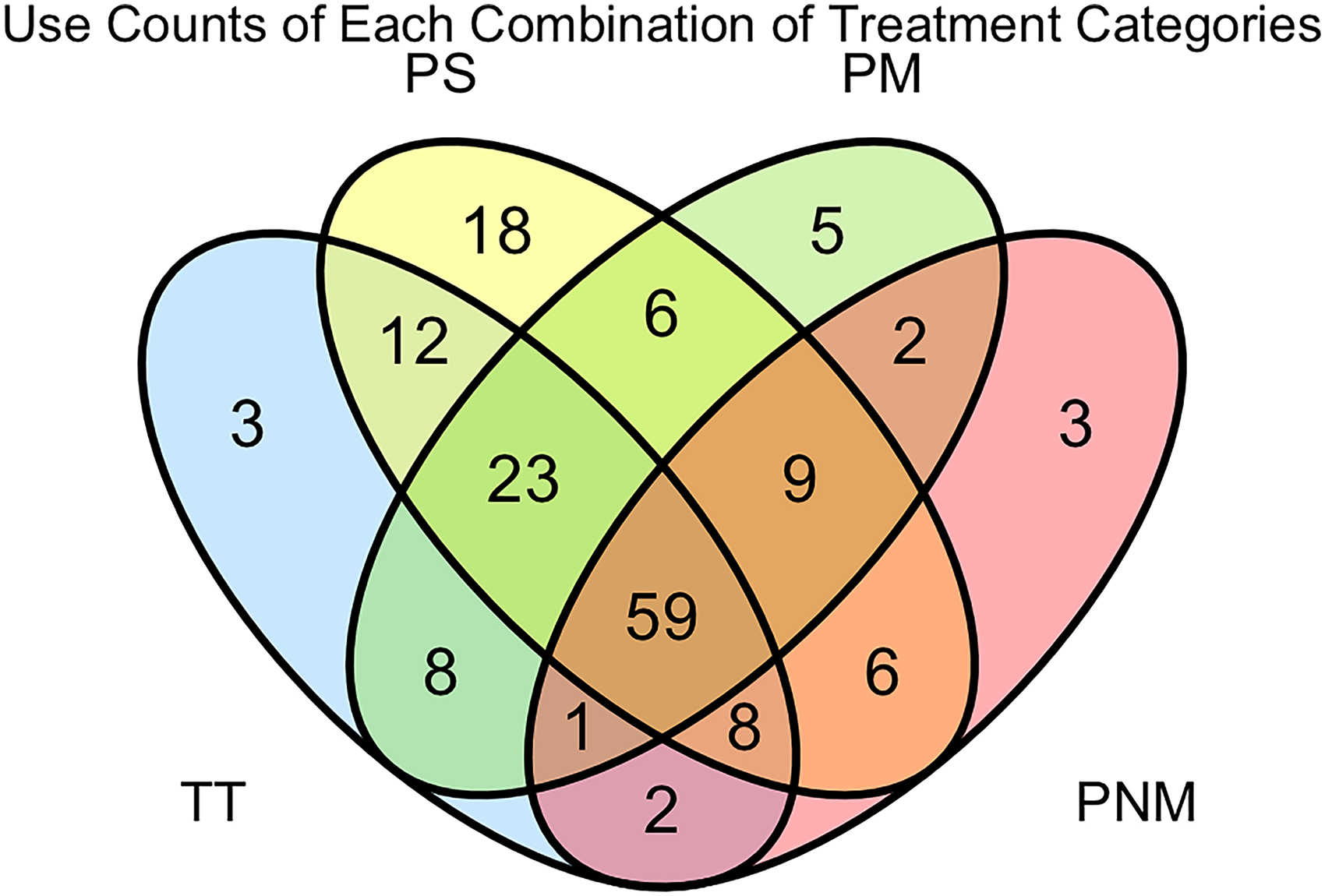
In total, 172 patients met inclusion criteria for analysis; 76% were female and median age was 14.5 years. 95% reported headache features consistent with migraine. Demographic and headache descriptive data have been provide previously. 11 Of these, 165 tried at least one treatment. Treatment outcomes are shown in Tables 1 and 2. Of the 165 patients, 116 (70%) tried a transitional therapy, 141 (85%) tried a preventive supplement, 113 (68%) tried a preventive medication and 90 (55%) tried a preventive non-medication therapy. The distribution of patients who tried various combinations of these treatment categories is illustrated in Figure 1.
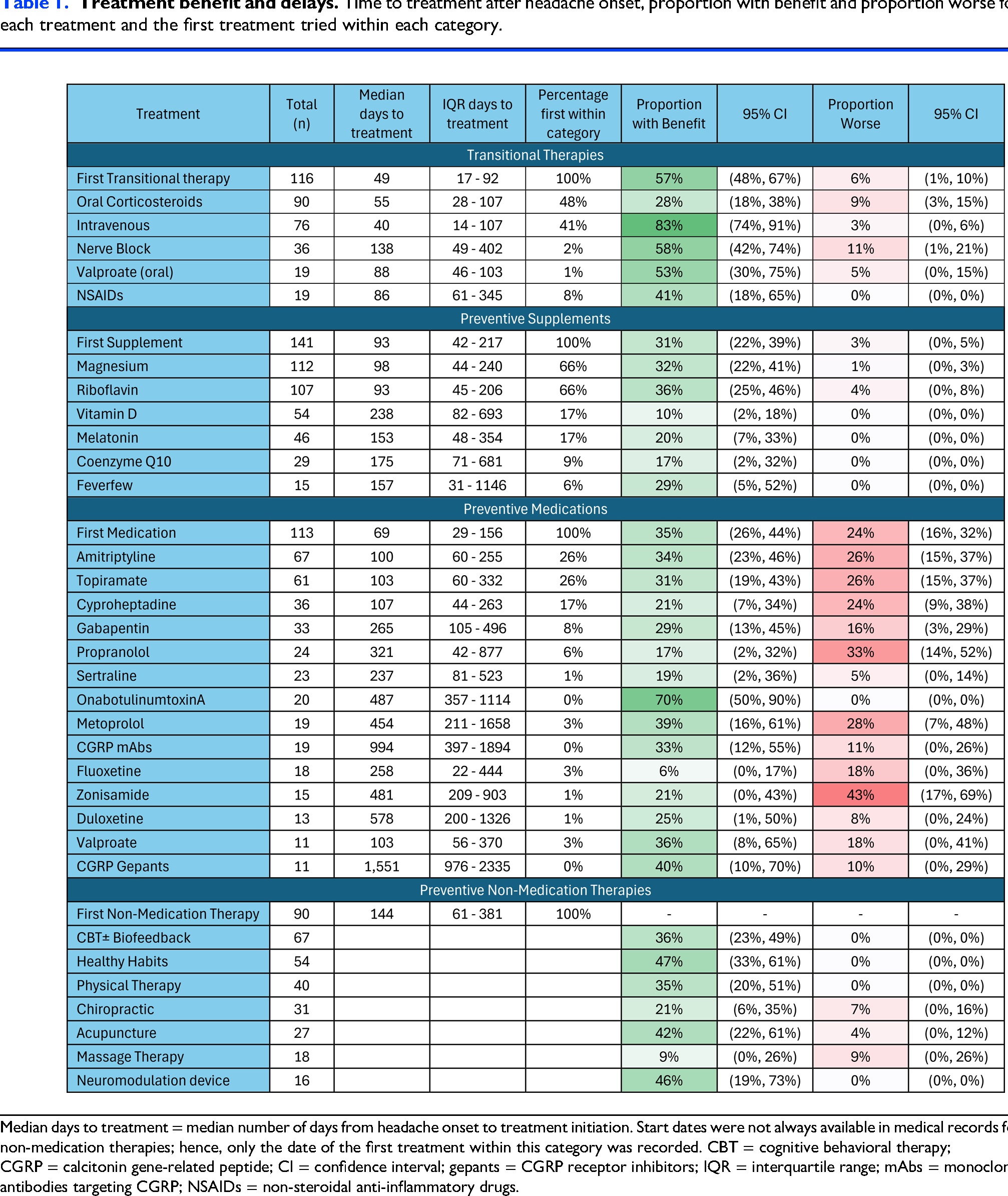
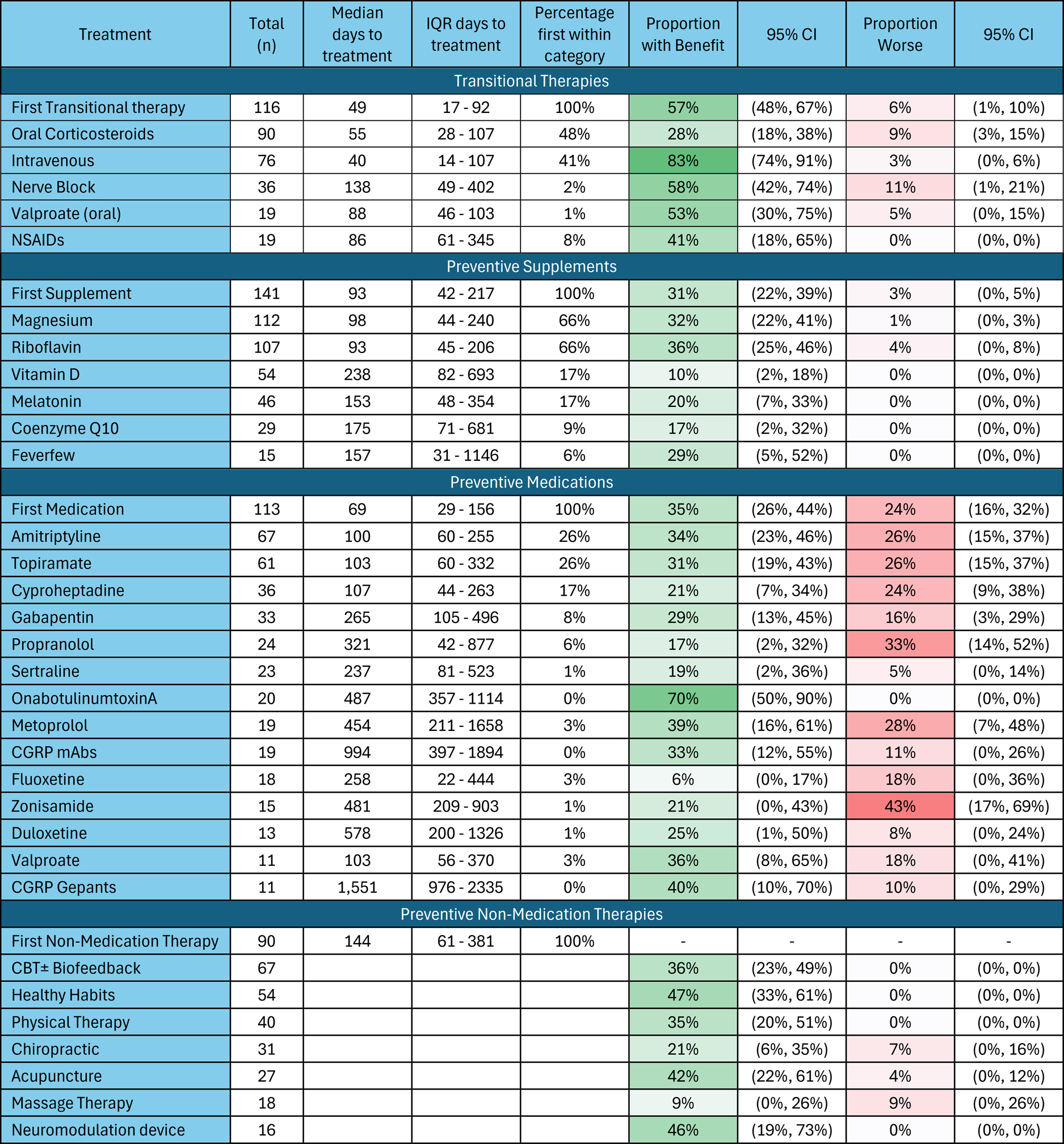
Median days to treatment = median number of days from headache onset to treatment initiation. Start dates were not always available in medical records for non-medication therapies; hence, only the date of the first treatment within this category was recorded. CBT = cognitive behavioral therapy; CGRP = calcitonin gene-related peptide; CI = confidence interval; gepants = CGRP receptor inhibitors; IQR = interquartile range; mAbs = monoclonal antibodies targeting CGRP; NSAIDs = non-steroidal anti-inflammatory drugs.
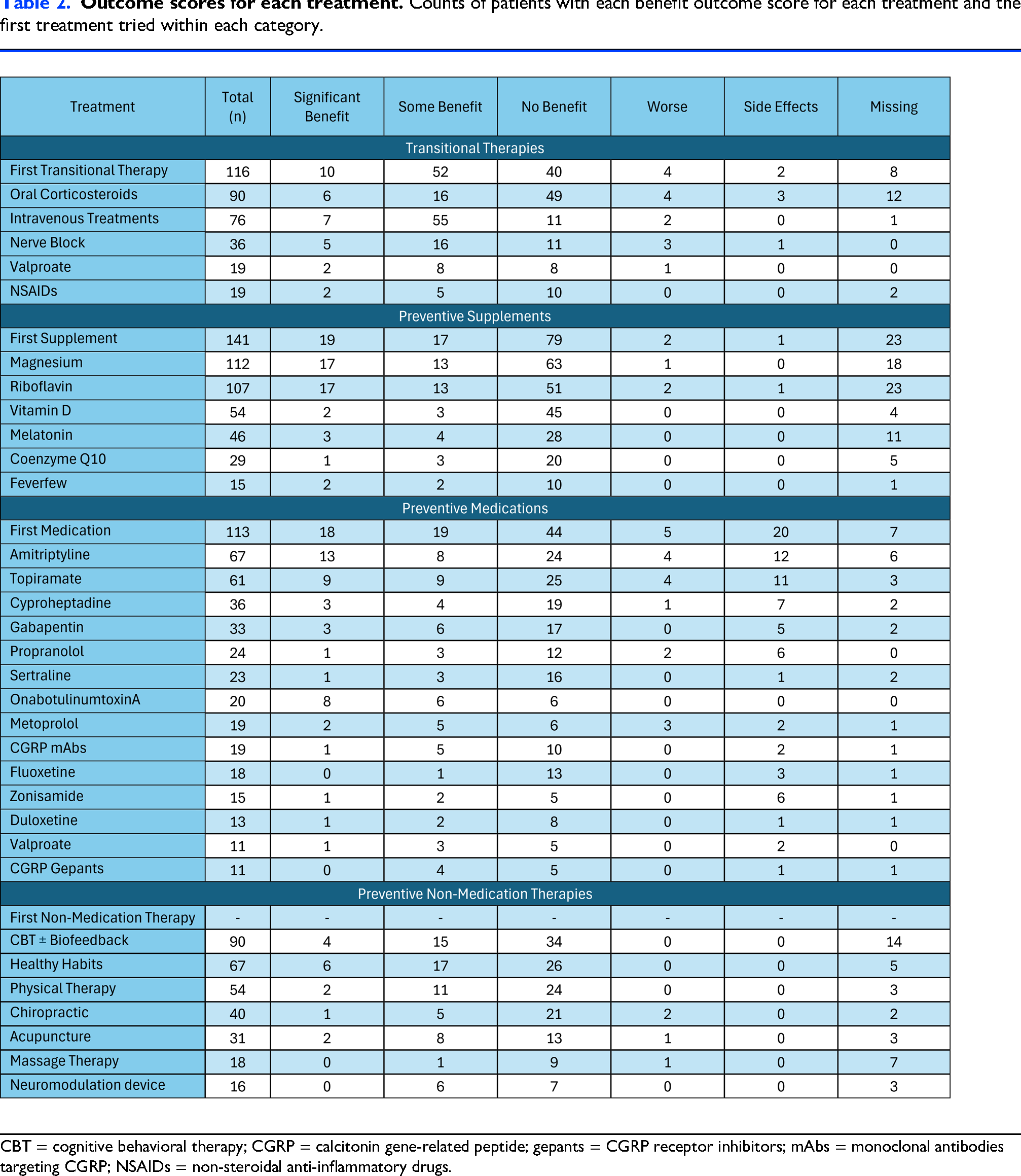
CBT = cognitive behavioral therapy; CGRP = calcitonin gene-related peptide; gepants = CGRP receptor inhibitors; mAbs = monoclonal antibodies targeting CGRP; NSAIDs = non-steroidal anti-inflammatory drugs.
Transitional therapies
Amongst all who tried a transitional therapy (n = 116), corticosteroids were tried first for 56 (48%) and IV treatments for 47 (41%). Oral corticosteroids and IV treatments were also the most frequently tried (n = 90 and n = 76, respectively). Although there were some missing data on outcomes, among those with known outcomes, IV treatments provided benefit to the largest proportion (62/75; 83%; 95% CI = 74–91%), while oral corticosteroids provided benefit to the smallest proportion (22/78; 28%; 95% CI = 18–38%). The majority of these patients reported “Some benefit” rather than “Significant benefit” (Table 2). Nerve blocks (21/36; 58%; 95% CI = 42–74%) and oral valproate (10/19; 53%; 95% CI = 30–75%) provided benefit to a large proportion of patients but were less frequently used.
Preventives
The most commonly used preventive supplements were riboflavin (n = 107) and magnesium (n = 112). They were often used simultaneously as the first supplement(s). Within the preventive medication category, amitriptyline (n = 67) and topiramate (n = 61) were the most frequently tried, and the most frequently tried first medication (each for 29 patients). They had similar rates of benefit as seen with riboflavin and magnesium. The largest proportions of side effects and/or worsening headache were observed in the preventive medication category. For the non-medication therapies, very few patients endorsed headache worsening (Table 1). The use of neuromodulation devices for headache was limited in this dataset, but a modest proportion of patients found benefit with their use (6/13; 46%; 95% CI = 19–73%).
OnabotulinumtoxinA injections offered benefit to the largest proportion of patients (14/20; 70%; 95% CI = 50–90%) of the preventive medications without any reported negative outcomes (0%). The median first cycle with any benefit was the first cycle of treatment (median = 1; interquartile range (IQR) = 1), and the median first cycle with significant benefit was the second cycle of treatment (median = 2; IQR = 1). In general, patients received many cycles of treatment (median = 7l; IQR = 8.5) in the period of time reflected in this data. At the first cycle with any benefit, patients were usually using concurrent preventive treatments (median = 2; IQR = 2.25).
Comparison across treatment categories
Time to first treatment in each category was shortest for transitional therapies (median = 49 days; IQR = 17–92) and longest for non-medication therapies (median=144 days; IQR = 61–381). Time to first preventive medication (median = 69 days; IQR = 29–156) and to first preventive supplement (median = 93 days; IQR = 43–217) were widely distributed, although still generally initiated before preventive non-medication therapies.
Comparing the first therapy tried in each category, the first transitional therapy provided benefit to the largest proportion of patients overall (62/108; 57%). The first preventive supplement offered benefit in 36/118 (31%), with few patients reporting negative outcomes (3/118; 3%). The first preventive medication offered similar benefit (37/106; 35%) as the first supplement, but with more patients reporting negative outcomes (25/106; 24%).
A diverging bar chart plotting the proportion with benefit and the proportion worse for all treatments is provided in Figure 2.
Predictors of benefit
The results of the regression analyses are shown in Table 3. Outcomes are included if the predictor had p < 0.05 in the initial univariable analysis. No significant association was found between time to treatment initiation and the benefit of the first treatment within each category (transitional therapy, preventive supplement, preventive edication, or any treatment). In other words, in this data set, we did not find that time to initiation of a treatment was associated with the outcome of that treatment.
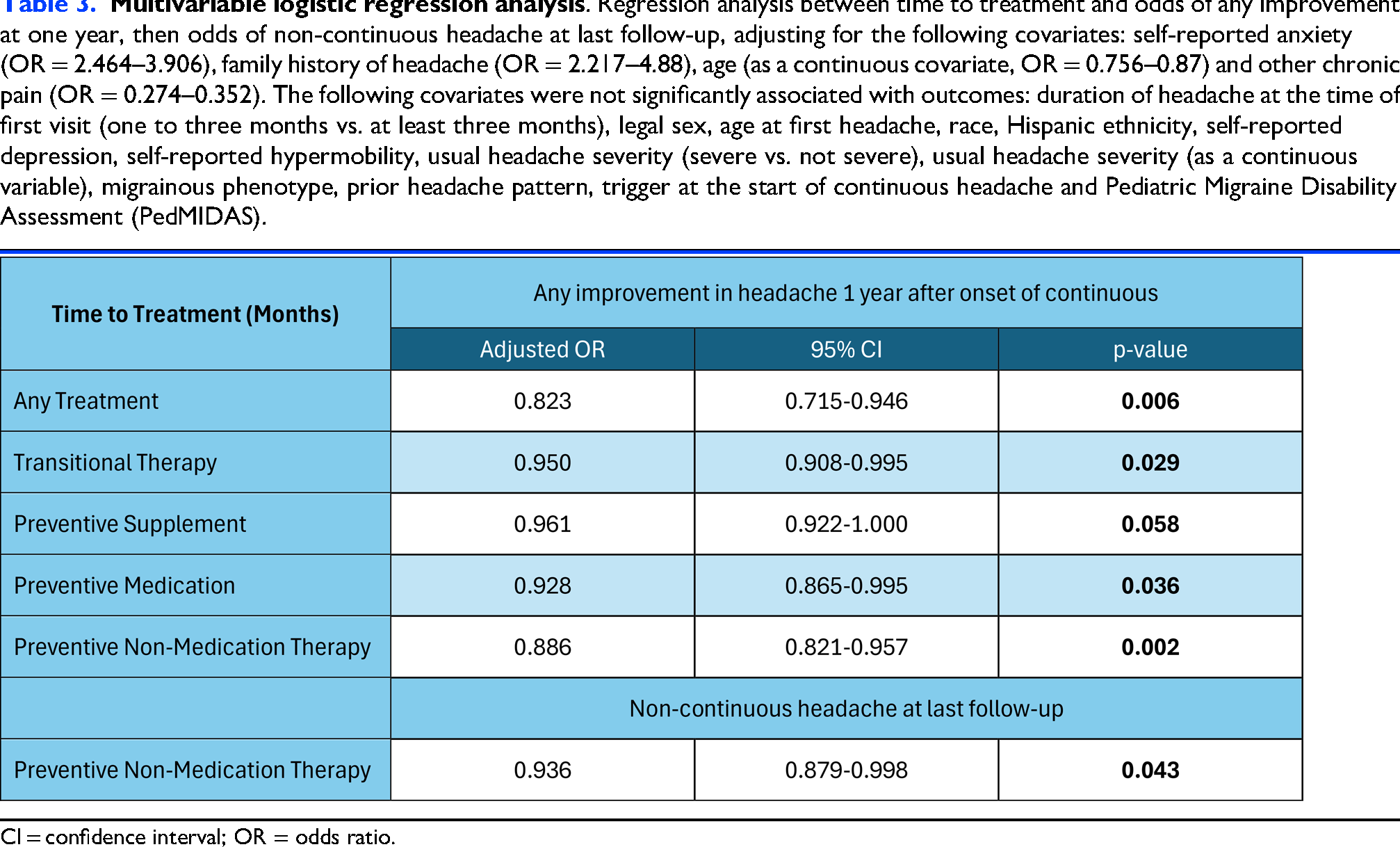
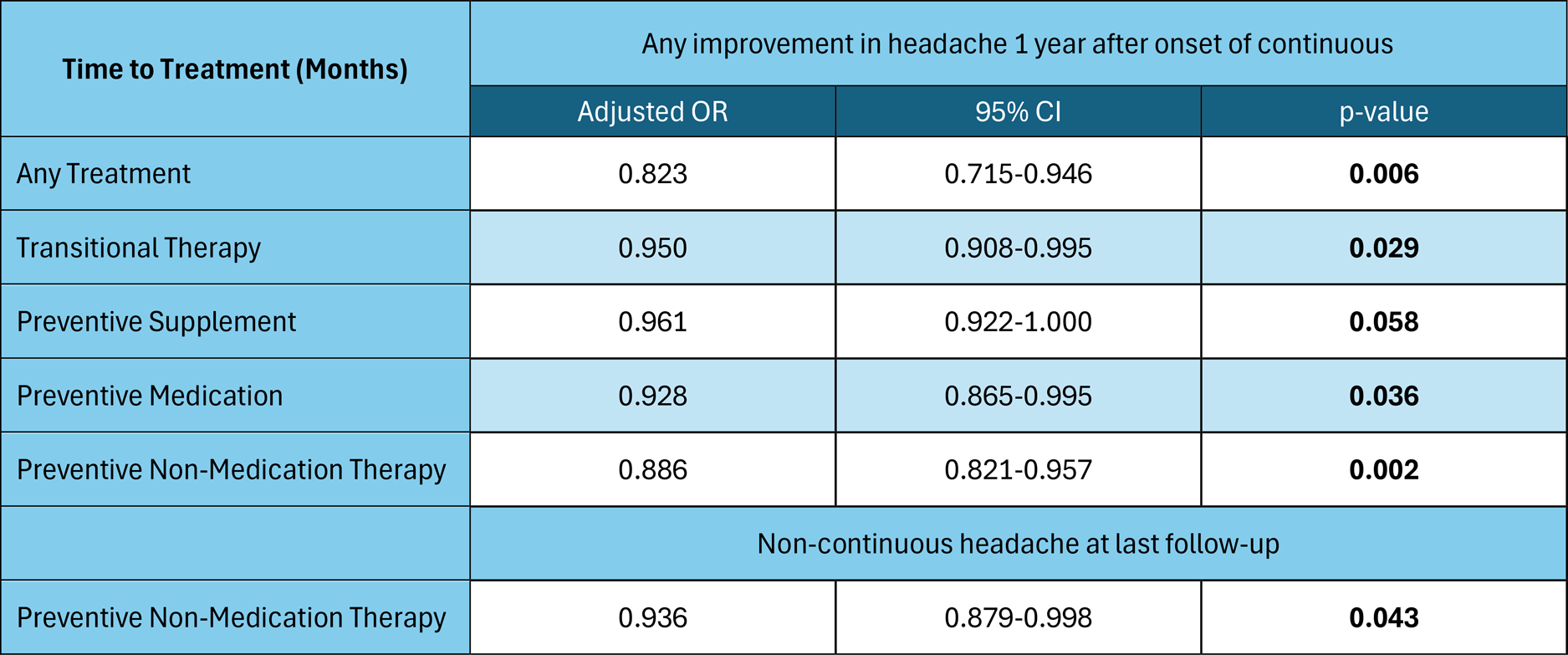
CI = confidence interval; OR = odds ratio.
On the patient level, most analyses were also not significant. The time to first transitional therapy, preventive supplement, preventive medication and preventive non-medication therapy was not associated with the odds that the patient would report any benefit by last follow-up or break in continuous pain within six months of initial visit. However, each month increase before receiving any treatment was associated with decreased odds of any improvement at one year (OR = 0.823; 95% CI = 0.715–0.946, p = 0.006). The time to first treatment in each category showed a similar relationship for improvement at 1 year, although with smaller magnitude compared to the time to any treatment. Additionally, each month delay in initiation of non-medication therapy decreased the odds that a patient's headache transitioned to non-continuous at last follow-up (OR = 0.936; 95% CI = 0.879–0.998; p = 0.043). These relationships persisted when adjusting for significant covariates, except for the relationship between preventive supplements and odds of any improvement at one year. Covariates which were significant in at least two univariable models of patient outcomes included self-reported anxiety (OR = 2.464–3.906), family history of headache (OR = 2.217–4.880), age (as a continuous covariate, OR = 0.756–0.870) and other chronic pain (OR = 0.274–0.352). Sensitivity analyses for missing data demonstrated similar patterns, so here we present only the primary analysis for each outcome.
Putting this together, while earlier initiation of any treatment does not necessarily improve the likelihood of response to that treatment, it does increase the odds that the patient will feel better at one year. Similarly, earlier initiation of non-medication therapy is not associated with better response to that therapy, but increases the odds that a patient will have non-continuous headache by the last follow-up visit in the data set.
Discussion
The findings of the present study suggest that earlier treatment of new onset continuous headache may be associated with better outcomes. In this retrospective study, for each month of delay in initiating any treatment, the odds of improvement at one year decreased by nearly 20% (OR = 0.823; 95% CI = 0.715–0.946). This is in contrast to our earlier reported finding from this same study cohort that showed that children and adolescents with new onset continuous headache of one to three months duration vs. more than three months at the time of first neurology visit did not have different headache outcomes. 11 Hence, time to treatment (including treatment given in other settings like the emergency department) seems to matter more than the duration of headache at time of first neurology visit. Notably, while self-reported anxiety and family history of headache appear to increase the odds of positive outcomes, older age and the presence of other chronic pain are independently associated with decreased odds of positive outcomes.
These data demonstrate that, even at an academic center with a large headache clinic, initiation of all categories of treatment is delayed in new onset continuous headache. While transitional therapies were typically the first treatment given, these were still given relatively late in the course of continuous headache. Preventive supplements were also often initiated after months of continuous headache despite their favorable safety profile and availability, and initiation of preventive non-medication headache therapies such as cognitive behavioral therapy (CBT) was even more delayed. Our regression analysis findings suggest that later use of non-medication therapies is associated with lower odds of transition to non-continuous headache.
In the present study, the use of transitional therapies was associated with the greatest proportion of benefit of any treatment category. The largest contributor to this proportion, however, is the “Some benefit” score, while preventive treatments provided “Significant benefit” to a higher portion of patients compared to transitional therapies (Table 2). Therefore, it may be that transitional therapies are effective in reducing the headache intensity seen in NDPH, but not in resolving the headache entirely, indicating the importance of also initiating preventive treatment.
The proportion of patients in this study who responded to a supplement was similar to the proportion who responded to a prescription preventive medication, suggesting that it is reasonable to start with either. However, the proportion of patients who had worse outcomes was higher with prescription medications. This was predominantly driven by side effects rather than headache worsening (Table 2). One interpretation may be that prescription medications are not more likely to provide benefit than a supplement but are more likely to cause side effects. However, prescription medications were often tried after supplements, and generally, only patients who did not respond to supplements went on to try prescription agents. It is therefore possible that prescription agents are also more likely to be effective than supplements in addition to being more likely to cause side effects. As is recommended in current pediatric migraine preventive guidelines, 20 clinicians treating youth with NDPH should engage in shared decision-making around preventive treatment trials.
With regards to second or third-line preventive therapy, this study suggests that onabotulinumtoxinA injections is a reasonable consideration. OnabotulinumtoxinA has demonstrated efficacy in adults with chronic migraine, 21 there is some evidence to support its use in adolescents with migraine, 22 and recent data have also suggested it may be helpful in treating NDPH. 23 In the present study, onabotulinumtoxinA injections provided “Significant benefit” to 8/20 and “Some benefit” to 6/20 patients, the largest proportion of benefited patients (14/20; 70%) without any reported negative outcomes, and benefit frequently occurred in the first or second cycle of treatment. However, n = 20 is a small number of patients, and it is possible that previously tried or concurrent therapies may have also contributed to the observed benefit. Of note, calcitonin gene-related peptide(CGRP) pathway preventive treatments were associated with moderate proportions of benefit and low proportions of negative outcomes in the present study. This is in contrast to primarily adult survey data of NDPH describing that CGRP-targeted therapies were amongst the most helpful. 24 However, given that CGRP-targeted therapies were approved in adults overlapping the start of this patient cohort, and insurance coverage is challenging, these treatments were used infrequently and late in the course of disease with a median time to treatment of approximately three to four years. Both CGRP-targeted therapies and onabotulinumtoxinA injections were notably only tried by patients who had previously tried and failed two or three classes of preventive medications due to insurance requirements.
The treatment of NDPH is often challenging due to its marked refractoriness to most therapies.6,7 Given this, a preventive treatment that helps even a small proportion of patients might still be worth trying in clinic. By that metric, almost every one of the treatments in the present study seemed helpful in at least a small proportion of the patients who tried it. Of course, because these data are from the clinical setting, some of the improvement may have been from natural history, the placebo effect, or concurrent therapies.
Limitations
The retrospective nature of our study limits our ability to infer causality between treatments and outcomes. Furthermore, patients tried treatments in varying order and at different points in their disease course, making it difficult to compare outcomes from different treatments. In clinical practice, insurance often limits access to certain therapies until others have been tried. As a result, only patients with the longest-lasting, most treatment refractory NDPH will have access to some treatments, making it difficult to know what the outcomes would be if these treatments were used as first-line therapy. Treatments were also sometimes given concurrently, including starting multiple therapies at the same time, making it difficult to determine if any one treatment drove outcomes, or if it was the combination of therapies that did. The study cohort is also subject to referral bias because only children seen by general neurology or headache clinic were included. The scoring of treatment benefit was often subject to reviewer interpretation and outcome data for some treatments was missing. The assumption that continued therapy for at least three months implied benefit when treatment outcome was not recorded may have resulted in more favorable benefit data for these treatments. Additionally, use of certain therapies was likely underestimated in this analysis. For example, non-steroidal anti-inflammatory drug (NSAID) transitional therapy may have been recommended more often but not necessarily recorded in the patient chart or not prescribed as many NSAIDs are available over the counter. Similarly, non-medication therapies may have been implemented or tried, but if this was not documented in the chart, we could not capture it. Lastly, our data are from a single tertiary center and thus our findings may not generalize to other settings.
Future research
Prospective studies are needed to clarify the relationship between early, aggressive treatment of NDPH and clinical outcomes in children and adolescents. Given the findings of the present study, future work focusing on strategies that decrease treatment delays should be prioritized. For example, delay in starting a prescription preventive may be due to how long it takes to get an appointment with pediatric neurology. Educating primary care pediatricians to initiate a transitional therapy and a preventive supplement when a patient presents with new onset continuous headache, even while work-up is ongoing, could be a strategy to reduce treatment delay. Future research should explore how to minimize barriers to initiation of non-medication therapy. Based on our clinical experience and previously published literature,25,26 we hypothesize that issues such as insurance coverage, concerns about time and stigma around psychological treatment options may be contributing factors.
Conclusions
Among children and adolescents with new onset continuous headache who are treated in neurology clinic, initiation of treatment is often delayed. Longer delay to treatment may be associated with worse headache outcomes. Currently used transitional and preventive therapies help a proportion of patients, although some patients also experience headache worsening or side effects. First-line treatment with either a preventive supplement or a prescription preventive is reasonable. Earlier initiation of non-medication therapies, such as CBT, may improve outcomes. Prospective studies are needed to guide clinical practice when treating NDPH.
Clinical implications
Amongst children and adolescents seen in neurology clinic for new onset continuous headache, treatment is often initiated late, yet earlier treatment is associated with better outcomes. Transitional therapies often improve but do not resolve headache and should be accompanied by preventive treatments. Preventive supplements, prescriptions and non-medication therapies are beneficial to some, but randomized trials are needed.
Supplemental Material
sj-docx-1-cep-10.1177_03331024261426562 - Supplemental material for Treatment outcomes in new daily persistent headache in children and adolescents
Supplemental material, sj-docx-1-cep-10.1177_03331024261426562 for Treatment outcomes in new daily persistent headache in children and adolescents by Nassim Abuhalaweh, Amy A. Gelfand, Morgan Evans, Blanca Marquez de Prado, Carlyn Patterson Gentile, Nichelle Raj, Andrew D. Hershey and Christina L. Szperka in Cephalalgia
Footnotes
ORCID iDs
Ethical considerations
Headache questionnaire data were collected clinically and extracted from the electronic health record into the CHOP Headache Registry with approval from the CHOP IRB, with a waiver of the requirement for informed consent.
Author contributions
Nassim Abuhalaweh: Writing - original draft; investigation; formal analysis; writing - review and editing. Amy A. Gelfand: Writing - review and editing; conceptualization. Morgan Evans: Data curation. Blanca Marquez de Prado: Data curation. Carlyn Patterson Gentile: Writing - review and editing. Nichelle Raj: Project administration. Andrew D. Hershey: Writing - review and editing. Christina L. Szperka: Writing - review and editing; conceptualization; formal analysis; investigation.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the Grant from the International Headache Society for seed funding in Child & Adolescent headache research, supplemented by funding from the CHOP CARES/Doris Duke COVID-19 Fund to Retain Clinical Scientists. Dr Szperka and Dr Patterson Gentile received research support from NIH NINDS (K23NS102521; K23 NS124986). Ms Evans was a participant in the Children’s Hospital Research Institute Summer Scholars Program (CRISSP), funded by R25HD101365 from National Institute of Child Health and Human Development, as well as the CHOP Research Institute.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/orpublication of this article: NA: None. AAG: In the last 24 months, Dr. Gelfand has received royalties from UpToDate (for authorship), and honoraria from Elsevier (for authorship), the American Academy of Neurology (for editing) and the Weill Cornell Neurology Department (for speaking). She receives a stipend from the American Headache Society or her role as Editor of Headache. She receives grant support from PCORI as a member of the Steering Committee for the REACH study and from the UCSF Resource Allocation Program as an investigator. She is also supported by a generous philanthropic donation made by Nathalie and Nicolas Giauque to the UCSF Child & Adolescent Headache Program. ME: None. BMP: None. CPG: Dr. Patterson Gentile receives salary support from the National Institutes of Health/National Institute of Neurological Disorders and Stroke (K23 NS124986) and Children's Hospital of Philadelphia Foerderer Grant. NR: None. ADH: Dr. Hershey or his institution have received compensation for serving as a consultant for AbbVie, Amgen, Biohaven, Eli Lilly, Lundbeck, Supernus, Teva, Theranica and Upsher-Smith. His institution has also received research support from Amgen, Biohaven, Eli Lilly, Theranica, Upsher-Smith, and the NIH NINDS/NICHDS. CLS: Dr. Szperka or her institution have received compensation for serving as a consultant for AbbVie, Lundbeck, and Teva. She has received personal compensation for serving on a data safety monitoring board for Eli Lilly and Upsher-Smith. She has also received research support from the NIH NINDS (K23NS102521), PCORI, and the CHOP CARES/ Doris Duke COVID-19 Fund to Retain Clinical Scientists.
Data availability
The data used for this article may be obtained from the authors with a reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.