
Abstract
Background
The International Headache Society has proposed new treatment goals for migraine prevention in real world, as a way to set higher standards of care. This study provides the first assessment of the proportion of individuals achieving them after 6 months of migraine-specific treatment with anti-CGRP monoclonal antibodies (MAbs).
Methods
This was a prospective, real-world, European multicenter study, including adults with migraine treated with anti-CGRP MAbs (EUREkA cohort). We assessed the proportions of individuals in each treatment goal category–migraine freedom (no monthly migraine days [MMD]); optimal control (< 4 MMD), modest control (4–6 MMD); insufficient control (>6 MMD)–after 6 months of treatment. We also assessed the proportion of individuals with ≥50% reduction in MMD in the insufficient control group.
Results
Of the 5818 individuals in the EUREkA cohort, 4963 had 6 months data. Of these, 82.3% (4086/4963) were females and the median age was 48.0 [40.0–55.0] years. At baseline, the median monthly headache days [MHD] and MMD were 20.0 [13.3–28.0] and 15.0 [10.0–20.0], respectively. All participants were classified as having insufficient headache control (>6 MMD) at baseline. At month 6, 6.9% (342/4963) had migraine freedom, 22.9% (1137/4963) optimal control, 24.6% (1223/4963) modest control and 45.6% (2261/4963) insufficient control. In the insufficient control group, 27.1% (613/2261) had ≥50% reduction in MMD.
Conclusions
High standards of care, defined as optimal disease control or even migraine freedom, are achieved in real-world settings with anti-CGRP MAbs in approximately 30% of individuals with a high migraine burden. These findings highlight the need to expand global access to these treatments. Future studies should explore whether initiating migraine-specific preventive treatments earlier could further reduce residual migraine days in responders, enabling a larger proportion of patients to achieve optimal disease control.
Introduction
Migraine-specific treatments, antagonizing the calcitonin-gene related peptide (anti-CGRP) have changed the scenario of migraine prevention. In fact, in real-world studies, 1 in 2 people with migraine when treated with these medications achieves more than 50% reduction in monthly headache days (MHD) with excellent tolerability. 1 The possibility of treating individuals with effective, well-tolerated, disease-specific medications can change the perspective on the standards of migraine prevention we should be aiming for, and set ambitious treatment goals for optimal outcomes in migraine care. A definition of higher standards in migraine care has been proposed by the International Headache Society (IHS) in a recent position statement. 2 Four treatment goal categories have been identified: migraine freedom (no monthly migraine days [MMD] or moderate-to-severe headache days [MSHD]); optimal control (< 4 MMD or MSHD), modest control (4–6 MMD or MSHD); insufficient control (>6 MMD or MSHD). 2 Since the definition is new, it has yet to be assessed if and to what extent migraine-specific drugs, such as anti-CGRP monoclonal antibodies (MAbs), help achieve the new standards of migraine care.
This study aims to provide the first assessment of the proportion of migraine patients achieving the IHS-defined treatment goals after 6 months of treatment with anti-CGRP MAbs using the EUREkA cohort, the largest real-world anti-CGRP cohort to date.
Methods
This is a prospective multicenter real-world study. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline 3 was followed as well as the guidelines of the International Headache Society for Real-World Evidence studies in migraine. 4 Adults with migraine treated with anti-CGRP MAbs (erenumab 70 mg or 140 mg monthly, galcanezumab 120 mg monthly + 240 mg loading dose, fremanezumab 225 mg monthly or fremanezumab 675 mg quarterly) were included. The study cohort and the methodology for data collection have been reported in a previous paper. 1 For this secondary analysis, we used the IHS definitions for treatment goal categories: migraine freedom (0 MMD); optimal control (< 4 MMD), modest control (4–6 MMD); insufficient control (>6 MMD). The primary outcome was the proportion of individuals treated with anti-CGRP MAbs in each category after 6 months of treatment. The secondary outcome was the proportion of subjects with ≥50% reduction in MMD at 6 months in the insufficient control category.
For the statistical analysis, we reported nominal (categorical) variables as frequencies (percentages), whereas the median and interquartile range (IQR) were reported for continuous variables. All analyses were performed using R (version 4.4.2).
Results
Cohort description
Thirty-five European hospitals from 7 countries participated (Spain, Italy, Portugal, United Kingdom, Germany, Norway, Poland).
Of the 5818 individuals of the EUREkA cohort, 4963 had 6 months data: 82.3% (4086/4963) were females and median age was 48.0 [40.0–55.0] years (See Table 1 for other baseline characteristics). Seventy-one-point-four percent (3546/4963) had a baseline diagnosis of chronic migraine. At baseline, the median MHD and MMD were 20.0 [13.3–28.0] and 15.0 [10.0–20.0], respectively. According to the IHS definition, all participants were classified as having insufficient headache control at baseline.
Baseline characteristics of the study cohort
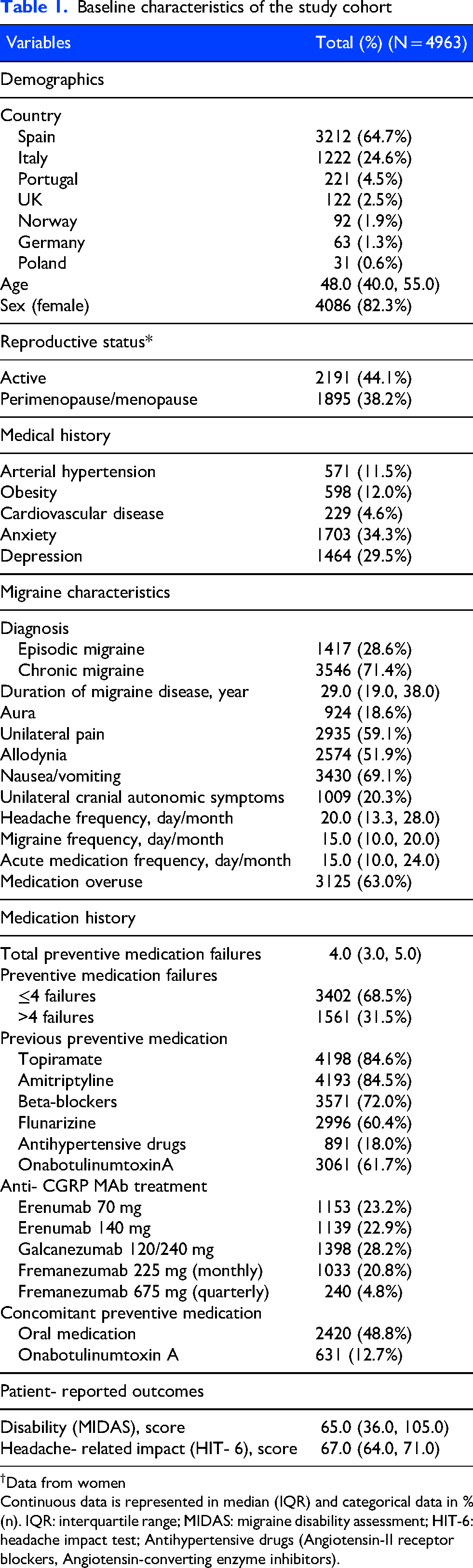
†Data from women
Continuous data is represented in median (IQR) and categorical data in % (n). IQR: interquartile range; MIDAS: migraine disability assessment; HIT-6: headache impact test; Antihypertensive drugs (Angiotensin-II receptor blockers, Angiotensin-converting enzyme inhibitors).
IHS treatment goals after 6 months of treatment
At month 6 of treatment with anti-CGRP MAbs, individuals were classified as: 6.9% (342/4963) migraine freedom, 22.9% (1137/4963) optimal control, 24.6% (1223/4963) modest control and 45.6% (2261/4963) insufficient control (Figure 1).
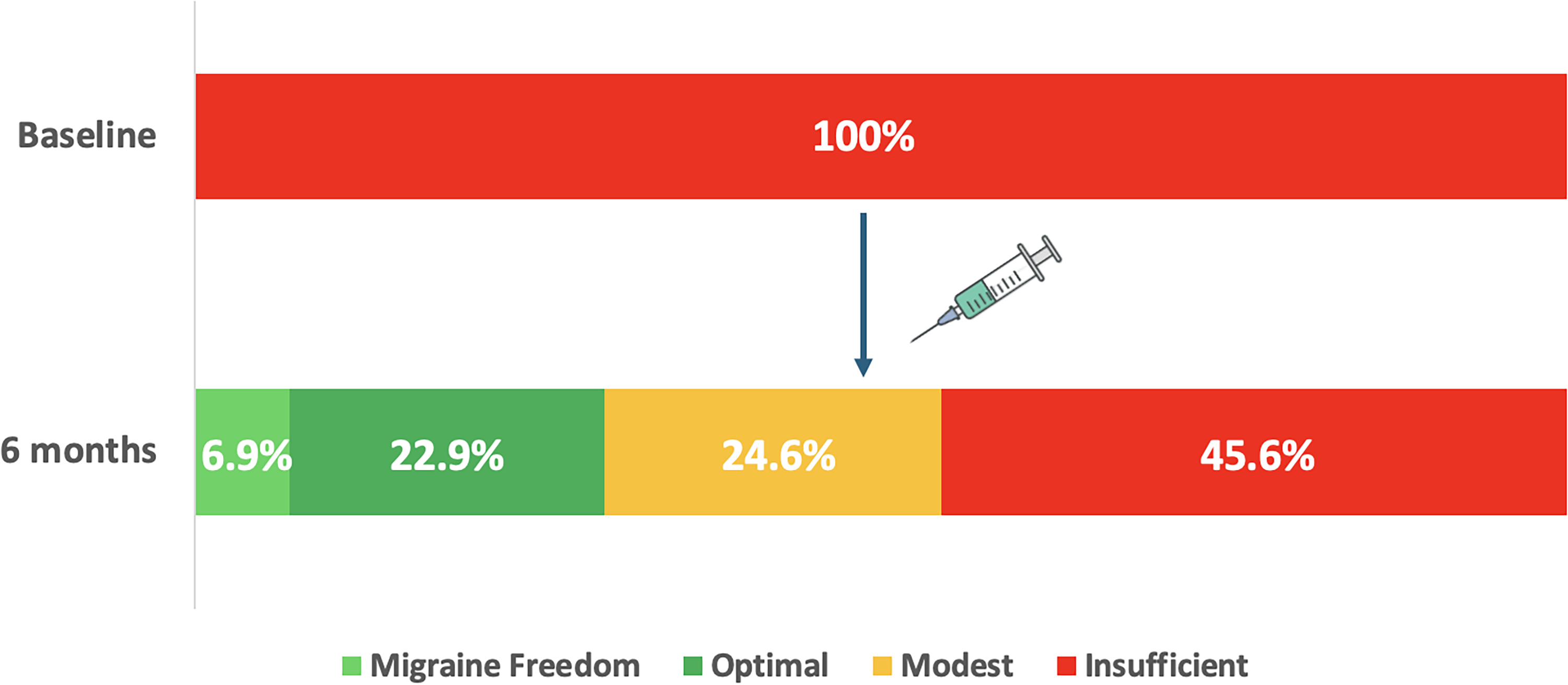
Proportions of people with migraine with insufficient, modest, optimal control and migraine freedom according to the IHS definition at baseline and after 6 months of treatment with anti-CGRP monoclonal antibodies for migraine prevention
In the insufficient control group, 27.1% (613/2261) of individuals were ≥50% responders.
Discussion
This is the first study assessing IHS-defined treatment goals in the real world and it is based on the largest cohort of migraine people (EUREkA) treated with anti-CGRP MAbs. We would like to draw attention to two important findings.
First, our migraine population experienced a high disease burden at baseline, with many participants suffering from chronic migraine, medication overuse, and multiple preventive treatment failures. 1 However, thanks to migraine-specific treatments, approximately 30% achieve optimal disease control (<4 MMD) or even migraine freedom at 6 months. These findings highlight the potential to achieve high standards of care for a significant proportion of highly disabled individuals, underscoring the need to make these treatments more widely and easily accessible on a global scale.5,6
Second, the concept of higher standards extends beyond a 50% response to treatment. In our study, approximately one in four participants with insufficiently controlled migraine after six months of monoclonal antibody therapy achieved a ≥ 50% reduction in monthly migraine days. This is because some individuals for whom anti-CGRP treatments are effective, have such a high baseline of MMD that their migraine frequency remains above the threshold for optimal control. It is reasonable to consider whether starting migraine-specific preventive treatments earlier could reduce the number of residual migraine days, thereby allowing a greater proportion of individuals to achieve optimal control. Our previous study 1 demonstrated that initiating anti-CGRP treatment earlier increases the likelihood of a response. Building on this, the current study raises the hypothesis that, among those who respond, earlier intervention could further enhance disease control. However, for some individuals, it is also possible that more time under treatment will be necessary to achieve better responses (later-responders). 7
Regarding study limitations, those related to multicenter data collection have already been addressed in our previous paper. 1 To mention, cutaneous allodynia was assessed through clinical interview rather than formal testing; however, interviews were conducted by headache specialists, which increases the reliability of the assessment. In this analysis, the main limitation is that the IHS definition was assessed at a single time point (6 months) rather than across the previous three months. However, these definitions are only “ideally” or “if possible” assessed over 3 months. 2 So, while our approach may simplify this aspect on the other it has the strength of gathering the data from a large cohort of participants, providing a preliminary picture of the new treatment goals with anti-CGRP MAbs in the real world.
Conclusion
In this largest anti-CGRP MAbs real-world cohort (EUREkA), 30% of people with a high migraine burden are able to achieve an optimal disease control (fewer than 4 monthly migraine days) or even migraine freedom with anti-CGRP MAbs, demonstrating the potential to reach high standards of care. Future studies should assess if this proportion can be increased by earlier migraine-specific preventive treatment strategies, able to ensure that, for those who respond, the residual migraine burden is reduced.
Article highlights
Anti-CGRP monoclonal antibodies provide optimal disease control (fewer than 4 monthly migraine days) or even migraine freedom at 6 months in around 30% of patients with high migraine burden in the real world
Among those with insufficient control, 27.1% still achieved ≥50% reduction in monthly migraine days
Expanding global access and exploring whether earlier preventive treatment can reduce residual burden in responders may be key strategies to achieving optimal disease control
Footnotes
Acknowledgements
Gabriella Egeo, Paola Torelli, Cinzia Aurilia, Sabina Cevoli, Bruno Colombo, Michele Trimboli, Fabio Frediani, Florindo d’Onofrio, Marco Aguggia, Antonio Salerno, Antonio Carnevale, Maurizio Zucco, Maria Albanese, Cinzia Finocchi, Angelo Ranieri, Francesco Zoroddu, Massimo Autunno, Piero Barbanti
ORCID iDs
Ethical considerations
The study was approved by the Vall d’Hebron Ethics Committee (EOM(AG)009/2023(6101)) as the coordinating center and shared with all participating centers. All participating centers gave their consent to the use of their data and, if necessary, local ethical approval to pool data was obtained. Data were anonymized and handled confidentially. No informed consent for this study was obtained from patients, considering that they had previously consented to the collection and use of anonymous data at each center, and no additional procedure, data collection or requirement was needed for the current study. The study was conducted in accordance with the declaration of Helsinki.
Patient and public involvement
Neither patients nor the public were involved in the conception or conduct of the study. No dissemination plan has been done.
Transparency statement
The manuscript is an honest, accurate, and transparent account of the study being reported. No important aspects of the study have been omitted and any discrepancies from the study as originally planned have been explained.
Consent for publication
The Corresponding Author has the right to grant on behalf of all authors and does grant on behalf of all authors, a worldwide licence to the Publishers and its licensees in perpetuity, in all forms, formats and media (whether known now or created in the future), to i) publish, reproduce, distribute, display and store the Contribution, ii) translate the Contribution into other languages, create adaptations, reprints, include within collections and create summaries, extracts and/or, abstracts of the Contribution, iii) create any other derivative work(s) based on the Contribution, iv) to exploit all subsidiary rights in the Contribution, v) the inclusion of electronic links from the Contribution to third party material where-ever it may be located; and, vi) licence any third party to do any or all of the above.
Author contributions
PPR and EC made substantial contributions to conception and study design. All authors worked for acquisition of data. EC and RMDV contributed to data analysis. All authors contributed to the interpretation of data. EC and RMDV wrote the first draft. All authors critically revised and finally approved the version to be published. All authors fully comply with and approve the version to be published.
The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: EC has received honoraria from Novartis, Chiesi, Lundbeck, MedScape, Eli Lilly, Organon, Dr Reddy's, TEVA; his salary has been partially funded by Río Hortega grant Acción Estratégica en Salud 2017–2020, Instituto de Salud Carlos III (CM20/00217). He is a junior editor for Cephalalgia.
RMDV reports no disclosures.
GE received travel grants and honoraria from Eli-Lilly, Novartis, Lusofarmaco, New Penta and Ecupharma. MMV reports no disclosures.
MMV reports no disclosures.
CNC has received honoraria for advisories, educational or commercial symposia from: Abbvie-Allergan, Kern Pharma, Chiesi, Lilly, Lundbeck, Novartis and Teva Pharmaceuticals And has participated as subinvestigator in Clinical Trials for: Abbvie-Allergan, Amgen, Biohaven, Lilly, Lundbeck, Pfizer and Teva Pharmaceuticals.
JAM has received honoraria as consultant and/or speaker for Lilly, Novartis, Teva.
GV reports no disclosures.
JRM reports no disclosures.
NFF reports no disclosures.
FSC received honoraria from Novartis, Lilly, TEVA, Abbvie.
AJ has received honoraria from Teva, Organon, and Allergan-AbbVie, as well as academic support from Lundbeck.
AMV has received honoraria from Teva, Lilly, Roche, UCB, Bial, Chiesi, Allergan, Esai, Zambon, Kern Pharma, Pfizer, Biogen Idec, Novartis, TEVA, Merck, Janssen, Neuraxpharm, Genzyme, Sanofi, Bayer, Almirall and/or Celgene.
RO reports no disclosures.
GG reports no disclosures.
YGO reports no disclosures.
JS received honoraria from Allergan, Lilly, Teva, Novartis.
GC has received honoraria from Teva
IBB received honoraria for presentations from Novartis, Lilly, Teva, Lundbeck and Abbvie.
MWP received honoraria from Pfizer, Allergan-Abbvie, TEVA, Polpharma. MWP is member of Editorial Board: The Journal of Headache and Pain.
LP received honoraria from Pfizer, Lilly, Abbvie, TEVA, Novartis.
ALR received honoraria for Abbvie, Lilly, Novartis and Teva.
IL received honoraria from Novartis, Abbvie, Teva, Eisai, Tecnifar and Bial.
LD received honoraria as a speaker for Allergan, Lilly, Teva and Lundbeck.
MRAE, received honoraria from ABBVIE, Lilly, and Novartis
AM has no COI to declare. The University Clinic Hamburg got an unrestricted scientific grant from Novartis (2019–2023)
ALB reports no disclosures
IPM has received honoraria from Allergan Teva, Novartis, Lundbeck and Eli Lilly for lecturing or participating in advisory boards; is principal investigator for phase IV trials sponsored by Novartis, Lundbeck and Teva.
CS has received personal fees for lectures/ advisory boards: Novartis, Abbvie, and TEVA.
PI received honoraria from TEVA, Novartis, Lilly, Abbvie, Lundbeck, Exeltis
ALR received honoraria from TEVA.
ABGV has received speaker honoraria and/or clinical advisor from Novartis, Lilly, TEVA, Exeltis, Chiesi, Abbvie, Pfizer and Lundbeck.
FVJ reports no disclosures
RR has received travel grants and/or honoraria for lectures or advisory boards or consultancy from Allergan/AbbVie, Betapharm, Lilly, Lundbeck, Novartis, Pfizer and Teva.
SS reports consultant, speaker, or advisory board fees from Abbott, Allergan/Abbvie, AstraZeneca, Bayer, Bristol Myers Squibb, Daiichi-Sankyo, Eli Lilly, Medscape, Medtronic, Novartis, Pfizer, Starmed, Teva, and Uriach.
ECG received honoraria from TEVA
DGA has received personal compensation for consulting/advising from the World Health Organization. Non-profit board membership in the Spanish Society of Neurology, and the European Union of Medical Specialist section of Neurology. Research funding from the Regional Health Administration (Gerencia Regional de Salud SACYL) in Castilla y Leon, Spain and Carlos III institute, Madrid, Spain. Speaker/travel grants/ clinical trials from Teva, Allergan, Amgen, Eli Lilly, Lundbeck, Novartis, and Biohaven.
JP has received honoraria from Abbvie, Lilly, Lundbeck, Novartis and Teva
RGG received honoraria from Allergan/ Abbvie, Lilly, Lundbeck, Novartis, Pfizer, Tecnifar, Teva
MHV has received honoraria for participating on advisory boards and for collaborations as consultant, scientific communications, speaker, research support as well as funding for travel and congress-attending expenses for Abbie-Allergan, Novartis, Lundbeck, Lilly, Almirall, Chiesi, Esai, Exeltis, Kern Pharma, Menarini, TEVA and Zambon. His research group has received research grants from Abbie-Allergan; and has received funding for clinical trials from Lilly, Novartis, TEVA.
JRV reports no disclosures
JVR received honoraria from Novartis, Abbvie, Lilly, TEVA, Lundbeck.
VO reports no disclosures
SSL received honoraria from Allergan, Almirall, Amgen, Chiesi, Eisai, Exeltis, Lilly, Lündbeck, Novartis, Pfizer y Teva.
MGS has received honoraria and been involved in research, education and advisory boards with Teva, Lily, Novartis and Abbvie.
CT received personal fees for participating in advisory or for speaking at scientific events from AbbVie, Allergan, Biohaven, Dompé, Eli Lilly, Lundbeck, Novartis and Teva. CT has received research funding from the European Commission, the Italian Ministry of Health and Migraine Research Foundation.
JDT has received honoraria as consultant and/or speaker for Lilly, Novartis, Teva.
SDI has received honoraria for advisories, educational or commercial symposia from: Abbvie-Allergan, Fundació Universitat-Empresa, Ipsen Pharma, Kern Pharma, Lilly, Lundbeck, MSD-Organon, Novartis and Teva Pharmaceuticals And has participated as PI in Clinical Trials for: Abbvie-Allergan, Alder, Amgen, Biohaven, Ipsen Pharma, Lilly, Lundbeck, Pfizer and Teva Pharmaceuticals
CGO participated in clinical trials from Novartis, St Jude Medical, Lilly, Lundbeck; TEVA, Biohaven, Pfizer. CGO received honoraria as consultant for Novartis, Lilly, Allergan-abbvie, Lundbeck, TEVA, Pfizer. CGO received honoraria as speaker for Allergan-Abbvie, TEVA, Novartis,Lilly, Chiesi, MSD, Almirall.
PB reports personal compensation for consulting, serving on a scientific advisory board, speaking, research support, collaborated for clinical trials, or other activities with Abbvie, Alder, Allergan, Amgen, Angelini, Assosalute, Bayer, Biohaven, ElectroCore, Eli-Lilly, Fondazione Ricerca e Salute, GSK, Lundbeck, Lusofarmaco, 1MED, MSD, New Penta, Noema Pharma, Novartis, Pfizer, Stx-Med, Teva, Visufarma, Zambon and serves as President with Italian Association of Headache Sufferers.
PPR has received, in the last three years, honoraria as a consultant and speaker for: AbbVie, Dr Reddy's, Eli Lilly, Lundbeck, Medscape, Novartis, Organon Pfizer and Teva. Her research group has received research grants from AbbVie, Novartis and Teva; as well as, Instituto Salud Carlos III, EraNet Neuron, European Regional Development Fund (001-P-001682) under the framework of the FEDER Operative Programme for Catalunya 2014–2020–RIS3CAT; has received funding for clinical trials from AbbVie, Amgen, Biohaven, Eli Lilly, Novartis, Pfizer, Teva. She is the Honorary Secretary of the International Headache Society. She is in the editorial board of Revista de Neurologia. She is an associate editor for Cephalalgia, Headache, Neurologia, The Journal of Headache and Pain and Frontiers of Neurology. She is a member of the Clinical Trials Guidelines Committee of the International Headache Society. She has edited the Guidelines for the Diagnosis and Treatment of Headache of the Spanish Neurological Society. She is the founder of ![]() . PPR does not own stocks from any pharmaceutical company.
. PPR does not own stocks from any pharmaceutical company.
DGA reports no disclosures.
RO reports personal fees from Eli Lilly, Novartis, Teva, and Pfizer, and non-financial support from Novartis, Teva, and Allergan/AbbVie.
CT has received honoraria for lectures from TEVA, Lundbeck and for advisory boards from TEVA. He has received travel support from TEVA and Lundbeck.
IFL reports no disclosures.
ASS received honoraria from TEVA.
AKH has received honorarium from TEVA Pharmaceuticals for a lecture.
BNV reports no disclosures.
HB received honoraria from Novartis, Teva and Lundbeck.
NPRP received honoraria from ABBVIE, Lilly, and Novartis
BFP reports no disclosures.
CF received honoraria from Novartis and Abbvie.
AAL received honoraria for Abbvie, Lilly, Novartis and Teva.
EMS received a grant from the Portuguese Headache Society, supported by Teva.
SB reports no disclosures.
PRA reports no disclosures.
AC reports no disclosures.
VJG reports no disclosures relevant to the manuscript.
LGD reports no disclosures relevant to the manuscript
MTF has received honoraria from Allergan-AbbVie, Novartis, Chiesi and Teva.
AA has received honoraria from Allergan-AbbVie, Novartis, Chiesi.
PT received grants and honoraria from Novartis, Teva, Eli-Lilly and Allergan
CA received travel grants from FB-Health, Lusofarmaco, Almirall, Eli-Lilly Novartis and Teva
SZ reports no disclosures
RLP reports no disclosures
MJRC reports no disclosures
RDI received speaker honoraria from Eli-Lilly, TEVA and Lundbeck.
GS received personal fees as speaker or advisory board from Eli Lilly, Novartis, Teva, Lundbeck, Pfizer.
SB has received honoraria from Teva.
HCO reports no disclosures
JW reports no disclosures relevant to the manuscript
SA reports no disclosures
IKZ reports no disclosures
AEU reports no disclosures.
AGG declares no disclosures.
SC has received honoraria from Teva, Lilly, Roche, UCB, Bial, Chiesi, Allergan, Esai, Zambon, Kern Pharma, Pfizer, Biogen Idec, Novartis, TEVA, Merck, Janssen, Neuraxpharm, Genzyme, Sanofi, Bayer, Almirall and/or Celgene.
IM reports no disclosures
EP reports personal fees from Novartis, Teva and Lilly.
VGQ declares no disclosures.
ALGP Research funding from the Regional Health Administration (Gerencia Regional de Salud SACYL) in Castilla y Leon, Spain. Speaker/travel grants/ clinical trials from Teva, Allergan, Amgen, Eli Lilly, Lundbeck, Novartis, Pfizer and Biohaven.
IM reports no disclosures.
JPS reports no disclosures.
VC reports no disclosures.
AS has received honoraria for advisory boards and lectures from Allergan/AbbVie, Hormosan, Lilly, Lundbeck, Novartis, Sanofi, Teva.
AGM has received speaker honoraria from TEVA, Lilly and Altermedica. Her salary has been partially funded by Río Hortega grant Acción Estratégica en Salud from Instituto de Salud Carlos III (CM21/00178) and Juan Rodés fellowship, Subprograma Estatal de Incorporación de la Acción Estratégica en Salud 2023 (JR23/00005). She is the principal investigator of the Research Project funded by Instituto de Salud Carlos III (grant number PI24/01085) and co-funded by FEDER and FSE. She is board member of the Future Headache Experts of the European Headache Federation, secretary of the Residents and Research Fellows (RRFS) of the European Academy of Neurology (EAN) and coordinator of the junior Headache Group of the Spanish Society of Neurology (jGECSEN).
SQ has received speaker honoraria from Novartis, Lilly and Exeltis
MSR has received consulting fees and honoraria for lectures/presentations from Eli Lily, Lundbeck, Novartis, Teva and Pfizer. Intellectual as Secretary of the European Headache Federation, Review Editor on the Editorial Board of Headache and Neurogenic Pain (specialty section of Frontiers in Neurology). Margarita Sanchez-del-Rio serves as a member of the Board of Directors in the European Headache Federation.
ET has received personal fees for lectures/ advisory boards: Novartis, Eli Lilly, Abbvie, TEVA, Roche, Lundbeck, Pfizer, Biogen. Consultant for and owner of stocks and IP in Man & Science. Stocks and IP in Nordic Brain Tech and Keimon Medical. Non-personal research grants from EU, Norwegian Research Council, Dam foundation, KlinBeForsk. Commissioned research (non-personal): Lundbeck, Pfizer.
BVP received honoraria from ABBVIE
AOD received honoraria from ABBVIE, Lilly, Teva, Novartis ”
MR received honoraria from Lilly, Novartis.
AFR reports no disclosures.
YVE reports no disclosures.
SC received travel grants, honoraria for advisory boards, speaker panels or clinical investigation studies from Novartis, Teva, Lilly, Allergan, Abbvie, Ibsa, Amgen, Angelini and Lundbeck;
BC received grants and honoria from Eli-Lilly, Novartis, Teva;
MT has no disclosures to declare;
FF has received fees for participation on advisory boards, speaker honoraria or consulting activities from Angelini, Cristalfarma, Ecupharma, IBSA, Lundbeck, Novartis, PIAM, Teva;
FdO received travel grant, honoraria as a speaker or for partecipating in advisory boards from Novartis, Teva, Neopharmed Gentili, Qbgroup srl, K link srl and Eli-Lilly;
MA received grants from Novartis and Lilly;
AS has no disclosures to declare;
AC has no disclosures to declare;
MZ received travel grants and honoraria from Novartis;
MA received travel grants and honoraria from Novartis, Teva, Eli-Lilly, Abbvie Allergan, Pfizer, Organon and Lundbeck;
CF received grants and honoraria from Novartis, Eli Lilly, TEVA, AIM group;
AR received travel grants and honoraria from Teva and Eli-Lilly;
FZ has no disclosures to declare;
MA has no disclosures to declare.
Data availability statement
All data are available and any anonymized data will be shared upon reasonable request from any qualified investigator.
Open practices
Not applicable