
Abstract
Background
It has long been proposed that some individuals with migraine are especially prone to experience headache on weekends, however, results have been contradictory. Electronic headache diaries offer the possibility to analyze this question more thoroughly in larger populations.
Methods
Two non-overlapping samples of individuals with migraine from the DMKG-App electronic headache diary were investigated. Cluster analysis and logistic regression were performed to study existence, prevalence and predictive factors of weekend headache.
Results
We included 1793 and 5840 patients with ≥35 headache day entries in the two samples (“registry sample” and “app-only sample”), respectively. In both samples, cluster analysis identified a cluster of patients with headache occurring preferably on weekends, accounting for 14–15% of all patients, and 18% of individuals with episodic migraine. Compared to the three other clusters identified (an early week cluster, a midweek cluster and a flat cluster without preference for a specific day), the weekend cluster was more frequent in working patients (p < 0.001, OR = 3.57 to 3.97) and in patients with lower headache frequencies (p < 0.001, OR = 0.86). A small association with older age (p < 0.001, OR = 1.01) was limited to the app-only sample. Longitudinal analysis showed that headache patterns of single patients were variable over time.
Conclusions
Results from two large samples corroborate that there is a subgroup of individuals with migraine prone to weekend headache. Association with working status supports the notion that release from stress could be a trigger factor in these patients, although change in sleep, caffeine and alcohol intake and other factors might also contribute.
Background
It has long been recognized that some individuals with migraine experience their headache attacks preferably on weekends.1–3 While a weekend preponderance may at first seem paradoxical for a (partially) stress-related condition, several provoking factors have been proposed, such as release from work stress, and change in sleep patterns and in caffeine and alcohol intake. 4 One study suggested that in patients with high habitual caffeine consumption, weekend headache may be related to caffeine withdrawal caused by sleeping in on weekends 3
However, previous studies on the existence and prevalence of weekend headache in individuals with migraine have yielded conflicting results. While early chart reviews and questionnaire studies suggested existence of weekend headache,1,3 smaller headache-diary based studies did not identify a clear predilection for a specific day of the week for migraine attacks5–7 or found a non-weekend preference. 8 Emergency department presentations for migraine in a Turkish study were more frequent on Saturdays and Sundays, while in Spain headache presentations peaked on Mondays and Tuesdays.9,10 Also, patterns of emergency department presentations may be influenced by additional factors such as work schedules and availability of other forms of headache care. One study analyzed data of 1085 individuals with migraine from a German electronic headache diary and found that Saturday was the single most frequent day with headache per patient, and that 18% of the patients showed this pattern. 11 Also, a review including 7 studies found that more studies identified Saturday as the most frequent day with migraine than any other day. 4 Taken together, there is moderate evidence that a subgroup of patients with migraine may exhibit weekend headache. It is, however, an open question if there are individual factors predicting weekend headache.
Data from electronic headache diaries offer the opportunity to study the issue of weekend headache more thoroughly. Especially, as weekend headache would be hypothesized to affect only a subgroup of individuals with migraine, cluster analysis of large populations may allow to identify patients belonging to this subgroup. Therefore, we investigated two separate datasets from the electronic headache diary operated by the German Migraine and Headache Society (“Deutsche Migräne- und Kopfschmerzgesellschaft”, DMKG-App) and used cluster analysis and logistic regression to study existence, prevalence and predictive factors of weekend headache in individuals with migraine.
Methods
This analysis used data from the smartphone headache diary application of the DMKG-App, available in Germany for Android and iOS since June 2020. It is part of the larger project “DMKG Headache Registry” 12 that has been approved by the ethics committee of the Ludwig-Maximilians-University Munich (Nr. 20-004), complies with European and German Data Protection laws and is registered with the German Clinical Trials Register (DRKS 00021081). Each participant consented with use of their data for headache research in anonymized form. Consent was obtained in digital form within the user account on the DMKG Headache Registry platform. This study is reported in accordance with the STROBE guidelines for observational studies.
The DMKG-App records headache days and non-headache days. Only headache days were used for the present analysis. Headache and non-headache days can be documented for a maximum of 14 days retrospectively, as a compromise between usability and avoiding recall bias.
The analysis includes all patients ≥16 years old, with at least 35 recorded headache days and at least 80% adherence (≤20% of days with missing entries between the first and last day of app use) in the DMKG-App (data closure January 13, 2025). Two non-overlapping samples were defined by classifying patients also participating in the full version of the DMKG Headache Registry (with participation of the treating physician) as the “registry sample” and patients using only the DMKG-App as the “app-only sample”. For the registry sample, a migraine diagnosis, documented within the DMKG Headache Registry by the treating physician according to ICHD-3 13 criteria was mandatory. For the app-only sample, at least 5 migraine days documented in the DMKG-App were required. A headache day was classified as a migraine day if it fulfilled ICHD-3 criteria B, C and D for migraine without aura, if a migraine aura was recorded, or if a triptan was used for acute therapy with a moderate or good effect. Documentation of migraine symptoms is not mandatory in the DMKG-App, so apart from requiring at least 5 migraine days for the migraine diagnosis, the main analysis did not further consider migraine vs. non-migraine days. However, a sensitivity cluster analysis including only migraine days was performed.
Statistical analysis
Statistical analysis was done in R (version 4.4.2). P < 0.05 was considered significant. Comparison for multiple comparisons was performed using Bonferroni correction, and corrected p values (pc) are reported. Chi2 tests were used to compare frequencies.
For cluster analysis of headache patterns over the days of the week, we chose k++ means clustering which is a robust, euklidean-distance based iterative method with improved cluster center initialization, well suited for detection of structurally similar clusters in large datasets. 14 The main weakness of k++ means clustering is its sensitivity to outliers. Therefore, we preceded k++ means clustering by outlier elimination using hierarchical single link clustering. For outlier elimination, subjects with a single link height exceeding the median plus 3 standard deviations of the single link heights of all subjects were eliminated. 15 The determination of the best number of clusters can be challenging. In the present study, the elbow method revealed a slight elbow at 4 clusters (Supplementary Figure 1). In addition, clustering with 4 clusters resulted in stable, reproducible and clinically meaningful clusters in two different samples, so we decided on using 4 clusters. The ratio of the between sum of squares (BSS) and the total sum of squares (TSS) was used as goodness of fit criterion, where a BSS/TSS ratio of 1 would indicate perfect fit. However, there are no generally accepted thresholds for BSS/TSS ratios to indicate a sufficient or good goodness of fit. 16 Logistic regression was used to investigate predictors of cluster allocation. For both samples, the prediction by age, gender, headache frequency, medication overuse and days lost at work was evaluated as determined from app data and data captured at registration for app use. The registry sample additionally provides data from a headache questionnaire, allowing investigation of working status, use of migraine preventive medication, and depression, anxiety and stress scores from the depression, anxiety and stress scales (DASS 17 ).
To assess if patients change clusters over time, we included only patients with at least 140 headache day entries and performed cluster analysis on those patients. Subsequently, the 140 days were divided into 4 segments of 35 headache days, and each segment was classified as belonging to one of the 4 clusters using the Euklidean distance to the cluster center.
Results
A total of 1793 patients were included in the registry sample and 5840 in the app-only sample. Characteristics of the study population are listed in Table 1. In the registry sample, a median of 168 headache day entries per patient were analyzed (range 35–1549), amounting to a total of 410,894 headache days, while in the app-only sample, the median was 92 days (range 35–1561, total: 752,521).
Characteristics of the study population.
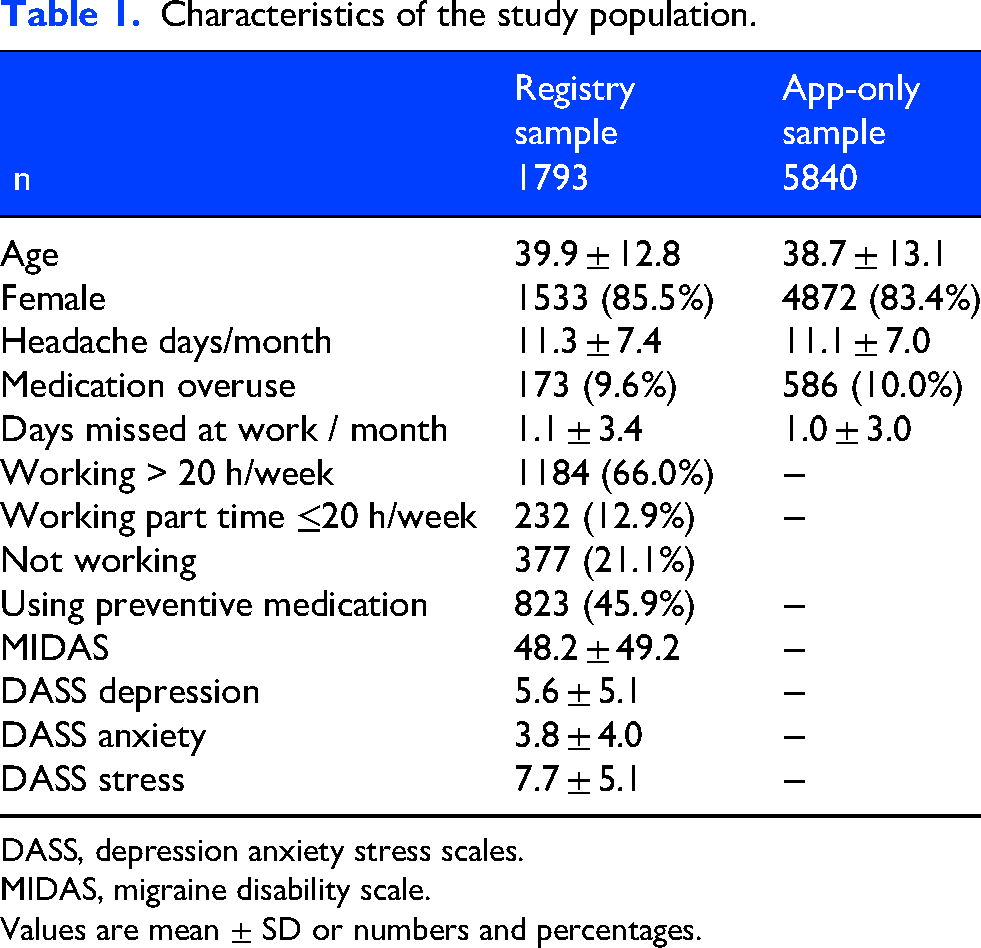
DASS, depression anxiety stress scales.
MIDAS, migraine disability scale.
Values are mean ± SD or numbers and percentages.
Overall distribution of headache days
For an initial overview, we averaged the occurrence of headache on each day of the week per patient over all patients (Figure 1(a)). The differences between days were significant (registry sample: chi2 = 15.0, p = 0.020, app-only sample: chi2 = 23.1, p < 0.001), but absolute differences were small. In the registry sample, Saturday was the most frequent day with headache, while Wednesday was most frequent in the app-only sample.
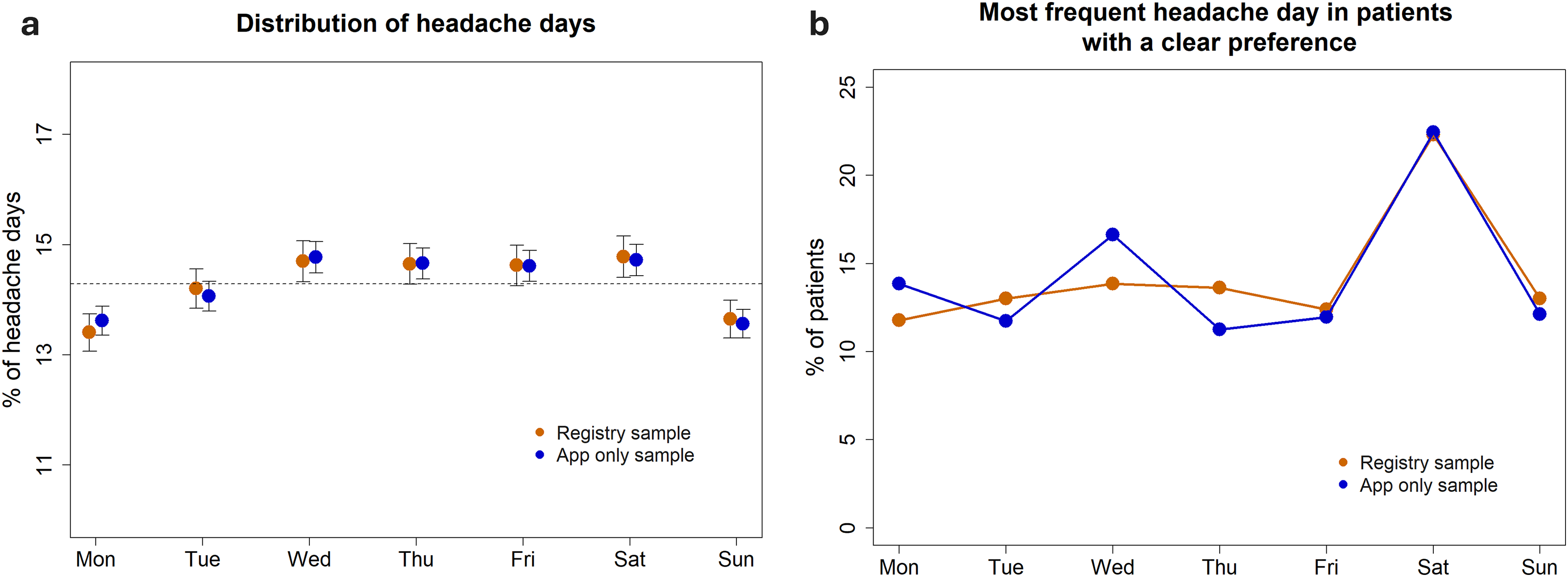
Distribution of headache days over the days of the week. Left, absolute distribution (mean ± standard error of the mean). Right, % of patients with most frequent headache per day, with analysis limited to the subgroup of patients with a clear preference (more than 20% of headache days on the same day of the week).
In a second step, we focused on the subgroup of patients with a relatively clear preference of experiencing headache on a specific day of the week (more than 20% of all headache days on the same day of the week, registry sample: n = 484, app-only sample: n = 2063) and determined the day of the week with most headache days for every patient. In this analysis, patients with a Saturday preference significantly exceeded all other days, accounting for 22.3–22.4% of the patients (registry sample: chi2 = 26.5, p < 0.001, app-only sample: chi2 = 141.6, p < 0.01, Saturday vs. all other days: all pc < 0.01, Figure 1(b)).
Cluster analysis
Results of the final cluster analysis are shown in Figure 2. Resulting clusters were similar between the registry sample and the app-only sample. BSS/TSS ratios were 0.534 and 0.531 in the registry sample and the app-only sample, respectively. In both samples, clustering identified a cluster with predominance of headache on weekends, especially Saturday and Sunday, encompassing 14.3–14.8% of the patients. In addition, an early week cluster (14.6–18.6%), a midweek cluster (17.5–20.7%) and a flat cluster without preference for a specific day of the week (45.9–53.6% of the sample) were identified. In the weekend cluster, the average probability of having a headache on a Saturday was 1.82–1.92 times as large as having a headache on a Tuesday (the day with least headache probability in this cluster).
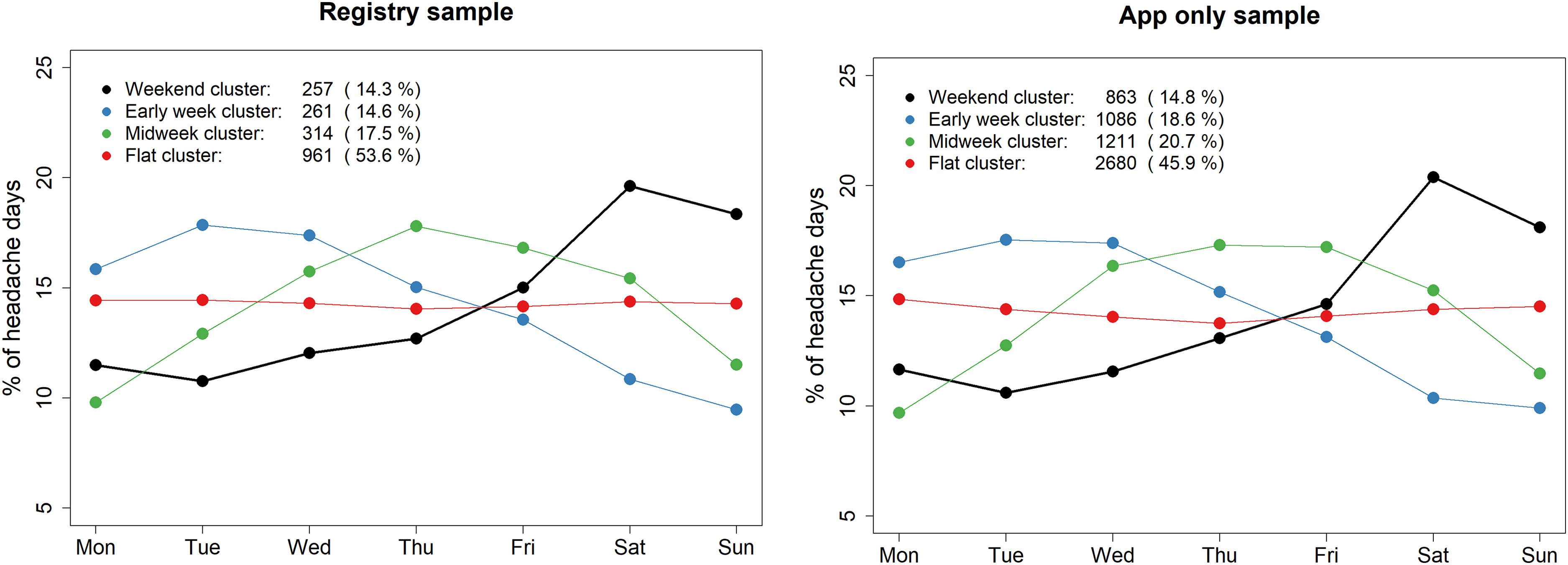
Cluster analysis of weekly headache patterns.
There was a strong dependency of cluster allocation from headache frequency, with the flat cluster becoming more frequent and all other clusters decreasing with increasing headache frequency (Figure 3). When separately looking at episodic and chronic migraine, the weekend cluster accounted for 17.6–18.1% and 2.7–3.2% of the patients, respectively. Proportions for the other clusters are listed in Supplementary Table 1.
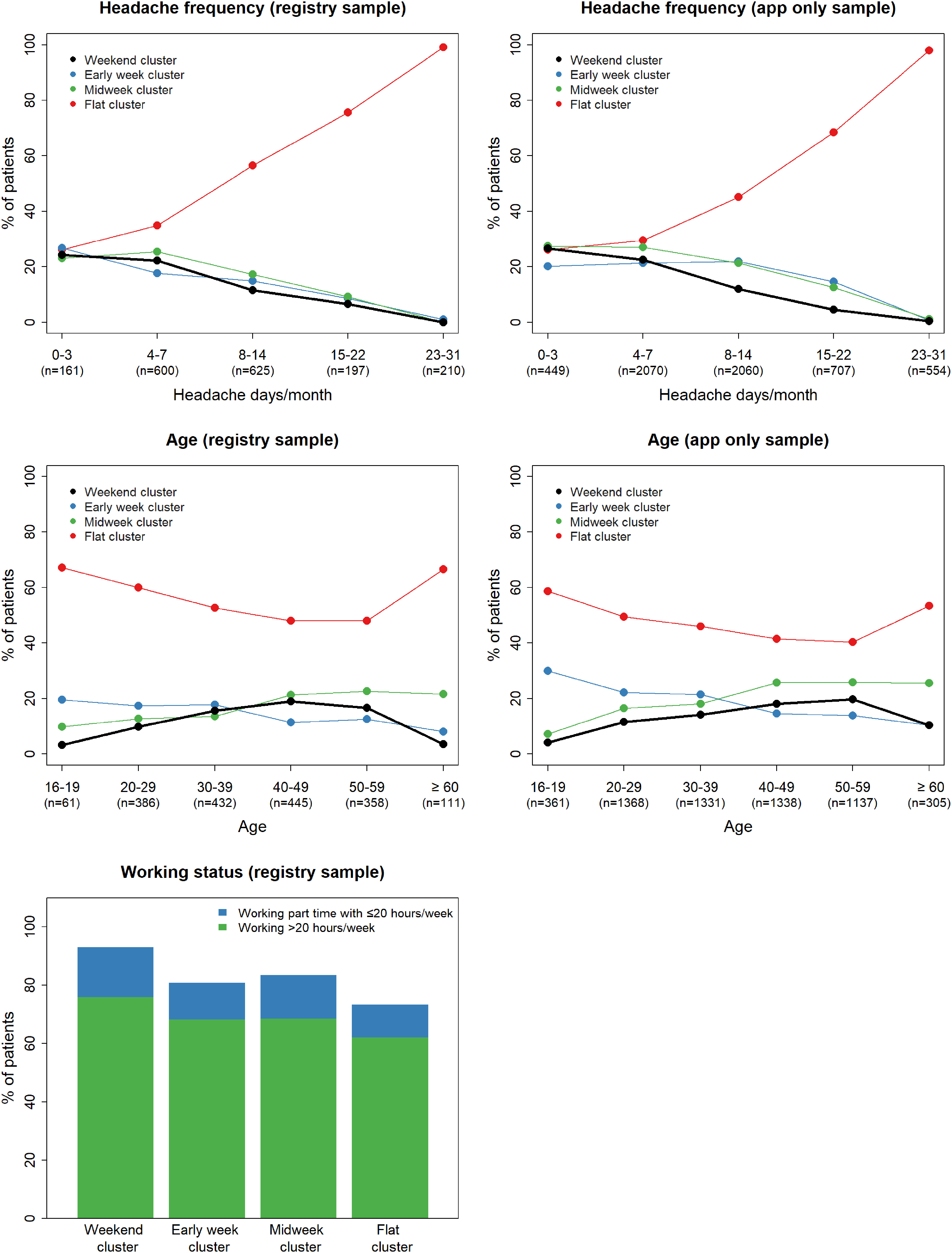
Associations of weekly headache pattern clusters. Associations with headache frequency (top row), age (middle row) and working status (bottom).
A sensitivity analysis limited to migraine days (thus necessarily limited to a smaller subgroup of participants) was performed and resulting clusters are shown in Supplementary Figure 2. Again, in both samples, clustering identified a weekend cluster, accounting for 14.1 and 19.7% of participants in the registry and app-only sample, respectively.
Predictors of weekend headache
We tested for prediction by age, gender, headache frequency, medication overuse, days lost at work and (only in the registry sample) working status, preventive medication and DASS scores. Descriptive statistics are listed in Table 2.
Characteristics within the 4 weekly headache patterns.
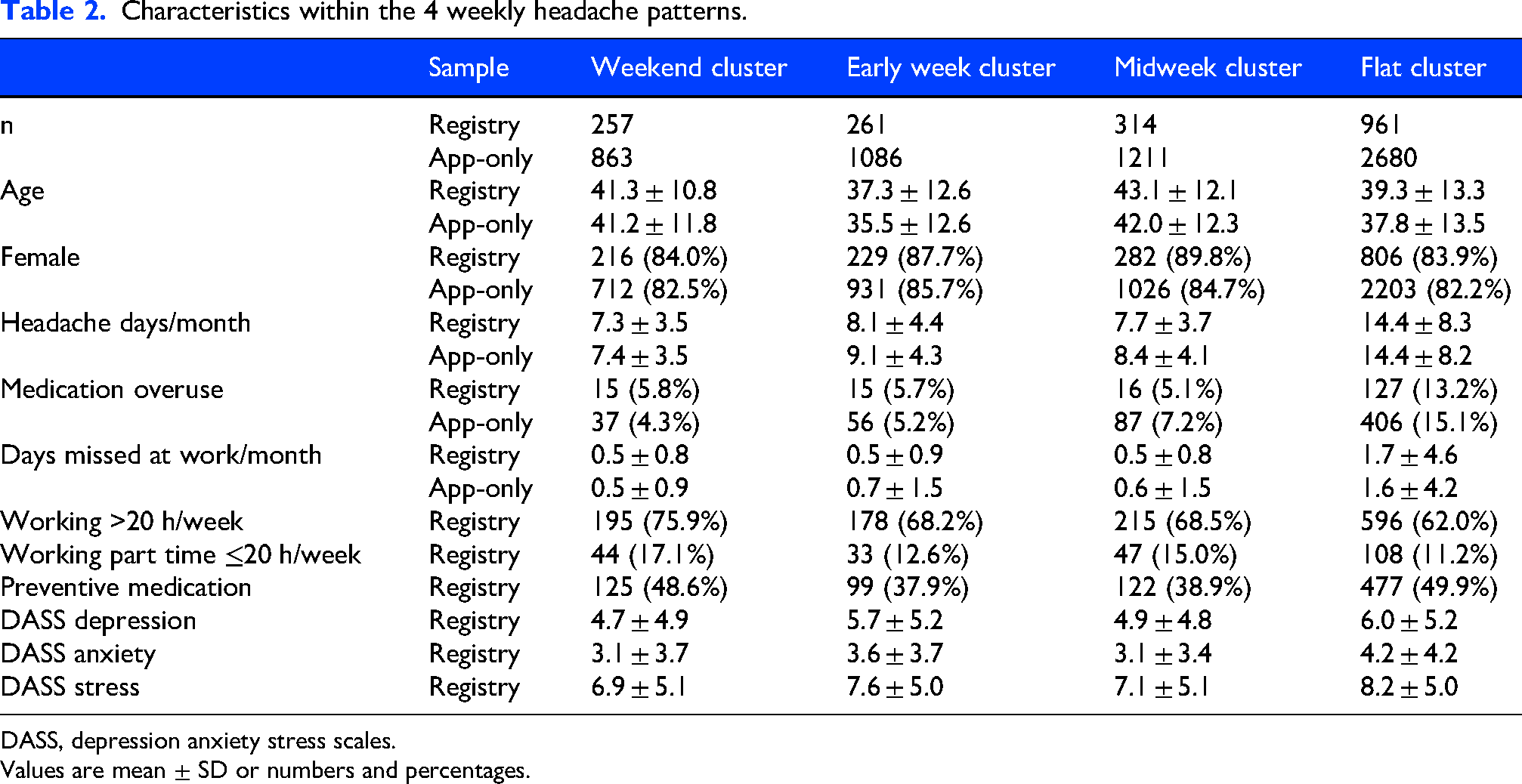
DASS, depression anxiety stress scales.
Values are mean ± SD or numbers and percentages.
Details of the logistic regression are shown in Table 3. The overall regression was significant (registry sample: chi2 = 160.2, df = 11, p < 0.001; app-only sample: chi2 = 417.6, df = 5, p < 0.001), but the explained variance according to Nagelkerkès R2 was small (R2 = 0.15 and 0.12, respectively). Both in the registry sample and the app-only sample, lower headache frequency predicted allocation to the weekend headache cluster (both p < 0.001, OR for headache frequency = 0.86). In addition, working >20 h/week and even working part time with ≤20 h/week were strong predictors (both p < 0.001, OR = 3.57 and 3.97, respectively). Older age had a small effect limited to the app-only sample (p < 0.001, OR = 1.01) and medication overuse was a predictor only in the registry sample (p = 0.045, OR = 1.92). Main differences between the weekend cluster and the other clusters are illustrated in Figure 3.
Prediction of weekend headache: results of logistic regression.
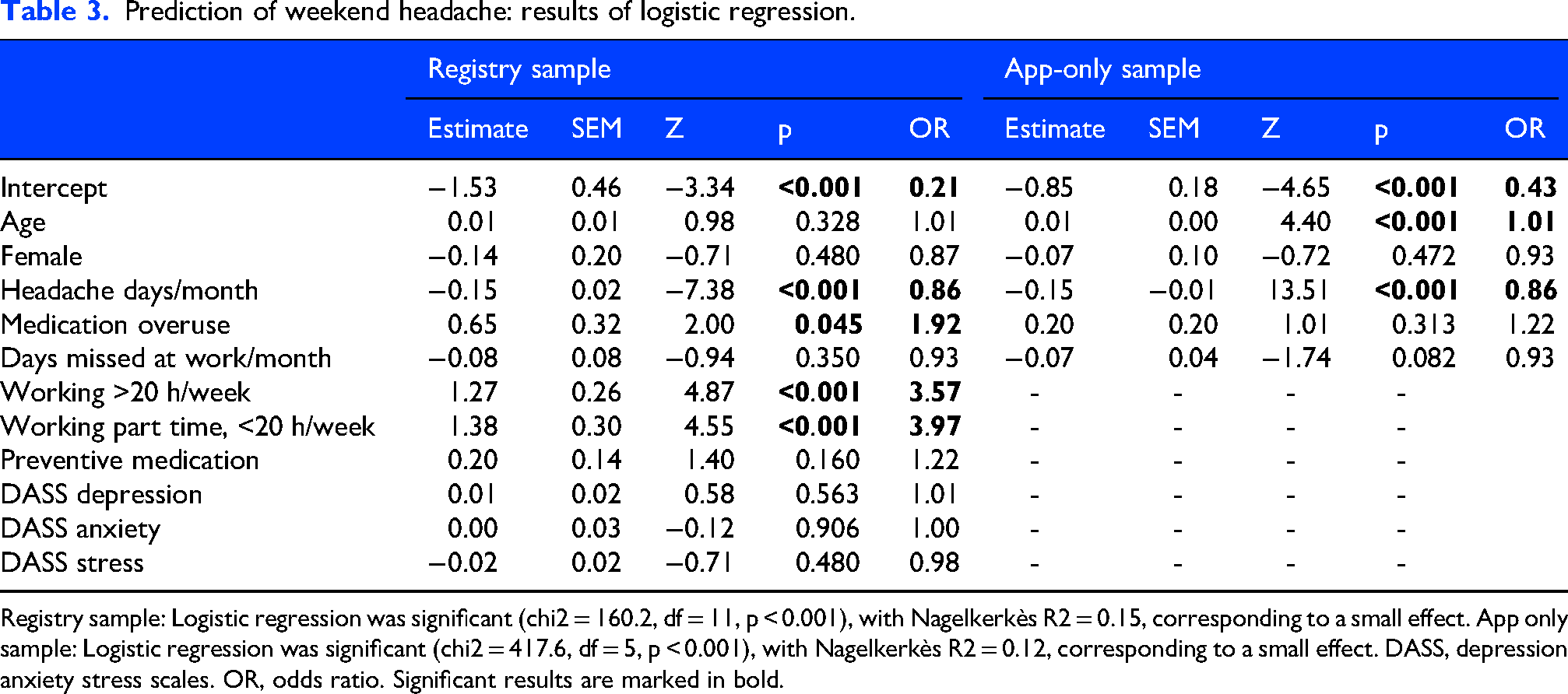
Registry sample: Logistic regression was significant (chi2 = 160.2, df = 11, p < 0.001), with Nagelkerkès R2 = 0.15, corresponding to a small effect. App only sample: Logistic regression was significant (chi2 = 417.6, df = 5, p < 0.001), with Nagelkerkès R2 = 0.12, corresponding to a small effect. DASS, depression anxiety stress scales. OR, odds ratio. Significant results are marked in bold.
As higher headache frequencies were strongly associated with belonging to the flat cluster (see Figure 3 and below), we further tested prediction of weekend headache after excluding flat cluster patients. Lower headache frequency (registry sample p = 0.049; app-only sample p < 0.001, OR = 0.95 and 0.92) and working >20 h/week or working part time with ≤20 h/week remained predictors of weekend headache (both p < 0.001, OR = 2.73 and 3.11). Older age still was a small predictor limited to the app-only sample (p < 0.001, OR = 1.01).
Predictors of other headache patterns
Results are only briefly summarized and focused on the main effects. Details can be found in Table 2 and Supplementary Tables 2–4. All regressions were significant at p < 0.001. Nagelkerke's R2 was between 0.07 and 0.14 for the early week cluster and the midweek cluster, and somewhat higher in the flat cluster (0.25–0.32).
Patients with higher headache frequencies were more often found in the flat cluster (both samples p < 0.001, OR = 1.18–1.20) while patients with lower headache frequency more often belonged to one of the two other clusters (early week cluster: both p < 0.001, OR = 0.90–0.93; midweek cluster: both p < 0.001, OR = 0.89–0.91).
In addition, there were small effects for younger age in the early week cluster (both p < 0.001, OR = 0.97–0.98) and for older age in the midweek cluster (both p < 0.001, OR = 1.02–1.03). Female gender predicted allocation to the midweek cluster (p = 0.005 and p = 0.022, OR = 1.18 and 1.24). The flat cluster was predicted by a not working status (>20 h/week and working part time with ≤20 h/week: both p < 0.001, OR = 0.50) and by using preventive medication (p < 0.001, OR = 1.43).
Change of headache pattern over time
We included 1027 patients from the registry sample with at least 140 headache day entries in this analysis. In the next step, 35-headache-day segments (4 per patient) were classified as belonging to one of the 4 clusters as detailed in methods. A total of 468 of these patients had at least 1 segment classified as belonging to the weekend cluster. Of these, 201 (42,9%) had ≥2 segments within the weekend cluster, 69 (14.7%) had ≥3 segments within the weekend cluster and only 16 (3.4%) were classified as belonging to the weekend cluster throughout all 4 segments. Results for the other three clusters are shown in Supplementary Table 5.
Discussion
The main result of the study was that there is a subgroup of individuals with migraine who exhibit a weekend headache pattern. In a group of rather severely affected individuals with migraine (11 ± 7 headache days/month), this accounted for 14–15% of the patients, increasing to 18% when analysis was limited to episodic migraine. Patients belonging to the weekend headache cluster had less headache days per month and were more likely to be working than patients of the three other clusters (flat cluster, early-week cluster, midweek cluster). However, headache patterns changed over time in many patients.
Regarding the single most frequent day of the week with headache per patient, results were very similar to a previous electronic headache diary analysis from Germany, identifying Saturday as the most frequent and Wednesday as the second most frequent day. 11 When analysis was limited to patients with a clear preference for a specific day of the week, Saturday was by far the single most frequent day with headache per patient.
To the best of our knowledge, this is the first study using cluster analysis to identify weekly headache patterns. It turned out that different patterns exist; a 4-cluster solution seemed clinically reasonable and was reproduced in two non-overlapping samples. The existence of individually different headache patterns and might be the reason why earlier, smaller studies could not identify a single clear pattern. In our analysis, the weekend headache pattern accounted for 14–15% of patients. This is similar to a previous questionnaire study, where 22% of 151 patients reported a weekend headache pattern 3 and a previous headache diary study, where the most frequent headache day was Saturday in 18% of the patients. 11 In the present study, weekend headache was more frequent in patients with less headache days and in working patients. It must be considered that part of this effect might be due to patients recording headache more reliably on their free days, compared to workdays, which would need to be studied separately. However, our results also align with data showing that release from stress (“let-down”) might be a headache trigger in a subgroup of patients.4,18 Of course, the change from workdays to weekend might also entrain other possible trigger factors of migraine such as irregular sleep, and change in caffeine and alcohol intake, or even interactions between these, like sleeping in leading to caffeine withdrawal. 3 A small placebo-controlled study suggested that caffeine withdrawal can indeed induce migraine attacks. 19 Interestingly, while sleep disturbances and alcohol consumption are among the most frequent trigger factors for migraine indicated by patients, 20 diary studies have shown a limited influence,21,22 maybe due to migraine triggers being individually very different and/or susceptible persons avoiding these triggers. On the other hand, the flat cluster without a weekly pattern was associated with not working, which might be a further hint towards weekend headache being work-associated. The early week pattern and midweek pattern were not associated with working status. Maybe these are associated with specific work patterns not captured in the present study. Data from the 1980s and 1990s suggested that weekend headache is relatively more frequent in males than in females.1,3,23 This could not be corroborated in the present study, which might be due to the fact that females are now more often employed than previously.
Overall, apart from working status (discussed above) and higher headache frequency (which unsurprisingly was a strong predictor of the flat cluster, as frequent headache offers less possibility to express a specific weekly pattern), there were few predictors of cluster allocation. The early week cluster might be regarded as the mirror image of weekend headache and was more frequent in younger patients. One could hypothesize that younger patients might have a more excessive disruption of sleep patterns on weekends and may party more on weekends. Sleep deficit and hangover might then trigger a migraine attack on Mondays. However, this remains purely speculative as we do not have data on sleep patterns and weekend activities, and effects of sleep disturbances and alcohol on migraine are inconclusive (see above). Alternatively, these patients may represent a subgroup having their attacks triggered by onset of stress (e.g., working stress) on Mondays. 24 Interestingly, a prospective study in 60 children, on average 11,8 years old, found more headaches during the week than on weekends. 25
In total, prediction of cluster allocation by the investigated variables was small, showing that other individual factors must play an important role. It seems unlikely that endogenous infradian rhythms are responsible for weekly headache patterns. More probably, individual reactions to work patterns and social activities related to specific days of the week play a role. 4 Assessing weekly habits and work patterns in more detail might have allowed to better explain cluster allocation. In addition, there might be genetic factors determining the individual reaction to stress and change in daily patterns. Our data also show that weekly headache patterns are not fixed, as most patients change between clusters over time. Likely, many factors including lifestyle changes can affect headache patterns over time. Assuming that work has an important influence, shift work and vacations could also play a role that was not assessed in the present study.
Strengths and limitations
It is an important strength of the present study that it investigated two non-overlapping large datasets of prospectively collected headache diary data from individuals with migraine, with very similar results. It is a limitation that, as documentation of headache characteristics and accompanying symptoms is not mandatory in the DMKG-App, we could not generally distinguish between headaches fulfilling migraine criteria and those not fulfilling these criteria. However, a sensitivity analysis limited to migraine days (i.e., days where additional symptoms were documented and migraine criteria fulfilled, thus necessarily limited to a smaller cohort) gave largely comparable results. In addition, in the app-only group only a limited number of potential predictors were available for analysis. All data analyzed here were collected in Germany. On one hand this can be considered a strength as it ensures a greater homogeneity of the data, e.g., regarding social factors such as most people not working on Saturdays and Sundays. However, further research is needed to determine if these findings are generalizable to individuals with migraine from other countries. In addition, as discussed above, data on weekly sleep patterns, caffeine and alcohol consumption patterns would have allowed to test the hypothesis that these factors contribute to weekend headache. More detailed information on working days and hours would also have further enriched the analysis. Therefore, it must be emphasized that the correlations reported here are only exploratory and these factors should be considered for future studies on weekly patterns of migraine.
Conclusions
In summary, the present data indicate that weekend headache affects a subgroup of individuals with migraine, especially those with episodic migraine and working full-time or part time. However, weekly headache patterns change over time, maybe in response to social and working factors.
Article highlights
This study detected a weekend headache pattern in 15% of individuals with migraine (18% in episodic migraine) in two large, independent DMKG-App data samples
Patients with weekend headache were more often working and had less monthly headache days, compared to the other patterns
Other patterns included an early week cluster, a midweek cluster, and a flat cluster.
Supplemental Material
sj-docx-1-cep-10.1177_03331024261444664 - Supplemental material for Weekend headache in migraine – fact or fiction? An observational study from DMKG-app data
Supplemental material, sj-docx-1-cep-10.1177_03331024261444664 for Weekend headache in migraine – fact or fiction? An observational study from DMKG-app data by Ruth Ruscheweyh, Thomas Dresler, Gudrun Gossrau, Torsten Kraya, Lars Neeb, Bianca Raffaelli, Victoria Ruschil and Jörg Scheidt in Cephalalgia
Supplemental Material
sj-docx-2-cep-10.1177_03331024261444664 - Supplemental material for Weekend headache in migraine – fact or fiction? An observational study from DMKG-app data
Supplemental material, sj-docx-2-cep-10.1177_03331024261444664 for Weekend headache in migraine – fact or fiction? An observational study from DMKG-app data by Ruth Ruscheweyh, Thomas Dresler, Gudrun Gossrau, Torsten Kraya, Lars Neeb, Bianca Raffaelli, Victoria Ruschil and Jörg Scheidt in Cephalalgia
Footnotes
Acknowledgements
First, we wish to thank all participating patients and headache centers. In addition, we thank Dirk Reinel, Johannes Drescher and Florian Wogenstein at the software development company ‘smartlytic’ (Hof, Germany) and Yannic Siebenhaar at the Institute for Information Systems at the University of Applied Sciences Hof (Germany) for their excellent technical development of the DMKG Headache Registry, and Beatrix Weber and Katharina Diersch at the University of Applied Sciences Hof (Germany) and Lukas Wagner (HK2 Comtection GmbH) and Jonas Jacobsen (clover law), both Berlin, Germany for excellent management of the legal and data protection aspects. Moreover, we wish to thank the ‘Münchner Studienzentrum’ at the Technical University of Munich, Germany for outstanding organisational support. Finally, we thank the above-mentioned pharmaceutical companies for their financial support.
Ethical considerations
The “DMKG Headache Registry” has been approved by the ethics committee of the Ludwig-Maximilians-University Munich (Nr. 20-004), complies with European and German Data Protection laws and is registered with the German Clinical Trials Register (DRKS 00021081).
Consent to participate
Each participant consented with use of their data for headache research in anonymized form. Consent was obtained in digital form within the user account on the DMKG Headache Registry platform.
Consent for publication
All authors agree with publication of the manuscript in Cephalalgia.
Author contributions
All authors made substantial contributions to the conception and design of the work and the interpretation of the data. RR and JS performed the data analyses. RR and JS drafted the manuscript; all other authors substantially revised the manuscript. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The DMKG Headache Registry is funded by the German Migraine and Headache Society and by unrestricted grants from companies with an interest in headache research (up to the time of submission of this work, Lilly, Teva, Novartis, Pfizer and Lundbeck have made contributions). Supporting companies were given the opportunity to comment on the research protocol, and their comments were considered where judged to be scientifically relevant. Apart from that, supporting companies did not influence the study design. None of the companies influenced data collection, analysis, interpretation or writing of the manuscript.
Declaration of conflicting interests
RR has received honoraria for consulting and/or lectures and/or congress travel support from AbbVie, Betapharm, Lundbeck, Novartis, Pfizer, and Teva within the past 3 years
TD has received honoraria for consulting and lectures from Hormosan Pharma, Novartis Pharma, and Teva.
GG has received honoraria from Lilly, Novartis Pharma, Teva, Lundbeck, and research grants from Novartis Pharma during the last 3 years.
TK has received travel grants and/or honoraria from Allergan/AbbVie, Hormosan, Lilly, Novartis and Teva.
LN received honoraria for lectures and advisory boards from Hormosan, Lilly, Novartis, Teva, AbbVie/Allergan.
BR is Editor of The Journal of Headache and Pain and Cephalalgia. BR reports research grants from Novartis, Lundbeck, German Migraine and Headache Society (DMKG), German Research Foundation (DFG) and Else Kröner-Fresenius-Stiftung, and personal fees from Abbvie, Lundbeck, Novartis, Organon, Perfood and Teva.
VR received the Soyka award as a research grant from Novartis. She has received honoraria from Teva.
JS declares no conflict of interest.
Data availability statement
The datasets analysed during the current study are available from the German Migraine and Headache Society on reasonable request. Please note that access to data principally suitable for conducting additional analyses must be reviewed by the Headache Registry's Scientific Steering Committee.
Supplemental material
Supplemental material for this article is available online.
Open practices
Not applicable.
List of abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.