
Abstract
Background
This study compared treatment persistence of individuals newly initiating treatment with rimegepant or lasmiditan for the acute treatment of migraine.
Methods
A retrospective cohort analysis was conducted on individuals from MarketScan (commercial and managed Medicare) newly initiating treatment with rimegepant or lasmiditan between March 2020 and December 2022. Treatment persistence was defined as the proportion of individuals with ≥1 medication refill within 12 months of the index prescription. Subgroups included individuals with chronic migraine, index lasmiditan dose (50 and 100 mg) and individuals with a history of two or more uses of controlled substances (prior repeated use of controlled substances [PRUCS] defined here as opioids, butalbital, nausea medications with central nervous system action). Treatment persistence was compared between inverse probability of treatment weighting (IPTW)-adjusted cohorts using odds ratios (ORs) and 95% confidence intervals (CIs).
Results
The primary analysis included 16,603 rimegepant and 716 lasmiditan users. A significantly higher proportion of individuals in the rimegepant cohort were treatment persistent compared with the lasmiditan cohort (OR 3.79 [95% CI 3.23–4.41]). This finding remained consistent across lasmiditan dosages (50 mg: 5.05 [3.87–6.60]; 100 mg: 3.33 [2.78–4.00]), chronic migraine diagnosis (3.89 [3.21–4.71]), or PRUCS (ORs ranged from 2.78 to 4.63; all statistically significant).
Conclusion
Rimegepant users demonstrated higher treatment persistence over 12 months compared to lasmiditan users, which could reflect better real-world treatment satisfaction.
This is a visual representation of the abstract.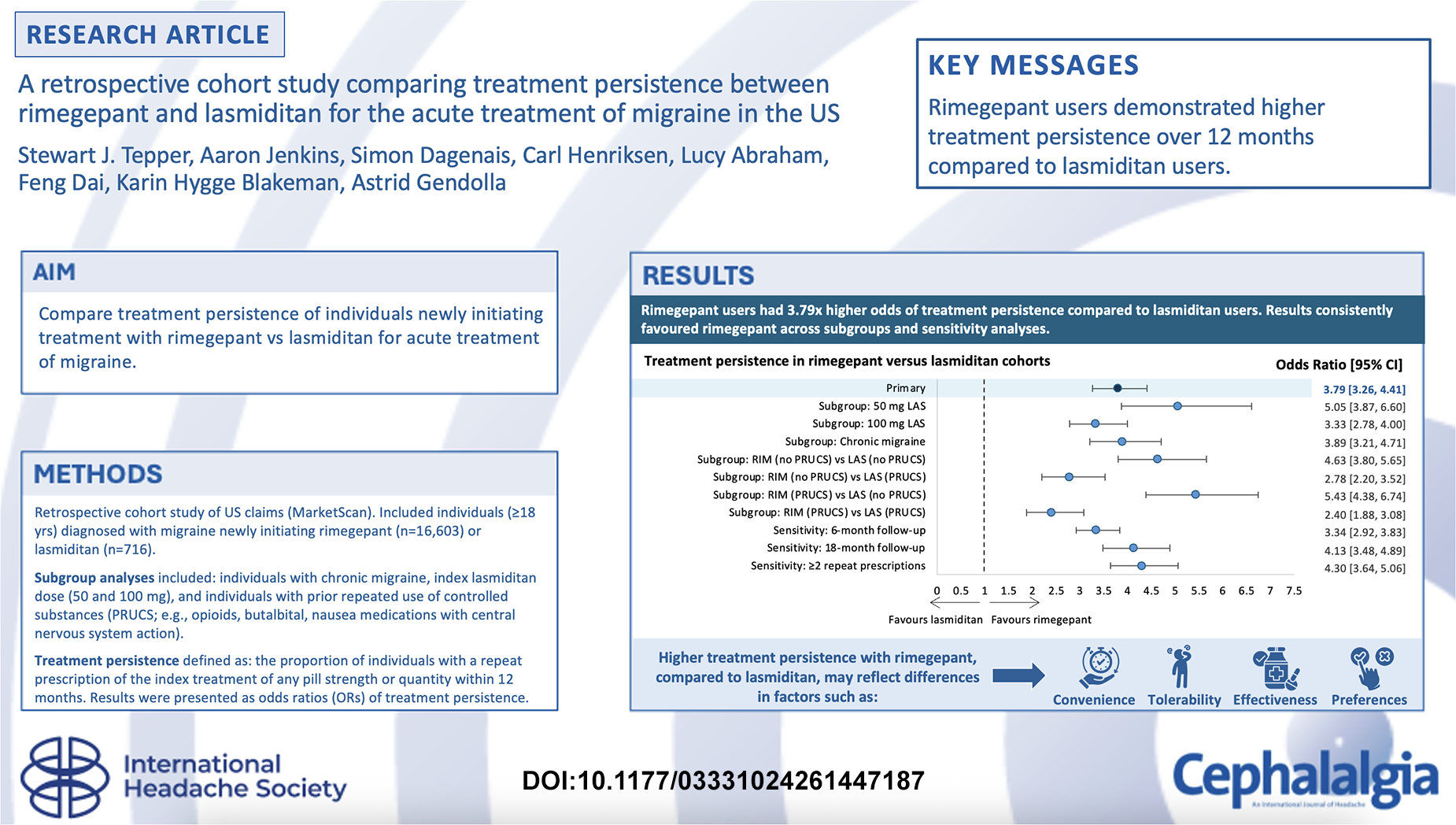
Introduction
Migraine is a highly prevalent chronic neurological condition which negatively impacts individuals’ quality of life, is associated with substantial impact to the healthcare system,1–3 and results in direct and indirect costs to individuals and employers due to workplace absenteeism and presenteeism.3,4 In recent years, there have been notable advancements in migraine treatment with the introduction of novel therapeutic agents with more selective and targeted mechanisms of action. These include gepants, oral calcitonin gene-related peptide (CGRP) receptor antagonists, and lasmiditan, a selective 5-HT1F receptor agonist, which represent two distinct pharmacological approaches for the acute treatment of migraine. 5
Treatment persistence, defined as the continued use of a therapy over time (often measured by repeat prescription claims), is a helpful measure that reflects effectiveness, tolerability, and treatment satisfaction.6–8 Unlike conventional efficacy endpoints measured in clinical trials, such as 2-h pain freedom, treatment persistence provides a more comprehensive assessment of a drug's overall benefits, tolerability profile, and clinical utility. 9 When individuals treat migraine attacks acutely (PRN), they must weigh the benefits and risks, typically without direct input from a health care practitioner. The decision to continue using a treatment as measured by treatment persistence reflects overall treatment satisfaction, including confidence in how quickly the therapy works and whether it enables return to normal function. 10 Several factors influence an individual's treatment decision, including the probability and expected degree of treatment effectiveness (e.g., degree of pain freedom, consistency, speed of onset, and probability of headache recurrence after migraine resolution, based on individuals’ past treatment history and personal experiences), and the risk of side effects which may hinder return to function even if some symptom relief is achieved.
Both the American Headache Society (AHS) and International Headache Society (IHS) suggest that gepants (e.g., rimegepant) or lasmiditan (currently the only approved ditan) be prescribed for acute treatment of migraine to individuals who do not respond to, cannot tolerate, or are contraindicated to triptans.11–13 Rimegepant is approved by the US Food and Drug Administration (FDA) for the acute treatment of migraine with or without aura in adults (75 mg orally disintegrating tablet [ODT] PRN) and for the preventive treatment of episodic migraine in adults (75 mg ODT, every other day). 14 It is supplied in cartons of eight tablets each. 14 Lasmiditan is FDA-approved only for the acute treatment of migraine with or without aura in adults (50 mg, 100 mg, or 200 mg, PRN) and is similarly supplied in cartons of eight tablets of 50 mg or 100 mg each. 15 Although head-to-head trials are lacking, network meta-analysis demonstrated comparable efficacy (pain freedom at 2 h, freedom from most bothersome symptoms at 2 h, pain relief at 2 h) notably among individuals with a history of insufficient triptan response. 16 The most common side effect associated with acute rimegepant treatment is nausea (2% of users), 14 while lasmiditan is associated with dizziness, fatigue, paresthesia, and sedation (each occurring in over 5% of users). 15 The disparity in adverse event (AE) profiles between these treatments is also reflected in a significant difference in economic burden, due to substantial costs related to managing lasmiditan AEs. 17 Further, the treatment persistence of lasmiditan use may be influenced by its classification as a Schedule V drug in the US due to its abuse potential, which may lead to variations in treatment persistence rates due to factors such as the drug's psychological or physiological effects (which could increase use), 18 or the administrative obstacles required to access the drug (which could hinder its use).19,20 Additionally, there is a driving restriction for 8 h after lasmiditan use, and AEs, in addition to the driving restriction, could also alter use and treatment persistence. As previously mentioned, the individuals who are prescribed rimegepant or lasmiditan are likely to have significant prior treatment history, which may include medications that are regulated by the US Controlled Substances Act (21 US Code § 812) such as opioids and butalbital, as well as anti-nausea medications with central nervous system (CNS) activity.11,12 While the AHS and IHS no longer recommend use of opioids or butalbital for acute treatment of migraine,11,12 past use may influence present behaviors including persistence on novel treatments. For example, due to the abuse potential of controlled substances, a history of use of opioids or butalbital may indicate that an individual is more likely to persist on lasmiditan. Conversely, a history of opioid use may impact how a health care provider chooses to prescribe controlled substances. It is uncertain whether the sum of these effects leads to overall higher or lower treatment persistence.
Another subgroup that may show different treatment and persistence patterns is chronic migraine. According to the International Classification of Headache Disorders, 3rd edition (ICHD-III), chronic migraine is defined as headache occurring on 15 or more days per month for more than 3 months, which, on at least 8 days/month, has the features of migraine headache; this is considered to represent a more severe form of migraine. 21 Individuals with chronic migraine show more frequent use of both acute and preventive treatments for migraine than those with episodic migraine. 22 This may have further implications for treatment persistence, as this is measured by the repeat prescription claims.
The primary objectives of this study were to characterize cohorts diagnosed with migraine who are new users of rimegepant or lasmiditan and to compare treatment persistence between these cohorts. Secondary objectives included subgroup analyses of treatment persistence in individuals by index dose of lasmiditan, those with chronic migraine, and according to treatment history with controlled substances.
Methods
Data source
This retrospective cohort study utilized US closed-network claims data from the Merative MarketScan Commercial Claims and Encounters, and Medicare Advantage and Medicare Supplemental administrative databases to assess individuals with commercial or managed Medicare health insurance. Access to these databases was obtained by subscription. This database started in 1996, represents individuals from all US census regions, includes over 94 million unique individuals, and is often used in pharmaco-epidemiology research, including a previously published retrospective cohort study comparing the treatment persistence of rimegepant and oral triptans. 23 This study is reported in accordance with the STROBE guidelines for a retrospective cohort study.
Study design
The study period (i.e., the period used to create the analyzed study dataset, including exposures, inclusion and exclusion criteria, covariates, outcome, and follow-up) spanned from 01 March 2019 to 31 December 2023. Within this, the identification period (i.e., the period during which individuals could enter the study cohorts) spanned from 01 March 2020 to 31 December 2022. The start of the identification period was chosen to correspond with the FDA approval of rimegepant for acute treatment of migraine on 27 February 2020, marking the earliest time point when both treatments had regulatory approval from the FDA. The index date was defined as the date of the first prescription fill for either rimegepant 75 mg (quantity of 8 tablets) or lasmiditan doses of 50 mg, 100 mg or 200 mg (given as two tablets), occurring within the identification period. The available tablet dose strengths of lasmiditan were 50 or 100 mg. Individuals with lasmiditan 200 mg dosage had twice the number of tablets as number of days supplied on the index date. This definition was based on the variables available in the data source. The baseline period was defined as the 12 months prior to the index date, and the follow-up period extended from the day after the index date until 12 months post-index. For more details, see Supplementary Figure 1.
This study was conducted according to legal and regulatory requirements, maintaining scientific purpose, value, and rigor, and followed established research practices, including Good Practices for Outcomes Research issued by the International Society for Pharmacoeconomics and Outcomes Research (ISPOR). Authors determined that Institutional Review Board approval was not required because the study database contained de-identified claims data without protected health information, in compliance with the Code of Federal Regulations, title 45, part 46.104.
Analysis population
The study included adults (≥ 18 years) with at least one claim with a diagnosis of migraine (ICD-10-CM code: G43.xxx) during the baseline period or on the index date who were new users of rimegepant or lasmiditan for the acute treatment of migraine.
Rimegepant is approved for two indications in the FDA label, both using a 75 mg dose but differing in the dosing regimen: 1) PRN dosing for acute treatment of migraine and 2) every other day dosing for prevention of episodic migraine. 14 As information on the prescribed indication was not available in the claims databases, the dispensed quantity of rimegepant on the index date was used as a proxy for the indicated treatment. A quantity of 8 tablets was assumed to indicate acute treatment of migraine using PRN dosing, as preventive treatment (i.e., every other day dosing over 4 weeks) would require a minimum quantity of 15 tablets per 30 days. A similar approach to defining the number of tablets for acute treatment was employed in previously published claims-based studies that reported utilization patterns among new users of rimegepant that were consistent with this assumption.23,24
Individuals from both cohorts were excluded if they were prescribed any triptan on the index date, or if they had a prescription for ubrogepant or atogepant in the baseline period or on the index date. Those in the rimegepant cohort were excluded if they had a prescription for lasmiditan in the baseline period or on the index date or a prescription for rimegepant in the baseline period. Similarly, those in the lasmiditan cohort were excluded if they had a prescription for rimegepant in the baseline period or on the index date or a prescription for lasmiditan in the baseline period. All individuals were required to have a minimum of 12 months of continuous enrollment in medical and pharmacy benefits both before and after the index date.
Outcomes
Treatment persistence was defined as the proportion of individuals with a repeat prescription claim of the index treatment of any pill strength or quantity within 12 months. Given the PRN utilization of these medications, treatment persistence was evaluated based on a minimum number of refills obtained over a pre-specified length of follow-up. 25 A 12-month timeframe was selected to allow the majority of individuals with low migraine frequency to have a repeat claim, thereby reducing the potential for misclassification of infrequent treatment as non-persistence.
The primary endpoint was treatment persistence for rimegepant vs. lasmiditan (any approved dosage) measured over a 12-month follow-up period. Secondary endpoints included treatment persistence for (1) rimegepant vs. lasmiditan 50 mg or 100 mg or 200 mg in the overall population; (2) rimegepant vs. lasmiditan among individuals with a diagnosis of chronic migraine (ICD-10-CM code: G43.701, G43.709, G43.711, G43.719 during the baseline period [see definition above] or on index date), and (3) rimegepant vs. lasmiditan among individuals with and without prior repeated use of controlled substances (PRUCS), defined as more than one claim for mono- or combination therapies containing opioids, butalbital, or anti-nausea medications with CNS activity during the baseline period up to the index date (Supplementary Table 1).
Statistical analysis
Baseline demographics and clinical characteristics were summarized using descriptive statistics (i.e., mean, standard deviation, median, and inter-quartile range for continuous variables and differences across cohorts; counts and proportions for categorical variables). Comparative analyses were performed using inverse probability of treatment weighting (IPTW) to address differences between groups in baseline sociodemographic and health characteristics, thereby minimizing confounding. IPTW was selected as the method for adjusting differences between cohorts based on the anticipation that all individuals could potentially be candidates for either rimegepant or lasmiditan in clinical practice. The model for propensity score calculation included calendar year, age, sex, menstrual migraine, insurance type, region, relevant comorbidities (including triptan contraindications, triptan warnings, cardiovascular risk factors, depression, anxiety, and seizures/epilepsy), treatment history with prevention agents (beta blockers, tricyclic antidepressants, antidepressants, anticonvulsants, anti-CGRP monoclonal antibodies [mAbs], and onabotulinumtoxinA), treatment history with acute agents (oral triptans, nasal triptans, injectable triptans, nasal dihydroergotamine, injectable dihydroergotamine, nasal nonsteroidal anti-inflammatory drugs [NSAIDs], injectable NSAIDs, acetaminophen, and isometheptene combinations), and PRUCS. Note that for the PRUCS subgroup analysis, the PRUCS baseline variable was not included in the propensity score model. The standardized mean difference (SMD) was used to quantify differences in covariate distributions between cohorts, with a threshold of less than 0.1 considered indicative of adequate balance. 26 Treatment persistence was compared between weighted cohorts using a multiple logistic regression analysis that adjusted for covariates with an SMD ≥ 0.1 after IPTW weighting. The odds ratios (ORs) with 95% confidence intervals (95% CI) and associated p-values were reported. Subgroup analyses, using de novo IPTW, were performed on specific index pill strength of lasmiditan, individuals with a chronic migraine diagnosis, and individuals with and without PRUCS between treatment cohorts.
Sensitivity analyses were conducted to test the robustness of the primary outcome to assumptions regarding the definition of treatment persistence. Specifically, the sensitivity analyses evaluated the impact of varying the follow-up periods (6 and 18 months), refining the definition of treatment persistence to include only individuals with ≥ 2 post-index prescriptions, and using propensity score matching (PSM) instead of IPTW to balance differences in baseline covariates between groups. To assess the strength of a hypothetical unmeasured confounder that might explain away a specific treatment-outcome association, an analysis using the E-value method was conducted. 27 An E-value was calculated for each primary or secondary outcome. Those with a significant p-value (i.e., p < 0.05) were interpreted as follows: the observed association could only have been caused by residual confounding if the unmeasured covariates had an association greater than or equal to the E-value with both treatment type (rimegepant or lasmiditan) and treatment persistence. All analyses were performed using SAS statistical software (version 9.4, SAS Institute, Cary, North Carolina).
Results
The rimegepant cohort included 16,603 individuals, while the lasmiditan cohort consisted of 716 individuals. In the chronic migraine subgroup, the rimegepant and lasmiditan cohorts comprised 6518 and 264 individuals, respectively. The lasmiditan cohort also contained a 50 mg subgroup with 229 individuals and a 100 mg subgroup with 487 individuals. An exploratory analysis of individuals initiating lasmiditan treatment at a 200 mg dose (two 100 mg pills at index date) identified 13 individuals satisfying all other eligibility criteria in the 100 mg subgroup. Due to the small number of such individuals (representing <3% of the 100 mg subgroup), separate subgroup analyses on this dose were not pursued.
Prior to IPTW adjustment, the mean age was 45.5 years in the lasmiditan cohort and 43.1 years in the rimegepant cohort (Table 1). The proportion of women in the lasmiditan cohort was 85.5% and 87.7% for the rimegepant cohort. The distribution of comorbidities among the lasmiditan cohort was 8.7% for ischemic cerebrovascular disease, 7.7% structural heart disease, 8.2% for arrythmias, 2.1% for cardiac surgery, 38.1% hypertension, 40.4% for depression and 48.3% for anxiety-related disorders. Among the rimegepant cohort, 5.7% had ischemic cerebrovascular disease, 5.0% for structural heart disease, 5.2% for arrythmias, 0.8% for cardiac surgery, 31.0% for hypertension, 31.2% for depression, and 41.1% for anxiety-related disorders. Treatment history with preventive agents ranged from 13% (onabotulinumtoxinA) to 26% (anti-CGRP mAbs) in the rimegepant cohort, and from 16% (tricyclic antidepressants) to 48% (anti-CGRP mAbs) in the lasmiditan cohort. Treatment history with acute agents ranged from < 0.01% (isometheptene combinations) to 51% (oral triptans) in the rimegepant cohort, and from 0% (isometheptene combinations) to 52% (oral triptans) in the lasmiditan cohort. After adjustment with IPTW, sociodemographic and health characteristics were balanced between the two cohorts (SMD < 0.1), except for age, diabetes and ischemic heart disease (Table 1), and thus were further adjusted for in the regression analysis of the treatment persistence outcome.
Baseline demographics and clinical characteristics before and after IPTW (primary analysis).

Abbreviations: CGRP, calcitonin gene-related peptide; CVD, cardiovascular disease; IPTW, inverse probability of treatment weighting; mAbs, monoclonal antibodies; NSAID, nonsteroidal anti-inflammatory drugs; PRUCS, prior repeated use of controlled substances; SD, standard deviation; SMD, standardized mean difference.
In the primary analysis, a statistically significant higher proportion of individuals in the rimegepant cohort were treatment persistent compared with the lasmiditan cohort (OR 3.79; 95% CI 3.26–4.41, p < 0.001; Figure 1; Table 2). Subgroup analyses yielded consistent findings (Figure 1; Table 2): lasmiditan 50 mg (OR 5.05; 95% CI 3.87–6.60), lasmiditan 100 mg (OR 3.33; 95% CI 2.78–4.00), and chronic migraine (OR 3.89; 95% CI 3.21–4.71) subgroups all showed that significantly more individuals in the rimegepant cohort were persistent than in the lasmiditan cohort (all p < 0.001). Subgroup analyses of individuals according to PRUCS all showed that rimegepant was associated with a higher proportion of persistent individuals, regardless of PRUCS status. Among individuals with no PRUCS, the OR of rimegepant vs. lasmiditan was 4.63 (95% CI 3.80–5.65, p < 0.001). Among individuals with PRUCS, the OR of rimegepant vs. lasmiditan was 2.40 (95% CI 1.88–3.08, p < 0.001). Comparing rimegepant users with no PRUCS to lasmiditan with PRUCS, the OR was 2.78 (95% CI 2.20–3.52, p < 0.001). In the reverse scenario, the OR was 5.43 (95% CI 4.38–6.74, p < 0.001).

Forest plot of odds ratios of treatment persistence for rimegepant compared with lasmiditan for primary, subgroup and sensitivity analyses.
Proportion of individuals treatment persistent in rimegepant versus lasmiditan cohorts.

Abbreviations: CI, confidence interval; OR, odds ratio; PRUCS, prior repeated use of controlled substances.
Sensitivity analyses showed that the odds of treatment persistence were consistently higher in the rimegepant cohort relative to the lasmiditan cohort regardless of duration of follow-up, whether 6 months (OR: 3.34; 95% CI 2.92–3.83, p < 0.001) or 18 months (OR: 4.13; 95% CI 3.48–4.89, p < 0.001; Figure 1; Table 3). The sensitivity analysis defining treatment persistence as two repeat prescriptions in a 12-month follow-up period (as opposed to a single prescription) also showed higher treatment persistence for the rimegepant cohort compared with the lasmiditan cohort (OR 4.30; 95% CI 3.64–5.06, p < 0.001; Figure 1; Table 3). The use of PSM instead of IPTW to balance differences in baseline covariates between groups produced similar results (Supplementary Table 2).
Sensitivity analyses.
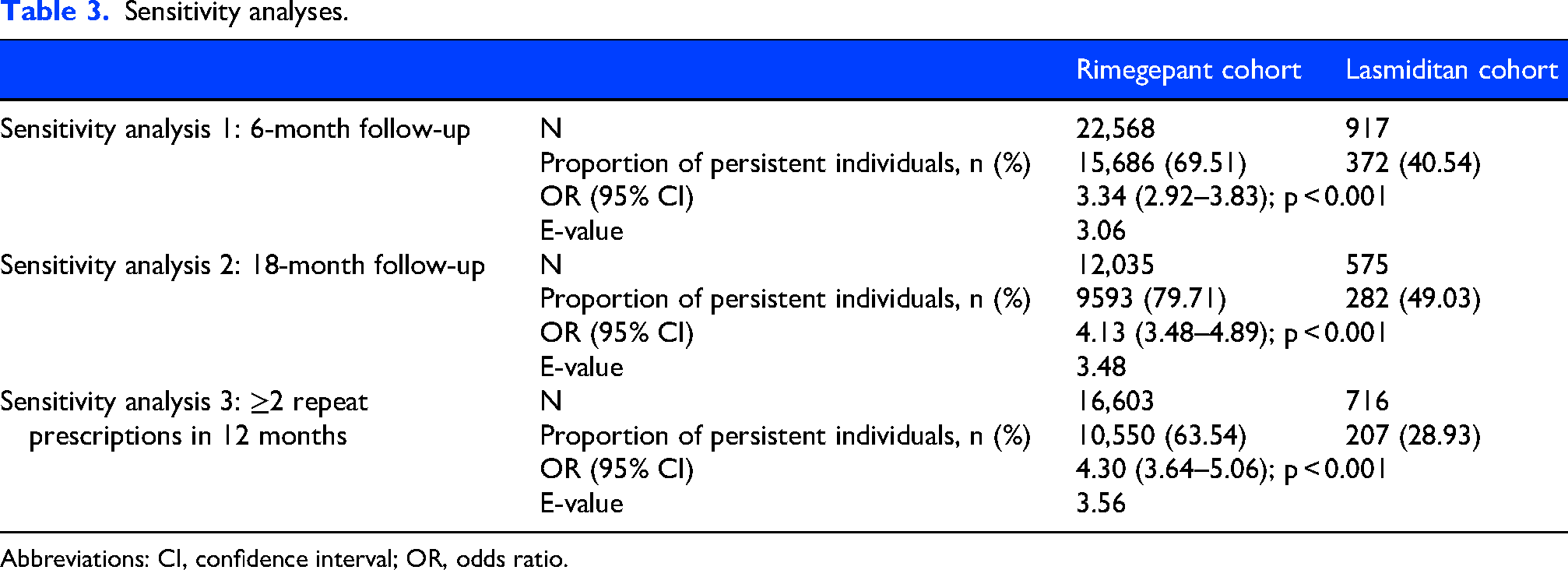
Abbreviations: CI, confidence interval; OR, odds ratio.
The E-value calculated for the primary analysis was 3.30 (Table 2). For the subgroups, the calculated E-values ranged from 2.40 to 4.09 (Table 2). E-values calculated for sensitivity analyses ranged from 2.47 to 3.56 (Table 3).
Discussion
This was the first observational study comparing treatment persistence between lasmiditan and rimegepant for the acute treatment of migraine. Treatment persistence is a valuable consideration when evaluating the effectiveness of migraine treatments, as it reflects individuals’ long-term satisfaction with their medical management. Further, the real-world evidence generated by this study provides valuable insights into the performance of treatments in the context of routine clinical practice, impacted by the complexities of patient care and treatment patterns across diverse populations. 28 Several factors impact treatment persistence for acute migraine therapy, including effectiveness, speed of onset, confidence in the medication, tolerability, ability to use when needed, and treatment satisfaction.10,29 Optimal treatments deliver rapid symptom resolution with acceptable tolerability, enabling a complete return to normal function, supporting sustained use over time.
The findings from this retrospective claims data analysis suggest that individuals are more likely to remain on rimegepant compared with lasmiditan. The results demonstrated significantly and substantially greater treatment persistence with rimegepant compared with lasmiditan in the overall population, as well as within all subgroups, including individuals with chronic migraine, using any dose of lasmiditan, and with any history of repeated controlled substance use or CNS active anti-nausea medication. The lower treatment persistence with lasmiditan may be related to AEs such as dizziness, or sedation, and to the FDA label restriction requiring individuals to avoid driving for at least 8 h after each dose because of the risk of incoordination documented from driving simulator tests.15,30 Notably, this incoordination is observed regardless of whether dizziness or sedation are present. 30 The label restriction limits the use of lasmiditan to times and places when driving or other activities requiring coordination are not necessary, which may cause individuals to delay treatment until they are home in the evening or opt to stop treatment altogether rather than using lasmiditan immediately at migraine onset, as recommended.
The consistency of the result within the chronic migraine subgroup indicates that the value of rimegepant as an effective and tolerable treatment for migraine is relevant not only to the general migraine population, but also to subset of individuals with more severe disease. Further, this subgroup is typically not included in clinical trials of acute treatment, making this result particularly informative in the chronic migraine context. This may provide reassurance to health care providers and individuals with migraine that despite the complexity of managing chronic migraine, rimegepant is persistent relative to other available treatments.
While there is no single 200 mg lasmiditan tablet available, individuals may be prescribed a 200 mg dosage as two 100 mg tablets. In this study, a small number of individuals were identified as potentially having a 200 mg dose, observed as having twice the number of tablets compared to the number of days’ supply (i.e., two tablets per day). However, this was an insufficient number of individuals for a subgroup analysis to be conducted, despite the use of a large and comprehensive dataset and previous findings reporting 200 mg as the most efficacious dose.31–33 Since this study evaluated individuals who were newly initiating lasmiditan, this may reflect that health care providers were unlikely to initiate treatment with the highest approved dose. This may also suggest that factors beyond effectiveness influence use, such as tolerability, which may contribute to individuals’ satisfaction with their treatment experience. Clinical evidence shows that lasmiditan 200 mg is associated with a higher incidence of dizziness and fatigue than lasmiditan 100 mg or 50 mg.31,32,34 This tolerability profile may deter some individuals from seeking and/or using higher doses. These findings also suggest that a broader value assessment of acute therapies can be achieved by complementing efficacy outcomes such as 2-h pain freedom with those that incorporate other features of clinical utility (e.g., return to function), to better inform clinical decision making. Treatment persistence reflects an individual's willingness to continue a therapy, taking into account the features of usefulness for the person treating a migraine attack. Future research should further explore factors influencing treatment persistence in therapies for acute migraine.
Strengths of the study include the consistency of the findings across all subgroups, suggesting that the treatment persistence advantage of rimegepant over lasmiditan is generalizable to a broad population of migraine individuals. The MarketScan databases offer comprehensive sources of real-world data that have powered numerous observational studies, covering a large and diverse population of adults with migraine, and thus may also enhance the generalizability of the findings. Sensitivity analyses corroborated the strength of these findings, affirming that varying assumptions of the study design, populations, and definitions of treatment persistence did not impact the conclusions. IPTW controlled for key sociodemographic and clinical characteristics, including comorbidities and treatment history. Also, the potential influence of unmeasured confounding was assessed using the E-value method and found that an unmeasured confounder would need to be associated with both treatment persistence and the treatment type (rimegepant or lasmiditan) with an OR > 3.30 (“E-value”) to explain the results of the primary analysis. The unmeasured factors that are most associated with discontinuation from acute treatment of migraine in the published literature are effectiveness, tolerability, and treatment satisfaction, which may in fact mediate treatment persistence rather than confound it, in accordance with the conceptual framework of treatment persistence in this study.10,35
Several limitations warrant consideration when interpreting the findings of this study. The reliance on administrative claims databases, designed primarily for billing purposes, limits the type of information available for analysis. For example, over-the-counter medication use was not captured in the claims. The potential for miscoding or incomplete claims inherent in health insurance data introduces a risk of inaccuracies in the analysis. Furthermore, the requirement for a minimum 12-month continuous enrollment post-index may introduce bias if prolonged eligibility correlates with an increased likelihood of remaining on treatment, implying that individuals who are more likely to be persistent were also more likely to remain in the study. The definition of treatment persistence used in this study does not distinguish between positive and negative reasons for treatment discontinuation. Some individuals may have discontinued treatment as it was no longer required. It is also possible that individuals were exposed to the intervention prior to the 12-month baseline period (i.e., the index date was not the first time they initiated treatment). While both treatments have identical FDA indications for acute treatment and recommendations from the AHS consensus statement and were expected to have broad similarities in treatment history and disease severity, the risk of channeling bias remains. Despite using multiple techniques to balance differences in baseline cohort characteristics (IPTW and PSM), the potential for residual confounding by other unaccounted factors remains (though E-values were calculated to quantify their potential impact). The study period comprised the first three years of rimegepant's availability on the US market, while lasmiditan in this period had more established treatment use patterns. Thus, the two cohorts may not have been composed of individuals who were equally likely to be prescribed either treatment. However, the findings of the study remained consistent across multiple established statistical techniques for balancing the cohorts (IPTW and PSM), and E-values provide reassurance that there was a substantial threshold that unmeasured confounders would have to exceed to explain the reported results, as described above.
Conclusions
Rimegepant was associated with significantly higher treatment persistence compared with lasmiditan, irrespective of lasmiditan index dose, chronic migraine diagnosis, history of controlled substance use, or history of use of CNS active anti-nausea medications. Given the evidence supporting rimegepant as an effective and generally well-tolerated acute migraine treatment, it is hypothesized that the higher proportion of persistent individuals in the rimegepant cohort may reflect a more favorable treatment experience, potentially including improved tolerability, convenience, and resultant treatment satisfaction. Further research is warranted to confirm and expand upon these findings as well as to explore the potential benefits of rimegepant for improving long-term outcomes among individuals with migraine.
Clinical implications
Individuals initiating rimegepant for the acute treatment of migraine were more likely to be treatment persistent vs. those initiating lasmiditan.
Treatment persistence results were consistent in subgroup analyses of individuals diagnosed with chronic migraine, prescribed specific lasmiditan dosages, and having prior repeated use of controlled substances.
Supplemental Material
sj-docx-1-cep-10.1177_03331024261447187 - Supplemental material for A retrospective cohort study comparing treatment persistence between rimegepant and lasmiditan for the acute treatment of migraine in the US
Supplemental material, sj-docx-1-cep-10.1177_03331024261447187 for A retrospective cohort study comparing treatment persistence between rimegepant and lasmiditan for the acute treatment of migraine in the US by Stewart J Tepper, Aaron Jenkins, Simon Dagenais, Carl Henriksen, Lucy Abraham, Feng Dai, Karin Hygge Blakeman and Astrid Gendolla in Cephalalgia
Supplemental Material
sj-png-2-cep-10.1177_03331024261447187 - Supplemental material for A retrospective cohort study comparing treatment persistence between rimegepant and lasmiditan for the acute treatment of migraine in the US
Supplemental material, sj-png-2-cep-10.1177_03331024261447187 for A retrospective cohort study comparing treatment persistence between rimegepant and lasmiditan for the acute treatment of migraine in the US by Stewart J Tepper, Aaron Jenkins, Simon Dagenais, Carl Henriksen, Lucy Abraham, Feng Dai, Karin Hygge Blakeman and Astrid Gendolla in Cephalalgia
Footnotes
Abbreviations
Acknowledgements
The authors wish to thank Sally Miller (Broadstreet HEOR) for assisting with medical writing and manuscript submission activities (including all statements and declarations of conflicts of interest and funding), which were funded by Pfizer UK Ltd These activities have been undertaken with the approval of all authors.
Ethical considerations
Authors determined that Institutional Review Board approval was not required because the study database contained de-identified claims data without protected health information.
Consent to participate
Not applicable
Consent for publishing
All authors agree to publish this work in Cephalalgia.
Author contributions
Stewart J Tepper: Conceptualization; Investigation; Methodology; Validation; Visualization; Writing - review & editing.
Aaron Jenkins: Conceptualization; Funding Acquisition; Investigation; Methodology; Project Administration; Supervision; Validation; Visualization; Writing - review & editing.
Simon Dagenais: Conceptualization; Investigation; Methodology; Supervision; Validation; Visualization; Writing - review & editing.
Carl Henriksen: Data Curation; Formal Analysis; Investigation; Methodology; Project Administration; Resources; Software; Validation; Visualization; Writing - review & editing.
Lucy Abraham: Conceptualization; Funding Acquisition; Investigation; Methodology; Project Administration; Supervision; Validation; Visualization; Writing - review & editing.
Feng Dai: Conceptualization; Formal Analysis; Investigation; Methodology; Validation; Visualization; Writing - review & editing.
Karin Hygge Blakeman: Conceptualization; Investigation; Methodology; Validation; Visualization; Writing - review & editing.
Astrid Gendolla: Conceptualization; Investigation; Methodology; Validation; Visualization; Writing - review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was sponsored by Pfizer UK Ltd.
Declaration of conflicting interests
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: SJT reports financial support from the following:
AJ, SD, LA, FD and KHB, are full-time employees of and own stock in, hold stock options in or receive stock-based compensation from Pfizer.
CH is a contract programmer for Pfizer.
AG reports financial support for advisory boards, consulting and speaker honoraria from: Grünenthal, Mundipharma, Abbvie/Allergan, Lilly, Teva, Amgen, Novartis, Hormosan, Stada, Lundbeck, Pfizer, Hexal, Esanum, Perfood, Medscape, streamed up, Ärztekammer Nordrhein, Ärztekammer Westfalen Lippe, DGS, Regionalbeauftragte der DMKG.
Data availability statement
Open practices
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.