
Abstract
Background
Disruption of the endocannabinoid system has been implicated in both migraine and depression, which are frequently comorbid in patients. Nevertheless, supporting evidence for this hypothesis is limited. Hence, we investigated whether the endocannabinoid system is disrupted in interictal migraine patients and whether confounding factors were of influence.
Methods
To this end, we measured the levels of endocannabinoids N-arachidonoylethanolamine (AEA) and 2-arachidonoylglycerol (2-AG), and the endocannabinoid analogue docosahexaenoylethanolamine (DHEA) in the cerebrospinal fluid (CSF), obtained from 194 individuals with episodic migraine between attacks (97 migraine with aura and 97 migraine without aura individuals) and from 94 healthy volunteers, using micro-liquid chromatography – tandem mass spectrometry (micro-LC-MS/MS). Groups were age- and sex-matched. Timing and processing of sampling was protocolized. Multivariate linear regression analyses for log10-transformed endocannabinoid concentrations were performed to compare groups. Covariates that were included were sex, age, BMI, substance use and depressive symptoms.
Results
No differences were detected between individuals with migraine with or without aura and healthy controls in the CSF for AEA (p = 0.46, p = 0.08), 2-AG (p = 0.46, p = 0.90) and DHEA (p = 0.58, p = 0.79), respectively. For 2-AG, levels were, however, positively correlated with depressive symptoms (β = 0.053; 95% CI: 0.014 to 0.093, p = 0.008).
Conclusion
CSF endocannabinoids (AEA, 2-AG, and DHEA) may not serve as effective biomarkers for distinguishing interictal episodic migraine patients from controls. Instead, CSF levels of 2-AG are linked to depressive symptoms, shedding further light on the relevance of endocannabinoids in patients with migraine and depression. This study highlights the intricate nature of the endocannabinoid system concerning episodic migraine and confounding factors.
This is a visual representation of the abstract.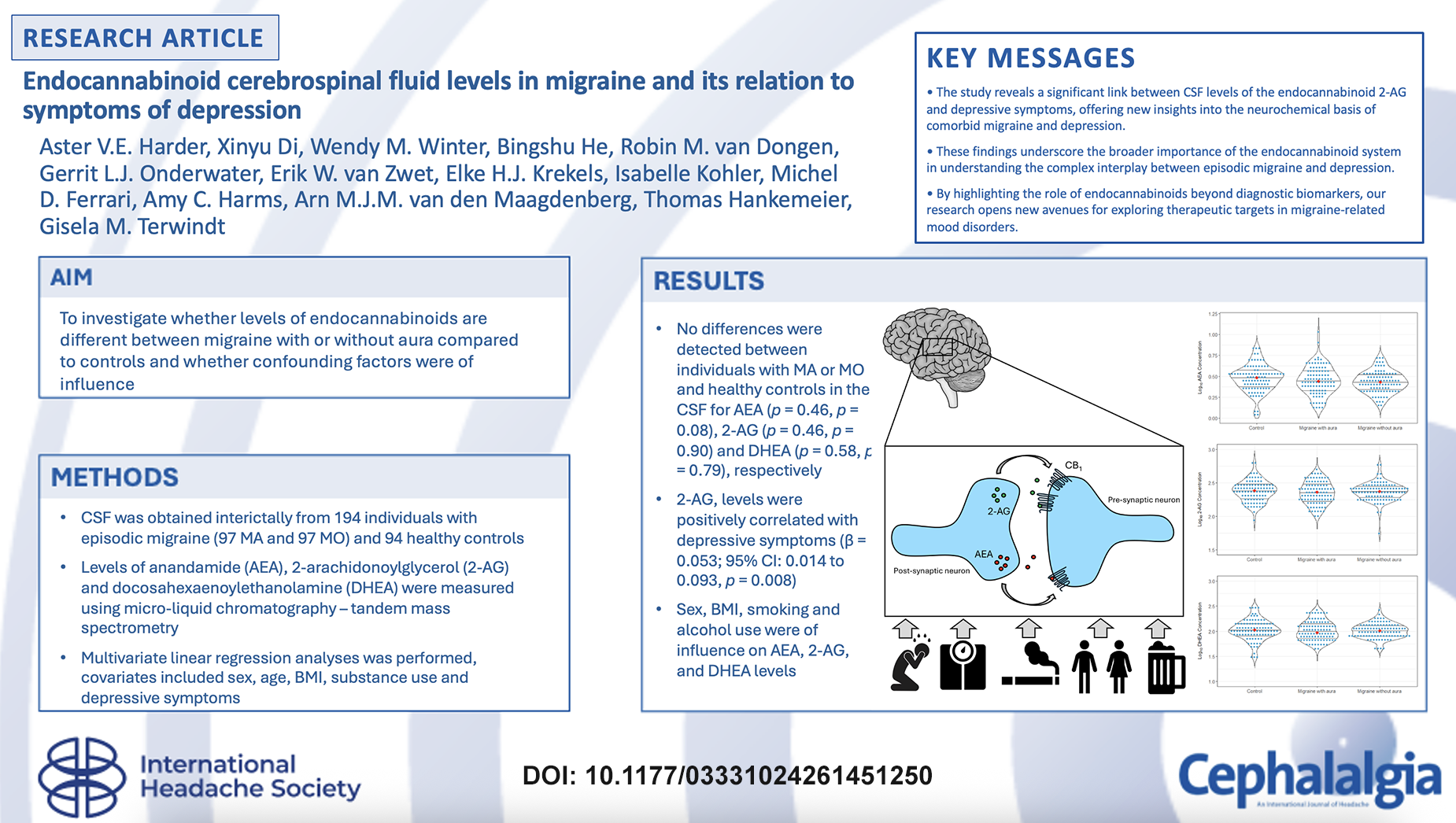
Introduction
Migraine is a highly prevalent, disabling, primary brain disorder characterized by attacks of severe headache and associated symptoms. 1 Depression and anxiety are common comorbid disorders.2,3 Research into neurochemistry in individuals with migraine between attacks may help elucidate its pathophysiology and provide useful treatment targets. Given the repeated nature of migraine attacks there likely is a difference between individuals with migraine and healthy controls that is due to the disease itself or is a consequence of experiencing multiple attacks. A possible contributor that makes patients vulnerable to migraine attacks could be changes in the endocannabinoid system, which has a strong influence on neurotransmission, the neuroendocrine and neuroimmune systems,4–6 which are all involved in migraine pathophysiology.7,8 In addition, it has been shown that the endocannabinoid system is involved in pain perception, depending on the mode of action, activation of the endocannabinoid system can both lead to the increase and decrease of pain either directly or indirectly via anti-inflammatory properties. 9 Previous studies have suggested that endocannabinoids consisting of N-acylethanolamines (NAEs), act in the trigeminovascular system, a key component in migraine pathophysiology.10,11 One study of mRNA expression of cannabinoid receptors in rat trigeminal ganglia has revealed that 30% of the fibers contain mRNA of this receptor, however, expression was mainly in Aβ-fibers and there was little colocalization with putative nociceptor markers, illustrating that it is unclear how endocannabinoids are involved in peripherally mediated antinociceptive effects. 12 Thus, it remains poorly understood what the exact role of endocannabinoids in migraine is. Still, cannabinoids are currently considered as treatment for migraine, thus it is highly relevant to determine the role of endocannabinoids in migraine. 13
The endocannabinoid system consists of two major cannabinoid receptors (CB1 and CB2) and their lipid signaling ligands; the endocannabinoids. 14 Endocannabinoid signaling is a key regulator of synaptic communication through retrograde inhibition of the release of inhibitory and excitatory neurotransmitters. 15 CB1 receptors are expressed throughout the peripheral and central nervous system, whereas CB2 receptors are mainly located on immune cells. The two most widely studied endocannabinoids are N-arachidonoylethanolamine, also called anandamide (AEA) and 2-arachidonoylglycerol (2-AG). AEA is a partial agonist for both cannabinoid receptors, with a high affinity for CB1 and a low affinity for CB2. 14 Additionally, AEA is a full agonist at the transient receptor potential vanilloid 1 (TRPV1), where it modulates the release of calcitonin gene-related peptide (CGRP).16,17 CGRP is a key neurotransmitter of the trigeminovascular system and a known contributor in causing migraine attacks. 2-AG is a full agonist at CB1 and CB2 receptors and an important endocannabinoid ligand in nervous tissue.14,18 Docosahexaenoylethanolamine (DHEA) is a CB2 receptor partial agonist, 19 however, its exact role in the endocannabinoid system has not been as extensively studied as that of AEA and 2-AG. 20
In a relatively small study (n = 50), AEA was suggested to be lower and palmitoylethanolamide (PEA) to be higher in cerebrospinal fluid (CSF) of chronic migraine patients. 21 Fatty acid amide hydrolase (FAAH), which degrades AEA, and endocannabinoid membrane transporter (EMT) activity in platelets was found increased in women but not in men with migraine suggesting an altered endocannabinoid system in female patients. 22 Gene expression and peripheral protein levels of endocannabinoid system components (those involved in biosynthesis of NEAs, e.g., NAPE, MAGL and DAGL) were elevated in the blood of people with migraine. 23 Additionally, evidence has emerged for a role of the endocannabinoid system in depression. 24 Depression has a bidirectional relationship with migraine.2,25 Women with depression had reduced endocannabinoid levels in blood serum, 26 and chronic treatment with antidepressants seems to alter the endocannabinoid system. 27
As brain endocannabinoid concentrations do not directly correlate with peripheral endocannabinoid levels, 9 measuring endocannabinoids in CSF, the biofluid closest to the brain, likely is the best choice of body fluid to assess what activity has occurred in the brain. Hence, we compared CSF levels of endocannabinoids in a large cohort of people with migraine with or without aura and healthy controls matched for sex and age, whilst taking depressive symptomology into account. Our goal was to investigate whether levels of endocannabinoids are different between migraine with or without aura compared to controls. The primary outcome was to detect a difference in AEA, 2-AG and/or DHEA levels using micro-liquid chromatography – tandem mass spectrometry (micro-LC-MS/MS) between those with or without aura compared to controls, whilst controlling for possible confounders. As secondary outcome the effects of confounding factors, such as depressive symptoms, on endocannabinoid levels were investigated. Thus, we sought to detect differences in the endocannabinoid system that hopefully aid in the development of better treatment for migraine.
Methods
Study design and participants
The collection of the study population has been described in Onderwater et al. 28 In brief, we enrolled n = 198 individuals with migraine (n = 100 migraine with aura and n = 98 migraine without aura) and n = 96 healthy controls and group-matched them for age (using 5-year strata) and sex. Migraine was diagnosed according to the International Classification of Headache Disorders (ICHD3) by experienced physicians (supervised by G.M.T. and M.D.F.). 1 For the first few years, we instead used the ICHD2 version without essential differences between patients, at least for this study of episodic cases, so we feel that using different versions of ICHD2 did not influence the outcome of the study. The majority of participants were recruited from the LUMINA (Leiden University Medical Center Migraine Neuro Analysis) database, which encompasses both migraine patients and healthy volunteers from the Dutch population, all of whom volunteered to contribute to research focused on migraine. Some patients and healthy volunteers were recruited through a public advertisement or through the Leiden University Medical Center Headache Clinic. All participants were between 18 and 65 years (41 ± 14) and had a body mass index (BMI) between 18 and 28 (24 ± 3). Individuals suffering from migraine did not use acute migraine drugs on more than 8 days per month. None of the patients suffered from chronic migraine or medication overuse headache. Also, they did not suffer from frequent episodic tension-type headache. Healthy volunteers had no signs or symptoms of a disease and had no history of headache (except for infrequent episodic tension-type headaches) or other pain-related syndromes. They also did not have first-degree relatives with migraine or trigeminal autonomic cephalalgia. Other exclusion criteria were (1) severe psychiatric disorder (such as major depressive disorder), (2) history of oncological disease, or (3) contra-indication for lumbar puncture (LP) (signs and symptoms of increased intracranial pressure, local skin infection, or a coagulopathy including use of anti-coagulant drugs or platelet-inhibitors).
Participants were asked to fill out a questionnaire on the day of the LP that included questions related to their migraine characteristics and possible history of depression. To compute symptoms of depression (either current of past depressive symptoms), additional questionnaires were preferentially completed on the day of LP but otherwise extracted from electronic medical records. The presence of symptoms of depression was determined based on previously described criteria. 29 In short, symptoms of depression were determined using validated cut-off scores for the (CES-D). Depressive symptoms was defined as HADS-D ≥ 8 or CES-D ≥ 16 or (past) depression diagnosed by a physician or (past) use of antidepressants for depression.
Cerebrospinal fluid collection
Sampling and handling of CSF samples was described in Onderwater et al. 28 In brief, samples were collected between 2008 and 2016, the time of the LP was between 8:30 a.m. and 1:00 p.m. and in random order to minimize diurnal and seasonal variation. Participants were required to refrain from eating or drinking, apart from water and to abstain from smoking, use of hash and other recreational drugs, for at least 8 h prior to sampling. Sampling occurred interictally with migraine individuals being attack-free for a minimum of 3 days. Participants were urged to refrain from the use of prophylactic or any other chronic medication (other than oral contraceptives) in the four weeks preceding the LP. The LP and subsequent CSF collection were performed in a standardized matter to limit inter-individual variation.
For endocannabinoid measurements, 3 mL CSF was sampled directly in a 15-mL polypropylene Falcon tube (Cat. No. 188271; Greiner Bio-One B.V.) that already contained 6 mL of ice-cold ethanol (to instantly stop any metabolic activity). The tube was immediately put back on ice after CSF collection. After gently shaking the tube, the CSF was divided in aliquots of 1.5 mL in 1.8-mL cryotubes (Art. No. 368632; NUNC Brand, Sigma-Aldrich, Zwijndrecht, The Netherlands). The cryotubes were transferred to a −80°C freezer as soon as possible. All CSF samples remained at −80°C until sample preparation for analysis.
Analysis of endocannabinoids using micro-LC-MS/MS
The analysis of endocannabinoids in CSF was performed using a validated method. 30 Sample preparation, except the evaporation step, was carried out under ice-cold conditions. Analytes were extracted using liquid-liquid extraction. In brief, 750 µL of CSF samples (CSF:ethanol = 1:2, v/v) was evaporated to approximately 100 µL using a SpeedVac (Thermo Fisher Scientific, Waltham, MA, USA). Then, 10 µL of isotopically labelled internal standard solution and 50 µL of a buffer solution (0.1 M ammonium acetate solution, adjusted to pH 4 with formic acid) were added to each sample. One milliliter of methyl-tert-butylether (MTBE) was then added prior to agitation for 10 min using a bullet blender and subsequent centrifugation for 5 min at 16,000 g. The organic supernatant (900 µL) was collected and evaporated to dryness using the SpeedVac. The dry residues were then reconstituted in 20 µL of an ice-cold solution of water and acetonitrile (ACN) 50:50 (v/v), prior to agitation (20 min) and centrifugation at 16,000 g for 50 min. Finally, 15 µL of the supernatant was transferred into a glass vial and 3 µL was injected into a nanoAcquity micro-LC system (Waters Corporation, Mildford, MA, USA) hyphenated with a Shimadzu 8060 triple quadrupole mass spectrometer (Shimadzu Corporation, Kyoto, Japan). Separation was performed using a micro C18 column (0.3 × 150 mm, 2.6 μm) from Phenomenex (Torrance, CA, USA) maintained at 45°C. The mobile phase was composed of 2 mM ammonium formate and 10 mM formic acid in water (A), and acetonitrile (B). The flow rate was 4 μL/min. Ionization of the compounds was performed using a customized micro-electrospray ionization (micro-ESI) source in positive mode. Selected Reaction Mode (SRM) was used for MS/MS acquisition. SRM transitions were individually optimized for targeted analytes and respective isotopically labelled internal standards. Data acquisition and pre-processing was performed using LabSolutions LCMS Version 5.97 SP1 (Shimadzu Corporation). Data quality was monitored using regular injection of quality control (QC) samples prepared from pooled CSF. Samples were injected in a randomized order. QC samples were used to correct for inter-batch variations using the in-house developed mzQuality workflow (available at http://www.mzQuality.nl). Relative standard deviations (RSDs) of peak area ratios were calculated for each targeted analyte detected in the QC samples. The absolute concentration of the endocannabinoids in CSF samples was calculated using calibration samples. Quality control was set on RSDqc < 15% and blank effect < 15%. The data as relative response ratios (target area/ISTD area; unit free) of these metabolites after QC correction were calculated and converted to concentrations.
Statistical analysis
Principal component analysis (PCA) was performed on the concentration measurements of all measured endocannabinoids together. Based on the first two principal components outliers were identified by visually inspecting the plots. Log10-transformed endocannabinoid concentrations (pM) were used for further statistical analyses. Multivariate linear regression was used to detect metabolite differences between individuals with migraine and healthy controls for each endocannabinoid separately. Based on literature, BMI, sex, age, weekly alcohol consumption, cigarettes per day, drug use and depressive symptoms were identified as potential covariates and therefore included as independent variables. Prior to data analysis, missing data for relevant covariates was imputed with Multiple Imputation by Chained Equations (MICE). 31 For MICE, we used 10 imputations and 30 iterations as settings and included the following variables: Log10 endocannabinoid concentrations, age, sex, BMI, migraine without aura/migraine with aura/control-stratus, depression score, drug use and the amount of alcohol and smoking. Regression analyses were performed on the imputed data and results were pooled. All data analyses were performed using R version 4.3.1. and RStudio version 2023.06.0 + 421 (RStudio: Integrated Development for R. RStudio, PBC). 32 P-values of ≤ 0.05 were considered statistically significant.
Results
Clinical characteristics
Of all measured endocannabinoids the levels of AEA, 2-AG, and DHEA in CSF of 195 individuals with episodic migraine (n = 98 migraine with aura (MA); n = 97 migraine without aura (MO)) and 94 healthy controls were reliably measured; for 5 individuals there was not enough CSF sample available (< 1.5 mL). Next, one population outlier with migraine with aura was excluded based on the PCA plot, leaving 194 people with migraine and 94 controls for the statistical analysis. The clinical characteristics are shown in Table 1. Sex distribution (two third female) of this selected group was similar between cases and controls. There were no differences between the migraine groups, except for a higher monthly attack frequency in migraine without aura (2.0 IQR 1.0–3.5) versus migraine with aura (1.5 IQR 1.0–3.0) (p = 0.017). There was a difference between the three groups in, total HADS related score (p < 0.001), total CES-D score (p < 0.001) and weekly alcohol consumption (p = 0.009) and headache days (p < 0.001) (Table 1). Additional analyses showed a difference between those with migraine and controls, as those with migraine had more headache days (p < 2.2 × 10− 16 ) a higher total HADS score (p = 9.147 × 10−9) and CES-D score (p = 7.217×10−7), but consumed less alcohol in units of alcohol per week (p = 0.006). This is in line with prior results on migraine comorbidities and lifestyle characteristics, as those with migraine more often suffer from headache, symptoms of depression and are more inclined to refrain from alcohol.2,3,33 Data was assumed to be missing at random for weekly alcohol consumption (n = 6 (3 MA and 3 MO)), migraine days (cases n = 7 (5 MA and 2 MO), depressive symptoms (n = 45 (cases n = 13 (8 MA and 5 MO), controls n = 32)), HADS scores (n = 9 (1 MA and 1 MO), controls n = 7)), total CES-D (n = 48 (cases = 16 (9 MA and 7 MO), controls = 32)) and drug use (n = 1 (cases n = 1 (1 MA), controls n = 0)). The missing values used for the regression analysis were imputed. No group differences were observed for fasting time (in hours) and time of CSF collection (data not shown). In addition, no time effect of collection time or storage time was observed (data not shown).
Characteristics of control and migraine patient cohort
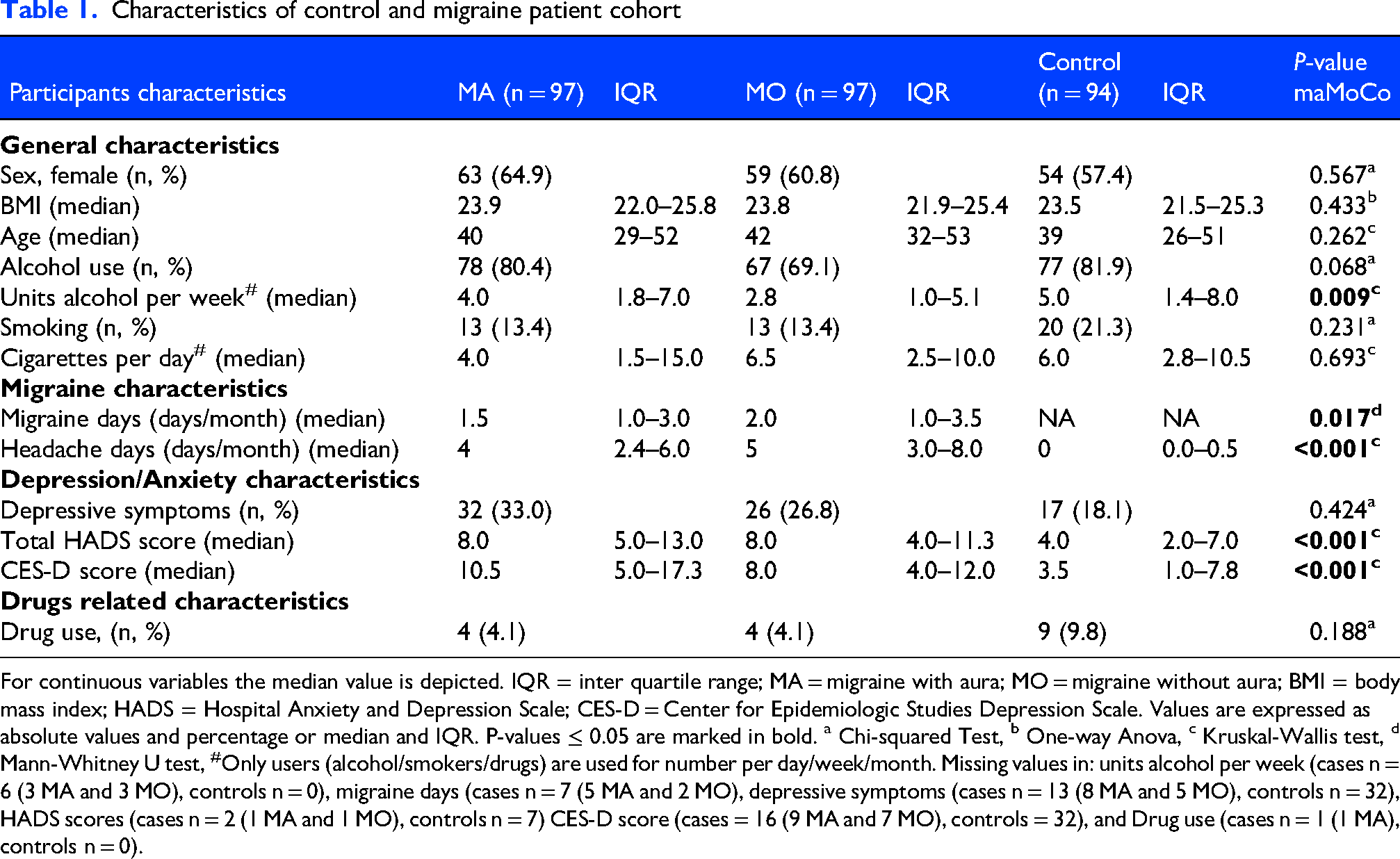
For continuous variables the median value is depicted. IQR = inter quartile range; MA = migraine with aura; MO = migraine without aura; BMI = body mass index; HADS = Hospital Anxiety and Depression Scale; CES-D = Center for Epidemiologic Studies Depression Scale. Values are expressed as absolute values and percentage or median and IQR. P-values ≤ 0.05 are marked in bold. a Chi-squared Test, b One-way Anova, c Kruskal-Wallis test, d Mann-Whitney U test, #Only users (alcohol/smokers/drugs) are used for number per day/week/month. Missing values in: units alcohol per week (cases n = 6 (3 MA and 3 MO), controls n = 0), migraine days (cases n = 7 (5 MA and 2 MO), depressive symptoms (cases n = 13 (8 MA and 5 MO), controls n = 32), HADS scores (cases n = 2 (1 MA and 1 MO), controls n = 7) CES-D score (cases = 16 (9 MA and 7 MO), controls = 32), and Drug use (cases n = 1 (1 MA), controls n = 0).
CSF levels of AEA, 2-AG and DHEA in migraine patients and controls
Multivariate linear regression analyses showed that there were no differences in concentrations in migraine with aura or migraine without aura versus control for each of the three endocannabinoids (Figure 1A-C) p = 0.46 and p = 0.08 for AEA, p = 0.46 and p = 0.90 for 2-AG and p = 0.58 and p = 0.79 for DHEA, respectively (Supplementary Table 1). Some of the covariates, however, did have a significant effect on endocannabinoid concentration in the regression model. AEA concentration was associated with sex (β = -0.081; 95% CI: −0.12 to −0.04, p < 0.001) and number of cigarettes per day (β = 0.007; 95% CI: 0.00 to 0.01, p = 0.004). Female sex was associated with a lower AEA concentration (Figure 2A) and the number of cigarettes per day was positively correlated with the AEA concentration (Figure 2B). 2-AG concentration was also negatively correlated with female sex (β = -0.084; 95% CI: −0.12 to −0.05, p < 0.001) (Figure 3A) and positively correlated with depressive symptoms (β = 0.054; 95% CI: 0.014 to 0.09, p = 0.008) (Figure 3B and 3C). DHEA concentration was positively correlated with age (β = 0.003; 95% CI: 0.00 to 0.00, p < 0.001), BMI (β = 0.010; 95% CI: 0.00 to 0.02, p = 0.013), smoking per day (β = 0.006; 95% CI: 0.00 to 0.01, p = 0.03), alcohol units per week (β = 0.004; 95% CI: 0.00 to 0.01, p = 0.033), and also negatively correlated with female sex (β = -0.046; 95% CI: −0.08 to −0.00, p = 0.034), and drug use (β = -0.102; 95% CI: −0.20 to −0.00, p = 0.042) (
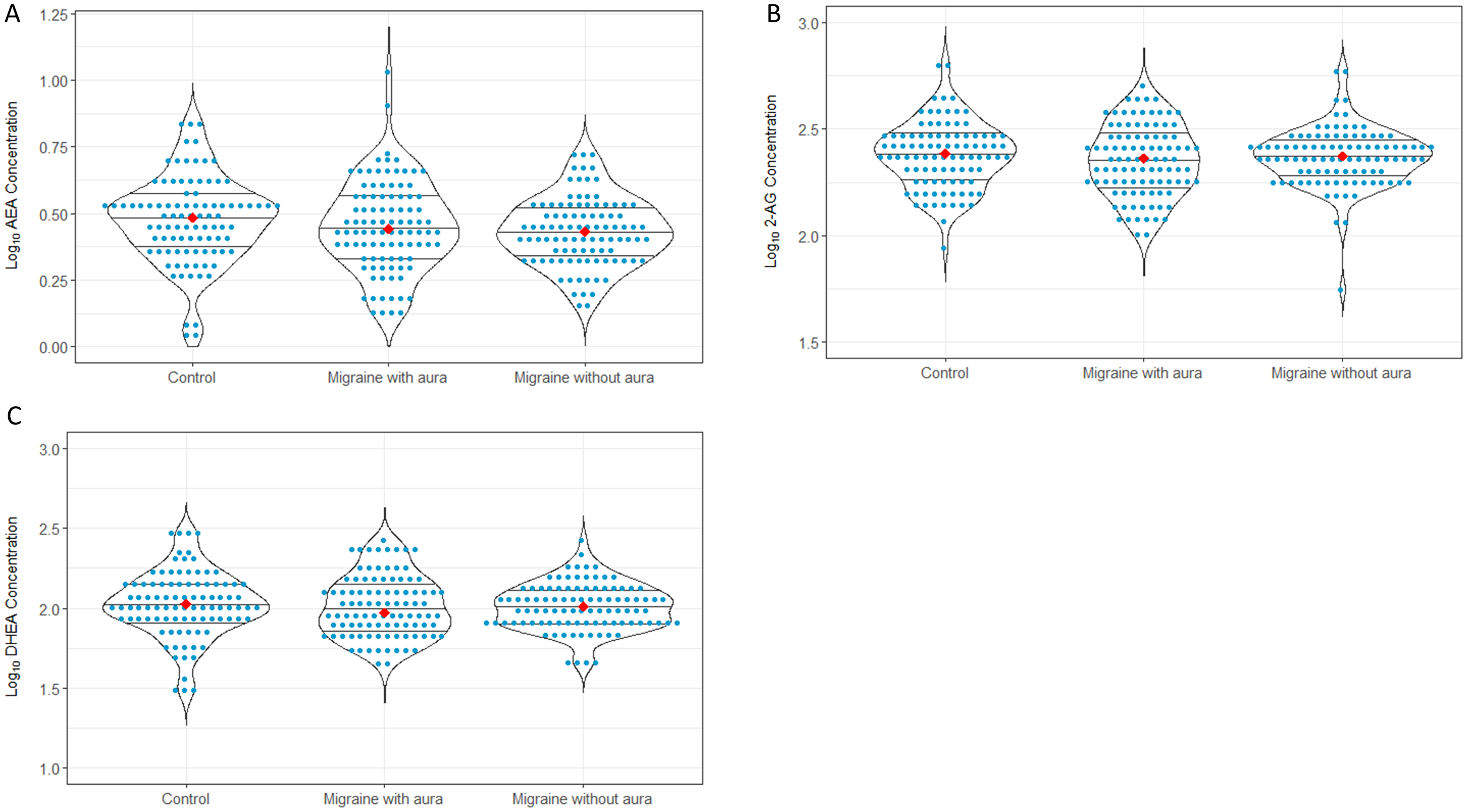
Endocannabinoid concentration per subgroup.
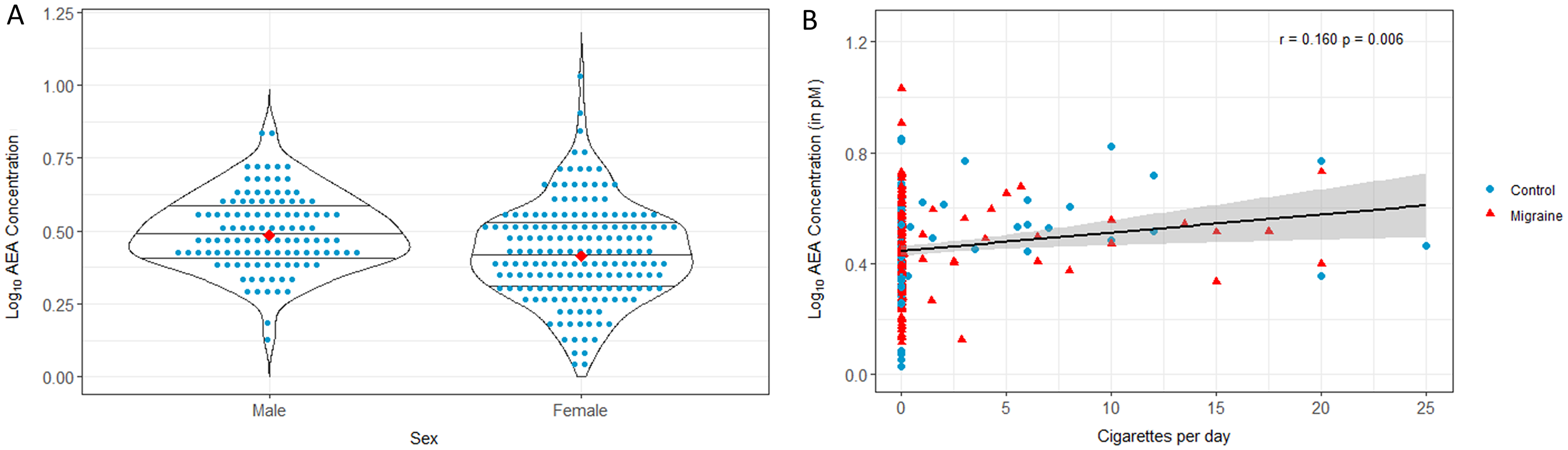
Relation of AEA concentration with covariates.

Relation of 2-AG concentration with covariates.

Relation of DHEA concentration with covariates.
Discussion
Here we measured and compared concentrations of the endocannabinoids AEA, 2-AG, and DHEA in CSF of 194 individuals with migraine with (n = 97) or without aura (n = 97) outside migraine attacks (interictal state) compared with 94 healthy matched controls to determine whether the endocannabinoid system is disrupted in interictal episodic migraine patients and whether depressive symptoms were of influence. The CSF sampling and processing was strictly protocoled, and the analysis was performed with our validated micro-LC-MS/MS method. 30 As for our primary outcome we found no differences in endocannabinoids related to migraine status, so we regard this a negative study. For our secondary outcome, however, covariates age, sex, daily number of cigarettes, units alcohol per week, drug use, depressive symptoms and BMI, all had an effect on the different endocannabinoid concentrations.
The effect that the covariates have on the endocannabinoids concentrations in CSF emphasizes the complexity of the endocannabinoid system regarding confounding factors. Interestingly, 2-AG levels were positively correlated with depressive symptoms, which has implications for further research as comorbidity with depression in migraine patients makes them also more prone for chronification and medication overuse. 34
So far, only two studies have assessed the levels of endocannabinoids in body fluids of individuals with migraine, but the results are contradictory.21,35 In one study, concentrations of AEA were lower and those of the endocannabinoid analogue PEA were higher in the CSF of 15 individuals with chronic migraine versus 20 age-matched controls. 21 However, in that study, the analysis of endocannabinoids was based on a different extraction method (i.e., the Bligh and Dyer liquid-liquid extraction method), which may generate AEA during the analytical step (see Figure S1, supplemental material). Most importantly, there was no correction for confounding factors, as was done in our study. Given that chronic migraine often coincides with depression one should wonder whether the difference found by Sarchielli et al. 21 is actually due to depression or other confounding factors rather than migraine status. Addmittedly, the current study encompasses a less severly affected migraine cohort that could in part also be explanatory for the difference in results. In the other study, 16 different endocannabinoids were measured by LC-MS/MS in blood plasma from 38 females with episodic migraine between attacks and 26 healthy controls collected on days 1 and 14 of the menstrual cycle. 35 In line with our study, there were no differences for AEA and N-acylethanolamines. In addition, in a subset of study participants endocannabinoids were measured in plasma collected during attacks and compared with the interictal measurement; again, no differences were found. 35 In both studies, the number of participants was limited, the body fluids in which the measurements were done were different, the sampling conditions were not protocoled, and no correction for possible confounding factors was done. Because no prior CSF endocannabinoid study in migraine with low-frequency attacks existed, we estimated 50 patients per group from comparable literature 36 and our preliminary data, but enrolled nearly twice as many to minimize the chance of missing clinically meaningful differences.
In addition to the well-established relation between depression and endocannabinoids, endocannabinoids have also been associated with BMI, sex, age, weekly alcohol consumption, smoking and drug use.9,37–39 Energy homeostasis is one of the processes best known to be controlled by the endocannabinoid system.9,40,41 Although the pathways underlying sex differences in the endocannabinoid system are not fully elucidated, it is generally accepted that differences exist between the male and female endocannabinoid system.42,43 Female rats had different concentrations of AEA and 2-AG compared to male rats in different brain structures. 44 The endocannabinoid system is involved in the reward circuits of the brain, so an effect of drug use on the endocannabinoid system is not surprising.39,45 Additionally, studies in mice have found that chronic exposure to ethanol leads to increased levels of AEA and 2-AG. 46 There is some evidence on a decrease in the expression of CB1 molecules and an increase in the AEA level in smokers.47,48 Given that these factors could influence both the exposure and the outcome, they were considered when studying endocannabinoid levels in the present study.
Contrary to most previous presented evidence on the influence of endocannabinoids in migraine pathophysiology,10,21,49,50 in our CSF study, no association was detected between the levels of certain endocannabinoids and (episodic) migraine, at least not in the interictal phase. A dysregulation of the endocannabinoid system might have remained undetected in case it involves only a localized (e.g., near the synapse) or short-lasting migraine-attack related disturbance of the endocannabinoid system, and not a steady-state adaptation of the body to experienced migraine attacks. Future studies should focus on endocannabinoid levels during an attack to discern whether there is a difference in concentration that can be directly related to a migraine attack itself. Further limitations of our study are that due to the size of the study and the great care taken to match our study groups, including for age, sex and diurnal and seasonal time of sampling, that the samples were collected over a long period of time. This could have potentially affected the stability of the compounds studied, even though they were stored at the recommended −80°C. 51 We acknowledge that the collection of samples was done over a fairly long time, which is hard to avoid for a difficult to obtain body fluid as CSF and the samples had been stored for variable time in the freezer (in all cases for at least 6 years) until measurement in 2022, as the method to analyze endocannabinoids first needed to be developed. However, the actual pre-analytical phase was protocoled and running of the analyses was done in consecutive batches in only a few days, so we feel that the variation in collection and storage did not have a major influence on the outcome, also because we took along quality control and blank samples for each run. Furthermore, only minor changes of oxylipins were observed after prolonged storage at −80°C of blood samples and the metabolome and lipidome of CSF were found to be stable for longer periods.51,52 Additionally, we have focused on patients with episodic migraine to investigate whether there is a difference with controls outside of an attack. Strong exclusion criteria and guidelines were used in this study, such as medication use prior to the study; hence most participants are on the milder end of the episodic migraine spectrum. This study population was chosen to investigate the relation with endocannabinoids as “purely” as possible. However, this might limit the generalizability of our results.
Our study also has several strengths. First, we studied and compared CSF from uniquely large groups of people with migraine and controls. Moreover, unlike other CSF studies, control samples were collected from people who can be considered healthy and had not undergone a lumbar punction because of neurological symptoms and almost all had no first-degree relatives with migraine. 53
Second, sample preparation for assays and the demographic characteristics of patients can contribute to variability of metabolite concentrations. Thus, when investigating a putative role of endocannabinoids in disease, it is crucial to use standardized protocols as the collection and processing of endocannabinoid samples can affect the concentration.51,54
Furthermore, it is imperative to correct the statistical model for possible confounders, in our case most importantly, depression. We want to stress that multivariate linear regression analysis was used in our study to model the relationship between endocannabinoids and explanatory variables simultaneously. Although people with major depression were excluded in our study, we found a positive correlation between 2-AG and depressive symptoms, as screened with the validated tools (HADS-D and CESD) for depressive symptomatology. Previous research on the role of AEA and 2-AG in depression has been conducted primarily in individuals with major depressive disorder (MDD).26,55 The hypothalamic–pituitary–adrenal (HPA)–axis, neurogenesis and neuroinflammation have all been implicated in the etiology of MDD, 56 and all are dependent on proper functioning of the endocannabinoid system, 24 suggesting a crucial role for the endocannabinoid system in MDD. Given the increased risk of depression in migraine, it is important to realize that depressive symptoms may have a significant effect on endocannabinoid levels, even when MDD has been ruled out. The association between migraine and endocannabinoids may therefore depend on depressive symptomatology rather than on migraine itself. Our study shows that depressive symptoms functions as confounder on the relationship between migraine and endocannabinoid levels. Again, it is important to note that our study was not designed to specifically investigate the role of depression, but given our results and the current literature, 26 it is likely that depression has a confounding effect on the relationship between migraine and endocannabinoids. One should realize that in studies that are similar to ours, finding an association between migraine and endocannabinoid levels, or not, might possibly be due to whether or not depressive symptoms were taken along as confounding factor in the statistical model. Afterall, given that migraine and depression are comorbid conditions, it is very likely that in such studies a considerable number of migraine cases may have suffered from depressive symptoms. Again, future studies should therefore take depressive symptomology into account when studying the role of the endocannabinoid system in migraine. Contrary to many studies to minimize possible confounding effects, we have added drug-use of participants as a variable to our statistical model. Thus, we believe the effect of drug-use on our outcome to be negligible. However, a complete abolishment of any confounding effect can never be claimed.
In conclusion, CSF endocannabinoids may not serve as effective biomarkers for distinguishing interictal migraine individuals from controls. However, 2-AG levels are likely linked to depressive symptoms, but also sex, BMI, smoking and alcohol use were of influence on AEA, 2-AG, and DHEA levels. This study shows the relevance of endocannabinoids in patients with migraine and highlights the intricate and complex role of the endocannabinoid system in relation to both migraine and confounding factors, such as depressive symptoms.
Highlights
The study reveals a significant link between CSF levels of the endocannabinoid 2-AG and depressive symptoms, offering new insights into the neurochemical basis of comorbid migraine and depression.
These findings underscore the broader importance of the endocannabinoid system in understanding the complex interplay between episodic migraine and depression.
By highlighting the role of endocannabinoids beyond diagnostic biomarkers, our research opens new avenues for exploring therapeutic targets in migraine-related mood disorders.
Supplemental Material
sj-xlsx-1-cep-10.1177_03331024261451250 - Supplemental material for Endocannabinoid cerebrospinal fluid levels in migraine and its relation to symptoms of depression
Supplemental material, sj-xlsx-1-cep-10.1177_03331024261451250 for Endocannabinoid cerebrospinal fluid levels in migraine and its relation to symptoms of depression by Aster V.E. Harder, Xinyu Di, Wendy M. Winter, Bingshu He, Robin M. Van Dongen, Gerrit L.J. Onderwater, Erik W. Van Zwet, Elke H.J. Krekels, Isabelle Kohler, Michel D. Ferrari, Amy C. Harms, Arn M.J.M. Van Den Maagdenberg, Thomas Hankemeier and Gisela M. Terwindt in Cephalalgia
Supplemental Material
sj-png-2-cep-10.1177_03331024261451250 - Supplemental material for Endocannabinoid cerebrospinal fluid levels in migraine and its relation to symptoms of depression
Supplemental material, sj-png-2-cep-10.1177_03331024261451250 for Endocannabinoid cerebrospinal fluid levels in migraine and its relation to symptoms of depression by Aster V.E. Harder, Xinyu Di, Wendy M. Winter, Bingshu He, Robin M. Van Dongen, Gerrit L.J. Onderwater, Erik W. Van Zwet, Elke H.J. Krekels, Isabelle Kohler, Michel D. Ferrari, Amy C. Harms, Arn M.J.M. Van Den Maagdenberg, Thomas Hankemeier and Gisela M. Terwindt in Cephalalgia
Footnotes
ORCID iDs
Consent to participate
All participants provided written informed consent prior to participation in the study.
Consent for publication
All authors have agreed to publish this work in Cephalalgia.
Ethical considerations
The study was conducted according to the criteria of the Declaration of Helsinki and was approved by the Leiden University Medical Center institutional ethics committee.
Author contributions
Funding
This study was supported by the Dutch Research Council (NWO) (VICI 918.56.601 and Spinoza 2009 to M.D. Ferrari, Vidi 917.11.31 to G.M. Terwindt), the Netherlands Organization for Health Research and Development (ZonMw) (Clinical Fellowship 90700217 to G.M. Terwindt), and European Community (EC) FP7-EUROHEADPAIN – no. 602633 (to M.D. Ferrari and A.M.J.M. van den Maagdenberg).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data not published within the article is available from the corresponding author upon reasonable request.
Open practices
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.