
Abstract
Background
The role of angiotensin II receptor blockers (ARBs) in migraine prophylaxis varies globally, partly due to insufficient evidence from randomized controlled trials (RCTs) supporting their efficacy. We aimed to conduct a systematic review and meta-analysis of ARBs in migraine prophylaxis.
Methods
We searched PubMed/MEDLINE, Embase, Cochrane, Google Scholar, Clinicaltrials.gov, ITCRP, and EudraCT from database inception to 22 September 2025. The searches were conducted between 19 and 22 September 2025 for controlled trials comparing any ARB to placebo or other preventive migraine drugs in individuals with episodic or chronic migraine. Guidelines, letters, editorials, narrative reviews, case reports, and news were excluded. Summary data were extracted by two reviewers, and random-effects meta-analyses were performed, with heterogeneity assessed using Cochrane I2 statistic. Primary outcomes were monthly headache/migraine days or attacks, and response rates. Adverse event occurrence was also assessed. The risk of bias was assessed using the Cochrane RoB2 tool and the certainty of evidence was assessed using GRADEpro. The study was pre-registered in Prospero (CRD42023405372) and received no funding.
Results
Four trials published between 2003 and 2025 were included in the meta-analysis: three RCTs on candesartan, and one on telmisartan. All four studies reported the outcomes migraine days and responder (≥50% reduction of migraine days) rates, and three reported headache days. A total of 659 participants were included in the meta-analysis. The combined effect size for migraine days and headache days were reductions of −1.00 (95% CI: −1.51 to −0.49, p<0.001), and −1.21 (95% CI: −1.62 to −0.81, p<0.001) days per month from baseline respectively. The odds ratio for being a responder was 2.68 (95% CI: 1.91 to 3.78, p<0.001). The certainty of evidence was low for migraine days, moderate for responder rates and high for headache days, with heterogeneity between studies categorized as ‘might not be important’ and no serious risk of bias.
Discussion
The systematic review and meta-analysis provide robust evidence on the effect of ARBs, particularly candesartan, in prevention of episodic migraine, supporting the rationale for reconsidering its position in international guidelines.
Trial Registration
Prospero CRD42023405372
This is a visual representation of the abstract.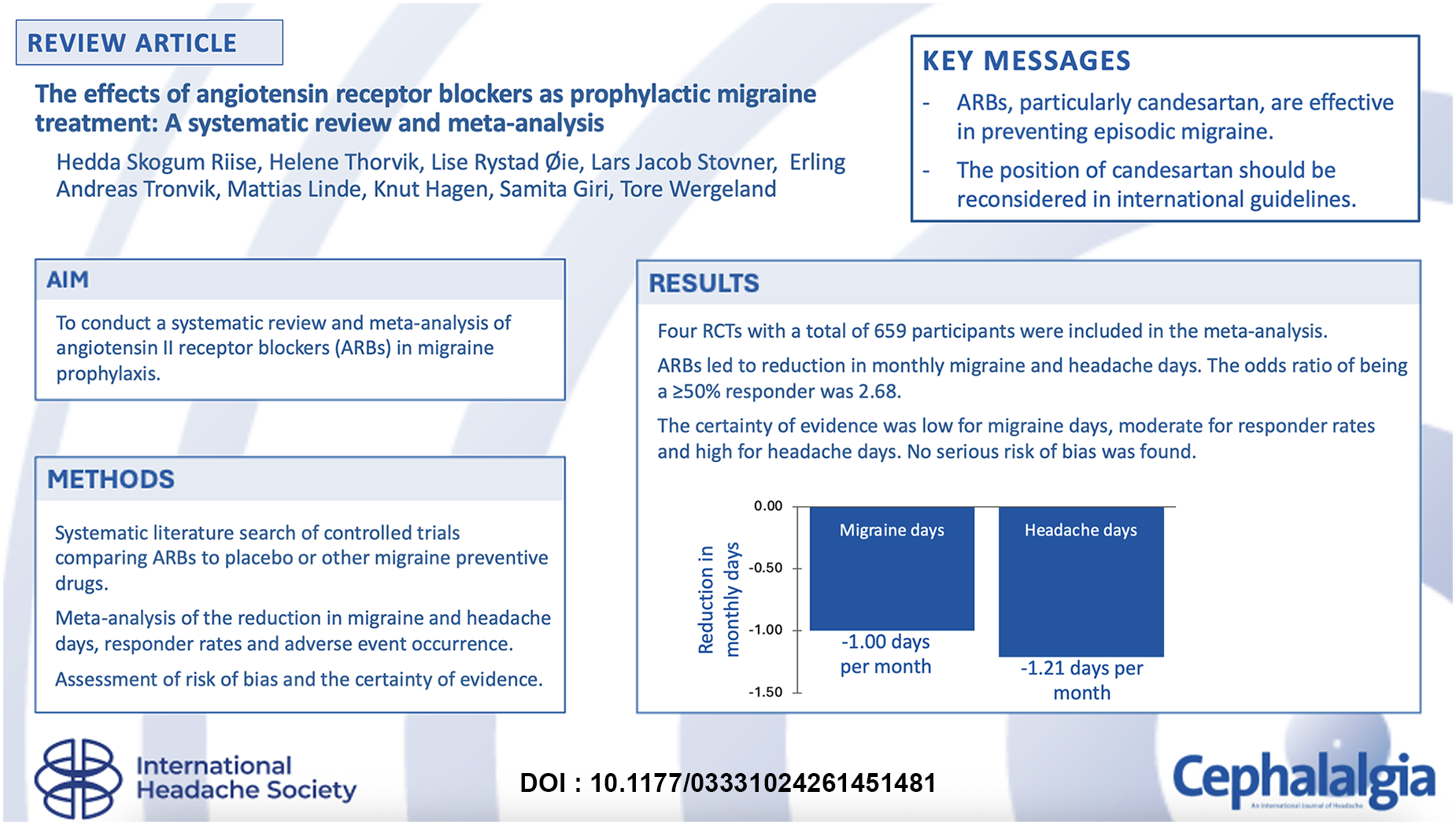
Background
Oral prophylactic treatment options for migraine comprise several repurposed drugs from diverse drug classes, including antihypertensives. Among the antihypertensives used for migraine prophylaxis are beta-adrenergic receptor antagonists and drugs targeting the renin-angiotensin-aldosterone system, such as angiotensin II receptor blockers (ARBs).
The role of ARBs in migraine prophylaxis differs around the world, partly due to insufficient evidence from randomized controlled trials (RCTs) supporting their efficacy. For instance, European consensus statement 1 and the American Headache Society 2 list candesartan as a first-line option, whereas Japanese guidelines give only a weak recommendation for its use in migraine prophylaxis. 3 The International Headache Society guidelines indicate that the quality of evidence supporting candesartan for migraine prevention is low when chronic and episodic migraine are assessed together, and moderate in episodic migraine. 4 The limited evidence base for ARBs in migraine prophylaxis has confined their use to off-label practice in many health care systems, 5 which may restrict reimbursement and availability. Previous meta-analyses on the topic have focused on multiple drug classes 6 or several different types of anti-hypertensive drugs 7 simultaneously, and do not include a recently published RCT on candesartan. 8
The aim of this paper was to conduct a systematic review and meta-analysis evaluating the effects and safety of ARBs in migraine prophylaxis.
Methods
The systematic review and meta-analysis was conducted according to the Cochrane Handbook for Systematic Reviews of Interventions, 9 and the recommendations of Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) statement. 10 The systematic review and meta-analysis was pre-registered in Prospero (CRD42023405372).
Search strategy and selection criteria
The search was carried out 19–22 September 2025, searching the databases from inception to 22 September 2025. We used both thesaurus and free text terms of the two main concepts ‘migraine’ and ‘angiotensin-II receptor blockers’. The concepts were combined and adapted to search the following databases: MEDLINE/PubMed, Embase, Cochrane, Google Scholar, WHO International Clinical Trials Registry Platform (ITCRP), European Union Drug Regulating Authorities Clinical Trials Database (EudraCT), and ClinicalTrials.gov. The search results were imported to PICO Portal 11 where duplicates were removed. Only the first 100 results in Google Scholar were imported. A concept table for the literature search can be found as Supplementary Table 1 (Additional file 2).
Studies included were non-randomized or randomized controlled trials, both parallel group and crossover, examining the effects of ARBs as migraine prophylaxis. The studies were required to compare the effect of ARBs (any dosage) with placebo or other migraine preventive medications in individuals diagnosed with episodic or chronic migraine. The studies were required to report a primary outcome; either monthly migraine or headache days, number of headache or migraine attacks per month, and/or response rates (30%, 50% or other). Headache days and attacks include all types of headache, encompassing both migraine and non-migraine days and attacks. Secondary outcomes included reduction of acute headache medication usage, adverse events (AEs), health-related quality of life, and disability. No restrictions were applied regarding publication date or language. Guidelines, letters, editorials, narrative reviews, case reports, news and retrospective studies were excluded.
Articles identified in the literature search were screened independently by two reviewers (HSR and HT), using the systematic review platform PICO Portal. 11 Screening was conducted in two sequential stages: first based on titles and abstracts, followed by full-text assessment. Full-text articles were retrieved in collaboration with the Medicine and Health Library at The Norwegian University of Science and Technology (NTNU), and by reaching out to the corresponding author directly via E-mail. Any disagreements between the two reviewers at any stage were resolved through discussion, potentially with a third reviewer (SG) if needed.
Data collection process
Data from the studies was extracted independently by the two reviewers using a premade data collection form (Additional file 1). This included study details/characteristics, methodology, characteristics of participants, information about intervention and comparison groups, and outcomes, and was also used to confirm the eligibility of the studies.
Risk of bias assessment
Risk of bias was assessed for each predefined primary outcome. This assessment was done independently by the two reviewers using the Cochrane Risk of Bias in randomized trials 2 (RoB2) tool. 12 Any disagreements were resolved through discussion with a third reviewer (SG). The assessment included risk of bias arising from five different domains; randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. 13 An extra domain was used to assess the risk of bias in cross-over studies; ‘Risk of bias arising from period and carryover effects’. 14 Each outcome was given a score of ‘Low risk’, ‘High risk’ or ‘Some concerns’ in each of the five domains based on the answers to the signaling questions and the accompanying algorithm. 13 The total risk of bias for the outcome was then assessed. We utilized both the full-text articles and the study protocols, if available.
Certainty of evidence assessment (GRADE)
The certainty of the evidence for the different outcomes across the studies was assessed using the Cochrane GRADE approach (Grading of Recommendations, Assessment, Development, and Evaluations). 15 The assessment was done by the two reviewers using the GRADEpro tool. 16 Each outcome was assessed according to five domains: risk of bias, inconsistency of results (heterogeneity), indirectness of evidence, imprecision, and publication bias. The certainty for each outcome was assessed as either ‘high’, ‘moderate’, ‘low’ or ‘very low’. 15
Analysis
Estimates were extracted by HSR & HT from the included studies and converted to a standardized summary statistic with 95% confidence interval (CI) when necessary (mean difference for continuous outcomes). We sought to present continuous outcomes as mean change from baseline with standard deviations (SDs). If this was not reported as the summary estimate in the papers, the data was requested from the authors or, if unavailable, calculated. We standardized headache/migraine frequency measurements to a 4-week time period for studies presenting data from longer time spans (e.g., 12 weeks). Data were then transferred to STATA 18.5 (StataCorp LP, College Station Texas, USA), and random effect meta-analysis was performed. A random-effects model was used to account for between-study heterogeneity in populations and outcome definitions, given expected clinical and methodological heterogeneity across studies (e.g., populations, interventions, and outcome definitions). Mean differences and odds ratios were used as statistical outcome measures in the meta-analysis. When studies included more than one intervention group (e.g., two different doses), a single combined estimate from these two groups was used for the single pairwise comparison to avoid unit-of-analysis error. 14 Narrative syntheses were applied to secondary outcomes where meta-analysis was not feasible. Meta-analysis of reductions in acute headache medication use was not performed due to heterogeneity in outcome reporting (e.g., days vs. doses). Health-related quality of life and disability were each reported by a single study, precluding quantitative synthesis. Subgroup analyses based on dose, comparison groups or age groups were not feasible due to a limited number of studies. Additional meta-analysis restricted to candesartan was performed.
Results of the meta-analysis are presented in forest plots, with box size indicating weighting of the independent studies. Weighting was calculated using an inverse variance method. Heterogeneity was assessed using Cochrane I2 statistic and categorized as ‘might not be important’ (≤40%), ‘moderate’ (30%-60%), ‘substantial’ (50%-90%) or ‘considerable’ (75%-100%). 17
Results
After removing duplicates and supplemental records, 1037 records entered the screening process. After abstract screening, 19 articles were identified for full-text retrieval. One article was not retrieved in full-text, despite reaching directly out to the author. This was an abstract titled ‘Comparison of Onabotulinumtoxin A with other preventive medications (amitriptyline, topiramate and candesartan) in the management of chronic migraine’, presented at the International Conference on Central Nervous System Disorders & Therapeutics in 2016. 18 After full-text review, six RCTs met the eligibility criteria and were included in the review.8,19–23 Four of these were included in the meta-analysis.8,19–21 The selection process and reasons for exclusion at full-text screening are summarized in a PRISMA flow diagram (Figure 1).
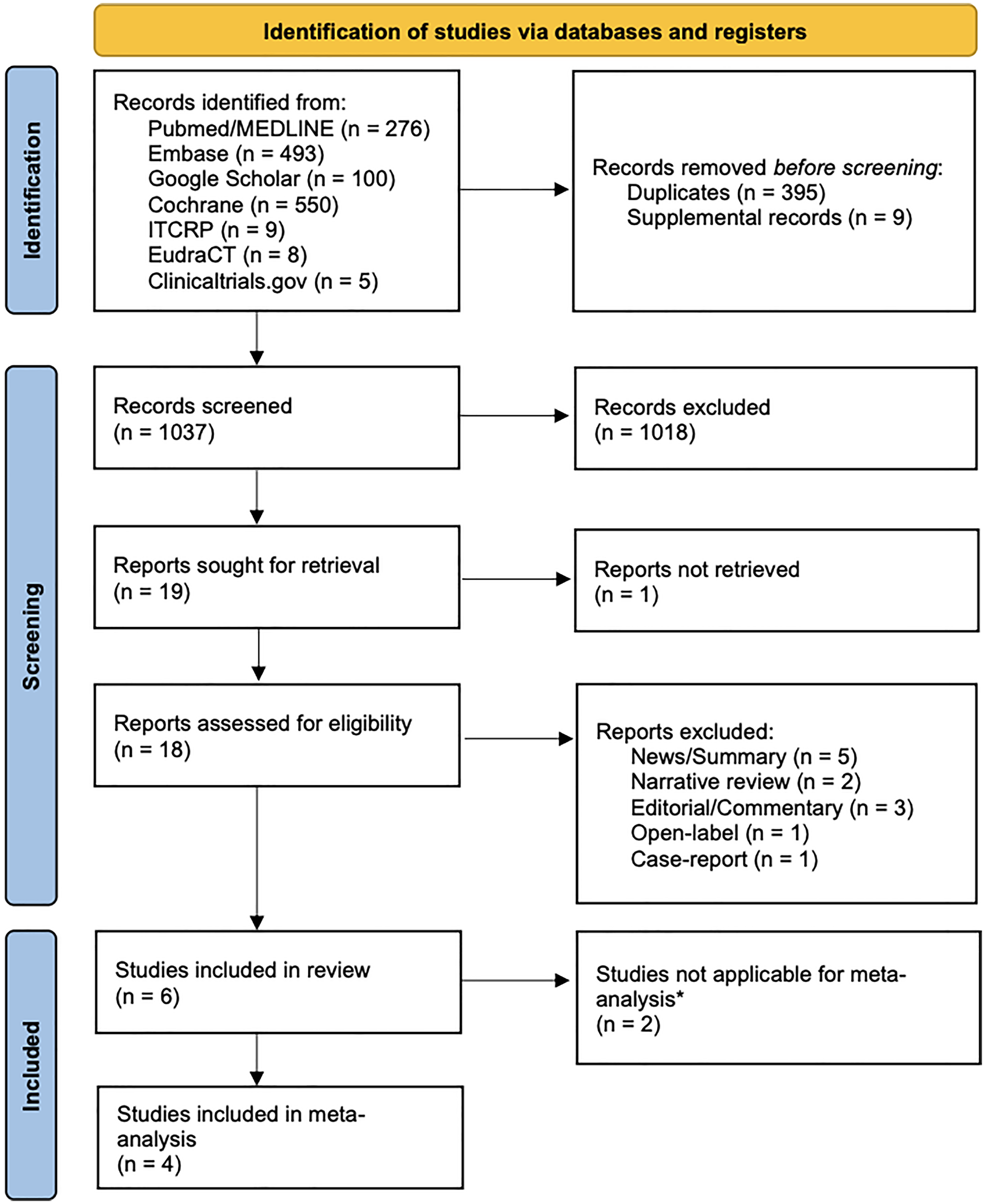
PRISMA Flow Diagram showing the selection process, Adapted from PRISMA statement, 10 licensed under CC BY 4.0.
Of the included studies, three investigated candesartan,8,19,20 two telmisartan,21,22 and one valsartan 23 (Table 1). Two studies were not included in the meta-analysis:’one on valsartan by Mosarrezaii et al. (2025) 23 and one on telmisartan by Carcel et al. (2025). 22 The study by Mosarrezaii et al. (2025) 23 was conducted in Iran, comparing valsartan 40 mg to propranolol. The only relevant outcome reported was the number of headache attacks per month, which could not be combined with other data for the meta-analysis. We reached out to the authors to access any additional data but did not receive any response, and it was not possible to access the preregistration of the study. The paper concluded with valsartan being as effective as propranolol and did not present any data on side effects. The study by Carcel et al. (2025) 22 was an Australian pilot RCT, investigating triple combination of antihypertensive treatment (telmisartan 20 mg, amlodipine 2.5 mg, and indapamide 1.25 mg). As it was impossible to isolate the effects of telmisartan, the study was not included in the meta-analysis. The authors concluded with the combination treatment being safe and well-tolerated, although the study was not powered to detect efficacy.
Characteristics of included studies. Study design, country and setting, intervention and comparator groups, sample size, study duration, participant characteristics (age and sex), baseline migraine frequency, and relevant outcomes reported are presented.
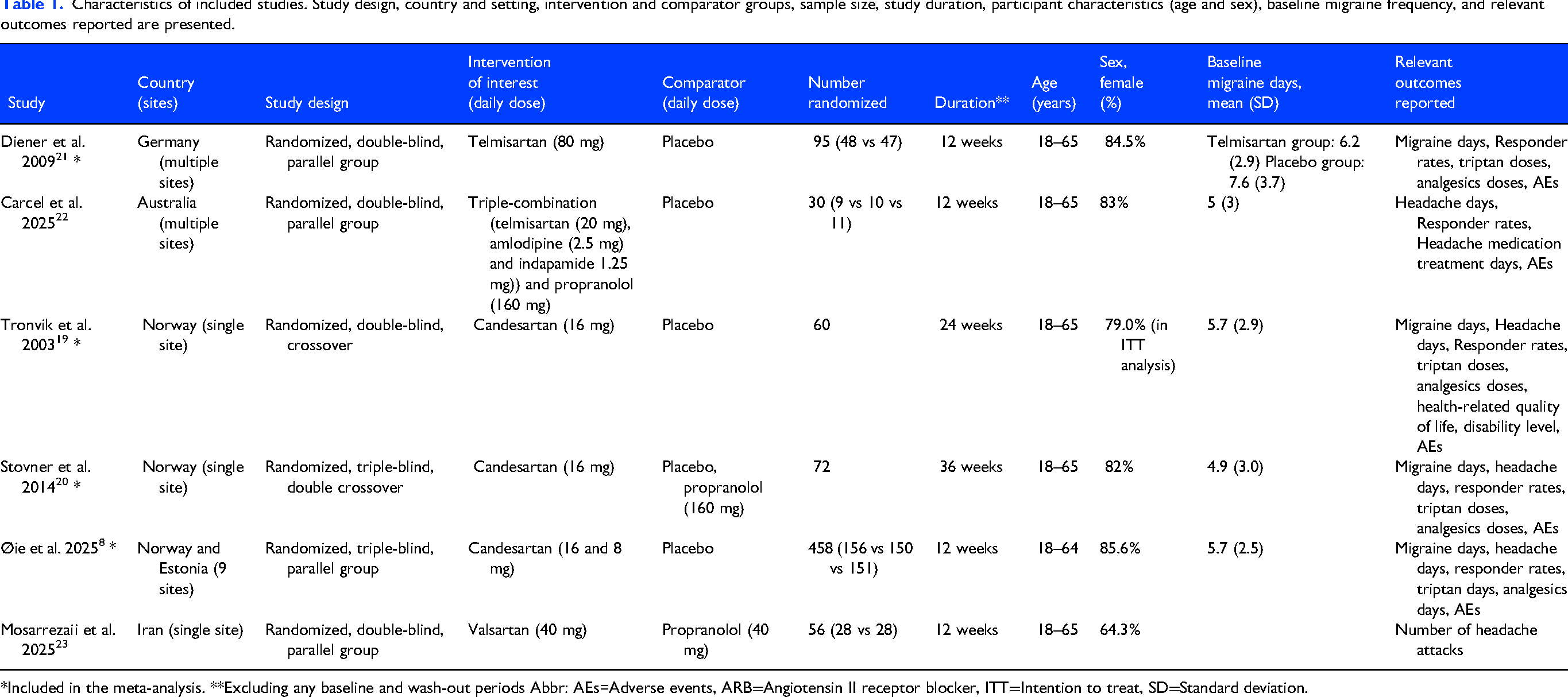
*Included in the meta-analysis. **Excluding any baseline and wash-out periods Abbr: AEs=Adverse events, ARB=Angiotensin II receptor blocker, ITT=Intention to treat, SD=Standard deviation.
Characteristics of studies included in the meta-analysis
The telmisartan study included in the meta-analysis was a multi-center, parallel-group trial conducted in Germany comparing telmisartan 80 mg with placebo, conducted by Diener et al. (2009). 21 The studies by Tronvik et al. (2003) 19 and Stovner et al. (2014) 20 both used a crossover design, comparing 16 mg candesartan with placebo. Stovner et al. (2014) 20 included a third treatment arm with propranolol. The third candesartan study by Øie et al. (2025) 8 was a three-arm parallel-group RCT in which participants received placebo, 8 mg, or 16 mg candesartan, with the comparison of 16 mg versus placebo defined as their primary endpoint. All candesartan studies originated from the same site in Norway, with the most recent being a binational, multi-center study including participants from Norway and Estonia. 8 A summary of the characteristics of included studies is found in Table 1.
A total of 659 participants were included in the meta-analysis, 575 from the candesartan studies,8,19,20 and 84 from the telmisartan study. 21 The studies included participants aged 18 to 64 or 65 years, with a large proportion of female participants (79.0% to 85.6%). They included participants with episodic migraine; however, Stovner et al. (2014) included one participant with chronic migraine. 20 All studies included in the meta-analysis reported migraine days and responder rates. In all studies, responder rates were defined as the proportion of participants with a ≥50% reduction in migraine days from baseline. Despite allowing multiple thresholds (e.g., 30% or 50%), all included studies reported ≥50% responder rates based on reduction in migraine days. Tronvik et. al (2003) 19 also reported ≥50% responder rates for other outcomes; headache days, headache hours, migraine hours and headache severity index. The three candesartan studies also reported the number of headache days.8,19,20 None of the studies reported the number of headache or migraine attacks per month. All studies reported the secondary outcomes triptan doses or days, analgesics doses or days, and AEs, but there were some differences in definitions and reporting. Tronvik et al. (2003) reported quality of life and level of disability. 19 The four studies also reported other secondary outcomes that were not within the scope of this paper and that will not be further mentioned. The treatment duration was 12 weeks in all studies. In the studies by Tronvik et al. (2003) 19 and Stovner et al. (2014), 20 data from the entire treatment period were analyzed. In the studies by Diener et al. (2009) 21 and Øie et al. (2025), 8 analyses were limited to data from the final 4 weeks of treatment.
Primary outcomes
Migraine days
A total of 459 participants receiving an ARB and 313 receiving placebo were included in the meta-analysis on change in monthly migraine days. All four studies showed a reduction in migraine days from baseline in the intervention group compared with placebo (Figure 2). The pooled effect size showed a mean reduction of −1.00 migraine days per month (95% CI: −1.51 to −0.49) compared to placebo (p-value(p)<0.001, Figure 2). The meta-analysis of migraine days restricted to candesartan is presented in Supplementary figure 1, revealing similar results.

Forest plot of comparison of change in monthly migraine days from baseline between angiotensin II-receptor blockers versus placebo. Abbr: SD=Standard deviation, CI=Confidence interval.
The definition of a migraine day varied across the studies. Stovner et al. (2014) 20 and Øie et al. (2025) 8 defined a migraine day as a day with moderate or severe headache lasting ≥4 h or that is treated with acute medication. Øie et al. (2025) 8 further required the presence of nausea and/or phonophobia/photophobia accompanying the headache. 8 Diener et al. (2009) 21 defined a migraine day as a day with migraine symptoms lasting ≥1 h, not following the recommendation for this outcome in the applicable guidelines at the time the study was conducted. 24 The study by Tronvik et al. (2003) 19 did not provide any definition for this outcome in the published paper or study protocol, but stated that the study was conducted in accordance with the prevailing guidelines for controlled clinical trials at the time. 24
Headache days
Three studies evaluating the effect of candesartan reported data on headache days, whereas Diener et al. (2009) 21 did not, despite listing it as a secondary outcome. The meta-analysis of headache days included 419 participants on candesartan, and 269 participants on placebo. All three studies showed a reduction in headache days, and the combined effect size was −1.21 days (95% CI: −1.62 to −0.81; p<0.001) (Figure 3).
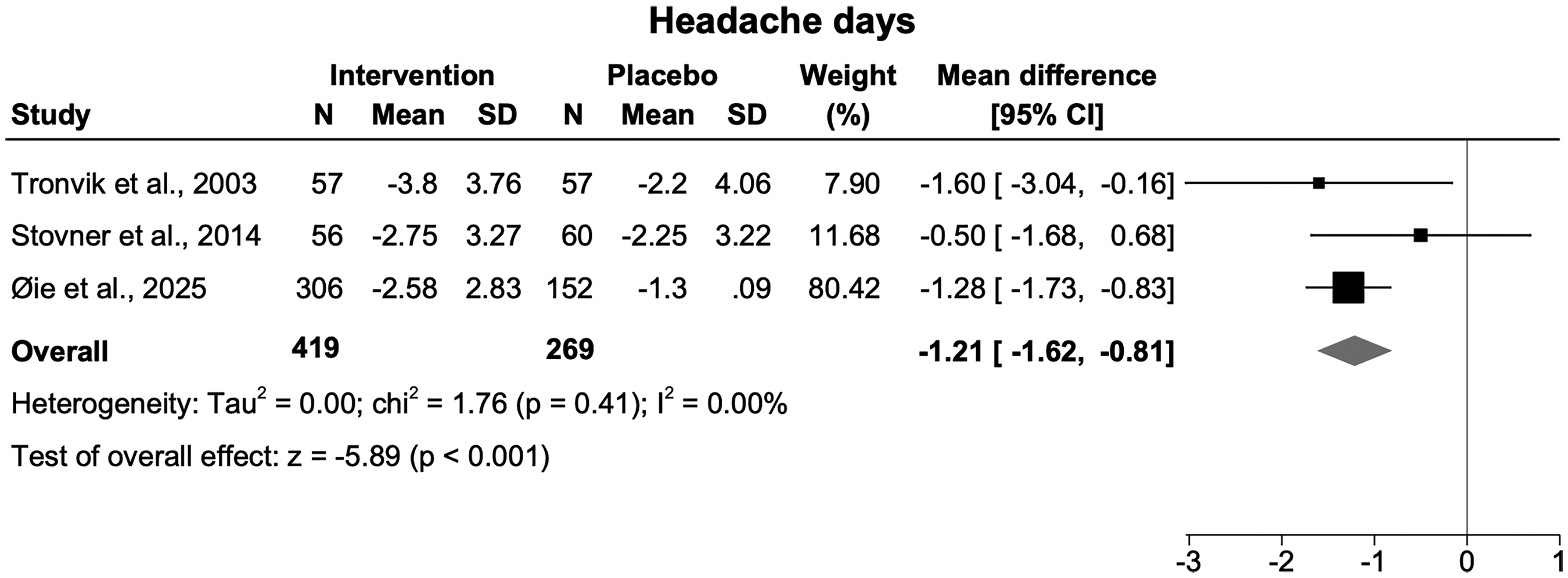
Forest plot of comparison of change in monthly headache days from baseline between angiotensin II-receptor blockers versus placebo. Abbr: SD=Standard deviation, CI=Confidence interval.
Responder rates
All four studies contributed to the meta-analysis of responder rates. A total of 303 participants receiving placebo and 450 participants receiving either candesartan or telmisartan were included. All studies observed a higher responder rate on candesartan or telmisartan than on placebo (Figure 4). The combined effect size showed an odds ratio of 2.68 (95% CI: 1.91 to 3.78, p<0.001). Results of the responder rate analysis restricted to candesartan are presented in Supplementary figure 2, showing consistent findings.
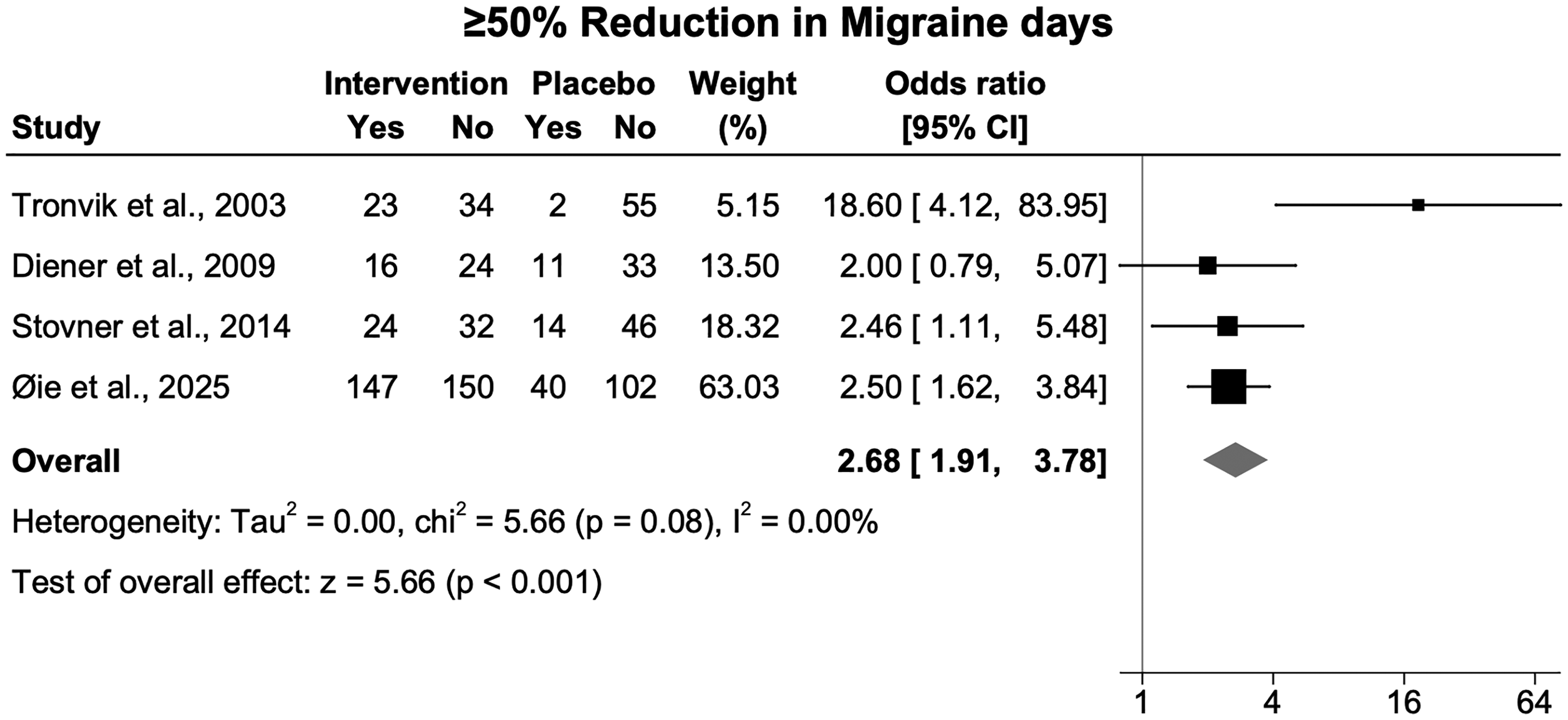
Forest plot of comparison of angiotensin II-receptor blockers and placebo regarding the proportion of participants with ≥50% reduction in migraine days from baseline. The total number of participants in the study by Øie et al. was lower for this primary outcome, likely due to missing data. Abbr: SD=Standard deviation, CI=Confidence interval.
Secondary outcomes
All four studies reported AE occurrences, comprising a total of 315 participants receiving placebo and 467 receiving candesartan/telmisartan, which were included in the meta-analysis of AEs. The definition of an AE was assumed to follow applicable guidelines and included all treatment-emergent events. 25 Three studies reported the number or proportion of participants experiencing at least one AE or symptom during the treatment periods,8,19,21 while Stovner et al. (2014) 20 reported the number of participants who had experienced an AE since the last visit. These measures were considered comparable and used in the meta-analysis. The pooled analysis demonstrated a difference of 0.10 (95% CI: 0.00 to 0.20; p=0.04), indicating a 10% higher risk of AEs with candesartan and telmisartan compared to placebo (Figure 5). Meta-analysis of AEs restricted to candesartan can be found as Supplementary figure 3, showing similar results.

Forest plot of comparison of adverse event occurrence between angiotensin II-receptor blockers versus placebo. Abbr: SD=Standard deviation, CI=Confidence interval.
The three candesartan studies8,19,20 differentiated between types of AEs and reported the number of participants experiencing each AE at least once during the treatment period. Diener et al. (2009) 21 did not provide details on the specific types of AEs. Tronvik et al. (2003) 19 found only a slight increase in dizziness and fatigue with candesartan compared to placebo. Dizziness, tiredness, and paresthesia were more frequently reported with candesartan than placebo in the study by Stovner et al. (2014). 20 The same study also reported two serious AEs related to pregnancies during the candesartan treatment period. 20 Øie et al. (2025) 8 observed more dizziness with candesartan, but similar rates of tiredness between treatment arms. This study also reported one pregnancy, but it was not defined as a serious AE. 8 In total, six serious AEs among the participants using candesartan were reported in this study, with one assessed to be related to the drug. 8 This was a syncope leading to concussion and hospitalization.
Three studies19–21 reported either the number or the change of analgesics and triptan doses, while Øie et al. (2025) 8 reported the change in number of triptan days. Tronvik et al. (2003) 19 found significantly lower number of both triptan and analgesics doses on candesartan compared to placebo. Similarly, Stovner et al. (2014) 20 observed a reduction in both outcomes, however, only the decrease in triptan doses reached statistical significance. Øie et al. (2025) 8 reported a significantly greater reduction in triptan days with both 8 mg and 16 mg candesartan compared to placebo. Diener et al. (2009) 21 reported greater reductions in analgesics and triptan doses with telmisartan compared to placebo, but these differences were not statistically significant. Additionally, Tronvik et al. (2003) 19 found significantly lower levels of disability scores with candesartan compared to placebo, whereas health-related quality of life did not differ between treatment periods.
Other comparisons
The study by Øie et al. (2025) 8 also presented analysis of secondary endpoints, comparing 8 mg and 16 mg candesartan. No statistically significant differences were observed between the two doses for any efficacy endpoint, and the proportion of participants experiencing at least one AE was similar.
Stovner et al. (2014) 20 observed no significant differences between candesartan and propranolol for any of the primary outcomes. The proportion of participants reporting AEs was not significantly different between the two treatment periods, however, dizziness was reported more frequently with candesartan. A greater reduction in analgesics doses was observed for propranolol compared to candesartan.
Risk of bias
The risk of bias assessment for each domain for each of the primary outcomes (migraine days, headache days, and responder rates) is presented in Supplementary Table 2 (Additional file 2). The assessments were consistent across outcomes within the four studies. We found a high risk of bias across outcomes in the study by Diener et al. (2009) 21 primarily due to missing outcome data (12% of the randomized participants) and possible selective reporting (only last 4 weeks of the treatment period were analyzed). The study by Tronvik et al. (2003) 19 raised some concerns for risk of bias across outcomes due to insufficient information on allocation concealment. The risk of bias was assessed as low for the studies by Stovner et al. (2009) 20 and Øie et al. (2025) 8 for all primary outcomes.
Certainty of evidence (GRADE)
The GRADE assessment for each primary outcome is presented in Table 2. For migraine days and responder rate, some concerns were identified regarding indirectness and risk of bias. The certainty of evidence for responder rate was upgraded to moderate due to a large effect size, whereas the certainty for migraine days was assessed as low. The certainty of evidence for headache days was assessed as high. Although headache day was not reported in the study by Diener et al. (2003), 21 raising concern for selective reporting, the candesartan trials demonstrated low risk of bias and precise estimates; therefore, the certainty of evidence was not downgraded. Heterogeneity was categorized as ‘might not be important’ for all primary outcomes (I2=0.00% for headache days and responder rates and I2=26.70% for migraine days), and moderate (I2=41.45%) for AEs.
Summary of findings table with certainty of evidence (GRADE).

Two studies had low risk of bias, one study had some concerns of risk of bias, and one study had high risk of bias.
Indirectness due to differences in the definitions of a migraine day.
Abbr: CI: confidence interval, OR: Odds ratio, RCT: Randomized controlled trial.
Discussion
The results from the meta-analysis suggest that ARBs, particularly candesartan, are effective in the prevention of episodic migraine. The analysis included three studies investigating candesartan, and one study investigating telmisartan in migraine prophylaxis. The pooled effect sizes demonstrated significant efficacy in reducing migraine days, headache days, as well as improving responder rates.
The reductions in migraine days and headache days observed in our analysis are consistent with a previous meta-analysis evaluating all types of blood pressure-lowering medication. 6 The meta-analysis was conducted in 2023 and included three of the same studies (two on candesartan, and one on telmisartan). 7 They found a significant reduction of −0.9 migraine days, and −0.7 headache days. However, it was conducted before the publication of the most recent RCT on candesartan. 8 Other previous meta-analyses have not included all relevant studies 26 or/and have focused on several medication groups simultaneously. 6 Our meta-analysis focused exclusively on ARBs and included the multi-center RCT from 2025 with a larger study population than any previous RCT, 8 contributing to a larger pooled effect size for these outcomes than seen in previous meta-analyses. Additionally, our meta-analysis found higher responder rates with ARBs compared to placebo, an outcome that was not assessed in the previous meta-analysis. 7 The present meta-analysis highlights the evidence for the use of ARBs, particularly candesartan, for preventive migraine treatment in episodic migraine. This supports the rationale for reconsidering their position as a cost-effective alternative in international guidelines. The efficacy of other ARBs (e.g., valsartan, telmisartan) remains unclear, owing to the paucity and low quality of available data.
The certainty of evidence was assessed as low for migraine days, moderate for responder rates, and high for headache days, providing strong and reliable evidence for the efficacy of ARBs in preventive treatment of episodic migraine. We identified high risk of bias in the study on telmisartan by Diener et al. (2009), 21 but the contribution of these data to the pooled estimates were generally low. The certainty of evidence was downgraded to low for migraine days due to risk of bias and the indirectness caused by differences in definitions of a migraine day. Headache days were reported only in the candesartan studies and had a high certainty of evidence. We assessed that the lack of reporting of this outcome in the study by Diener et al. (2009) 21 could contribute to a publication bias. However, a downgrade in certainty of evidence was not justified, as there was no consistent pattern of such omissions across studies, and as the study had minimal effect on the pooled estimates due to small sample size and low weighting in the meta-analysis of other outcomes. There were also differences regarding the time period during which the efficacy outcomes were measured, with two of the studies only using data from the last 4 weeks of the treatment period in the analysis. These differences did not lead to a further downgrade in the certainty of evidence for any outcome as both timeframes were judged to provide equally appropriate measures of the intervention's effect.
Although ARBs are generally considered well tolerated,8,27 dizziness, fatigue, and paresthesia were consistently reported across the candesartan trials and may be particularly relevant in a migraine population already vulnerable to central nervous system symptoms. Serious AEs were rare but included syncope with secondary injury and pregnancy-related concerns, underscoring the importance of individualized preventive treatment and appropriate follow-up and patient counseling.
Several limitations of this review should be acknowledged. Only one participant with chronic migraine was included, and the evidence of ARBs as preventive treatment in this patient group is currently limited to observational studies.27–29 A RCT in patients with chronic migraine is warranted to clarify the efficacy of candesartan in this population. This is particularly relevant in the current therapeutic landscape, where treatments targeting the calcitonin gene-related peptide system have been evaluated separately in chronic migraine, underscoring the need to establish similarly robust evidence for candesartan as a cost-effective alternative in this population. Furthermore, there was a large predominance of female participants across the studies, limiting the generalizability of the findings. The studies did not provide definitions for reporting sex and gender, nor did they collect data on gender identity. None of the studies reported participants’ race, or ethnicity, further restricting the ability to assess the generalizability across different demographic groups. There was heterogeneity in outcome definitions across studies, justifying a downgrade in certainty of evidence for two outcomes. A relatively small number of studies were included, the majority of which were conducted at single centers. The studies provided data from different countries; however, all three studies on candesartan were conducted at the same site in Norway, except for the recent study which also included participants from Estonia. 8 This may affect external validity. The meta-analysis combined different ARBs (telmisartan and candesartan) in analysis, limiting interpretability. However, additional analyses restricted to candesartan only revealed consistent results.
Conclusion
This systematic review and meta-analysis found ARBs, particularly candesartan, to be effective in preventing episodic migraine. The pooled results showed significant reductions in migraine days, headache days, and a strong association with responder rates. The evidence had low, high, and moderate certainty respectively, highlighting candesartan as an effective treatment option in prevention of episodic migraine and supporting the rationale for reconsidering its position in international guidelines. The effectiveness of other ARBs remains unclear.
Key Findings
ARBs, particularly candesartan, are effective in preventing episodic migraine The certainty of evidence was rated as low, moderate and high for migraine days, responder rates and headache days respectively, with no serious risk of bias. These findings support reconsideration of candesartan in international migraine prevention guidelines.
Supplemental Material
sj-docx-1-cep-10.1177_03331024261451481 - Supplemental material for The effects of angiotensin receptor blockers as prophylactic migraine treatment: A systematic review and meta-analysis
Supplemental material, sj-docx-1-cep-10.1177_03331024261451481 for The effects of angiotensin receptor blockers as prophylactic migraine treatment: A systematic review and meta-analysis by Hedda Skogum Riise, Helene Thorvik, Lise Rystad Øie, Lars Jacob Stovner, Erling Andreas Tronvik, Mattias Linde, Knut Hagen, Samita Giri and Tore Wergeland in Cephalalgia
Supplemental Material
sj-docx-2-cep-10.1177_03331024261451481 - Supplemental material for The effects of angiotensin receptor blockers as prophylactic migraine treatment: A systematic review and meta-analysis
Supplemental material, sj-docx-2-cep-10.1177_03331024261451481 for The effects of angiotensin receptor blockers as prophylactic migraine treatment: A systematic review and meta-analysis by Hedda Skogum Riise, Helene Thorvik, Lise Rystad Øie, Lars Jacob Stovner, Erling Andreas Tronvik, Mattias Linde, Knut Hagen, Samita Giri and Tore Wergeland in Cephalalgia
Supplemental Material
sj-png-3-cep-10.1177_03331024261451481 - Supplemental material for The effects of angiotensin receptor blockers as prophylactic migraine treatment: A systematic review and meta-analysis
Supplemental material, sj-png-3-cep-10.1177_03331024261451481 for The effects of angiotensin receptor blockers as prophylactic migraine treatment: A systematic review and meta-analysis by Hedda Skogum Riise, Helene Thorvik, Lise Rystad Øie, Lars Jacob Stovner, Erling Andreas Tronvik, Mattias Linde, Knut Hagen, Samita Giri and Tore Wergeland in Cephalalgia
Supplemental Material
sj-png-4-cep-10.1177_03331024261451481 - Supplemental material for The effects of angiotensin receptor blockers as prophylactic migraine treatment: A systematic review and meta-analysis
Supplemental material, sj-png-4-cep-10.1177_03331024261451481 for The effects of angiotensin receptor blockers as prophylactic migraine treatment: A systematic review and meta-analysis by Hedda Skogum Riise, Helene Thorvik, Lise Rystad Øie, Lars Jacob Stovner, Erling Andreas Tronvik, Mattias Linde, Knut Hagen, Samita Giri and Tore Wergeland in Cephalalgia
Supplemental Material
sj-png-5-cep-10.1177_03331024261451481 - Supplemental material for The effects of angiotensin receptor blockers as prophylactic migraine treatment: A systematic review and meta-analysis
Supplemental material, sj-png-5-cep-10.1177_03331024261451481 for The effects of angiotensin receptor blockers as prophylactic migraine treatment: A systematic review and meta-analysis by Hedda Skogum Riise, Helene Thorvik, Lise Rystad Øie, Lars Jacob Stovner, Erling Andreas Tronvik, Mattias Linde, Knut Hagen, Samita Giri and Tore Wergeland in Cephalalgia
Footnotes
Acknowledgements
The authors gratefully acknowledge Research Librarian Sindre Andre Pedersen for expert guidance in the literature search process, and NTNU University Library for assistance in the retrieval of full-text articles.
ORCID iDs
Ethical considerations
Because the study involved analysis of published literature without access to individual-level patient data, ethics’committee approval and patient consent were not applicable.
Consent to participate
Not applicable.
Consent for publication
All authors confirm that they had access to all data in the study and accept publication of their work in Cephalalgia.
Author contributions
The conceptualization of the systematic review and development of the protocol was carried out by HSR, HT, SG, and TW. The literature search was performed by HSR, and the study selection process was conducted by HSR and HT. Risk of bias assessment was completed by HSR, HT, and SG, while GRADE assessment was performed by HSR, HT, ML, and SG. Data analysis was conducted by HSR, SG, and HT, with interpretation of the results performed by HSR, HT, SG, TW, LRØ, LSJ, KH, ML. and KH. The manuscript was drafted by HSR, HT, SG, and TW. HSR, HT, LRØ, LJS, EAT, ML, KH, SG, and TW provided critical revision of the manuscript. HSR, HT and SG had full access to the underlying data for the meta-analysis and take full responsibility for the accuracy of data analysis.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
ML and EAT are coinventors and hold a patent related to a biofeedback intervention (Cerebri) for migraine prophylaxis. EAT is cofounder and shareholder of Nordic Brain Tech AS. EAT has received honoraria for lectures/advisory boards from Amgen, Novartis, Eli Lilly, AbbVie, TEVA, Roche, Lundbeck, Pfizer, Biogen, Organon and has stocks and IP in Man & Science and Keimon Medical AS and is consultant for Man & Science. ML has received honoraria for lectures / advisory boards from AbbVie, Lundbeck, Novartis, Pfizer, and TEVA. TW has received honoraria from TEVA, Roche, Lilly, Lundbeck and has stocks in two MedTech companies (Vilje Bionics AS and Keimon medical AS). LRØ, LJS, EAT, ML, KH and TW have authored or co-authored one or more of the studies included in this systematic review and meta-analysis. HSR, HT, and SG have no competing interests.
Data availability statement
Open practices
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.