
Abstract
Background
Anxiety is commonly reported among patients with migraine, and anxiety questionnaires are frequently used to assess anxiety symptoms. This narrative review examines how common anxiety screening tools are applied in migraine studies and whether they are applied and interpreted appropriately.
Method
A PubMed search included studies using the Hospital Anxiety Depression Scale (HADS), Generalized Anxiety Disorder 7-Items (GAD-7) or Beck Anxiety Inventory (BAI). The search also included studies using the Hamilton Anxiety Rating Scale (HAM-A) or State Anxiety Inventory (STAI). Eligible patients were diagnosed with migraine according to the International Classification of Headache Disorders (ICHD-2 or ICHD-3).
Results
Ninety-eight studies met the inclusion criteria. In 42 studies (41%), an anxiety score above the cut-off was interpreted as an anxiety diagnosis. This approach was used in 52%, 44%, 41%, 29% and 38% of studies using HADS-A, GAD-7, BAI, HAM-A and STAI. Only three studies confirmed the diagnosis through a structured clinical interview. Data presentation and interpretation across the studies were heterogeneous. Only a few of the scales are validated in a population of migraine patients.
Conclusion
This study shows that anxiety screening tools are commonly used in migraine studies but with considerable variation in cut-off scores and interpretation. Such methodological differences and limited validation of these tools may make it difficult to determine the true prevalence of anxiety in migraine studies. Further studies are needed to validate these instruments and to establish clear guidelines for their use in migraine research.
Keywords
Introduction
Migraine is a prevalent headache disorder affecting more than one billion people worldwide. 1 The one-year prevalence rate is approximately 10%, ranging from 4.5–6.0% in men and 14.5–18.0% in women. 2
Migraine is a disorder that has been suggested to be strongly associated with a wide range of comorbidities, including psychiatric disorders such as anxiety and depression.3–5 Studies of the relationship between migraine and anxiety have shown that patients with migraine are two to five times more likely to develop anxiety disorders compared to the general population.6,7
In studies examining the comorbidity between migraine and anxiety, self-report anxiety screening forms are often used to assess the presence and severity of anxiety symptoms. However, some studies have used these tools to diagnose anxiety disorders by reporting the percentage of patients scoring above a certain cutoff point. This practice may misestimate the prevalence of anxiety, particularly when the questionnaires have not been validated for use in patients with migraine. Although such anxiety screening questionnaires can be practical tools for identifying anxiety, they are not sufficient for making a definitive diagnosis. 8 According to national and international guidelines, a formal diagnosis should be made by a psychiatrist or a general practitioner. 9 Reliance on a single questionnaire without clinical evaluation is inadequate for diagnosing anxiety disorders.10,11 Instead, a two-stage approach, combining screening questionnaires with diagnostic interviews, can optimize resource use and provide more accurate prevalence estimates in patients with migraine. 12 Although anxiety screening tools are widely used in migraine research, their methodological application and interpretation have received limited critical evaluation. To our knowledge, very few studies have evaluated how these tools are applied and interpreted across migraine studies. Screening questionnaires are often used as measures for anxiety disorders, which may lead to misclassification and overestimation of psychiatric comorbidity. Therefore, this review aims to examine how the most common anxiety screening and assessment tools have been applied in migraine studies, and to assess whether they were used and interpreted correctly. Specifically, we investigated whether the use of screening scores led to the conclusion that patients had suffered from anxiety or symptoms of anxiety. Furthermore, we reviewed studies that combined screening questionnaires with diagnostic interviews. In the present study, we reviewed the Hospital Anxiety Depression Scale (HADS), Generalized Anxiety disorder Scale (GAD-7), Beck Anxiety Inventory (BAI), Hamilton Anxiety Rating Scale (HAM-A) and State-Trait Anxiety Inventory (STAI). Moreover, we compiled the studies that validated the different screening tools in patients with migraine.
Methods
The screening tools
Hospital anxiety and depression scale (HADS)
The Hospital Anxiety and Depression Scale (HADS) is a self-assessment tool developed to screen for anxiety and depression in outpatient settings and to measure the severity of emotional distress. 13 The scale consists of 14 items, seven assessing anxiety (HADS-A) and seven assessing depression (HADS-D). The cut-off scores for the two subscales vary across studies, although a threshold of eight on each subscale is commonly used. 14 One study reported that a cut-off score of eight or greater provided the optimal balance between sensitivity and specificity for HADS as a screening instrument for depression and anxiety, with both metrics averaging 0.80. 15 One clinical-based study including 300 patients with migraine validated the HADS-D in this population. 16 At a cut-off score of eight, the HADS-D had a sensitivity of 86.5%, a specificity of 86.5%, negative predictive value (NPV) of 95.0% and positive predictive value (PPV) of 68.2%. The area under the curve (AUC) was 0.92. It was further observed that higher cut-off scores were associated with decreased sensitivity but increased specificity. In contrast, a clinical study of 62 headache patients found that a cut-off score ≥13 was the most effective cut-off value for anxiety disorders, with a sensitivity of 84% and a specificity of 42%. 17
Beck anxiety inventory (BAI)
The Beck Anxiety Inventory (BAI) is a self-report instrument developed to distinguish anxiety from depression. 18 The BAI consists of 21 items, each rated by patients on a 0–4 scale, yielding a total score between 0 and 63. Both the original BAI and the revised BAI-II use this 21-item format, although cut-off scores for anxiety severity differ. For the BAI-I, scores of 0–9 indicate minimal anxiety, 10–18 mild anxiety, 19–29 moderate anxiety and 30–63 severe anxiety. 19 For the BAI-II scores of 0–7 indicate minimal anxiety, 8–15 mild anxiety, 16–25 moderate anxiety and severe anxiety 26–63. 20 One study reported that the BAI demonstrated stronger convergent and discriminant validity than the State-Trait Anxiety Inventory. 20 While the BAI is not intended to establish a formal diagnosis of an anxiety disorder, it has been validated for assessing the presence and severity of anxiety symptoms and for screening probable cases of major anxiety disorders. 19 To date, no studies have validated the BAI in patients with migraine.
Hamilton anxiety rating scale (HAM-A)
The HAM-A is used to assess the severity of anxiety symptoms in patients already diagnosed with an anxiety disorder according to DSM-5 or ICD-10. The HAM-A is administered by a trained clinician and consists of 14 items, each rated on a 5-point scale from 0 to 4. The total score is obtained by summing the individual item scores and ranges from 0 to 56. A score of <17 indicates mild anxiety, 18–24 indicates moderate anxiety and ≥25 indicates severe anxiety. 21 To date, no studies have validated the use of the HAM-A in patients with migraine.
The generalized anxiety disorder 7 items (GAD-7)
The GAD-7 is a self-report questionnaire used to identify, and measure generalized anxiety disorder. The scale consists of seven items derived from the DSM-5. Each item is rated on a 4-point scale from 0 to 3, based on a symptom frequency over the previous two weeks. 22 The total score ranges from 0 to 21. GAD-7 scores of 5, 10 and 15 indicate mild, moderate and severe levels of anxiety, respectively. The cut-off values vary across studies. One clinical study reported that a cut-off score ≥9 showed a sensitivity of 89% and a specificity of 82% for detecting GAD. 23 The optimal balance between sensitivity and specificity for the GAD-7 was achieved at a cut-off score ≥10. 23 Another clinical study that was conducted in health centers reported a sensitivity of 100% and a specificity of 83% at a cut-off score ≥9. 24 A separate clinical study evaluated 146 consecutive patients with migraine, assessing the performance of the GAD-7. 25 The study found that at a cut-off score of five, the GAD-7 demonstrated 78% sensitivity and a specificity of 75%, a positive predictive value (PPV) of 46.3% and a negative predictive value (NPV) of 92.4%. This study concluded that a cut-off score ≥5 provided the highest balance between sensitivity and specificity.
State-trait anxiety inventory (STAI)
The Spielberger State-Trait Anxiety Inventory (STAI) is a self-report questionnaire developed to distinguish two forms of anxiety, “state anxiety” and “trait anxiety”. 26 The scale consists of 40 items, divided into 20 separate items on each subscale. The STAI-State (STAI-S) measures state anxiety, defined as a temporary emotional response to a specific situation and characterized by tension and apprehensive thoughts. 27 In contrast, the STAI-Trait (STAI-T) reflects a more stable aspect of personality and a general tendency to experience anxiety across various situations. 28 Since migraine symptoms fluctuate over time, distinguishing between state anxiety and trait anxiety may be relevant. Each item is rated on a 4-point scale from 1–4, yielding a total score ranging from 20 to 80, with higher scores indicating greater anxiety. According to Spielberger, scores of 20–39 indicate low anxiety, 40–59 moderate anxiety and 60–80 high anxiety. 29 To date, no studies have validated the use of the STAI in patients with migraine.
Search strategy
This study was conducted as a narrative review aimed at critically examining how commonly used anxiety screening tools have been applied and interpreted in migraine. A targeted literature search was conducted in PubMed database and last updated on 27 March, 2025. Titles, abstracts, and full texts were screened by one author (M.Y.H.P.); no duplicate independent screening was performed. The purpose of the search was to identify studies that used one of the five selected anxiety screening tools for assessing the presence or severity of anxiety or anxiety symptoms in patients with migraine. The search strategy centered on key terms including: “migraine AND Generalized Anxiety Disorder (GAD-7)”, “migraine AND Beck Anxiety Inventory”, “migraine AND State-Trait Anxiety Inventory”, “migraine AND Hospital Anxiety and Depression scale (HADS)”, and “migraine AND Hamilton Anxiety Rating Scale”. Studies were grouped by screening instrument for narrative synthesis. A flow diagram illustrating the study selection process is presented in Figure 1.
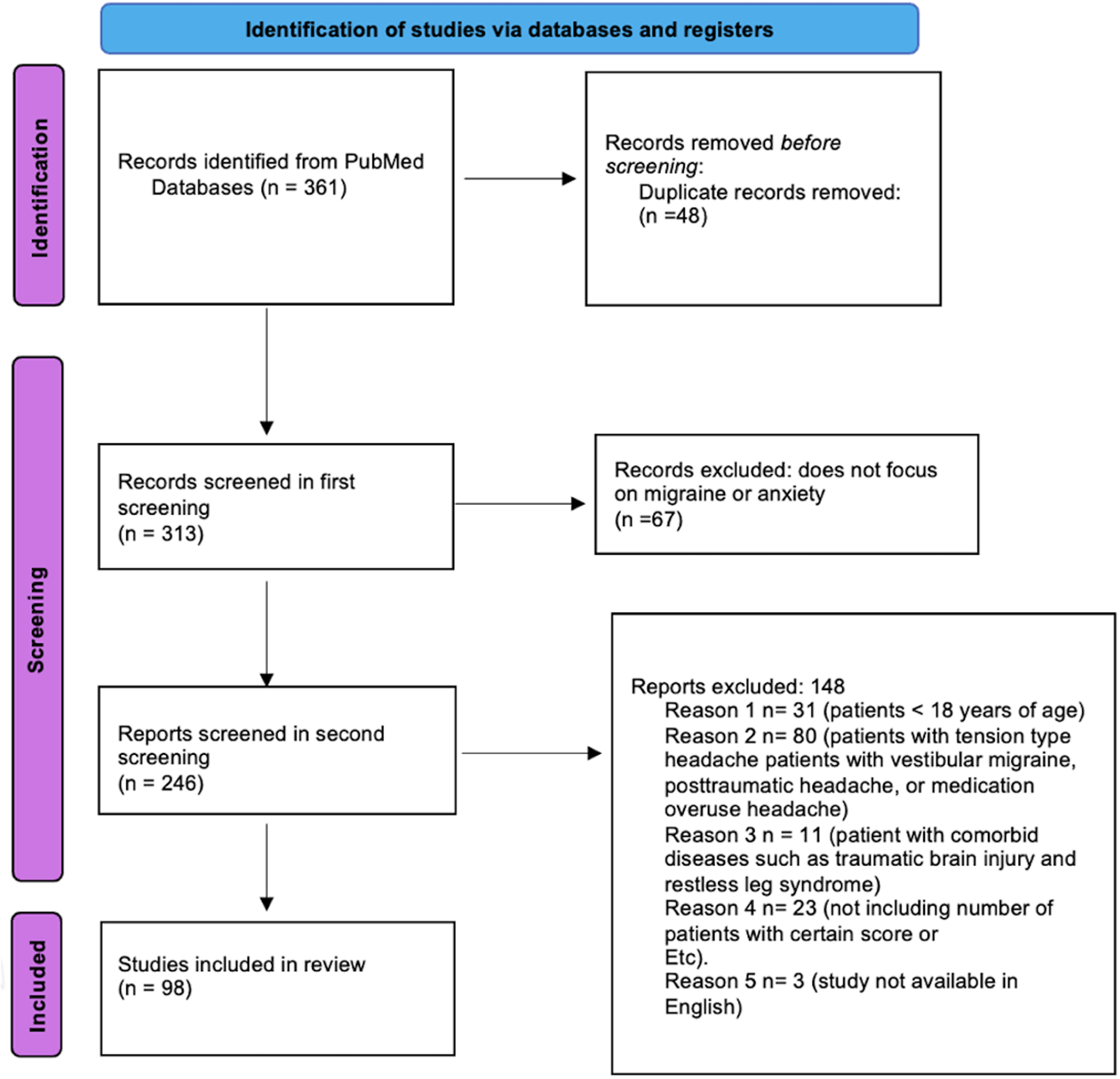
PRISMA flow chart diagram
Studies were included if they met following criteria:
Participants diagnosed with migraine according to the International Classification of Headache Disorders (ICHD-2 or ICHD-3). Use of one of the five specified tools for anxiety. Participants aged 18 years or older.
Studies were excluded if they met the following criteria:
Other headache types such as tension-type headache, vestibular migraine, post-traumatic headache or medication overuse headache. Migraine patients with comorbid conditions such as traumatic brain injury or restless legs syndrome, except for overweight or obese patients. Studies that did not include number or proportion of patients with a given cut-off score or the mean score from a screening tool. Articles not available in English.
Data extraction
The initial search identified a total of 361 studies. After the removal of 48 duplicate records, 313 articles were screened by title and abstract. Sixty-seven (n = 67) articles were excluded due to a lack of focus on migraine and anxiety. A secondary full-text screening of 246 articles was conducted to determine eligibility. A total of 148 articles (n = 148) were then excluded according to the exclusion criteria. As a result, 98 studies were included (see figure 1). From the included studies, information was collected on the method of data collection, type of migraine diagnosis (episodic or chronic), the proportion of patients scoring above or below specific cut-off points, mean scores (if available) and the authors’ conclusions (i.e., whether anxiety or symptoms of anxiety were identified). In studies where the scores were presented but not interpreted by the authors, these were classed as “not discussed”. The following terms were considered inaccurate conclusions, if the authors did not specify that a diagnosis was made according to DSM or ICD-10 criteria: “anxiety”, “level of anxiety,” and “anxiety disorders”. Studies that compared the scores from the anxiety screening questionnaires with results from a diagnostic interview were not included in the tables. However, these data were discussed in the Discussion section. The majority of the studies did not report screening or prevalence scores for patients with and without aura. For this reason, these data were not extracted. The extracted data were organized into five separate tables, one for each screening instrument. In studies comparing multiple patient groups, only data from patients with migraine were included. In studies that reported pre-and post-treatment scores, only baseline values were considered. For studies that divided patients with migraine into subgroups, the overall mean score was calculated as the mean of subgroup means.
Results
The literature search yielded 361 articles, of which 98 were included. All articles before 2017 used the ICHD-2 to classify migraine. Fifty-eight articles published after 2018 used ICHD-3 to classify migraine. Nineteen articles used the International Headache Society (IHS) guidelines to classify migraine. The number of eligible studies applying HADS-A, BAI, HAM-A, GAD-7, and STAI to measure anxiety was 14–16, respectively. The overall number of participants was 37,870, of whom 79% were women. Among them, 34% and 29% classified as chronic migraine and episodic migraine, respectively. The remainder (37%) had unknown migraine type or probable migraine. When interpreting the scores, the following terms were used: anxiety, level of anxiety, anxiety symptoms, anxiety scores, symptom score of anxiety, psychological distress and psychological burden. Overall, 41% of the studies concluded that participants had anxiety if they scored above a specified cut-off point (Tables 1 and 2).
Characteristics and application of anxiety screening tools in the included migraine studies.
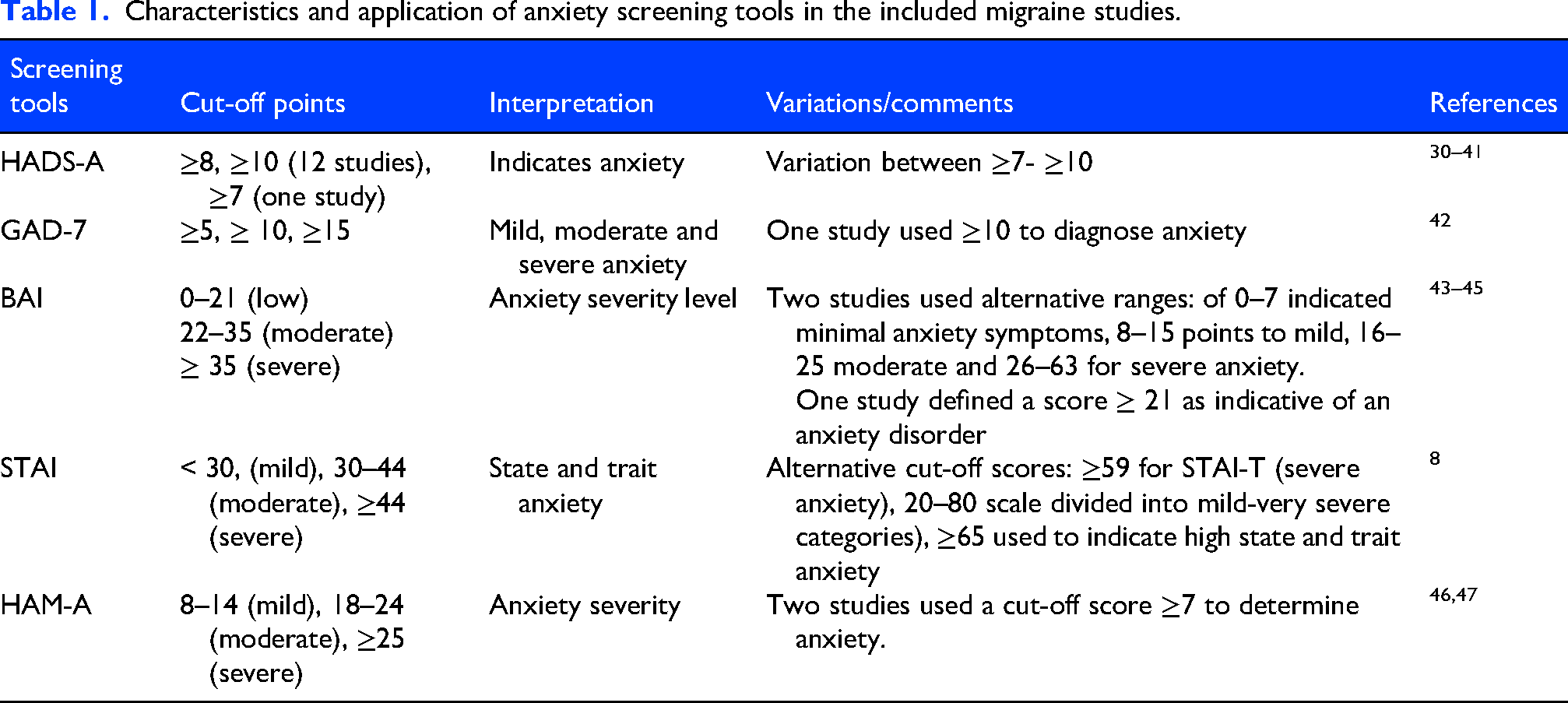
Cut-off scores for anxiety measures used by the screening tools varied across studies (Table 3). HADS-A cut-offs ranged from 7–10. The GAD-7 applied 5,10 and 15 to indicate mild, moderate and severe anxiety. BAI, STAI and HAM-A used comparable categorical ranges.
Study Characteristics for each screening tool.
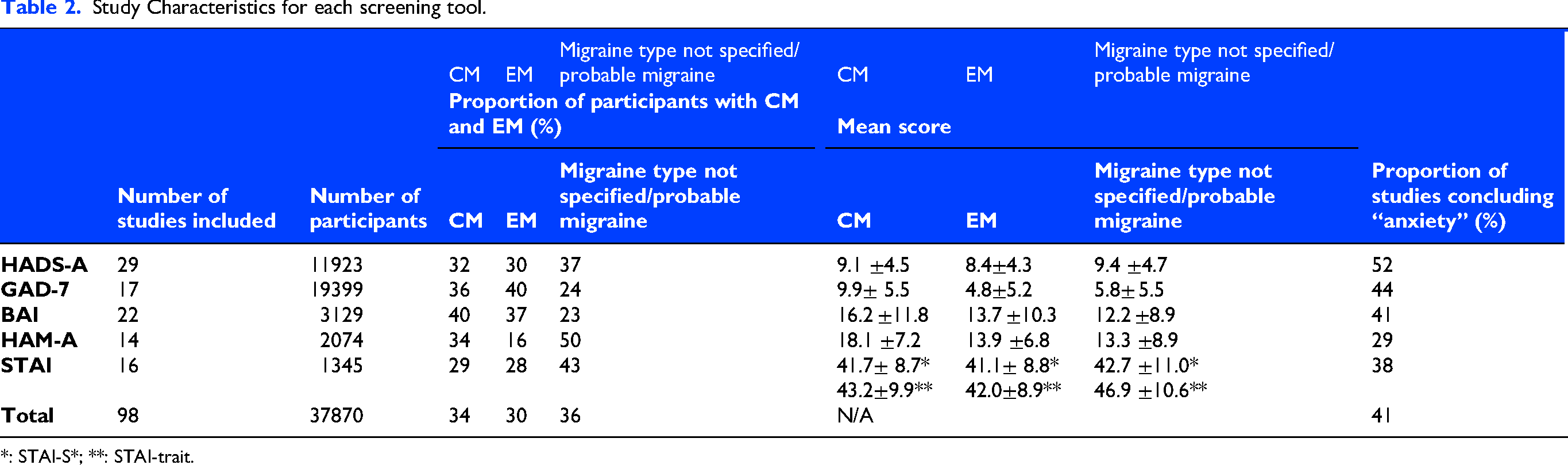
*: STAI-S*; **: STAI-trait.
Study characteristics for the included studies using HADS-A.
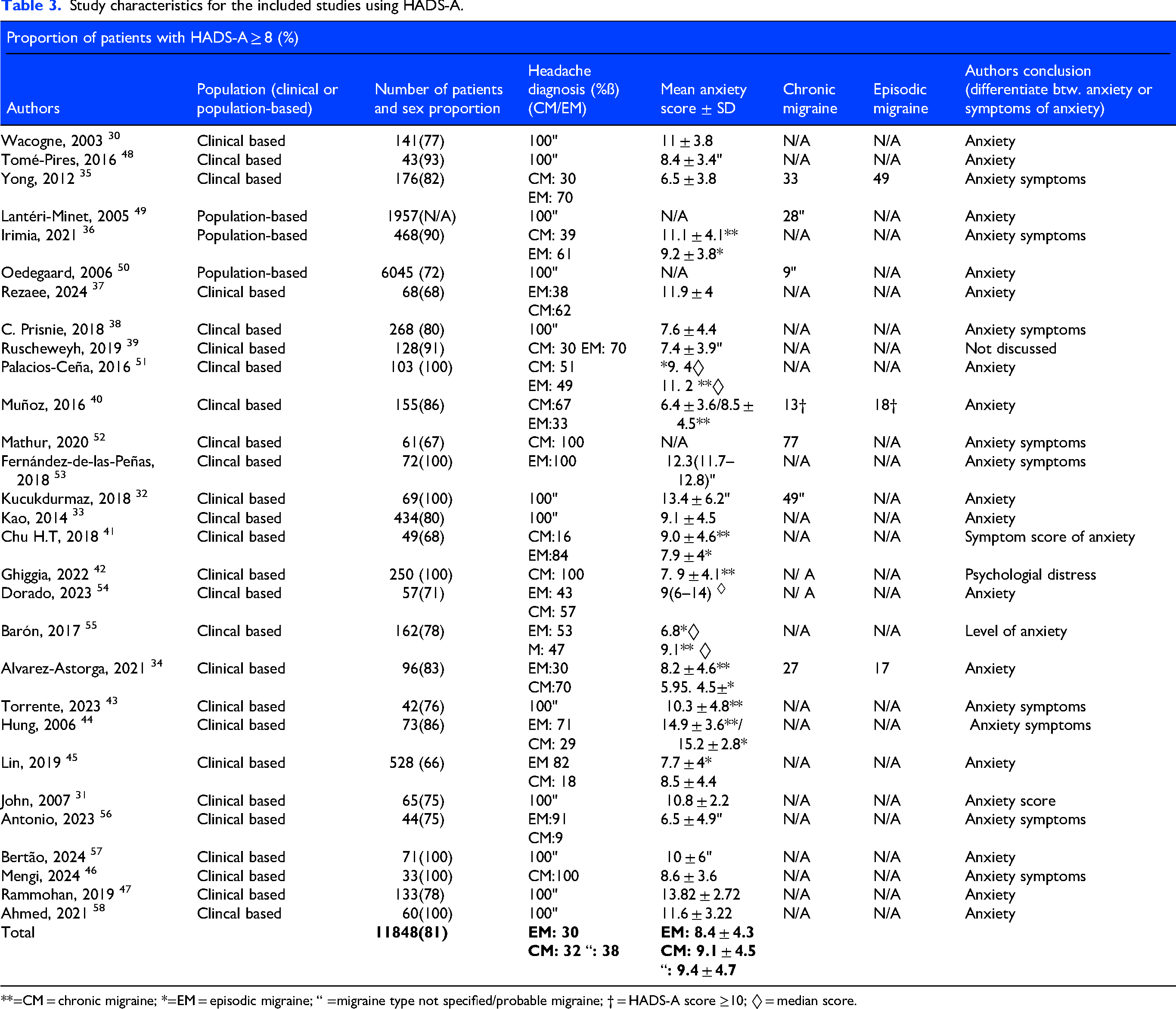
**=CM = chronic migraine; *=EM = episodic migraine; “ =migraine type not specified/probable migraine; † = HADS-A score ≥10; ◊ = median score.
Across studies using the HADS-A (Table 2), 11,848 participants were included: 27% had chronic migraine, 28% episodic migraine and 41% an unknown migraine or probable migraine type. The mean HADS-A scores were 9.1 ± 4.5, 8.4 ± 4.3 and 9.4 ± 4.7 for chronic migraine, episodic migraine and unknown/probable migraine, respectively. Twenty-two studies30–4856–58 reported a mean score and four studies51,53–55 reported a median score range. Six studies34,37,40,43,47,58 (21%) reported the proportion scoring ≥8 and 15 studies30,32–3437,40,45,47–51,54,57,58 (52%) concluded that participants scoring above the cut-off point had anxiety.
In the studies using the BAI (Table 4), 3129 participants were included: 40% chronic migraine, 37% episodic migraine and 23% unknown migraine type or probable migraine. The mean BAI scores were 16.2 ±11.8, 13.7 ±10.3 and 12.2 ±8.9, respectively. Seventeen studies4,58–73 reported mean scores and four studies74–77 reported median values. Seven studies60,63,68,72–75 (32%) provided proportion within a range and nine studies (41%) reported that scores above the cut-off reflected anxiety.
Study characteristics for the included studies using BAI.
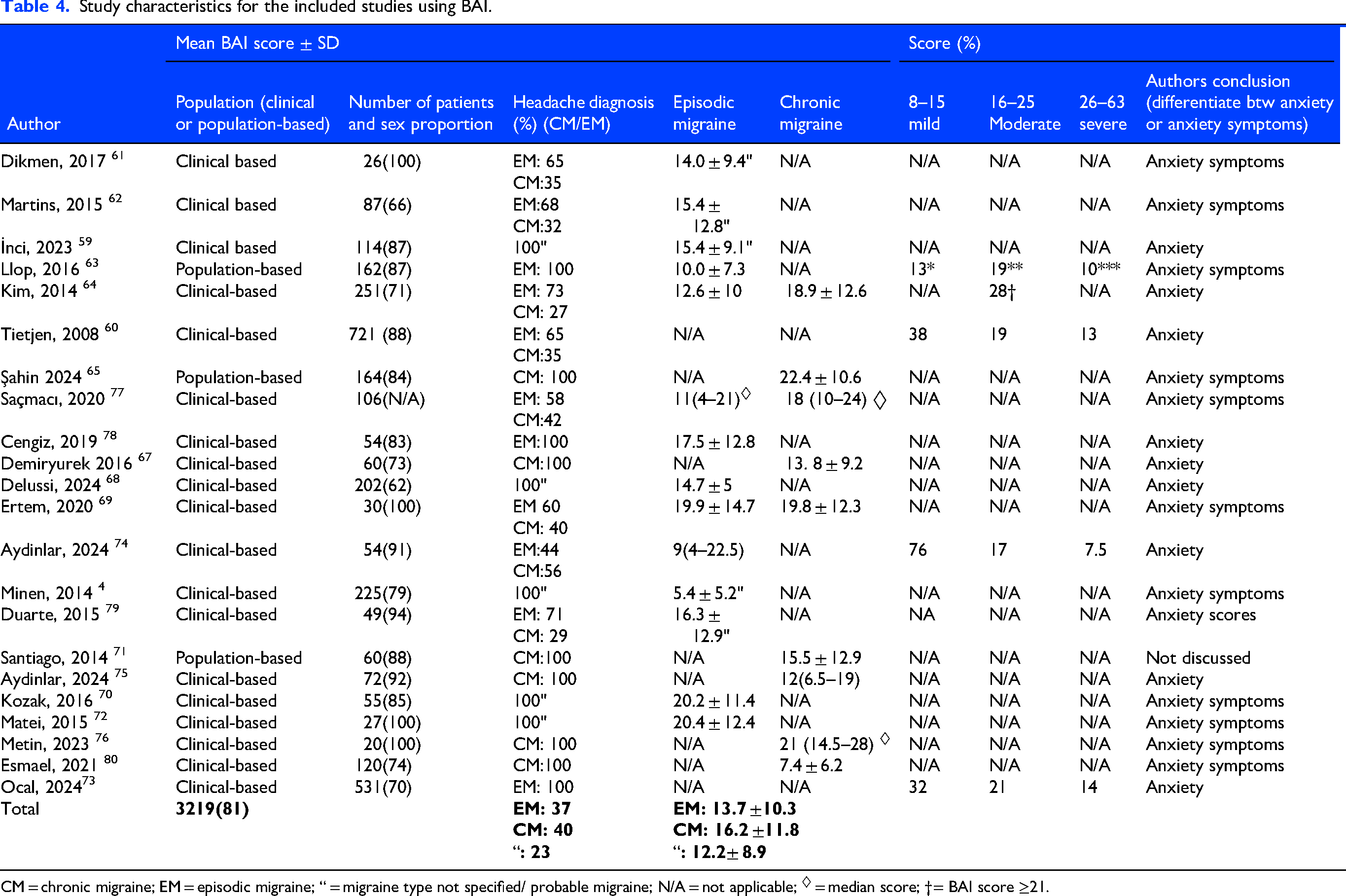
CM = chronic migraine; EM = episodic migraine; “ = migraine type not specified/ probable migraine; N/A = not applicable; ◊ = median score; †= BAI score ≥21.
Among studies using the STAI (Table 5), 1345 participants were included: 28% chronic migraine, 29% episodic migraine and 43% unknown migraine type or probable migraine. STAI-S (state anxiety) mean scores were 41.7 ± 8.7, 41.1 ± 8.8, and 42.7 ± 11.0; STAI-T(trait anxiety) mean scores of were 43.2 ± 9.9, 42.0 ± 8.9 and 46.9 ± 10.6 Fifteen studies8,81–94 reported mean scores, and one study 53 a median. Three studies88,90,92 (19%) reported proportions within a range and six studies81,82,84,86,91,93 (38%) interpreted scores above a cut-off as anxiety.
Study characteristics for the included studies using STAI.
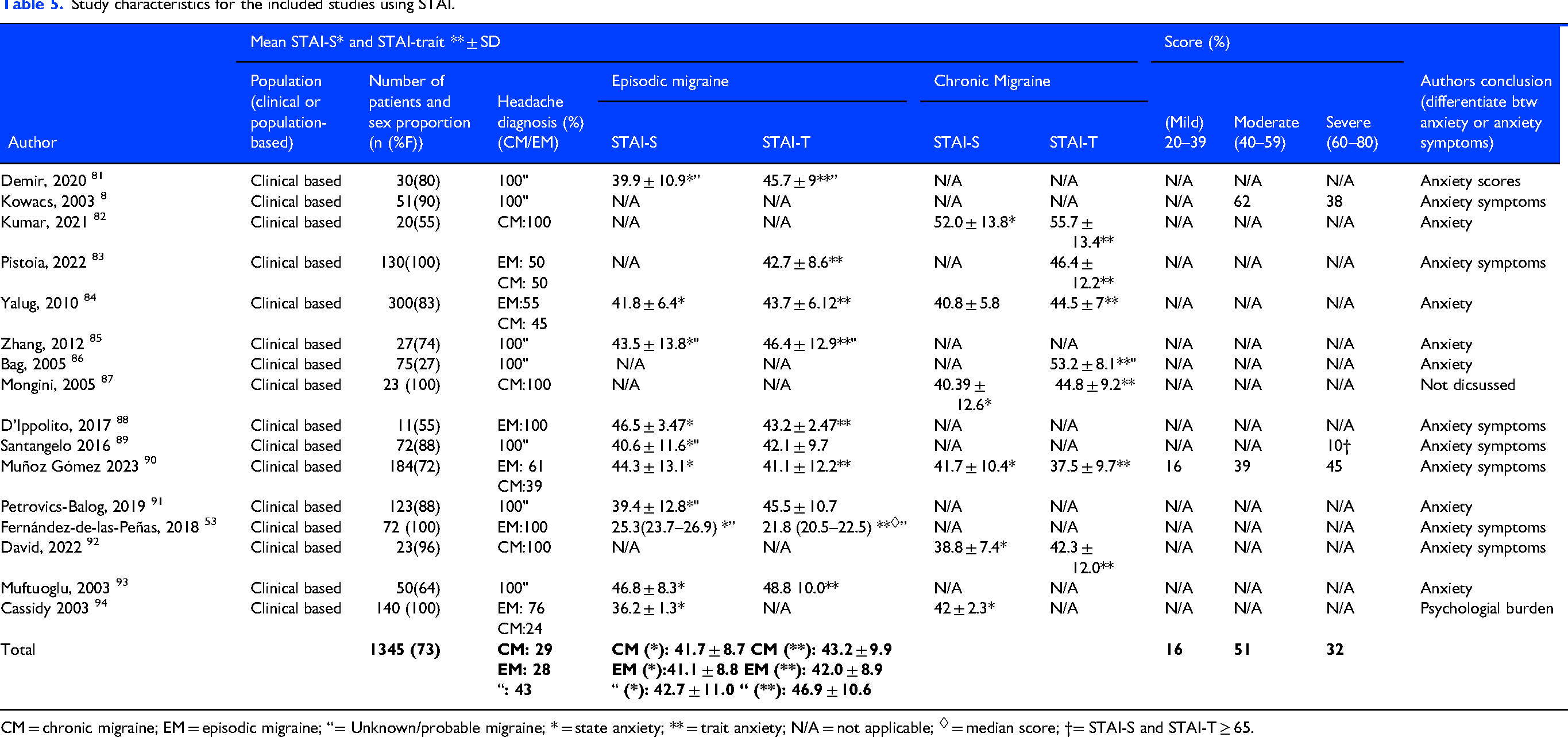
CM = chronic migraine; EM = episodic migraine; “= Unknown/probable migraine; * = state anxiety; ** = trait anxiety; N/A = not applicable; ◊ = median score; †= STAI-S and STAI-T ≥ 65.
For studies using the HAM-A (Table 6) 2074 participants were included: 34% with chronic migraine, 16% episodic migraine and 50% had unknown migraine or probable migraine. The mean scores were 18.1 ± 7.2, 13.9 ± 6.8, and 13.3 ± 8.9, respectively. All fourteen studies46,47,100,107–117 (100%) reported mean scores. Four studies98,101,105,106 (29%) reported proportion within a range and another four studies98,102,106,118 (29%) concluded that scores above the cut-off point indicated anxiety.
Study characteristics for the included studies using HAM-A.
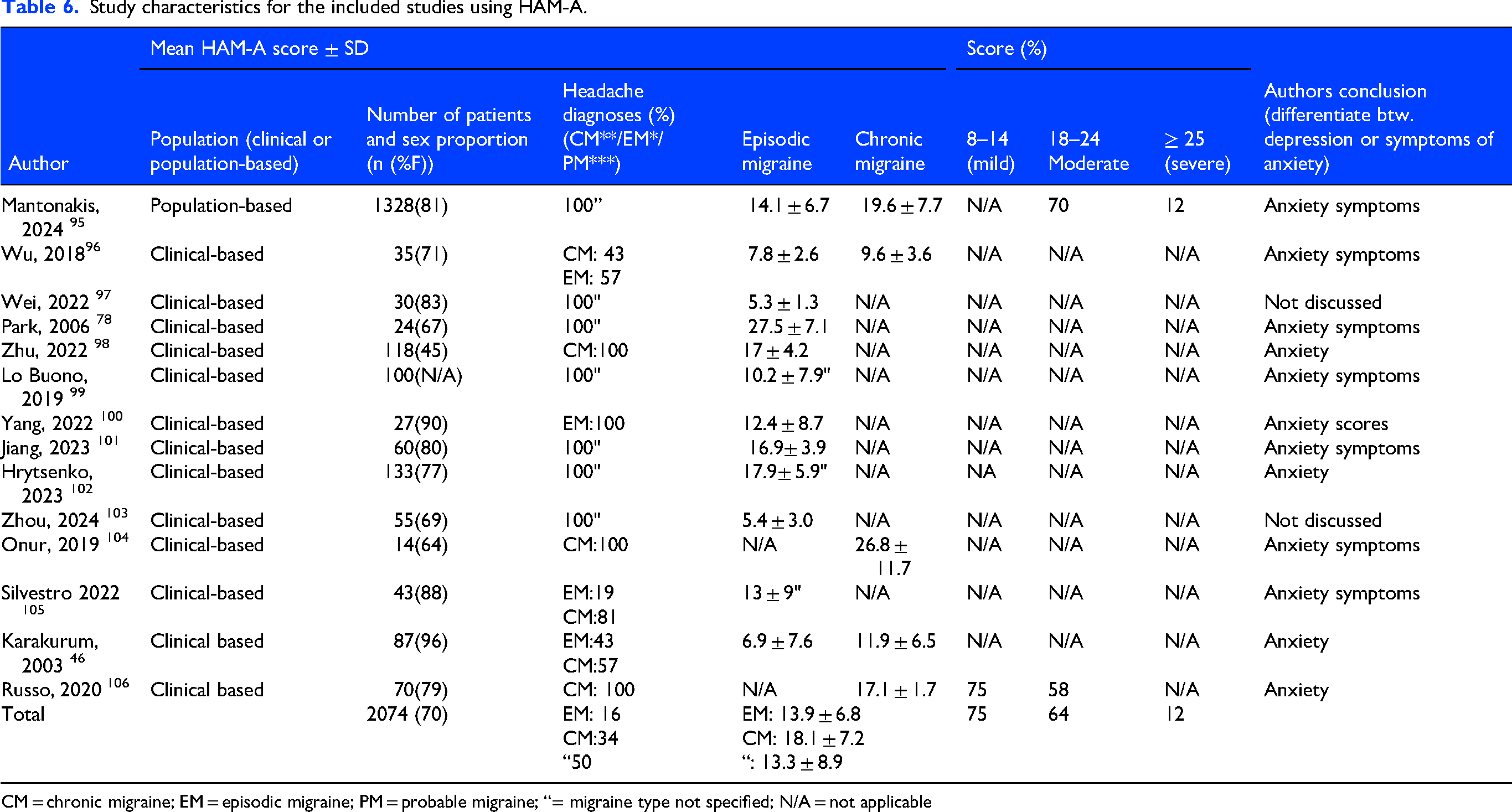
CM = chronic migraine; EM = episodic migraine; PM = probable migraine; “= migraine type not specified; N/A = not applicable
For studies using GAD-7 (Table 7) 19,399 participants were included: 40% chronic migraine, 36% episodic migraine, and 24% with unknown migraine or probable migraine type. The mean GAD-7 scores were 9.9 ± 5.5, 4.8 ± 5.2 and 5.8 ± 5.5 for chronic migraine, episodic migraine and unknown migraine type or probable migraine, respectively. Fourteen studies22,100,107–114119–122 reported mean scores, and two studies115,116 reported median. Seven studies107,108,110,114,120–122 (39%) reported proportion within score range and eight studies108,110–112116,120–122 (44%) concluded that scores above a cut-off point indicated anxiety.
Study characteristics for the included studies using GAD-7
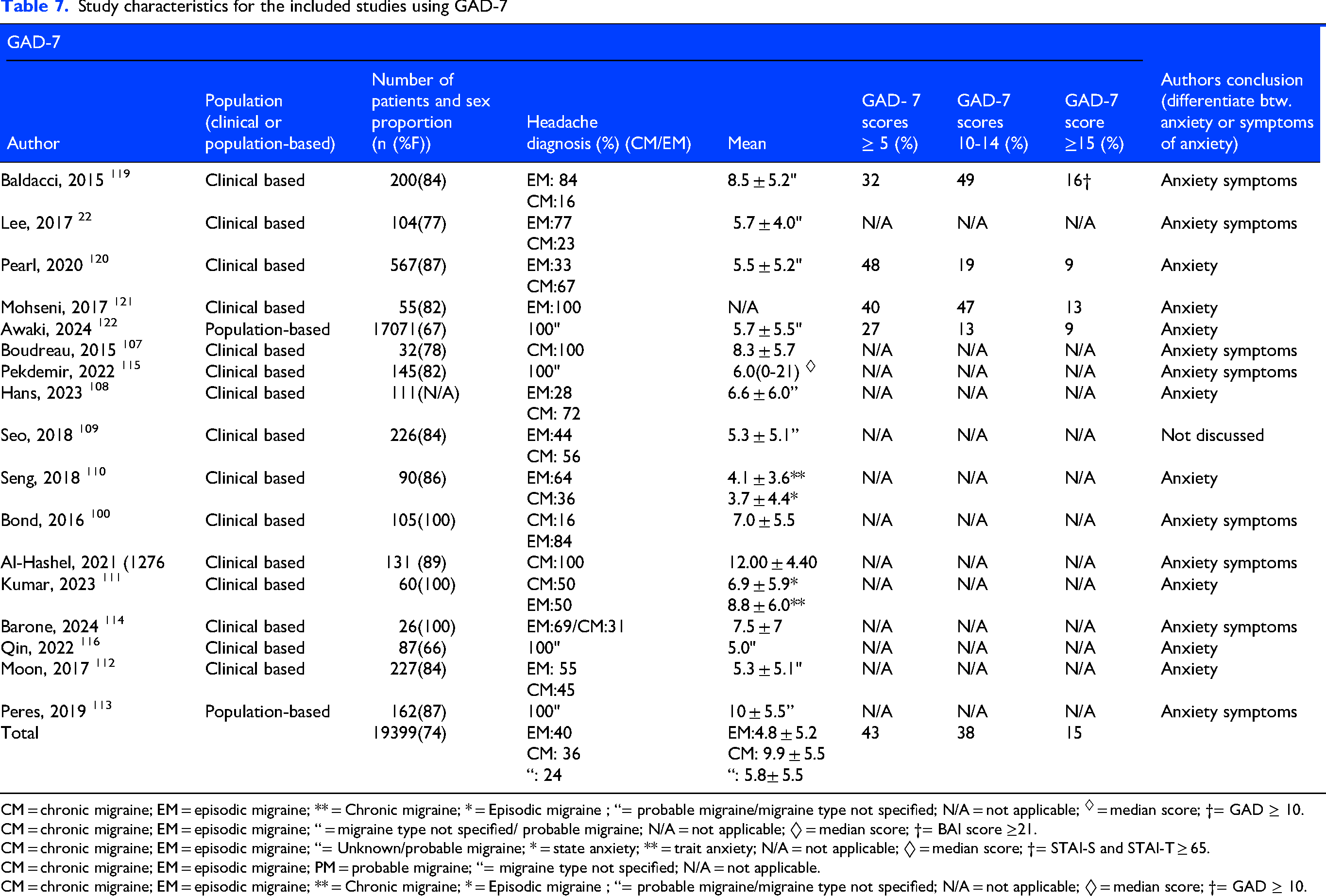
CM = chronic migraine; EM = episodic migraine; ** = Chronic migraine; * = Episodic migraine ; “= probable migraine/migraine type not specified; N/A = not applicable; ◊ = median score; †= GAD ≥ 10.
CM = chronic migraine; EM = episodic migraine; “ = migraine type not specified/ probable migraine; N/A = not applicable; ◊ = median score; †= BAI score ≥21.
CM = chronic migraine; EM = episodic migraine; “= Unknown/probable migraine; * = state anxiety; ** = trait anxiety; N/A = not applicable; ◊ = median score; †= STAI-S and STAI-T ≥ 65.
CM = chronic migraine; EM = episodic migraine; PM = probable migraine; “= migraine type not specified; N/A = not applicable.
CM = chronic migraine; EM = episodic migraine; ** = Chronic migraine; * = Episodic migraine ; “= probable migraine/migraine type not specified; N/A = not applicable; ◊ = median score; †= GAD ≥ 10.
Discussion
The main finding of this study is that 42 (41%) out of 98 studies used anxiety screening tools to diagnose anxiety. Among the studies that used the GAD-7, HADS, STAI and BAI, almost half of them used the screening tools as evidence of an anxiety disorder. In comparison, only 29% of studies using HAM-A used the score as an indicator of anxiety.
The use of screening tools as a diagnostic tool for anxiety
In this review, 42 studies were found to use questionnaires as evidence of anxiety. This approach was especially frequent in studies using screening tools validated in patients with migraine such as the GAD-7 and HADS.17,25 One reason may be that studies have treated screening tools as a diagnostic measure of anxiety. 12
For example, Spitzer et al. wrote that the GAD-7 scale was designed to reflect the DSM-IV diagnostic criteria for generalized anxiety disorder (GAD), 23 making it a valuable tool to complement clinical assessment and support the DSM-IV criteria for anxiety. However, this may not apply in cases where the screening tools have not been validated. Löwe 117 emphasized that a cut-off score ≥10 should be confirmed through extended diagnostic evaluation, highlighting that the screening tool should not stand alone in the diagnostic process. In addition, Veisy et al., concluded that GAD-7 is useful for quick screening, based on their comparison with SCID-5 (Structured Clinical Interview for DSM-5). 123 Therefore, the diagnostic interview should still be regarded as essential for both screening and intervention. Of the 98 included studies, only two compared the scores from anxiety screening questionnaires with results from a diagnostic interview for anxiety such as the SCID,123,124 and only one used the Mini International Neuropsychiatric Interview (MINI) as gold standard to validate its anxiety screening findings. 25 Nevertheless in 41% of the included studies, the screening tools were used to conclude that the patients had anxiety. These studies should compare the total screening scores and their subscale scores against a clinical interview to ensure diagnostic accuracy. While this approach is more time-consuming, it is essential for avoiding inaccurate estimates of anxiety prevalence.
Data presentation and interpretation
The presentation of data varied across the included studies, making systematic data collection challenging. In total, sixty studies (63%) reported the proportion of patients with chronic or episodic migraine, while the remaining studies did not distinguish between migraine types.22,34–3739–41,44–46,51–56,60–67,69,73–77,79,80,82–84,87,88,90,92,94,96,98,100,104–109,111,112,114,118–122,125,126 Eighty-three studies reported the mean screening score, and eight reported the median score. Different cut-off points were used in the studies, although most followed the standard cut-off points.1–4148,64,89,101,118 This may compromise cross-study comparisons and reduce the validity of the studies. Not all studies that concluded the presence of anxiety based on screening scores explicitly stated that the patients had anxiety. Instead, they emphasized that the score was an indicator of symptoms of anxiety. Phrases like “the percentage of patients meeting the criteria for anxiety and depression, was” 40 and “the higher the score, the worse symptoms of anxiety”74,86 were used. Such phrasing can be unclear and potentially misleading, as it may lead readers to assume that a clinical diagnosis had been made. While symptom scores may indicate the presence of anxiety symptoms, they do not necessarily equate to a clinical diagnosis. Accordingly, some authors who had screened for anxiety using a screening tool acknowledged that this method cannot replace diagnoses based on ICD or DSM criteria.8,36,115 The heterogeneity in data presentation, inconsistent cut-off points, and lack of clarity in reporting illustrate the methodological challenges across studies. These issues complicate cross-study comparison and highlight the need for clearer definitions and more precise data reporting in future migraine studies.
Selecting the appropriate screening tool
Selecting the appropriate screening instrument is essential, as its psychometric characteristics affect the accuracy of results. 127 If a screening tool has not been validated in the migraine patient population, its interpretability and usefulness are substantially reduced. Not accounting for these variables may result in misleading estimates of the prevalence of anxiety in patients with migraine.
Stein et al. argued that the GAD-7 is not specific to generalized anxiety disorder but is also relatively sensitive to other anxiety disorders. 128 In the context of migraine research, a high GAD-7 score can therefore reflect generalized anxiety, but it could also indicate other anxiety-related disorders. This supports the idea that screening tools are limited; they can measure the presence of anxiety symptoms but cannot differentiate between distinct anxiety disorders. Therefore, identifying overlapping conditions can help refine screening instruments, enabling them to distinguish true psychiatric disorders from comorbid symptoms. Even when an anxiety screening tool has been validated in the general population, its reliability must be critically reassessed in headache patients. An additional methodological issue rarely reported is whether anxiety screening questionnaires were completed during a migraine attack or outside of the migraine attack period. Since migraine related somatic symptoms can overlap with symptoms of anxiety, completing questionnaires during an attack may influence the reported anxiety scores. Future studies should therefore report whether questionnaires were completed in relation to migraine symptoms.
For instance, in a study involving 50 women, researchers compared the SCID with the Patient Health Questionnaire (PHQ) and found that the PHQ failed to identify 44% of the patients who met SCID criteria for at least one anxiety disorder. 129 Moreover, inconsistencies across studies have been reported regarding recommended cut-off scores, as well as the sensitivity and specificity of various screening tools.17,127 These inconsistencies can have both clinical and economic consequences. For example, in a systematic review 130 evaluating the accuracy of HADS in cancer patients, the authors reported variation in the threshold/cut-offs generated in varying prevalence estimates of both anxiety and depression. Consequently, selecting a screening instrument requires careful evaluation of its cut-off scores, validity, reliability and inherent limitations. Addressing these factors can improve the accuracy and interpretability of the screening results.
The study population
In this review, 93% of the studies were clinical-based. These patients are likely to have more complex medical histories than those in the general migraine population, which may contribute to a higher prevalence of anxiety. Studies comparing patients with headaches to healthy controls have shown that those attending a headache clinic experience a greater disease burden. They score higher on psychological scales and report more intense “most severe headache”. 131 Together, these observations highlight the need for more population-based studies to investigate the prevalence of anxiety in migraine. Comparisons between patients with chronic migraine and episodic migraine have demonstrated that higher headache frequency and intensity are associated with a greater disease burden and disability as well as anxiety.2,132 To better understand the prevalence of anxiety across different patient groups, it is thus essential to divide patients by headache frequency or intensity.133,134 Despite the use of similar anxiety screening tools, results varied considerably. This likely reflects the differences in the proportion of patients with chronic and episodic migraine and whether studies differentiated between these subgroups. Studies with a greater number of chronic patients with migraine tended to report higher mean scores and more patients in the moderate-to-severe range. In studies that did not categorize patients into subgroups, it is difficult to identify which factors may have influenced the results. Some studies may have divided patients by the occurrence of aura which we did not consider in this review. Over 80% of the participants in the included studies were female. Women generally report a higher migraine disease burden compared with men,132,135 and generally report higher anxiety scores. Therefore, the proportion of female participants should also be considered when interpreting study findings.
Comparing anxiety and depression screening tools in migraine
Depression-migraine comorbidity has been investigated, and studies have reported that migraine sufferers are two to four times more likely to experience depression. Asheer et al. found 35 out of 78 included studies (45%) of migraine-depression studies used screening tools as evidence of depression, equating a score above a cut-off with a diagnosis. 136 This approach tends to inflate prevalence estimates compared to diagnostic interviews; a finding supported by this study as well. Furthermore, Asheer et al. noted that only a few screening tools are formally validated for patients with migraine with only PHQ-9 and HADS-D validated in a headache population. Gantenbein et al. also emphasizes that the lack of migraine-specific validation is problematic since overlapping symptoms between migraine and depression can distort screening results. 137 As mentioned earlier, comparing the questionnaire results to structured psychiatric interviews provided the most accurate estimate of a diagnosis. In this review, very few studies made this comparison. Likewise, Asheer et al. found one out of 78 included studies used this method. As a result, the true accuracy of many anxiety screening tools in a migraine population remains uncertain. When comparing the use of anxiety screening tools versus depression screening tools in migraine, depression has received more methodological attention. For example, Levis et al. found that depression prevalence in migraine was 31% when using screening questionnaires but dropped to 17% with formal diagnostic criteria. 138 In contrast, anxiety screening tools have not undergone the same level of methodological scrutiny as depression. One study investigated the benefits and harms of an anxiety screening program and found evidence was insufficient to draw definitive conclusions. 139 Thus, anxiety screening tools have been evaluated to some extent, but the volume and depth of research remain more limited than for depression.
Limitations
This review has several limitations. As this study was designed as a narrative review rather than a formal systematic review, the literature search was limited to a single database (PubMed), and all studies were screened by one author (M.Y.H.P.). This may have increased the likelihood of unintentional exclusion of relevant studies, which could affect the quality and reliability of the review. This approach may also have increased the risk of selection bias during the screening process. Furthermore, not all retrieved studies were available in full text, leading to their exclusion. Additionally, several studies did not report mean scores or the percentage of participants within each severity level. Thus, reducing the amount of data. Moreover, not all included studies reported the proportion of patients with medication overuse, meaning some patients with medication-overuse headache (MOH) may have been included despite the exclusion criteria. One study found that anxiety and depression were more common in patients with MOH compared with patients with episodic migraine. 140 This may have caused patients with MOH to score higher on anxiety screening tools, contributing to variations across studies. In addition, no protocol was published or registered before the review was conducted, which limits methodological transparency and makes it more difficult to assess whether the review methods were prespecified. Given these methodological challenges, alternative approaches to improving the diagnostic validity have been proposed. One study suggested that headache studies investigating comorbid depression should apply the LEAD (Longitudinal Expert Assessment of All Data) as an index of validity. 141 There is reason to believe that the same approach can be applied to anxiety in headache studies. Like depression, anxiety is characterized by variable symptoms and frequent somatic comorbidities which can make the LEAD a useful tool for improving diagnostic accuracy. 142
Conclusion
Among the 98 studies that used anxiety screening tools in patients with migraine 42 (41%) of the studies applied the screening tools as evidence of anxiety. However, the screening tools are not intended to replace a validated diagnostic interview conducted by a psychiatrist for diagnosing anxiety disorders. Instead, they should only be used to measure the presence and severity of anxiety symptoms. A further challenge is the limited validation of these screening tools, as a few studies have compared them with a psychiatric gold standard such as structured diagnostic interviews (SCID and MINI) in patients with migraine. This process is further complicated by the overlap between anxiety symptoms and migraine-related somatic features which makes accurate assessment more difficult. This makes it harder to evaluate the accuracy of these tools. Therefore, studies should prioritize using screening tools that have been validated for the specific population under study, and authors should critically evaluate the obtained scores. Moreover, further research is needed to validate commonly used anxiety screening tools in patients with migraine such as HADS-A, HAM-A, GAD-7, and BAI. Overall, there is a need for clear guidelines regarding the use of anxiety screening instruments in patients with migraine. These implications of this review should, however, be interpreted with caution given the narrative design of the review, the use of a single database, the single reviewer screening process, and the absence of a published protocol.
Public health relevance
Almost half of the eligible studies used anxiety screening tools as evidence of anxiety, whereas only a few studies confirmed the diagnosis with a structured diagnostic interview. This resulted in potentially erroneous estimates of the prevalence of anxiety among patients with migraine. Correct diagnosis of anxiety disorders should be conducted in accordance with national and international guidelines and should not rely on a single screening questionnaire. More studies are needed to further validate commonly used anxiety screening tools in patients with migraine, such as the HADS A, GAD 7, HAM A, BAI and STAI. Clear guidelines for the use and interpretation of anxiety screening tools in patients with migraine are needed.
Footnotes
Acknowledgements
None.
Ethical considerations
The manuscript is a narrative review not requiring ethical reporting.
Consent to participate
Not applicable.
Consent for publication
All authors have reviewed and approved the final version of the manuscript and agree to publication in Cephalalgia, if accepted.
Author contributions
M.Y.H.P.: Conceptualization, Methodology, Investigation, Data Curation, Writing – Original Draft.
J.A.: Conceptualization, Writing – Review & Editing.
F.A.: Conceptualization, Writing – Review & Editing.
R.H.: Conceptualization, Writing – Review & Editing.
P.V.: Conceptualization, Writing – Review & Editing.
H.W.S.: Conceptualization, Methodology, Project Administration, Supervision, Writing – Review & Editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data availability is not applicable, as this is a narrative review based on previously published studies.
Open practices
Not applicable.