
Abstract
Background/Aim
Migraine and osteoporosis are highly prevalent in women and represent a substantial socio-health burden. We aimed to comprehensively assess bone status in women with frequent migraine.
Patients and Methods
Adult women with high-frequency episodic migraine (HFEM) or chronic migraine (CM) were recruited and compared with age- and body mass index–matched female controls. Serum parameters of bone metabolism, including 25-hydroxyvitamin D (25[OH]D), calcium and parathyroid hormone (PTH), as well as bone turnover markers (procollagen type 1 N-terminal propeptide [P1NP] and C-terminal telopeptide of type I collagen [CTX]), were measured. Bone mineral density (BMD), T-scores and trabecular bone score (TBS) were assessed by dual-energy X-ray absorptiometry.
Results
A total of 108 women with CM/HFEM and 129 matched controls were included. Compared with controls, women with migraine had lower serum 25(OH)D and calcium levels (p ≤ 0.001) and higher adjusted CTX levels (p = 0.039). Densitometric assessment revealed significantly reduction in BMD at femoral neck (g/cm2 and T-score) and total hip (T-score) in the migraine group (p < 0.001). Lumbar TBS was also lower in CM/HFEM patients (p < 0.001). After multivariable adjustment, TBS remained independently associated with migraine status. These alterations remained in women with HFEM and in those younger than 50 years, and were associated with reduced physical activity and sun exposure.
Conclusions
Women with frequent migraine exhibit impaired bone health, characterized by alterations in bone mass and trabecular microarchitecture. TBS appears to be a sensitive marker of early skeletal involvement in this population. The presence of bone impairment in HFEM and in premenopausal women supports early assessment of bone status and reinforcement of lifestyle interventions, including adequate physical activity and sun exposure.
This is a visual representation of the abstract.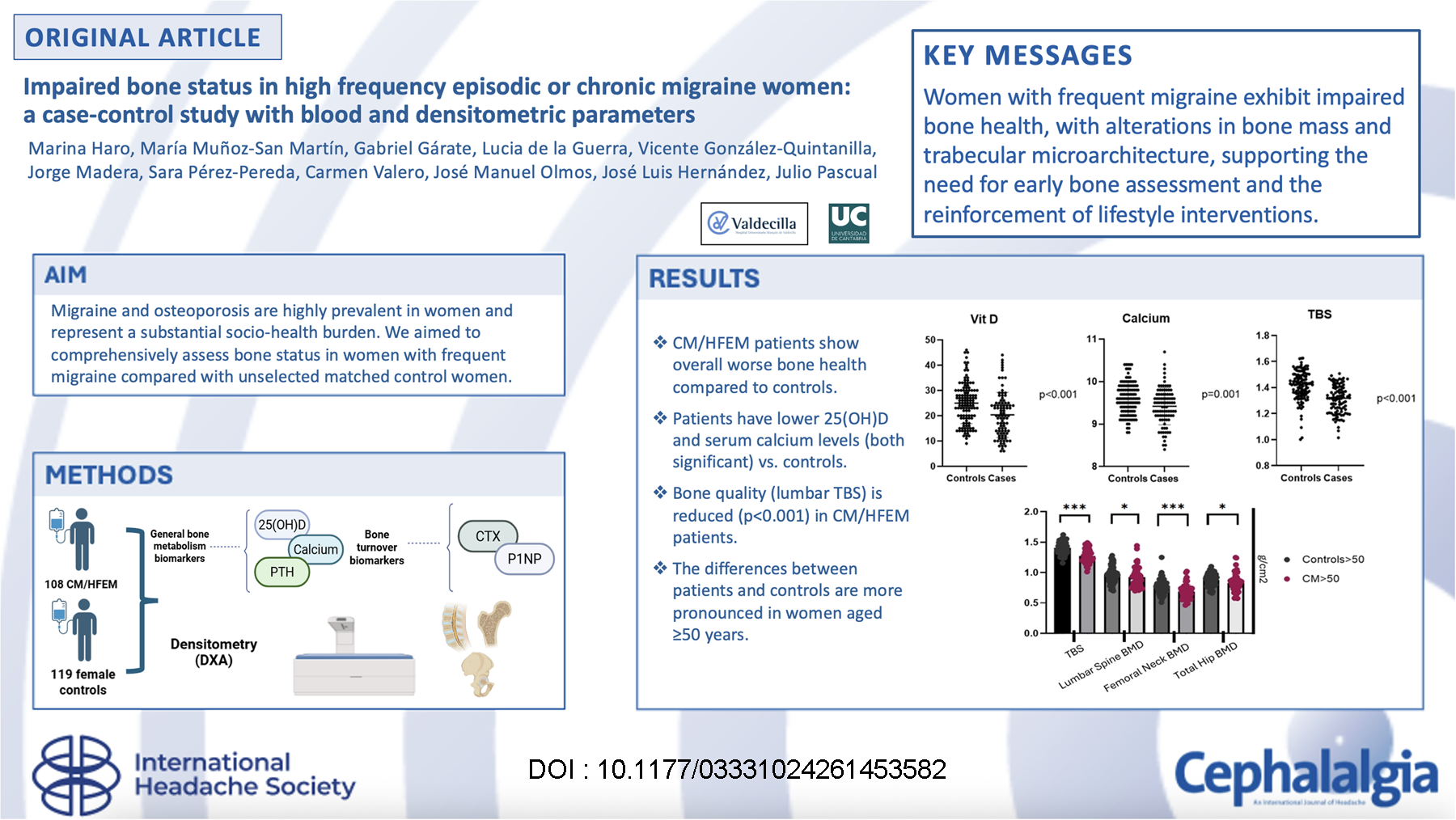
Introduction
Migraine and osteoporosis are frequent disorders with a highly negative impact in daily life activities.1,2 Both migraine, especially its most debilitating variant chronic migraine (CM), and osteoporosis are much more prevalent in women. According to the WHO criterion for osteoporosis, based on a value of −2.5 standard deviation (SD) or less in T-score for bone mineral density (BMD), around 6% of men and 21% of women aged 50 years are classified as having osteoporosis.2,3 In contrast to what happens in migraine, the prevalence of osteoporosis increases with age. The clinical repercussions of osteoporosis, such as the development of chronic pain and the morbidity and mortality associated with an increased risk of bone fractures, entail a high economic burden for healthcare systems due to increased hospitalizations and rehabilitation expenses. 4
Osteoporosis has been shown to be more frequent in a variety of unrelated chronic disorders, such as chronic obstructive lung disease, rheumatoid arthritis, multiple sclerosis, liver cirrhosis and celiac diseases, calling for a systematic assessment of bone health in chronic conditions. 5 The relationship between chronic diseases and BMD loss is explained by shared pathophysiological mechanisms, such the presence of low-grade chronic inflammatory states, which promote bone resorption and alter bone formation, the use of medications potentially influencing bone homeostasis and lifestyle changes inherent to these chronic diseases. All these pathophysiological mechanisms are applicable to migraine and especially to CM. A low-grade inflammatory status has been described in this condition 6 and also CM induces important lifestyle changes for bone homeostasis, such as reduced physical activity or sun exposure. 7 Finally, some drugs recommended for the preventive treatment of migraine can alter bone density. In fact, antiepileptic drugs also used for the preventive treatment of migraine, such as valproate or topiramate, can affect vitamin D and calcium metabolism and therefore bone mineralization. 8
The key involvement of calcitonin gene-related peptide (CGRP) in migraine pathophysiology is well-known, but blocking CGRP signaling may affect distant organ function, as CGRP or its receptor are expressed in a broad range of different organs, such as gut, immune system, cardiac, lung, renal, dermal and especially in bone tissues, whose periosteum is very rich in CGRP fibers.9,10 Alpha-CGRP, but not beta-CGRP isoform, 11 plays a crucial role in bone homeostasis upregulating bone formation and diminishing bone resorption by stimulating the proliferation of osteoblastic cells and inhibiting osteoclasts.12,13 This has been confirmed in experimental animals, where alpha-CGRP KO mice have been found to have reduced bone formation and developed osteopenia. 14 Alpha-CGRP has also been shown to play an important role in the repair of bone fractures. 15
Considering that women are predominantly affected both by migraine and osteoporosis, together with the growing body of evidence supporting the relevant role of alpha-CGRP in the regulation of bone mass and bone healing and the very negative impact of CM in daily activities which are important for keeping bone homeostasis, it seems obvious that bone metabolism should be assessed in women with frequent migraine. Consequently, our aim was to study in detail the status of bone in females with high-frequency migraine, therefore candidates to the new anti-CGRP medications, by using biomarkers of general bone metabolism, of bone turnover and densitometric parameters.
Patients and methods
Study participants
This is a case-control study nested in a prospective parallel cohort study, carried out between January 2021 and January 2024 and following the STROBE guideline. The study was’approved by the Ethics Committee of Investigations with Medications of Cantabria (Record 28/2020, 11th December). All participants gave and signed written informed consent for the inclusion in the study.
We recruited females with migraine fulfilling ICHD-3 high-frequency episodic migraine (HFEM) or CM criteria aged ≥18 years attending our Headache Clinic and who were candidates for anti-CGRP antibodies. 16 Following the regulations in our country, they had not responded to at least three oral preventatives and, in the case of CM’patients, also to onabotulinumtoxin type A. All patients were on preventatives at the time of the study measurements.
As parallel controls, we recruited females with similar age and body mass index (BMI) distribution as the CM/HEFM group with subjective absence of headache and without a history of migraine, who attended a primary care center in Northern Spain for their regular health examinations. At the baseline visit, subjects were interviewed by investigators and all participants provided data regarding age, weight, BMI, tobacco or alcohol consumption, presence of chronic disorders, and consumption of medications. We also asked patients if they were doing both the minimum recommended exercise to prevent osteoporosis (at least 30 min 3 days per week) 17 together with a minimum sun exposure and adequate vitamin D status (at least 5–15 min of sun exposure in face and arm during spring, summer and autumn). 18
Participants whose baseline assessment revealed the presence of conditions known to affect bone metabolism, such as osteoporosis treatment (selective estrogen modulator receptors, bisphosphonates, denosumab, teriparatide, abaloparatide or romosozumab), corticosteroids and diseases such as primary hyperparathyroidism, hyperthyroidism, kidney failure with serum creatinine >1.7 mg/dL, liver disease, malabsorption or cancer were excluded.
Biochemical tests
For each participant, we collected fasting blood samples between 09:00 and 11:00 h, to minimise diurnal variations of CTX and P1NP. Routine biochemical determinations, which included serum total calcium, creatinine and albumin, were measured by standard automated methods in an ADVIA 2400 Chemistry System autoanalyzer (Siemens, Germany). Serum concentrations of 25(OH)D, intact parathyroid hormone (PTH), procollagen type 1 N-terminal propeptide (P1NP), and C-telopeptide of type 1 collagen (CTX) were determined by a fully automated electrochemiluminescence system (Elecsys 2010, Roche Diagnostics, GmbH, Mannheim, Germany). In our laboratory, 19 the detection limit of serum 25(OH)D is 4 ng/ml, its intraassay coefficient of variation (CV) 5%, and its interassay CV 8.5%. Regarding intact PTH, the detection limit is 6 pg/ml, with a reference range of 15–65 pg/ml. Intraassay and interassay CV were 5.4% and 5.9%, respectively. The P1NP limit of detection was 5 ng/ml (reference range 20–76 ng/ml), intraassay and interassay CV 3.1% and 3.5%, respectively. CTX limit of detection was 0.010 ng/ml (reference range 0.100–1.000 ng/ml), intraassay and interassay CV was 4.2 and 4.7%, respectively.
Dual x-ray absorptiometry (DXA), and trabecular bone score (TBS)
BMD, expressed as grams per square centimeter, and T-scores (defined as the number of standard deviations (SDs) below the mean value for young people) were measured by DXA (Hologic QRD 4500, Bedford, MA, USA) at the lumbar spine, femoral neck and total hip.
To assess bone quality, trabecular bone score (TBS) was calculated from DXA images at the lumbar spine L1-L4 using TBS iNsight software (TBS iNsight V.2.1 Medimaps, Merignac, France). TBS microstructure values >1.310 are considered normal, between 1.310 and 1.230 partially degraded and <1.230 degraded. In vivo precision in our center is 0.4–1.5% at the different measurement sites.19,20
Statistical analysis
A between-group difference of approximately 5% in TBS was considered clinically meaningful, as it exceeds expected measurement variability and is consistent with the magnitude of skeletal microarchitectural changes associated with chronic low-grade inflammatory conditions. Based on this expected clinically meaningful 5% difference in TBS (Cohen's d = 0.5), a minimum of 63 participants per group was required to achieve 80% power at a two-sided alpha level of 0.05. The final study sample included 108 women with migraine and 129 population-based controls, providing >95% statistical power to detect the prespecified effect size.
Categorical variables are expressed as absolute and relative frequencies. The homogeneity of clinical characteristics of study groups was determined by Χ2 test or Fisher's exact test for categorical variables.
Continuous variables are reported as mean ± standard deviation (SD) and/or median and interquartile range [IQR]. Normality assumption of continuous and count data has been checked using the Shapiro-Wilk test. For normally distributed continuous data, the assumption of equal variances was verified by the Levene test of equality of variances. Continuous variables were assessed by the t-test, or Mann-Whitney U test as appropriate. A general linear model (GLM) was fitted to adjust for multiple covariates and to assess the independent effect of case–control status on the dependent variables. Models were progressively adjusted, including age, BMI, renal function and physical activity for general bone metabolism parameters; additionally adding vitamin D levels for bone turnover biomarkers; and further adding CTX and P1NP for densitometric parameters. All analyses were 2-tailed, and significance was set to 0.050. Missing data were handled using listwise deletion.
Statistical analyses were performed in Statistical Package for the Social Sciences (SPSS) version 31.0 (IBM SPSS Statistics, New York, USA). Figures were built using GraphPad PRISM v.10 (GraphPad Software, Boston, USA).
Results
Patients demographics
We included 108 CM/HFEM female patients (mean age 49.9 ± 9.8 years; range 24–74; median 50 years; [IQR]: 14; [43–57] years) and 129 female controls (48.3 ± 6.8 years; range 25–75; median 50 years; [IQR]: 4; [47–51] years; p = 0.246) (see Table 1 for more details). BMI of CM/HFEM females (mean BMI 25.1 ± 4.3; range: 17.2–35.9; median 25.1; [IQR]: 6.1; [22.0–28.1]) was matched (p = 0.135) to that of controls (mean BMI 25.9 ± 4.2; range: 15.5–36.3; median 25.3; [IQR]: 5.9; [22.9–28.8]). A history of anxiety-depression was more common in CM/HFEM females (68; 63.0%) as compared to controls (25; 19.4%; p < 0.001). Fibromyalgia was also more frequent in CM/HFEM (22; 20.4%) than in controls (6; 4.7%; p < 0.001). In addition, the number CM/HFEM patients who performed the minimum recommended physical exercise with solar exposure was significantly lower than that of controls (CM/HFEM: 45; 41.7%; controls: 127; 98.4%; p < 0.001) (Table 1). Thirty-three patients were using neuromodulators as preventive medications; 30 were on topiramate and the remaining 3 on valproate.
General characteristics of the participants.
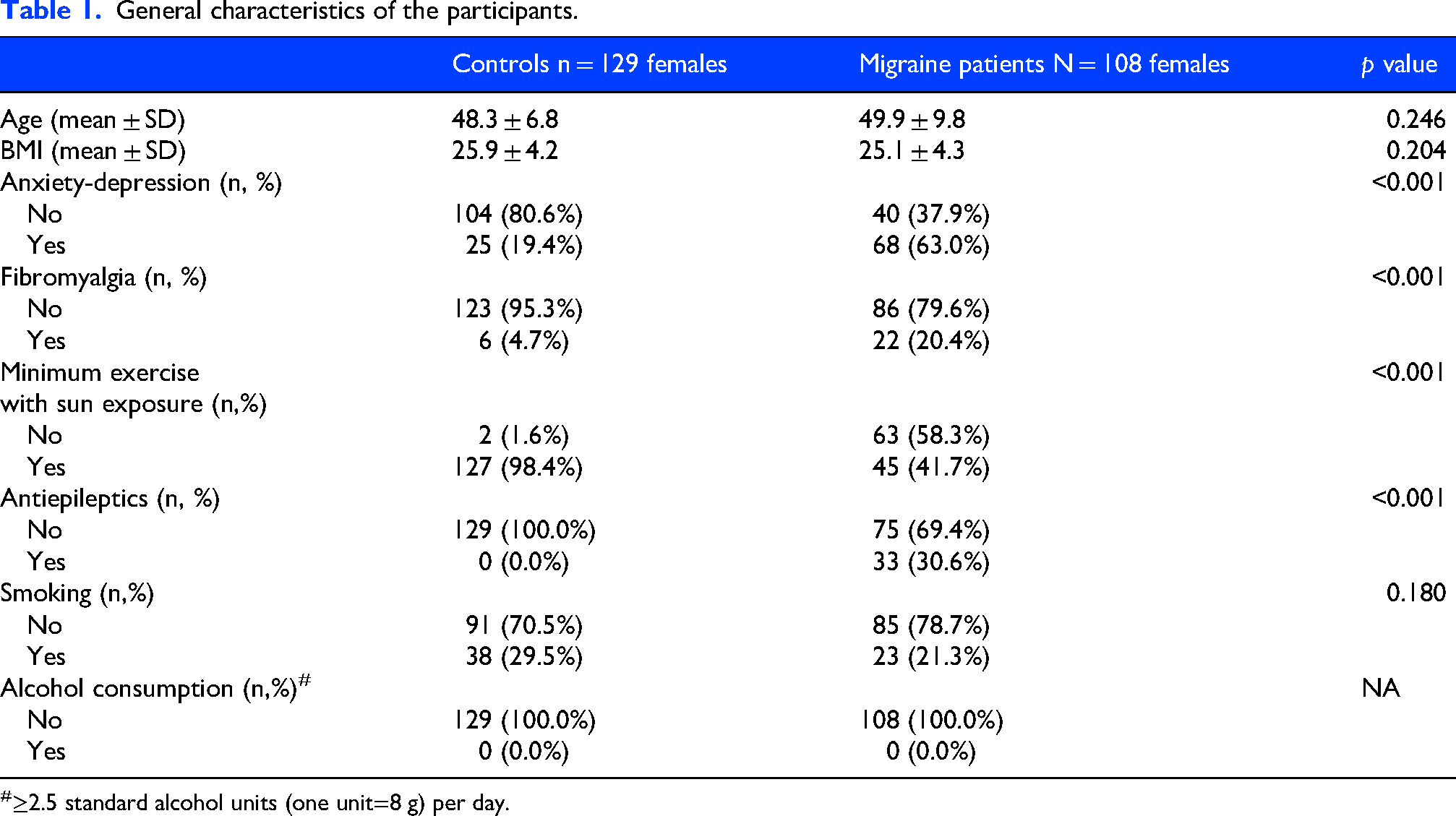
≥2.5 standard alcohol units (one unit=8 g) per day.
General bone metabolism parameters
Serum 25(OH)D levels were significantly decreased in CM/HFEM females (mean: 20.4 ± 8.9 ng/mL; range: 6–44; median 20.0; [IQR]: 12; [13.0–25.0] ng/mL) as compared to controls (mean: 25.0 ± 8.1 ng/mL; range: 9–46; median 25.0; [IQR]: 11 [19.0–30.0] ng/mL; p < 0.001).
PTH levels in CM/HFEM patients (mean 62.7 ± 30.8 pg/mL; range: 21–196; median 55.0 pg/mL; [IQR]: 26.5; [45.3–71.8] pg/mL) were not significantly different when compared to controls (mean 56.6 ± 22.6 pg/mL; range: 11–164; median 54.0; [IQR]: 24.0 [42.0–66.0)] pg/mL; p = 0.422).
Serum calcium levels in CM/HFEM females (mean 9.4 ± 0.4 mg/dL; range: 8.4–10.7; median 9.5; [IQR]: 0.5 [9.2–9.7] ng/mL) were significantly lower than those seen in controls (mean 9.6 ± 0.4 mg/dL; range: 8.8–10.4; median 9.6; [IQR]: 0.6 [9.3–9.9)] ng/mL; p = 0.001) (Figure 1, Table 2). These results did not change after multivariable analysis. Calcium intake was significantly higher in CM/HFEM patients (mean 950.8 ± 445.4; range: 235.0–2000.0; median 928.0; [IQR]: 678.5; [549.5–1228.0]) compared with controls (mean 711.7 ± 323.5; range: 0.0–2000.0; median 700.0; [IQR]: 448.4; [495.4–943.8]; p = 0.001). Additionally, we analyzed the correlation between calcium intake levels and blood calcium levels and found no significant association (Spearman's rho = 0.056; p = 0.476).
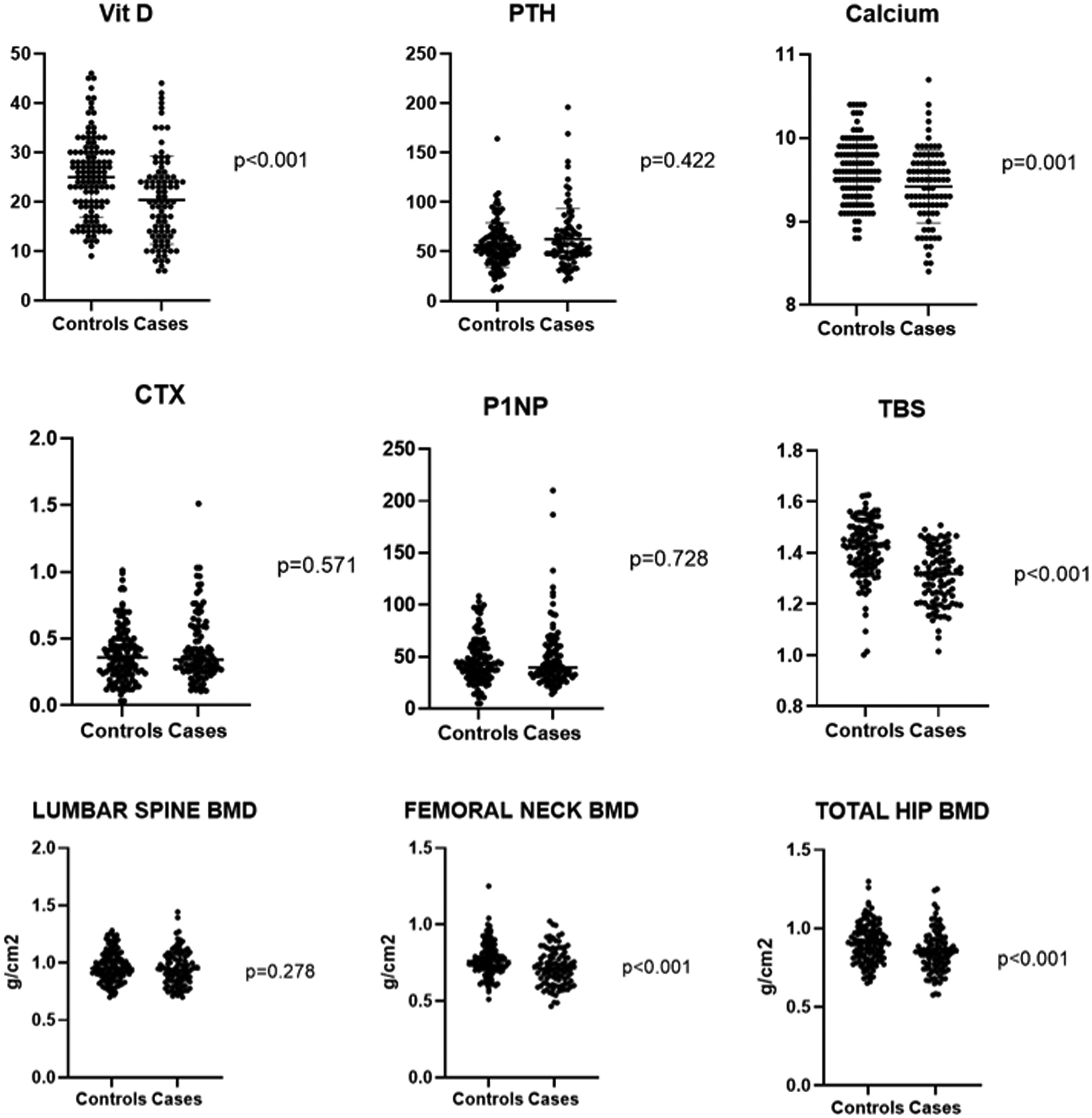
Summary of the unadjusted results for general bone metabolism (serum vitamin D, PTH and calcium values), for bone turnover biomarkers (CTX and P1NP) and for dual-energy X-ray absorptiometry (TBS and BMD) of women with HFEM/CM versus controls. See text for additional information.
Parameters of bone metabolism in controls vs migraine females.
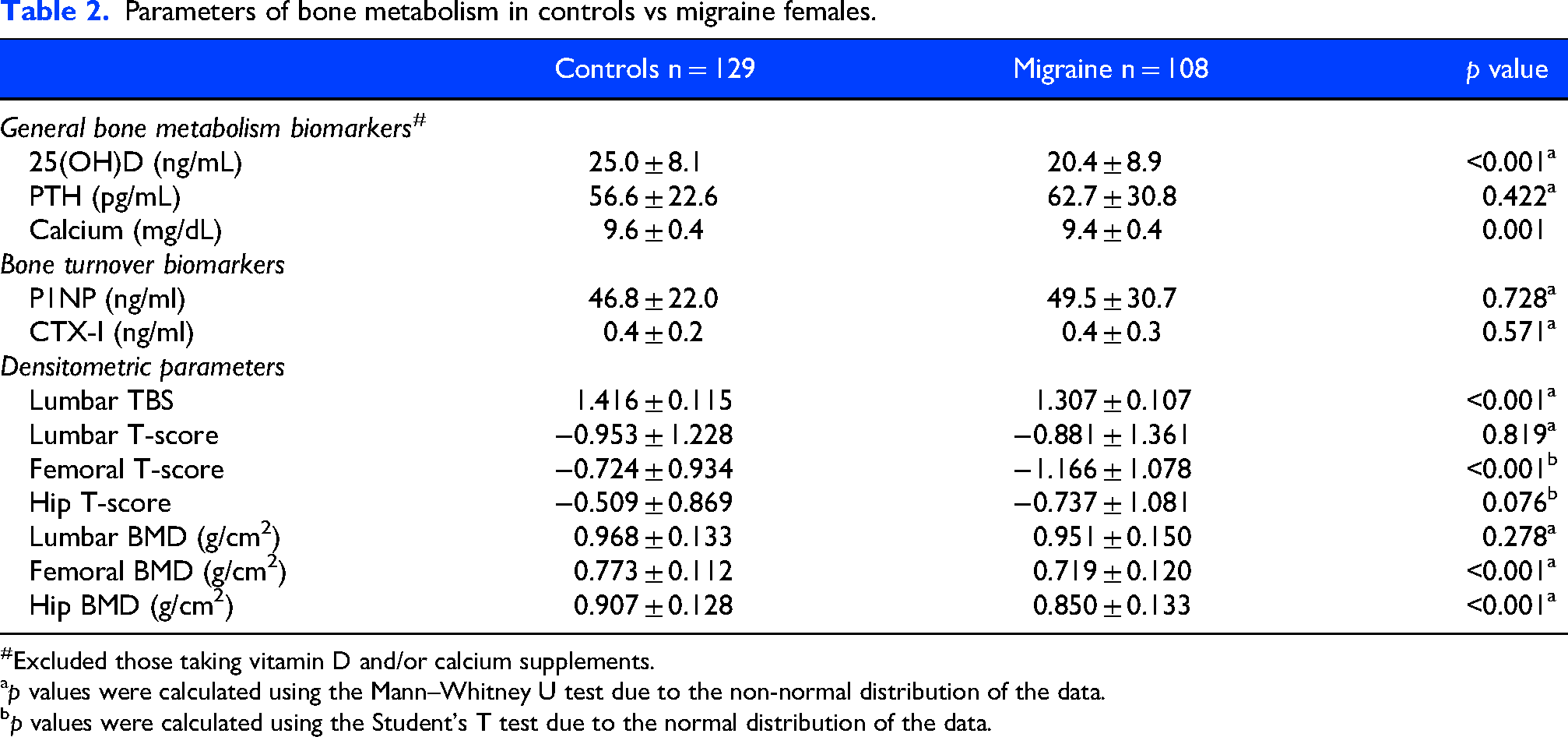
#Excluded those taking vitamin D and/or calcium supplements.
p values were calculated using the Mann–Whitney U test due to the non-normal distribution of the data.
p values were calculated using the Student's T test due to the normal distribution of the data.
Bone turnover biomarkers
P1NP levels in CM/HFEM patients (mean 49.5 ± 30.7 ng/ml; range: 14.1–210.0; median 40.3; [IQR]: 29.8 [30.5–60.3]) were not different to those found in controls (mean 46.8 ± 22.0 ng/ml; range: 5.0–108.5; median 43.4; [IQR]: 26.7 [32.1–58.8]; p = 0.728). Regarding CTX, levels did not differ between CM/HFEM (mean 0.419 ± 0.250 ng/ml; range: 0.106–1.510; median 0.343; [IQR]: 0.307 [0.257–0.564) and controls (mean 0.384 ± 0.207 ng/ml; range: 0.033–1.010; median 0.360; [IQR]: 0.258 [0.240–0.498]; p = 0.571) (Table 2). After adjustment for multiple covariates, the analysis revealed that patients had significantly higher levels of CTX than controls (0.450 vs. 0.361; mean difference 0.089; 95% CI 0.004 to 0.173; p = 0.039) (Figure 1, Table 2).
Imaging parameters of bone metabolism
Values for lumbar spine, total hip and femoral neck BMD (g/cm2 and T-Score), as well as lumbar TBS in CM/HFEM females and controls appear in Table 2. Differences showing a worse bone quality/density in HFEM/CM patients as compared to controls were noted for lumbar TBS (p < 0.001), T-score for femoral neck (p < 0.001) and for both total hip (p < 0.001) and femoral neck BMD (p < 0.001). After adjustment for multiple covariates, only TBS remained significantly associated with the study group; patients exhibited significantly lower TBS values than controls (adjusted mean 1.319 vs. 1.404; mean difference −0.085; 95% CI −0.129 to −0.041; p < 0.001) (Figure 1 and Table 2).
Other analyses: Age, use of antiepileptics and diagnostic subgroups
When stratified by age (<50 and ≥50 years), significant differences in CM/HFEM subjects younger than 50 years versus controls of the same age were limited to lumbar TBS and total hip BMD. In women with frequent migraine over 50 years of age, all densitometric parameters, with the sole exception of the lumbar T-score, were significantly worse than those of control women of the same age (Figures 2 and 3, Table 3). While hip BMD was the only densitometric parameter statistically different in controls >50 years versus those ≥50 years, most serum turnover and densitometric parameters impaired significantly in HFEM/CM females aged ≥50 years (Table 4).
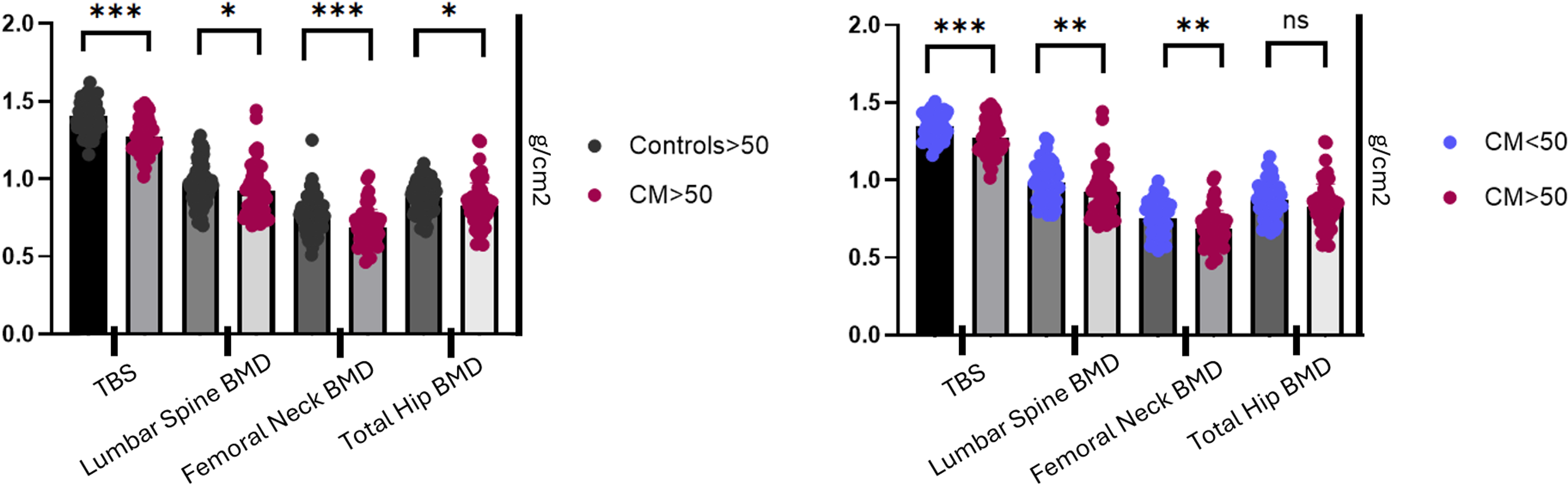
Analyses of dual-energy X-ray absorptiometry according to age. A: Densitometric parameters in women aged >50 years with CM versus controls. B: Comparison of densitometric values in CM women aged <50 years versus those ≥50 years. ***< 0.001, **< 0.01, *< 0.05.
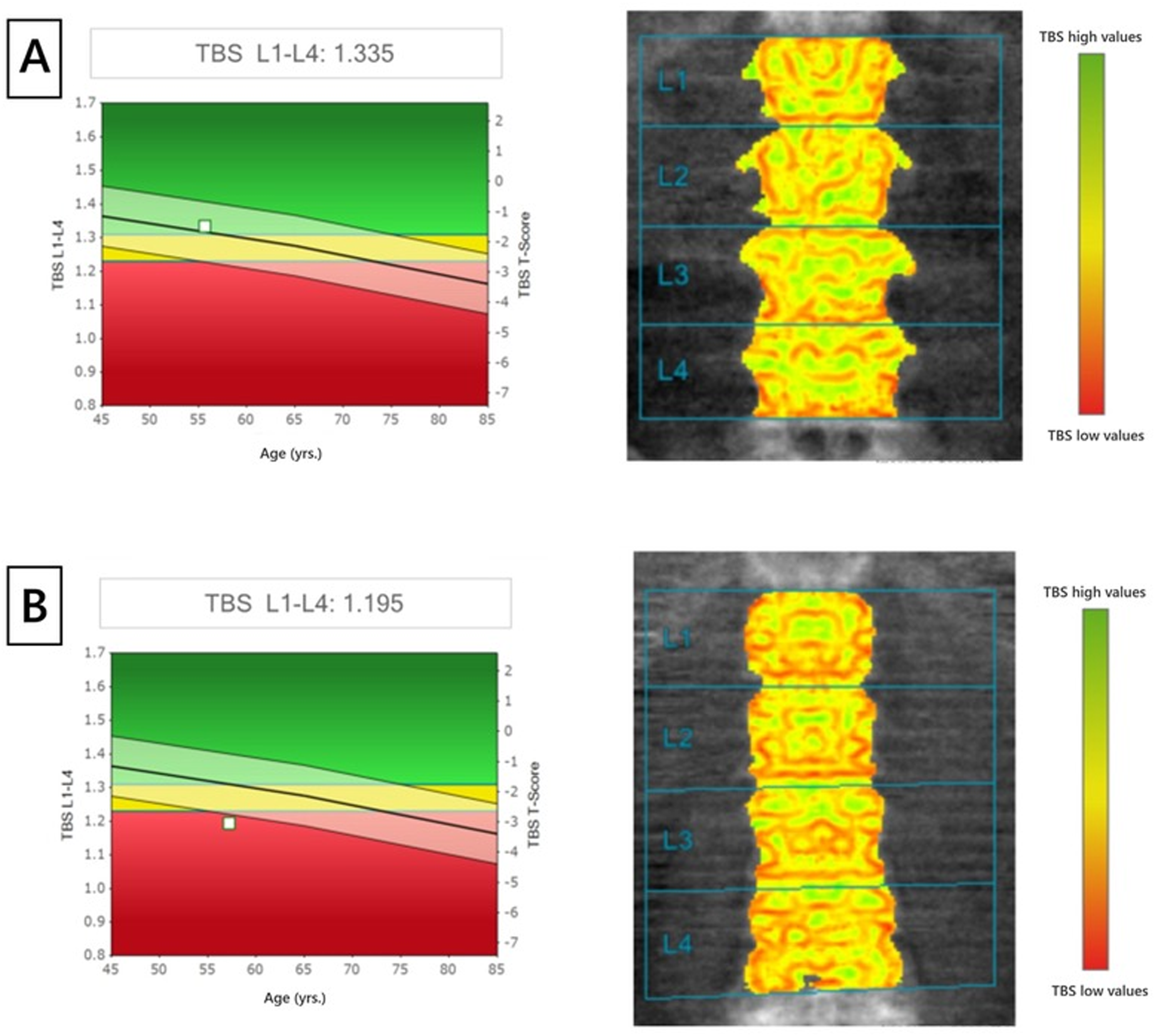
A: TBS assessment from a control woman. A score of 1.335 indicates a well-preserved bone microarchitecture. The corresponding spatial mapping displays a dense, homogeneous trabecular network. B: TBS assessment from a matched woman with CM. The lower score (1.075) demonstrates severe microarchitectural degradation. The marked decrease into the red-zone indicates a loss of structural integrity.
Parameters of bone metabolism in controls vs migraine by age.
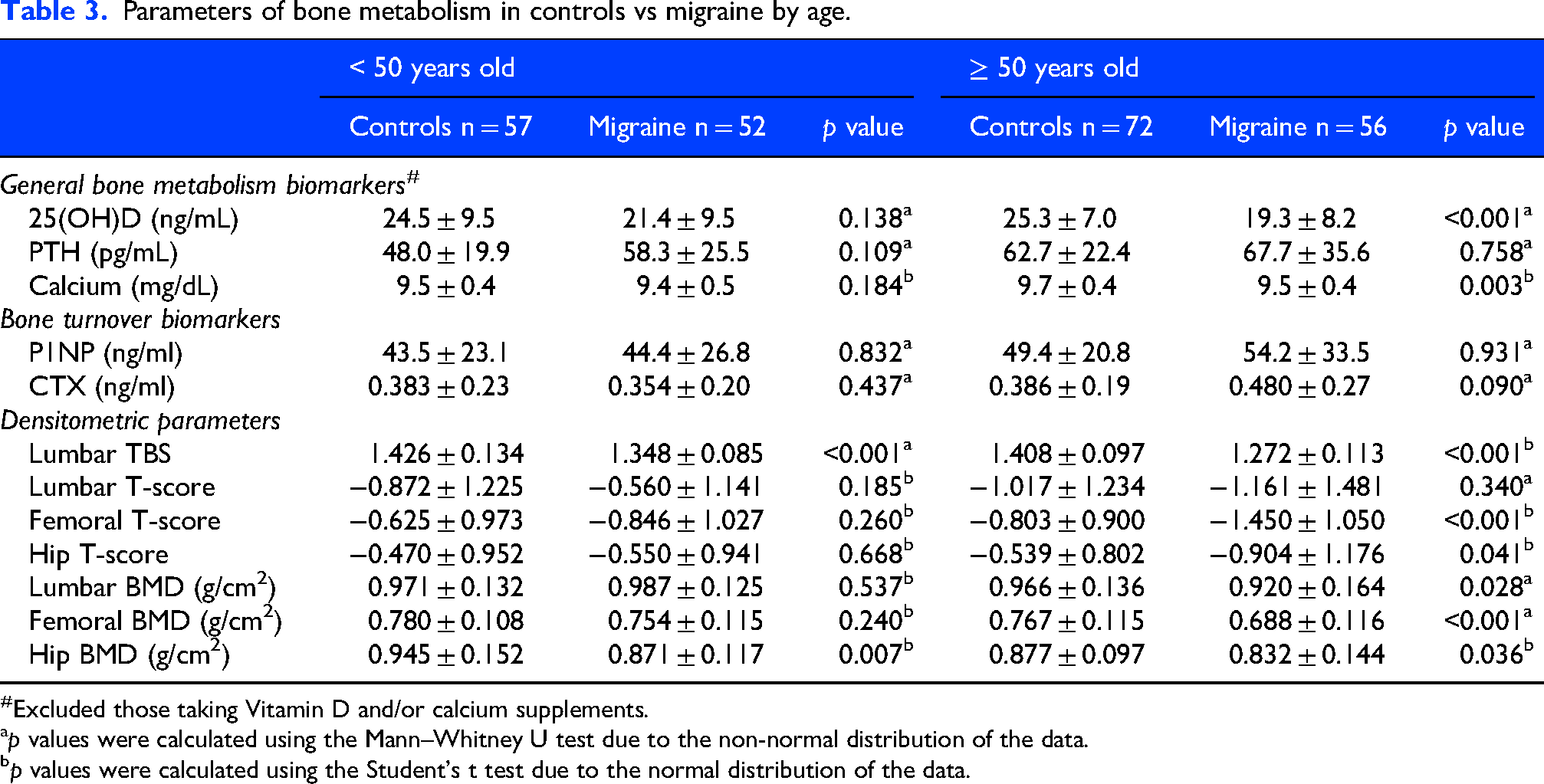
Excluded those taking Vitamin D and/or calcium supplements.
p values were calculated using the Mann–Whitney U test due to the non-normal distribution of the data.
p values were calculated using the Student's t test due to the normal distribution of the data.
Analysis of parameters of bone metabolism in controls and migraine women aged <50 vs ≥50 years.
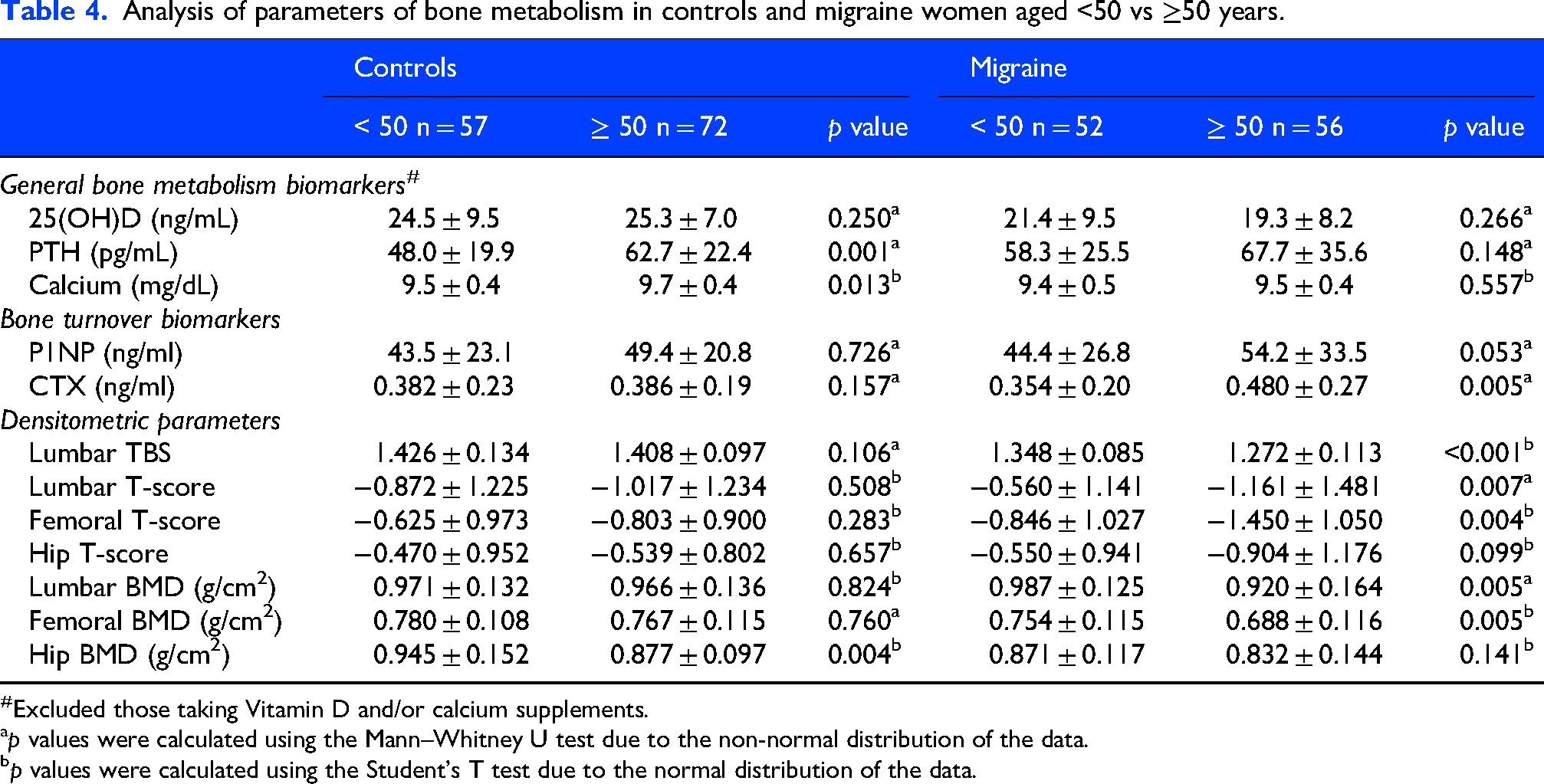
Excluded those taking Vitamin D and/or calcium supplements.
p values were calculated using the Mann–Whitney U test due to the non-normal distribution of the data.
p values were calculated using the Student's T test due to the normal distribution of the data.
We did not find significant differences in any bone parameter between patients with and without use of antiepileptic drugs.
Despite the relatively small number of patients with HFEM (n = 23), this group already exhibited significantly worse bone quality and density compared with controls. Specifically, HFEM patients showed lower lumbar TBS (1.270 ± 0.089 vs 1.416 ± 0.115; p < 0.001) and lumbar BMD (0.896 ± 0.111 vs 0.968 ± 0.133 g/cm2; p = 0.027). In addition, both femoral neck T-score (−1.539 ± 0.999 vs −0.724 ± 0.934; p < 0.001) and BMD (0.678 g/cm2 ± 0.110 vs 0.773 g/cm2 ± 0.112; p = 0.002) were significantly lower in the HFEM group, as were total hip T-score (HFEM: −1.294 ± 0.807; Controls: −0.509 ± 0.869; p < 0.001) and BMD (0.771 g/cm2 ± 0.097 vs 0.907 g/cm2 ± 0.128; p < 0.001).
Discussion
This is the first study specifically analyzing bone metabolism in women with frequent migraine (HFEM/CM) using laboratory and imaging parameters. Our data indicate that, overall, the bone health of women with HEFM/CM is worse than that of age- and BMI- matched women from the general population.
Women with frequent migraine exhibited significantly lower serum levels of both vitamin D and calcium compared with matched controls, indicating an overall impairment of mineral homeostasis. Reduced vitamin D levels in patients with migraine have been consistently reported in previous studies and are commonly attributed to behavioral factors, such as decreased outdoor activity and sun exposure due to headache-related disability and photophobia.21,22 In line with this, reduced physical activity and sun exposure were highly prevalent in our migraine cohort and were strongly associated with lower vitamin D levels. The concomitant reduction in serum calcium, although remaining within the normal range, may reflect a chronic, borderline negative calcium balance, possibly secondary to vitamin D deficiency and reduced intestinal calcium absorption.
Our next approach was to determine the levels of two specific bone remodeling markers: P1NP and CTX. 23 These peptides reflect bone formation and resorption, respectively. In our study, although unadjusted CTX values did not differ between groups, multivariable analysis revealed significantly higher CTX levels in the migraine group, consistent with a subtle but sustained increase in bone resorption.
Concerning DXA parameters, patients with frequent migraine had significantly lower BMD at femoral neck and total hip, and lumbar TBS. How do these results translate into clinical practice? Osteoporosis is characterized by low bone mass, bone fragility and increased fracture risk. Resilience to fracture depends on two pillars: bone mass (the amount of bone present) and bone microarchitecture (the material and organizational properties of bone). The T-score for the femur (normal values above −1), as an example of bone mass biomarker, was within normal limits (−0.7) for the control women and −1.2 in those with frequent migraine, which falls within the range of osteopenia and already represents a fracture risk twice as high as normal.24,25 Ideally, the skeletal assessment of bone fragility should also capture bone microarchitecture as the second pillar of fracture resilience to improve the identification of individuals at high risk of fracture. TBS provides a validated index of bone microarchitecture and correlates with mechanical properties of bone.26–28 TBS is able to predict hip and major osteoporotic fracture risk, at least partly independent of BMD parameters, being a densitometric biomarker potentially amenable to change as a result of pharmacological therapy.27,28 While mean TBS of our control women (1.416) is within the normal range (≥1.350), TBS of women with frequent migraine (1.307) is considered as early marker of a partially degraded bone and associates a moderate to medium fracture risk. In fact, vitamin D plus calcium together with anti-resorptive treatment, together with life-style changes, should be considered for women with these TBS scores according to current guidelines. 29 Interestingly, TBS was the only densitometric biomarker which remained significant after adjustment for a number of factors known to potentially influence bone metabolism.
In this study, women with frequent migraine exhibited a significant reduction in TBS values compared with population-based controls, indicating some deterioration of trabecular bone microarchitecture. In contrast, circulating levels of the dynamic bone remodeling biomarkers, showed differences only for CTX and after multivariate adjustment. These findings suggest that subtle but sustained increase in bone resorption would explain the observed microarchitectural changes in women with migraine. Our results highlight the sensitivity of TBS as an early structural biomarker capable of detecting subclinical skeletal changes not so accurately captured by conventional bone remodeling markers26–29 and suggest that migraine may be associated with long-term skeletal vulnerability independent of standard biochemical measures of bone metabolism.
Considering the decline in bone quality that occurs under physiological conditions after the onset of menopause, we specifically analyzed parameters of bone health in women under and over 50 years of age, which is the average age of menopause in our country.30–32 As in the overall study, serum vitamin D and calcium levels remained significantly reduced compared to control women, while bone turnover biomarkers were not significantly different in women with frequent migraine. Regarding bone densitometry, in patients with frequent migraine under 50 years of age, the values for hip BMD and lumbar TBS remained significantly worse than those of control women in the same age range. In women with frequent migraine over 50 years of age, all densitometric parameters, with the sole exception of the lumbar T-score, were significantly worse than those of control women of the same age. In this latter age group, we also observed a numerical increase in P1NP levels and, especially, in CTX, the biomarker of bone destruction, which in this case approached statistical significance. In line with this, bone metabolism parameters remained significantly worse than those of controls in the group of HFEM, despite the rather low numbers of HFEM patients in this series. These results show us that bone health in women with frequent migraine worsens with age and during menopause more than expected from physiological aging even in women with HFEM, but the analysis in younger women with migraine, in premenopausal age, indicates that even at these younger ages women with frequent migraine present indicators of worse bone health, both in quantity (BMD), and in trabecular quality (TBS). Although the observed between-group difference in TBS was relatively large (≈8%), this magnitude is consistent with a large standardized effect size (Cohen's d ≈ 1.0) and remained within a biologically plausible range for microarchitectural bone deterioration. Considering the narrow physiological range of TBS values, modest absolute differences translate into substantial relative changes, supporting the clinical relevance of the findings. 29
Given the rising burden of osteoporosis (1–4), in terms of costs and disability—including death—it seems desirable, in light of these data, to consider screening for metabolic bone disease in patients, especially women, with a history of HFEM/CM. Ideally, this screening should be carried out soon after diagnosis, also in the HFEM phase, in order to try to avoid the negative consequences of bone mineralization deficiency.
What could be the pathogenetic mechanisms of this impair bone status in women with frequent migraine? A variety of factors have been involved in the pathophysiology of osteoporosis in chronic disorders. Some of the most common, such as alcohol or tobacco consumption or malnutrition, can be immediately ruled out in our patients. Migraine, especially in its more severe forms of HFEM/CM, is known to negatively influence many aspects of daily life, including physical activity, which worsens migraine pain, or’sunlight exposure, which can develop a migraine attack or impair photophobia. 7 Lack of physical activity and sun exposure, as happened in our women with frequent migraine, correlates with low 25(OH)D levels and is one of the explanations for the insufficient bone mineralization in women with frequent migraine,21,22 though we cannot rule out an influence of comorbid conditions, such as fibromyalgia or anxiety-depression. The use of drugs, such as neuromodulators, as preventatives can also be another factor that could contribute to bone deficit, 8 though we could not confirm a significant influence in our series. Finally, we must remember that CGRP, and fundamentally its alpha-CGRP isoform, plays a relevant role in bone homeostasis. Indeed, under physiological conditions, CGRP regulates bone metabolism by stimulating osteoblast differentiation and inhibiting osteoclast formation, and alpha-CGRP is essential for fracture healing and is one of the peptides responsible for innate bone fracture pain.13–15,33 Theoretically, taking into account the aforementioned effects of alpha-CGRP on bone homeostasis, the long-term antagonism of CGRP could have a deleterious effect on the bone health of women with frequent migraine. This, however, has not occurred in two preliminary observational studies with a low number of cases.34,35
Limitations and strengths
This study has several limitations. Reflecting clinical practice, our women with HFEM/CM were not homogeneous, with a variable disease duration, use of preventives, abortive medications, different presence of comorbidities, and a history of failure to oral preventatives and botulinum toxin type A (in the case of CM). Therefore, our findings would be only extrapolatable to this subset of females with frequent migraine. Secondly, the cross-sectional nature of the study precludes the evaluation of longitudinal change in bone health in the participants. One unresolved issue in this study is the effect antiseizure drugs as a potential confounder, given the rather low number of patients who were taking neuromodulators. Finally, further data need to validate CM/HFEM as an independent risk factor for osteoporosis as our findings are limited to a single centre. Among the strengths, we would like to point out the good clinical characterization of the women participating in the study, the homogeneity of the methodology since all the women came from a single center and that it is the first time that bone health has been analyzed in a large group of women with frequent migraine compared with well-matched (unselected) women from the general population.
Conclusions
In summary, by using a variety of laboratory and imaging parameters, we found that women with HFEM/CM show worse bone health than age and BMI matched control women. In addition to confirming vitamin D deficit, multivariable analysis revealed significantly higher CTX levels in women with migraine, indicating a subtle but sustained increase in bone resorption. This finding is consistent with the densitometric results, which showed lower BMD at the femoral neck and total hip, and with the significant reduction in lumbar TBS observed in the migraine group. Taken together, these data suggest that a modest but persistent increase in bone resorption may contribute to both reduced bone mass and impaired trabecular microarchitecture. The fact that TBS remained independently associated with migraine status after full adjustment supports its role as a sensitive marker of early skeletal involvement, potentially preceding more pronounced changes in BMD.
Bone deterioration is also observed in women of childbearing age with HFEM. Our data suggest that bone status should be evaluated in women with frequent migraine, without waiting for menopause. Among contributing factors, reduced physical activity and limited sun exposure, likely resulting from migraine-related disability, showed the strongest association with poor bone health. Therefore, beyond correcting vitamin D or calcium deficiencies and prescribing anti-resorptive therapy when indicated, early emphasis on healthy lifestyle habits, including regular exercise and adequate sun exposure, is warranted.
Clinical implications
HFEM/CM women show impaired bone health, correlated with reduced physical activity and sun exposure.
These women show increased bone resorption, which may contribute to reduced bone mass and impaired trabecular microarchitecture, as shown by TBS in densitometry.
The presence of bone impairment in HFEM and in premenopausal women calls for early assessment of bone status and lifestyle interventions.
Footnotes
Acknowledgements
We wish to express our sincere appreciation to the patients for participating in this study. We also acknowledge our colleagues M. García-Unzueta and A. Maiztegui for their assistance with the laboratory determinations, Raquel Pascua for her help in densitometric studies and our nurses M. Sánchez and N. Cavada for their patience with the blood samples.
ORCID iDs
Ethical considerations
The study was approved by the Ethics Committee of Investigations with Medications of Cantabria (Record 28/2020, 11th December).
Consent to participate
All participants gave and signed written informed consent for the inclusion in the study.
Consent for publication
We, as the authors, submit this paper to Cephalalgia and agree to publish it if accepted.
Author contributions
J.P., J.M.O. and J.L.H. designed the study and wrote the manuscript. M.H., M.M.S.M., and G.G. analysed the data. M.H., G.G., VG.Q., J.M., S.P.P., C.V. and J.P. recruited participants for the study. All authors reviewed, contributed and edited the final draft. All authors approved the final version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication is part of the grant JDC2022-048637-I (M.M.-S.M.), funded by MCIN/AEI/10.13039/501100011033 and through the project from the Instituto de Salud Carlos III PMP22/00183, funded by the Recovery and Resilience Plan by the European Union NextGenerationUE.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets of the current study are avalilable from the corresponding author on reasonable request.