
Abstract
Background
Cognitive functioning worsens during migraine attacks and in the interictal period, especially in chronic migraine. This study aims to evaluate whether preventive treatment with anti-CGRP monoclonal antibodies (mAbs) or botulinum toxin (BoNT) improves interictal cognitive performance in migraine patients, and to compare cognitive changes between treatment responders and non-responders, controlling for treatment type.
Methods
A two-center prospective longitudinal comparative study of patients with Episodic (EM) or Chronic (CM) migraine receiving either mAbs or BoNT. Participants underwent two comprehensive cognitive evaluations targeting attention/processing speed, executive functions, episodic memory, and language, at baseline (visit 1) and after three to six months of treatment (visit 2). The primary end point was the degree of improvement measured by the z scores of each cognitive domain (adjusted for age and education), from baseline to follow-up, assessed using repeated-measures analysis with time as the within-subject factor and treatment response as the between-subject factor, controlling for treatment group. Treatment response was defined as a decrease in monthly moderate-to-severe headache days of ≥30% in CM or ≥50% in EM at follow-up.
Results
One hundred patients were included, and 90 completed the study (median age = 42 years, 96.7% women, 58 (64.4%) with CM, 64 (71.1%) treated with mAbs, and 26 (28.8%) with BoNT. Forty-seven (52.2%) were responders (59.4% in the mAbs group and 34.6% in the BoNT group) after a mean follow-up time of 4.5 months. Improvement in a measure of executive functions (comprising tests of working memory, alternating attention, and phonological fluency) was significantly higher in responders than in non-responders, independently of treatment group. No significant differences between responders and non-responders were observed in episodic memory, language, or processing speed. Among responders, the change in executive function score was not associated with the reduction in monthly moderate-severe headache days or the final number of monthly headache-free days.
Conclusions
Performance on measures of executive capacities, may improve in migraine patients after a few months of effective migraine treatment with mAbs or BoNT, regardless of the treatment group. Further research is needed to determine whether this effect augments over time, is associated to the reduction of pre-ictal and post-ictal days and /or to brain networks reorganization.
This is a visual representation of the abstract.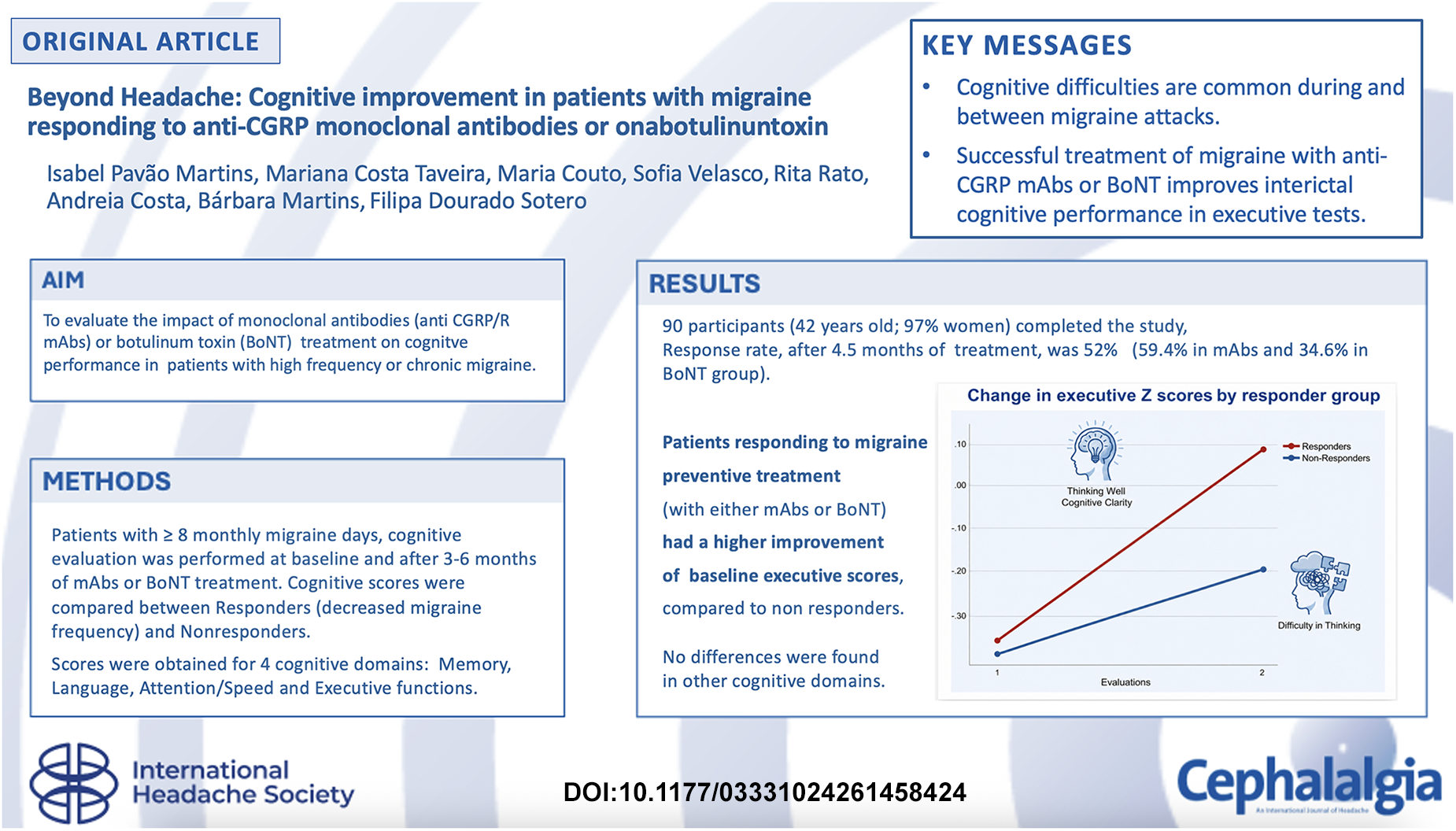
Introduction
Migraine is a complex brain network disorder characterized by recurrent attacks of headache, nausea, and intolerance to sensory stimuli. 1 It is increasingly conceptualized as a multisystem disorder 2 in which cognitive dysfunction represents a prominent and clinically relevant feature.3,4 During the attacks up to 89% of patients report impaired clarity of thought, characterized by reduced concentration, word-finding difficulties, and diminished multitasking capacity.5,6 Objective ictal neuropsychological assessments corroborate these subjective complaints, revealing significant impairments in attention, working memory, mental flexibility, and executive functioning. 7 Cognitive complaints are also frequently reported before (in the pre-ictal) and after the headache (post-ictal) phase, in spontaneous and experimentally induced migraine attacks, indicating that cognitive dysfunction extends beyond the most conspicuous symptoms of migraine.8,9 Interictal cognitive difficulties appear to be particularly common in chronic migraine, with up to 73% of patients reporting persistent cognitive complaints. These complaints are often associated with a poorer performance on cognitive tests compared with healthy controls or patients with episodic migraine, either in specific domains or in global cognitive function.10–13 Such findings substantially contribute to the interictal disease burden 14 and have raised concerns regarding a potential increased long-term risk of cognitive decline or dementia in this population.15,16 The mechanisms underlying these interictal difficulties are probably multifactorial and may involve changes in brain structure, function and connectivity, as well as processes related to accelerated brain ageing.17–21 Additionally, the cumulative effect of preventive medications, 13 medication overuse, 22 depression, 23 and other migraine comorbidities 24 may further increase cognitive symptoms.
The impact of migraine and its debilitating symptoms has been improved, over the past decade, by major advances in the understanding of migraine pathophysiology. They have led to the development of mechanism-based therapies targeting calcitonin gene-related peptide (CGRP) or its receptor, notably monoclonal antibodies (mAbs) and small-molecule CGRP receptor antagonists (gepants). These agents primarily modulate the trigeminovascular system, a key pathway in migraine pathogenesis. Clinical trials and real-world studies have consistently demonstrated their efficacy in reducing the frequency and impact of migraine attacks, as well as the need for acute medication. 25 Moreover, they have been associated with improvements in non-headache migraine-related symptoms, such as depressive symptoms and sleep disturbances. 26 Likewise, treatment with botulinum toxin (BoNT), which acts on peripheral nerve fibres, has been shown to reduce attack frequency and severity and to improve depressive symptoms in patients with chronic migraine. 27
Despite the well-established clinical efficacy of these treatments, their potential effects on cognitive functioning remain largely unexplored. Most available studies have relied on screening cognitive tools or reaction-time paradigms, providing limited insight into domain-specific cognitive changes and leaving the impact of preventive treatments on high order cognitive functions largely unknown.28,29
The present study aimed to evaluate whether treatment with anti-CGRP mAbs or BoNT is associated with a change in objective cognitive functioning. Based on the available evidence28,29 we hypothesized that patients who respond to treatment would show improvements in cognitive performance - particularly in executive functioning and processing speed, which are the domains most frequently affected during 7 or in-between the attacks.10–13 To address this question, we evaluated interictal cognitive performance in patients with migraine using a comprehensive neuropsychological battery targeting four cognitive domains, before and 3–6 months after treatment, and compared changes in performance between treatment responders and nonresponders.
Methods
Study design
The study was an observational, clinically based, two-center cohort study of patients with migraine initiating preventive treatment with mAbs or BoNT. The primary outcome was the effect of treatment response on changes of cognitive performance over time. This study is reported in accordance with the
Participants
Consecutive patients with migraine attending the headache outpatient clinics of two University Hospitals were invited to participate. Recruitment took place over 18 months, between October 2023 and March 2025.
Inclusion criteria were: a) episodic (EM) or chronic migraine (CM), diagnosed according to the ICHD third edition (ICHD-3) criteria (1), by the attending neurologist; b) age ≥18 years; c) more than four years of formal education; d) age at migraine onset <50 years of age; e) an average of ≥8 monthly migraine days during the previous three months, which is the minimum number of attacks required to initiate anti-CGRP mAb treatment, according to the National recommendations 30 ; and f) initiation of anti-CGRP mAbs or BoNT treatment due to failure (lack of response, contraindications or intolerance) to oral preventive medication. Patients were excluded if they were pregnant or willing to get pregnant in the following 12 months, had a known diagnosis of cognitive impairment of any cause, were participating in a clinical trial, had a previous diagnosis of major mental disorder (schizophrenia or major depression), or had a history of substance abuse. After providing written informed consent, patients were enrolled in the study.
The decision regarding the type of treatment was based on clinical judgment and local and international recommendations, namely the those of the National Headache Society 30 : a) for BoNT: CM (≥15 monthly headache days, eight of which with migraine features in the baseline period) and lack of response, contraindication or adverse events to oral treatments; b) for anti-CGRP mAbs treatment, a minimum of eight monthly headache days, or four-to-eight days with significant disability, and failure, contraindication or adverse events to oral treatment (including BoNT in the case of CM). Patients receiving anti-CGRP mAbs were treated with monthly subcutaneous injections of fremanezumab 225 mg, galcanezumab (a loading dose of 240 mg followed by monthly subcutaneous injections of 120 mg), or erenumab 140 mg. BoNT treatment consisted of 155–195 units administered every three months, following the PREEMPT protocol. 31 Patients receiving stable doses of oral preventive medication before baseline were allowed to continue their regimen throughout the study period unless safety concerns warranted treatment changes. This approach was intended to isolate the potential cognitive effects of newly initiated preventive medication while avoiding possible cognitive confounding due to discontinuation of previous medications.
Procedures
Patients underwent two cognitive assessment sessions scheduled to coincide with outpatient visits, and according to patient convenience: a baseline visit (visit 1) at the time of treatment initiation and a follow-up visit (visit 2) between three and six months after treatment initiation.
Sample size estimation was calculated from previous reports 28 showing significant improvement in computerized reaction time and working memory speed following BoNT treatment in patients with chronic migraine, with a sample size of 60 patients. Assuming a small-to-moderate effect size (Cohen's d = 0.4–0.5), a two-sided alpha level of 0.05, and 80% statistical power for paired comparisons, the required sample size was estimated at 34–52 patients. To account for potential missing data and dropouts, the target sample size was increased to 100 patients.
Patients were instructed to keep a headache diary and to record headache days, their severity, and acute treatment intake. Monthly headache days (MHD) and monthly moderate-to severe-headache (MMSH) were averaged over the three months preceding each assessment. Patients were classified as treatment responders if MMSH days decreased by ≥30% in patients with CM or by ≥50% in those with EM between baseline and the second visit. A less stringent criteria was used for CM because treatment response rates to anti-CGRP mAbs are usually lower in CM than in EM,32,33 and this threshold has been accepted by International Headache Society recommendations for clinical trials in chronic migraine. 34
Materials
In addition to current age, sex and age at migraine onset, the following clinical variables were collected at baseline and follow-up visits: diagnosis (EM or CM), MHD and MMSH, medication overuse (yes/no) according to the ICHD-3 criteria, 1 ongoing preventive medication, and the number of previous preventive treatment failures (either oral preventives, BoNT or anti-CGRP mAbs). Patients completed standardized scales assessing migraine impact, including the Headache Impact test (HIT-6) 35 and Headache-Attributed Lost Time (HALT), 36 anxiety and depressive symptoms using the Hospital Anxiety and Depression scale (HADS). 37 Subjective cognitive complaints were assessed using the subjective cognitive complains scale (SCC). 38
Cognitive assessments were conducted outside migraine attacks by trained neuropsychologists who were blind to treatment group and responder status. The neuropsychology battery consisted of the Portuguese versions of 11 standardized tests covering four cognitive domains:
Episodic memory: Rey Auditory Verbal learning test (RAVLT),39,40 which evaluates the learning of a list of unrelated words across multiple trials. Scores included immediate recall (RAVLT-1), learning (sum of five learning trials, RAVLT-1 to RAVLT-5), delayed recall (RAVLT-7), long term percent retention (LTPR) which is the delayed recall expressed as a proportion of the last learning trial, and recognition. To minimize learning effects between assessments, an alternative version (with different items but comparable difficulty) was used on the second evaluation. Language: semantic fluency for animals,
41
which measures the ability to retrieve names of animals within a fixed time (60 s). Attention and processing speed were assessed using the digit symbol coding from Wechsler adult intelligence scale (WAIS),
42
that measures the number of conversions of symbols into digits, in a fixed period of time; the Trail Making Test part A (TMT-A), that measures the time required to sequentially connect randomly arranged numbers43,44; and digit span forward,
42
which measures attention and immediate memory through the highest series of digits correctly repeated. Executive functions: Trail Making Test part B (TMT-B), assessing divided and alternating attention by measuring the time required to connect numbers and letters in alternating sequence43,44; digit span backwards, a measure of working memory based on the maximum number of digits repeated in the reverse order,
42
and phonemic fluency for the letter, assessing verbal initiative and mental control (ability to self-generate words according to a phonological rule and without repetitions).
41
Raw scores obtained on each measure were converted into standardized z- scores, adjusted for age and education. Four domain scores representing each cognitive domain were computed from the standardized scores of the corresponding tests: an executive score (including working memory, alternating attention and verbal initiative and mental control), an episodic memory score (including total list learning and long-term percent retention), a score of attention and processing speed (immediate memory, digit symbol and TMT-A), and language score (including semantic fluency). These scores were compared between baseline and follow-up evaluations to assess treatment-associated cognitive changes.
The study was conducted in accordance with the ethical principles of the Declaration of Helsinki. All patients provided written informed consent before study participation. The study protocol was approved by the Ethics Committee of both participating institutions. This study is reported in accordance with the STROBE guidelines for observational studies.
Statistical analysis
Baseline demographic, clinical and cognitive variables were computed for all participants and stratified by treatment response (responders and non-responders). Continuous variables were described using medians and interquartile ranges, and categorical variables were presented as counts and percentages. Baseline differences by responder status were evaluated using Chi-square test or Mann and Whitney test for categorical or continuous variables, respectively. Improvement on a scale or cognitive measure was defined as a better performance at the second evaluation relative to baseline.
Baseline cognitive scores were correlated with subjective cognitive complaints score, and with migraine variables (headache-free days, and monthly moderate-to-severe headache days) using Spearman correlation coefficients. These analyses aimed to assess the relationship between subjective and objective cognition and between migraine load and cognition. Change in each cognitive domain score, between the first and the second evaluations, was analysed using repeated measures mixed-effects models, with the first and second cognitive scores included as within-subjects variables and treatment response (responder/non-responder) as between-subject variables. Treatment group (mAbs or BoNT) and any variables showing significant baseline differences between responder groups, were entered in the model as covariates. To understand the impact of headache improvement on cognition, the differences between the second and the first cognitive z-scores per domain were correlated with the reduction in the number of MMSH and with the number of headache-free days (a variable computed by subtracting the total number of headache days on the second evaluation from 30). Statistical significance was defined as a two-sided alpha level of 0.05. Statistical analyses were performed using IBM SPSS Statistics, V.28.
Results
A total of 100 patients was enrolled, of whom 90 completed the study protocol. Loss to follow-up was primarily due to scheduling difficulties preventing completion of the cognitive assessment within the predefined time window (n = 7). Additional reasons included the development of a new medical condition (n = 1) and failure to initiate treatment after baseline because of travel or clinical improvement (n = 2).
Participants’ demographic and clinical data at baseline are summarized in Table 1. Participants had an average age of 42 years, and 96.7% were females. Fifty-eight (64.4%) had CM, 32 had EM (35.6%). Sixty-four (71.1%) were treated with anti-CGRP mAbs, and 26 (28.8%) with BoNT.
Baseline data of the total sample.
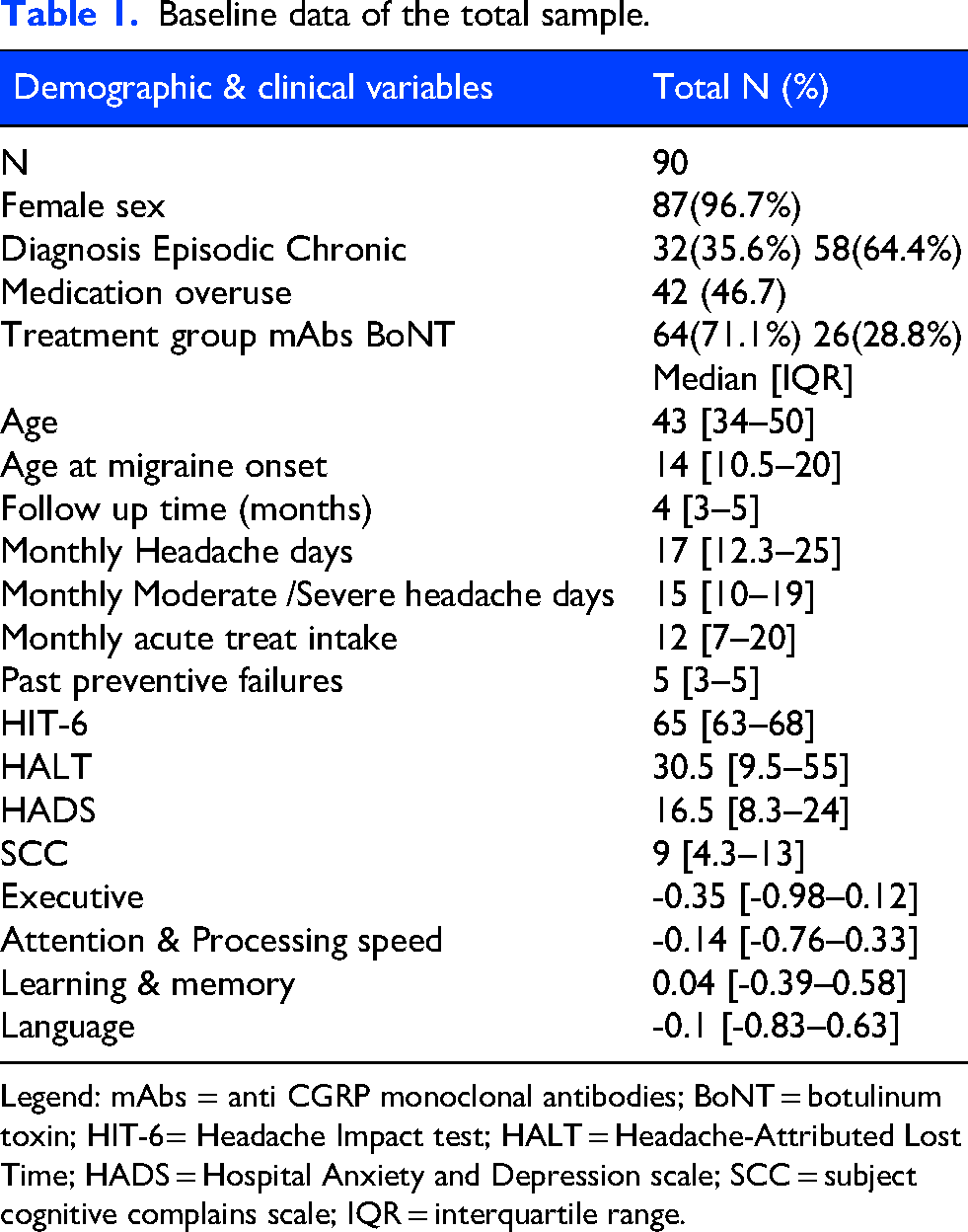
Legend: mAbs = anti CGRP monoclonal antibodies; BoNT = botulinum toxin; HIT-6= Headache Impact test; HALT = Headache-Attributed Lost Time; HADS = Hospital Anxiety and Depression scale; SCC = subject cognitive complains scale; IQR = interquartile range.
Overall, 47 participants (52.2%) were classified as responders after a mean follow-up time of 4.5 months. The proportion of responders was significantly higher in the mAbs group (59.4%) than in the BoNT group (34.6%). Patients who did not respond to treatment had a significantly higher baseline HALT score. Although they also presented higher baseline values for MHD, MMSH days, HIT-6, and cognitive complaints scores, the differences were not statistically significant. Participants’ average score on the cognitive complaints scale was 9.03 ± 5.88, which is above the cutoff score for healthy individuals (≤5). Baseline data according to responder category is presented in Table 2.
Baseline demographic, clinical and cognitive scores per responder group.
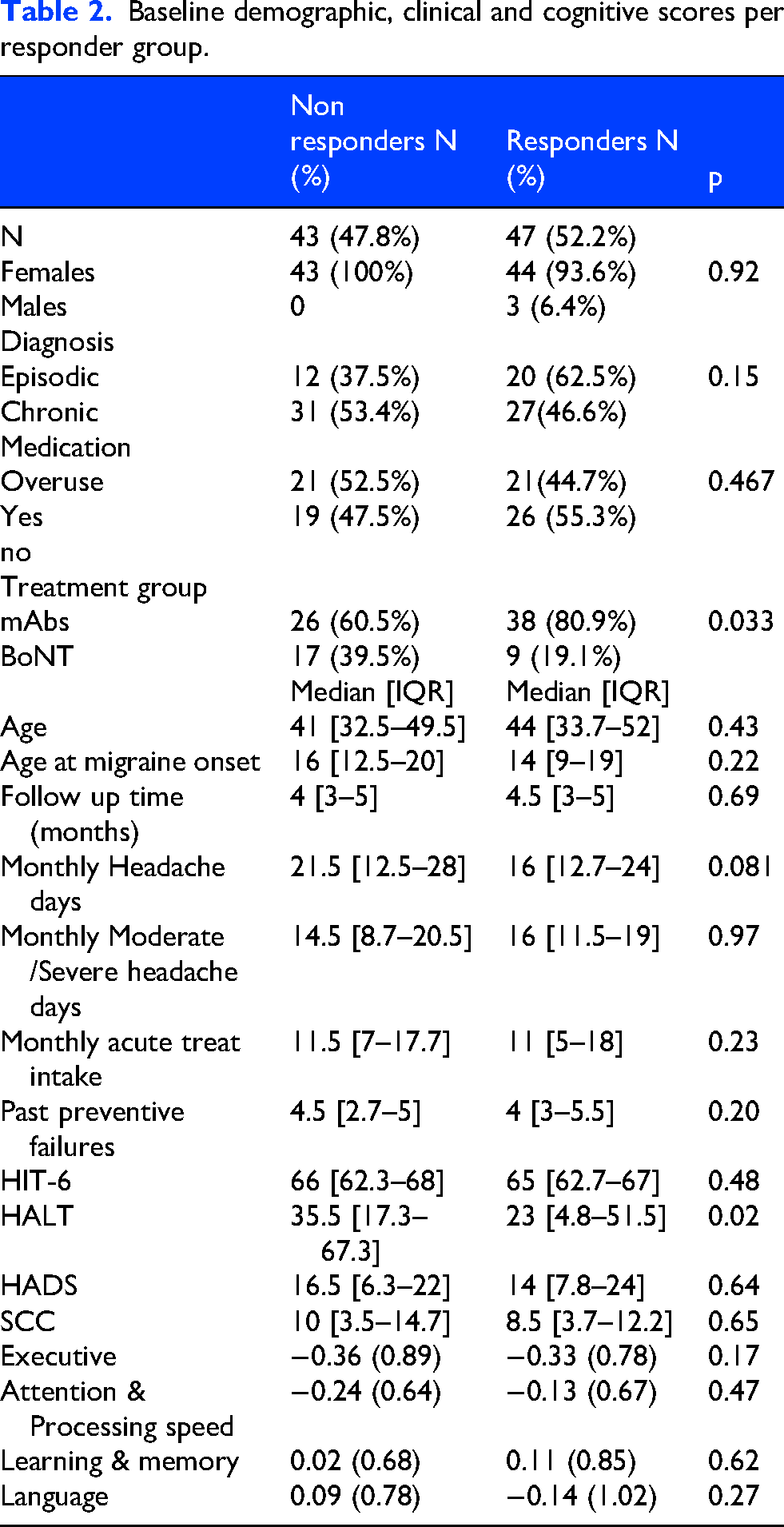
Baseline scores across the four cognitive domains were similar between responders and non-responders (Table 2). In addition, there were no significant correlations, at baseline, between the number of headache-free days, or of MMSH, and any of the four cognitive domain scores, neither between subjective cognitive complains and the objective performance in any domain (Spearman rho=0.07 for language, −0.17 for attention, −0.09 for executive functions and 0.02 for memory).
At the second evaluation, the average change in monthly moderate-to-severe headache days was of 11.2 days (median=11; IQR 8–13; 95% CI 8.7 to 13.7) in responders whereas non-responders showed a reduction of 1.6 days (median=1; IQR −2 to 5; 95% CI −0.68 to 3.9) (t = -5.75; p < 0.001). The number of monthly headache-free days at follow-up was 24.9 days among responders (median=26; IQR 22–27; 95% CI 23.9 to 25.9) and 12.1 days among non-responders (median=15; IQR 2–18; 95% CI 9.18 to 14.96).
Average scores per cognitive domain at baseline and at second evaluation, in responders and non responders, are displayed in Table 3.
Baseline and final cognitive scores (mean and standard deviation) per responder group.
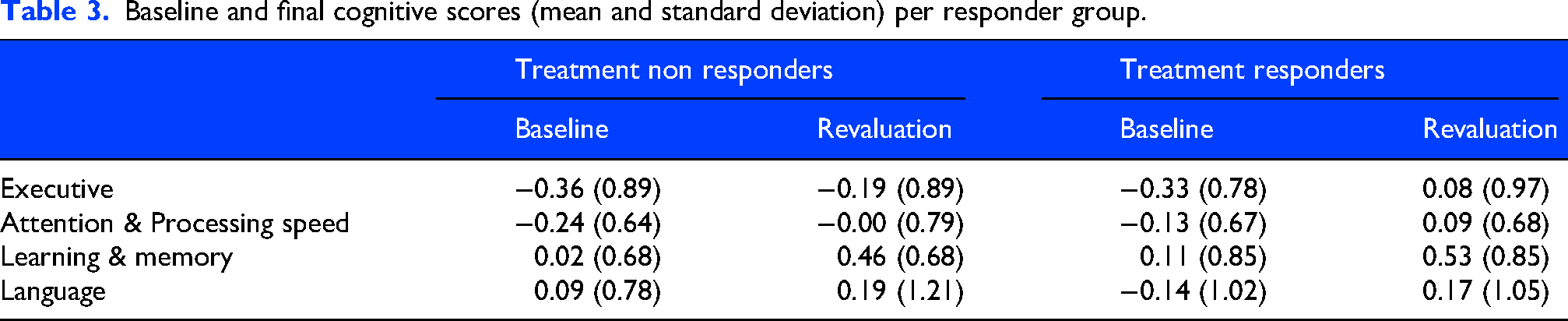
Repeated-measures analyses showed a significant within-subjects change (improvement) across the two evaluations in all domains: executive function (mean difference −0.29, 95%CI −0.42 to −0.18, p < 0.001), processing speed (mean difference −0.23, 95%CI −0.33 to −0.13, p < 0.001), language (mean difference −0.21, 95%CI −0.30 to −0.03, p = 0.01) and memory scores (mean difference −0.43, 95%CI −0.59 to −0.27, p=<0.001).
There was a statistically significant time by treatment responder interaction for the executive measures (Table 4). Responders showed a greater improvement in the executive score (average change=0.41 ± 0.55) compared with non-responders (average change=0.17 ± 0.55). No significant interactions were observed for the other cognitive measures. There was no significant interaction between time and treatment group (mAbs or BoNT) for any of the cognitive domain scores.
Time lag per domain with treatment and in responders.
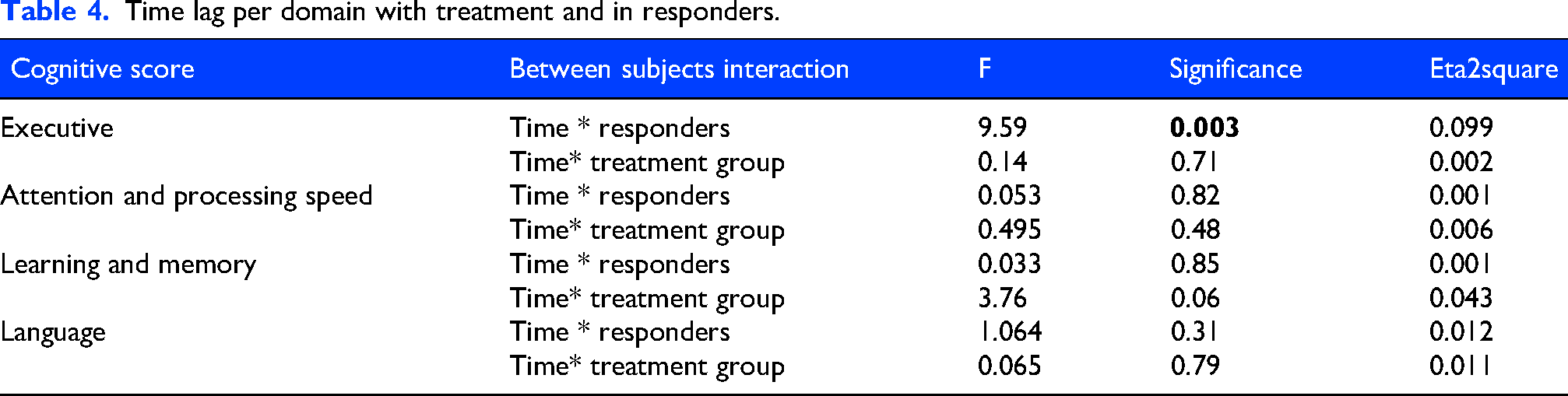
Among responders, improvements in executive scores (the difference between the second and the first executive score) were not correlated with either the reduction in MMSH (Spearman rho=0.18, n.s.) or the number of headache-free days at the second visit (Spearman rho=0.09, n.s).
Discussion
In this study we aimed to evaluate whether preventive migraine treatment, with mAbs or BoNT, had an impact on patients’ cognitive performance, with the hypothesis that treatment response would be associated with an improvement in executive and processing speed abilities. Our findings showed that an effective improvement in migraine frequency was associated with an enhanced interictal performance in executive function measures, compared with patients who did not respond to treatment. To our knowledge, this is the first prospective study using a comprehensive neuropsychological battery, to measure cognitive changes, across multiple domains, related to preventive treatment with BoNT and mAbs in migraine.
These findings are clinically relevant for three reasons. Firstly, they show that adequate control of migraine attacks may reverse cognitive difficulties in patients with high frequency episodic and chronic migraine, suggesting that treatment may also ameliorate another disabling dimension of the migraine spectrum. Secondly, this improvement was observed between three and six months after treatment initiation, offering practical guidance when counselling patients who report prominent cognitive complaints. And finally, because the participants included in this study are representative of the typical patients with migraine that are candidates to advanced migraine treatments. They had a high frequency of attacks, with a median of 17 monthly headache days, they were resistant to oral preventive treatments, had a high percentage of medication overuse and had other associated symptoms.
Among those symptoms were multiple cognitive complaints, exceeding the cutoff used to consider such complaints clinically significant. This finding indicates that patients were aware of cognitive difficulties. Yet the latter did not correlate with the scores obtained on cognitive tests. This suggests that patients’ perception of their cognitive functioning may not directly reflect their actual cognitive performance. This discrepancy is plausible since cognitive performance depends upon many different factors, namely the degree of education, occupational and daily activities demand, age, sleep quality, diet and emotional state, among others. Cognitive complaints may therefore reflect the additional effort patients require to accomplish the same tasks, or the perception of decline relative to their expected or previous abilities. Subjective cognitive complaints do also capture aspects of migraine interictal burden that are not fully reflected by objective testing even controlling for depressive symptoms. 14
At the second cognitive evaluation, it was found that most cognitive measures improved when compared to the baseline, which may be consistent with a learning effect, since participants may become more familiar with testing procedures and remember some tests. Score improvement was observed in all domains, including in the memory score, which was the only test that used a standardized alternative version at the second evaluation. This learning opportunity was identical, both in tests and time intervals, between responders and non-responders, yet a significant improvement in executive function measures was only observed among responders, supporting the interpretation that it reflects a true therapeutic effect rather than solely a practice or learning effect. Interestingly, executive abilities have been shown to decline during acute migraine attacks 6 and to be significantly reduced interictally in subjects with chronic migraine when compared to control populations.10,11 The executive measures used in this study include several processes such as working memory, verbal initiative, mental control and divided and alternating attention that have been related to the functioning of the frontal lobes. The degree of executive improvement was not correlated with the final number of headache free days, or the change in moderate to severe headache days and may reflect broader changes associated with migraine improvement rather than a strictly linear relationship with reductions in headache frequency. There were no significant differences in other cognitive domains namely in memory and language, between responders and non-responders.
Contrary to our initial hypothesis there was no significant improvement in attention and processing speed. These are broad cognitive functions that have been reported to improve in patients treated with BoNT, when evaluated with computerized reaction-time tests. 28 It may be necessary to use more sensitive or fine-grained measures of cognitive speed, such as computerized tests, to find a difference in these domains.
The disparity of cognitive improvement by domain is difficult to interpret and raises questions about the mechanisms underlying cognitive dysfunction or cognitive recovery in this disorder. Migraine, as much as other disorders of the brain, like epilepsy or multiple sclerosis, involves neural circuits that overlap with those supporting cognitive functions, making it plausible that the disease may also have an impact in cognition. In fact, brain imaging studies have shown that migraine patients, especially with chronic migraine, exhibit functional and connectivity changes, including reduced functional connectivity between the default mode network and the visuo-spatial system and reduced thalamic activity.19,20 Structural brain changes have also been reported, including cortical atrophy, reduced volume of thalamic nuclei,17,45,46 or even neurodegeneration, with iron deposition. 18 These data support the hypothesis of an evolving process that affects brain networks and could eventually influence cognitive performance and increase the risk of dementia. 15 The involvement of thalamic nuclei is of special interest since they have reciprocal connections with the frontal lobes, which could help explain changes in executive functioning.
Both anti-CGRP mAbs and BoNT are known to act predominantly outside the central nervous system. However, both have been associated with central effects, namely improvements in depression and sleep.26,27 Moreover, migraine improvement with erenumab has been associated with a reorganization of resting-state functional connectivity, as early as eight to twelve weeks after treatment initiation, whereas no such changes were observed in non-responders’ group,47,48 an effect that may be specific for the target of anti-CGRP mAbs. 49 Another study reported a decrease in iron deposition in the subcortical regions after anti-CGRP mAbs treatment. 50 These observations prompt consideration of potential central effects of anti-CGRP mAbs that might account for cognitive improvement. Nevertheless, comparable cognitive changes were also observed, in our study, in patients treated with BoNT, arguing against a mechanism exclusively attributable to central actions of mAbs. This suggests that the cognitive benefit may primarily reflect a better migraine control rather than a drug-specific mechanism.
Recent studies have also postulated that migraine may be associated with accelerated brain ageing, reflected by an increased brain-age gap, in particular in chronic migraine. 21 This hypothesis is relevant for the present data, since most cognitive processes associated with brain aging fall within the executive abilities (inhibition of irrelevant information, coordination of multiple simultaneous operations, manipulation of information within working memory, and control of memory operations). 51 These functions are impaired in chronic migraine and improved in the responder group in our study. A functional imaging study evaluating migraine patients during a working memory task (N-back task) showed that they exhibit a significantly greater activation in the left frontal pole and orbitofrontal cortex during the ictal period that may possibly translate the recruitment of inhibitory or compensatory networks to maintain task performance. 52 A similar strategy was described in healthy elderly individuals when performing some executive tasks. 53 Some authors hypothesize that the abnormal patterns of connectivity found in migraine may represent maladaptive plasticity processes secondary to chronic or repeated pain.54,55 As such, they could be liable to reorganization as migraine improves, unlocking the abnormal patterns of connectivity. In this perspective, effective treatment of chronic or high-frequency episodic migraine may improve the efficiency of the network associated with executive functions. Future studies combining cognitive assessment with functional connectivity measures could help address this alternative hypothesis or clarify the involved mechanisms.
The present results suggest that cognitive improvement is related to the improvement of migraine per se, since the effect was only observed in treatment responders and the lack of differences between treatment groups. This interpretation is supported despite the lack of a linear association between decrease in headache days or the total number of headache-free days and cognitive performance. A similar effect was demonstrated in patients responding to oral preventive medication. 56 It is also worth considering that cognitive symptoms are often part of migraine prodromes and postdromes. As migraine attacks become very frequent, with short interictal intervals, patients may enter a near-continuous state of brain dysfunction, with persistent cognitive changes that do not recover between attacks. As treatment widens the interictal periods, these cognitive alterations may progressively improve.
We acknowledge some limitations to this study, namely the short period of follow-up that may not have allowed the patients to have a more complete benefit of treatment. Our intention was to minimize attrition while aligning with the follow-up periods used in pivotal clinical trials with anti-CGRP mAbs. BoNT treatment is also associated with a main improvement within the first three months of treatment, although further benefit may occur with subsequent sessions. Although the study reached the estimated sample size, we acknowledge that treatment groups were relatively small, especially those receiving BoNT. Other limitations concern the selection of cognitive tests used. While the episodic memory test had an alternative version to preclude learning effects, to our knowledge, the other tests do not have validated alternative versions. We therefore repeated the same version at both sessions rather than using a similar but unvalidated versions. Although this may have introduced a learning effect, the comparison between responders and non-responders somehow controls for this learning opportunity.
In conclusion, adults with frequent or chronic, treatment-resistant migraine and significant cognitive complaints showed measurable improvement in executive functioning after approximately 4.5 months of sustained migraine control. These data support the view that migraine-related cognitive dysfunction is not necessarily permanent, but rather a dynamic and potentially reversible component of disease burden that parallels clinical response to preventive therapy.
Clinical Implications
Individuals with migraine frequently report cognitive difficulties during and between attacks
Cognitive symptoms contribute to migraine associated disability.
We found that effective migraine treatment, with monoclonal antibodies or botulinum toxin, improves performance in some cognitive tasks
Cognitive difficulties can be reversed with adequate migraine control
Footnotes
Acknowledgements
The authors would like to thank Dr Mariana Dias Costa (Serviço de Neurologia, Departamento de Neurociências e Saúde Mental, ULS Santa Maria, Lisboa) and Drs Beatriz Moutinho, Carolina Sousa and Ana Catarina Loureiro (Serviço de Neurologia, ULS São João, Porto) for their help in the inclusion of patients.
Ethical considerations
The study was conducted in accordance with the ethical principles of the Declaration of Helsinki. The study protocol was approved by the Ethics Committee of both participating institutions.
Author contributions
Isabel Pavão Martins: contributed to the conceptualization and design of the study, selection of patients, collecting and analysing data, writing the original draft and review the final version; Mariana Costa Taveira: contributed to collection, organization and verification of data, review the final version of the manuscript; Maria Couto and Sofia Velasco: contributed to the design the cognitive battery and performed the neuropsychological evaluation and reviewed the final version; Rita Nunes Rato, Andreia Costa and Barbara Martins, contributed to the selection of patients, collecting data, and review of the final version of the manuscript; Filipa Dourado Sotero contributed to the conceptualization of the study, selection of patients, collecting and analysing data, and review the final version of the manuscript.
Consent to participate
All participants provided an institutional and ethics approved written consent.
Consent for publication
All authors agree to publish with Cephalalgia if the manuscript is accepted.
Data availability statement
The data provided in this article can be made available in fully anonymized form, upon appropriate request.
Declaration of conflicting interests
Isabel Pavão Martins—received honoraria for lecturing, consultancy, or participation in clinical trials from AbbVie, Allergan, Amgen, Eli Lilly, Lundbeck, Organon, Pfizer, Novartis, Teva and Zambon. Andreia Costa—received honoraria for lecturing, consultancy, or participation in clinical trials from AbbVie, Allergan, Eli Lilly, Lundbeck, Organon, Pfizer, Novartis and Teva. Filipa Dourado Sotero— received honoraria for lecturing, consultancy, or participation in clinical trials from AbbVie, Allergan and Lundbeck. Bárbara Martins—received honoraria for lecturing, educational support, or travel grants from AbbVie, Lundbeck, Organon, Eli Lilly and Teva. Maria Couto, Sofia Velasques Mariana Taveira and Rita Rato declare no conflicts of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.