
Abstract
Background
Low-glycaemic diet may alleviate migraine; however, individual blood glucose variability can affect efficacy. In this open-label randomised controlled trial in Germany, we assessed whether the digital therapeutic (DTx) sinCephalea, which delivers personalised low-glycaemic nutritional recommendations supported by intermittent continuous glucose monitoring (CGM), reduces migraine frequency compared with a design-matched control application.
Methods
This open-label trial in Germany assessed the DTx sinCephalea for migraine prevention. Adults aged 18–65 years with episodic migraine were randomised 1:1 (in addition to standard treatment) to the digital therapeutic (intervention) or a design-matched control application. Patients completed a daily headache and medication diary, and 4-weekly patient-reported outcome questionnaires. Adherence to nutritional recommendations was monitored. Primary endpoint (Week 12): change from baseline in monthly migraine days (every 4 weeks) for intervention versus control. Secondary endpoints: change from baseline in monthly migraine days in patients with ≥50% adherence to nutritional recommendations, 30% response rates, migraine- and headache-related impairment, quality-of-life, and acute medication use for intervention versus control. Adverse events were recorded.
Results
842 patients were randomised between July 2021 and August 2023 (full analysis set: intervention = 416; control = 419). There were significantly greater reductions in monthly migraine days at week 12 for intervention versus control (mean [SD] change: 1.7 [3.4] versus 1.2 [3.2] days; between-group difference estimate: −0.53 [95% CI −0.98 to −0.09]; p = 0.0195) with similar monthly migraine days reductions observed in adherent patients (p = 0.0062; adjusted α = 0.05). Response rate was 54.9% (185/337) in intervention versus 42.9% (168/392) in control (odds ratio: 1.63 [95% CI 1.21–2.19]; p = 0.0012; adjusted α = 0.0125). Migraine- and headache-related impairment were lower at week 12 for intervention versus control (p = 0.0247, adjusted α = 0.0167and p = 0.0001, adjusted α = 0.01, respectively). There was no significant difference in quality-of-life or acute medication use and no digital therapeutic-related adverse events.
Conclusion
Personalised nutrition, supported by intermittent CGM, via the DTx sinCephalea, was efficacious for migraine prevention without DTx-related adverse events. This study provides evidence in support of the link between diet and migraine frequency and symptoms. Additionally, as this is a non-pharmacological treatment with no DTx-related side effects, it may be an attractive option for patients. DTx could also reduce the burden of migraine on healthcare systems by providing a scalable, remote, non-invasive and convenient treatment option.
Keywords
Introduction
Personalised nutrition, supported by continuous glucose monitoring (CGM), has shown promise in tailoring dietary advice for people with a variety of disorders, including diabetes and migraine.1,2 Migraine affects an estimated 14% of the global population, and is one of the main causes of disability worldwide. 3 Despite available guideline-based therapies, a substantial proportion of patients with migraine who qualify for preventive treatment do not receive it - and among those who are prescribed preventive medication, long-term adherence is often suboptimal due to insufficient efficacy, side effects, or complex dosing regimens, leaving many patients with inadequately controlled migraine. 4 Various dietary patterns and triggers have been explored for migraine prevention to varying success. 5 Current research suggests a potential role for blood glucose in migraine, as patients with migraine may have higher mean glucose values compared with healthy people, 1 and migraine attacks are associated with fluctuations in blood glucose level. 6 Furthermore, reducing the brain's glucose energy source with a ketogenic diet has been shown to alleviate migraine frequency and severity. 7 Technologies that utilise CGM as a tool to monitor and help stabilise blood glucose may therefore have a role in personalised nutrition for migraine prevention.
Digital therapeutics (DTx) are therapeutic interventions driven by software aimed at treating a disease. They include medical devices or phone applications (apps) that can help patients enhance their diet with personalised nutrition, provide recommendations for lifestyle modifications, and improve adherence to medication.1,8 Furthermore, DTx may reduce healthcare costs compared with standard of care alone through the reduced costs associated with self-monitoring as well as reduced resource use. 9 Germany has been at the forefront of digital health innovation with the introduction of the Act to Improve Healthcare Provision through Digitalisation and Innovation (Digital Healthcare Act-DVG) in 2019. 10
sinCephalea is a DTx app designed to provide individualised migraine prevention, including recommending a personalised low-glycaemic diet, supported by short-term use of CGM (10–14 days at baseline) To our knowledge, no other DTx intervention for migraine to date has utilised CGM to inform nutritional recommendations. 8 Previous proof-of-concept prospective and retrospective studies have demonstrated reductions in migraine frequency and attack duration with sinCephalea. 1 The present large randomised controlled trial was conducted to evaluate the efficacy of sinCephalea compared with a design-matched control app, each in addition to standard treatment, in patients with episodic migraine.
Methods
Study design
The study used a randomised, open-label, controlled design comparing the DTx sinCephalea with a design-matched control app, each in addition to standard treatment (Figure 1). Both groups completed a daily headache diary and regular patient-reported outcome (PRO) assessments. The study visits were conducted tele-medically by investigators at the Centre of Excellence for Inflammation Medicine at the University Medical Centre Schleswig-Holstein Campus Lübeck, Germany. The protocol has been previously published. 11 The study was approved by the Ethics Committee of the University of Lübeck (January 19, 2021, file number 20–285) and was registered with the DRKS (March 8, 2021, DRKS-ID:DRKS00024657). Written informed consent was obtained from all patients prior to individual study onset.
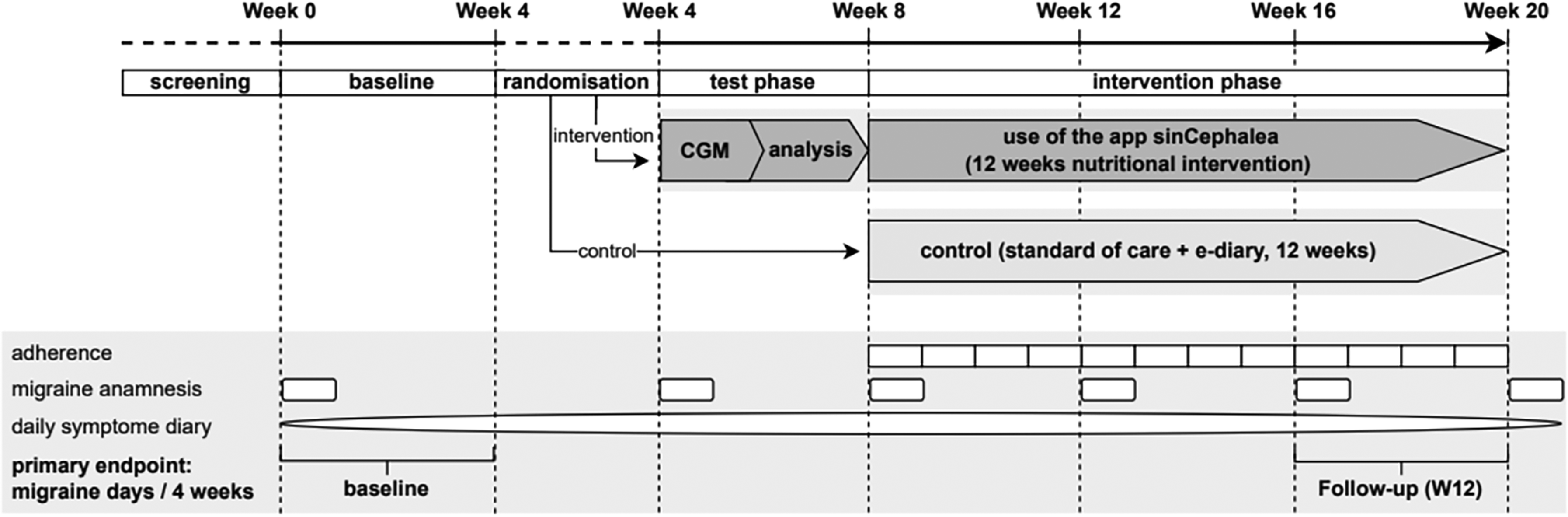
Study design.
Both arms comprised an equal 12-week intervention or control period; however, the total study duration was four weeks longer for the intervention arm due to the CGM phase (including kit shipment and sensor wear). Consequently, ‘Week 12’ refers throughout to week 12 of the respective intervention or control period - corresponding to absolute study week 16 for the control arm and absolute week 20 for the intervention arm (as illustrated in Figure 1) - and not to a shared calendar timepoint after randomisation.
Participants
Patients were recruited via digital channels, flyers, and notices. Adults aged 18–65 years with a clinically confirmed diagnosis of migraine (with or without aura) were eligible for enrolment (diagnosis 1.1 and 1.2 of the International Classification of Headache Disorders [ICHD-3]). 12 Diagnosis was confirmed by a trained study physician at the telemedical enrolment visit using a standardised assessment based on ICHD-3 criteria, comprising a structured neurological history and a systematic review of headache characteristics (location, quality, severity, duration, and associated symptoms including nausea, photophobia, phonophobia, and aura). Patients with atypical features or focal neurological deficits not consistent with migraine were excluded at the investigator's discretion. Eligible patients had a diagnosis of episodic migraine (fewer than 15 migraine days a month in accordance with the International Headache Society [IHS] Classification ICHD-3), had a self-reported history of ≥3 migraine days per 4 weeks (confirmed prospectively during the 4-week baseline phase using the electronic daily headache diary), were able to distinguish their migraine attacks from other headache types, as assessed by the study physician during the enrolment visit based on phenotypic attack characteristics consistent with ICHD-3 criteria, and had experienced migraine before aged 50 years for ≥12 months. Patients also had sufficient German language skills to understand the study document and owned a compatible smartphone.
Patients were excluded if they had used another Perfood product with CGM analysis in the past 24 months; were pregnant or breastfeeding; had chronic migraine (ICHD-3 diagnosis 1.3), 12 or complicated migraine with debilitating (e.g., hemiplegic) and/or long-lasting auras after a migraine cerebral infarction; had evidence of another headache type (tension headache was not excluded if it accounted for <50% of headache days per 4 weeks in the last 3 months and there was an indication for migraine prevention medication due to the symptoms); had changed migraine prevention medication in the past 12 weeks; had used an alternative migraine app in the past 12 weeks; were on ≥2 migraine prevention drugs; had received non-drug treatment with acupuncture; had a malignant disease diagnosis in the past 3 years; had insulin-treated diabetes; had a psychiatric illness (other than stably treated depression) requiring pharmacological treatment, or had required inpatient psychiatric treatment, within the past 12 weeks; suffered from eating disorders (binge-eating disorder, anorexia nervosa, or bulimia nervosa), chronic pain syndrome, or addiction; or were participating in other clinical trials.
Concomitant preventive treatments were allowed if stable for at least 12 weeks before enrolment. No dosage adjustments of any preventive medication were permitted during the trial.
Randomisation and masking
All patients initially entered a 4-week baseline phase to assess the severity of disease. Eligible patients were then randomised 1:1 centrally into two groups: the DTx (sinCephalea) group and the control app group. Permuted block randomisation was applied with stratification by sex (female/male) and number of migraine headache days in the last 4 weeks (<8 versus ≥8 days). Block sizes of 4 and 6 were used, stratified by sex and baseline migraine frequency.
Procedures and assessments
The study compared the DTx sinCephalea (intervention app) with a design-matched control app. Both apps shared an identical visual design and user interface, a daily electronic headache diary (recording migraine attacks, symptoms, and acute medication use in accordance with IHS guidelines), and 4-weekly PRO questionnaires (HIT-6, MIDAS, and EQ-5D-5L; PGIC at Week 12 only). The intervention app additionally provided: a CGM-integrated food diary and glucose monitoring functionality during the pre-intervention CGM phase; personalised low-glycaemic nutritional recommendations generated from the individual glucose response profile; educational content on migraine, nutritional principles, stress management, and sleep hygiene; and a weekly self-report questionnaire on adherence to nutritional recommendations. The control app did not include any personalised recommendations, educational content, CGM functionality, or adherence questionnaire. Each group continued to receive their standard treatments for migraine throughout the whole study.
The design-matched control app was chosen as the most appropriate and practically feasible comparator for this multicomponent DTx. True participant blinding is not achievable in personalised digital interventions and the chosen design with identical interface, daily diary, and PRO assessments in both arms controls for non-specific effects of app use while isolating the contribution of the personalised CGM-based recommendations.
The CGM phase was conducted exclusively in the intervention arm, following the 4-week baseline phase and prior to the start of the 12-week nutritional intervention. Participants received a CGM sensor kit by post and wore the sensor for a minimum of 10 days (maximum 14 days), using either the FreeStyle Libre 3 (Abbott Laboratories, Abbott Park, IL, USA) or the Dexcom G7 (Dexcom Inc., San Diego, CA, USA), depending on availability and patients’ choice. During this phase, participants recorded their food intake in the sinCephalea food diary while the sensor captured CGM data. These data were analysed by the sinCephalea algorithm to determine each participant's individual postprandial glucose response profile, on the basis of which personalised low-glycaemic nutritional recommendations were generated and delivered via the app. CGM was not used during the subsequent 12-week intervention or control period in either group. The complete study timeline is illustrated in Figure 1. The following PROs were assessed in each group: Headache Impact Test 6 item (HIT-6) to record migraine-related impairment in everyday life (total score 36–78; ≥60 indicates severe impact) 13 ; Migraine Disability Assessment (MIDAS) to record headache-related impairment (total score 0–465) 14 ; 5-level EuroQol 5-dimensional questionnaire (EQ-5D-5L) to assess patient's health status and quality-of-life (utility index −0.205 to 1.000) 15 ; and Patient Global Impression of Change (PGIC) to record patient assessment of change in overall health status (7-point scale, 1 = very much improved to 7 = very much worse). 16 HIT-6, MIDAS, and EQ-5D-5L were assessed every 4 weeks; and PGIC was assessed at Week 12. Headache and migraine attacks, as well as use of acute migraine medication, were collected via the daily electronic headache diary. 17 Adherence to the personalised nutritional recommendations was assessed via a brief weekly self-report questionnaire embedded in the sinCephalea app. Participants were asked how often they had followed their personalised nutritional recommendations during the preceding seven days. Participants who reported following the recommendations on ≥50% of occasions assessed were classified as adherent, in accordance with the pre-specified threshold defined in the statistical analysis plan.
Adverse events (AEs) and serious adverse events (SAEs) were recorded throughout the study and at the final visit. The study investigator classified each AE and SAE according to whether it was related to the DTx; SAEs were immediately reported to the medical monitor at Perfood for medical review. The medical monitor reviewed the information on the AE alongside all available information on the patient.
Outcomes
The primary endpoint was the change from baseline in the number of monthly migraine days (MMD) per 4 weeks at Week 12 for DTx versus control. Migraine days were self-reported by participants via the daily electronic headache diary, recorded in accordance with IHS guidelines. 17
Secondary endpoints assessed DTx versus control over the last 4 weeks of the study (referred to as the Week 12 timepoint) and included: (i) change from baseline in MMD per 4 weeks in patients with ≥50% adherence to the nutritional recommendations; (ii) change from baseline in impairment in daily life due to headache (HIT-6); (iii) responder status (≥30% relative reduction in the number of migraine days per 4 weeks based on use of a non-pharmacological intervention); (iv) change from baseline in migraine-related impairment (MIDAS); (v) change from baseline in number of days of acute migraine medication use per 4 weeks based on acute medication use logged in the headache diary; and (vi) change from baseline in quality-of-life (EQ-5D-5L).
Prespecified exploratory endpoints included: (i) assessment of the primary endpoint for the first 4 weeks of the study (referred to as Week 4) and following 4 weeks (referred to as Week 8 timepoint) of treatment; (ii) difference in responder status (≥30% threshold) at Week 4 and 8 of treatment for DTx versus control; (iii) difference in responder status based on a ≥ 50% relative reduction in migraine days at Weeks, 4, 8, and 12 for DTx versus control; and (iv) patient assessment of health status, measured by PGIC, at Week 12 in the DTx and control groups. Post hoc analyses were also carried out to: (a) assess the primary endpoint in patients on preventative medicine compared with those not on preventative medicine; (b) assess the proportion of patients with at least one MIDAS grade improvement according to baseline MIDAS grade; and (c) determine the proportion of patients with an improved PGIC (very much improved, much improved, or minimally improved), no change in PGIC, or worsened PGIC (minimally worse, much worse, or very much worse) Likert scale at Week 12.
Statistical analysis
The sample size calculation aimed to detect a mean change from baseline in the number of migraine days at Week 12 for DTx versus control of 2.07 in the DTx group and 1.19 in the control group with a standard deviation (SD) of 3.64 days (estimated from studies with patients in control group aware of their allocation and therefore comparable to this study). 1 A sample size of 417 patients per group (834 in total) was determined using a two-sample t-test with a significance level of α = 0.05 (two-sided) and a power of 1-β = 0.8 and accounted for an expected dropout rate of 20%.
After publication of the study protocol, 11 the sample size calculation was adapted based on new data of a second precursor pilot trial, which was analysed after the RCT was started and the trial registration was updated accordingly (DRKS00024657). As compared to the initial sample size estimation, this trial revealed a slightly lower mean reduction in migraine days and a higher standard deviation of change in a cohort, which was more closely comparable to the RCT study cohort. The mean change in the control group was estimated from studies with patients in control group aware of their allocation, therefore comparable to this study, and not adapted. The increase in sample size was approved by the Ethics Committee of the University of Lübeck on June 14, 2022, and submitted to the BfArM as the regulatory body on July 11, 2022. Of note, no data from the running RCT were considered for this adaption.
The primary analysis was carried out on the full analysis set (FAS), which included all randomised patients who provided informed consent and met the inclusion and exclusion criteria. The primary endpoint (including the subgroup analysis stratified by migraine prevention medication use) was tested using a linear model, assuming variance homogeneity, with a two-sided test using the exact F distribution at a significance level of α = 0.05. Sex and number of migraine days for the previous 4 weeks at baseline were included as covariables.
Secondary endpoints were tested using linear or logistic models in the FAS. A hierarchical testing procedure was used to correct for multiple testing and maintain the type I family-wise error rate at α = 0.05. Secondary endpoints were tested only if the primary endpoint was significant. The first secondary endpoint (reduction in migraine headache days per 4 weeks in adherent patients) served as an additional gatekeeper. If significant, other endpoints were tested using the Bonferroni-Holm method, ordering endpoints by p-values and adjusting significance levels accordingly. Testing stopped if significance was not found at any step.
Endpoint data from the headache diary were considered missing if data were available for <80% of days (or less than 22 of 28 days). For headache diaries with ≥80% coverage, missing data were replaced with the average of valid entries (prorated). For the primary efficacy analysis, multiple imputation based on the jump-to-reference method, with the control group as the reference, was performed. Models were estimated on each of the 500 draws of imputed data, and parameters were aggregated using Rubin's rules. No imputation was performed for other endpoints. In this case complete data were reported and samples sizes noted.
Sensitivity analyses evaluated all efficacy endpoints in the intention-to-treat (ITT) and per-protocol (PP) populations. The ITT set included all randomised individuals who did not withdraw consent. The PP set excluded patients with <50% adherence to nutritional recommendations, medication changes, or missing app data in the first 4 weeks. Three additional imputation methods were performed, and the imputed data were used to calculate the primary endpoint model. The first imputation was performed based on adherence to nutritional recommendations: adherent patients used the DTx effect as a reference and non-adherent patients used the control effect. The second imputation used Baseline Observation Carried Forward (BOCF), and the third imputation method used a complete-case analysis.
Descriptive statistics (mean, SD) were provided for relevant exploratory and post hoc endpoints. The safety analysis set included all randomised patients.
The analysis was performed with SAS® System 9.4 (SAS Inc., Cary/NC, USA).
The CONSORT guidelines for randomised controlled trials were followed.
Role of the funding source
This study was funded by Perfood (Perfood GmbH, Lübeck, Germany), who designed the study in collaboration with the investigators and provided the DTx and control app. Perfood had no role in the data analysis. Perfood contributed to data interpretation and writing of the publication in their role as authors.
Results
Patients were recruited between July 2021 and August 2023. Of the 4000 patients identified, 1070 met the inclusion criteria (Figure 2). At the end of the baseline phase, 842 were randomised to DTx or control. 7 patients were excluded from final analysis because of major violations of inclusion-/exclusion criteria (≥ 2 prophylactic agents used (DTx = 2, control = 1), change of prophylactic medication before study start (DTx = 1, control = 0), deletion of all app data (DTx = 1, control = 0), consent withdrawn (DTx = 0, control = 2)). The FAS included 835 patients (DTx = 416, control = 419), most of whom were female (95%; 793/835). The number of migraine days per 4 weeks, medication use, and comorbid conditions were similar across groups (Table 1, Table 2).

CONSORT diagram of patient disposition.
Baseline demographics and disease characteristics.

Data are n (%), mean (SD), or median (IQR). Assessed in the full analysis set.
*Percentages calculated using common medication as denominator. †Analysis of acute medications used in the baseline period was not predefined. ‡Moderate to severe intensity.
CGRP = calcitonin gene-related peptide. DTx = digital therapeutic. EQ-5D-5L = 5-level EuroQol 5-dimensional questionnaire. HIT-6 = Headache Impact Test-6. IQR = interquartile range. MIDAS = Migraine Disability Assessment. SD = standard deviation.
Endpoints in order of statistical hierarchy.
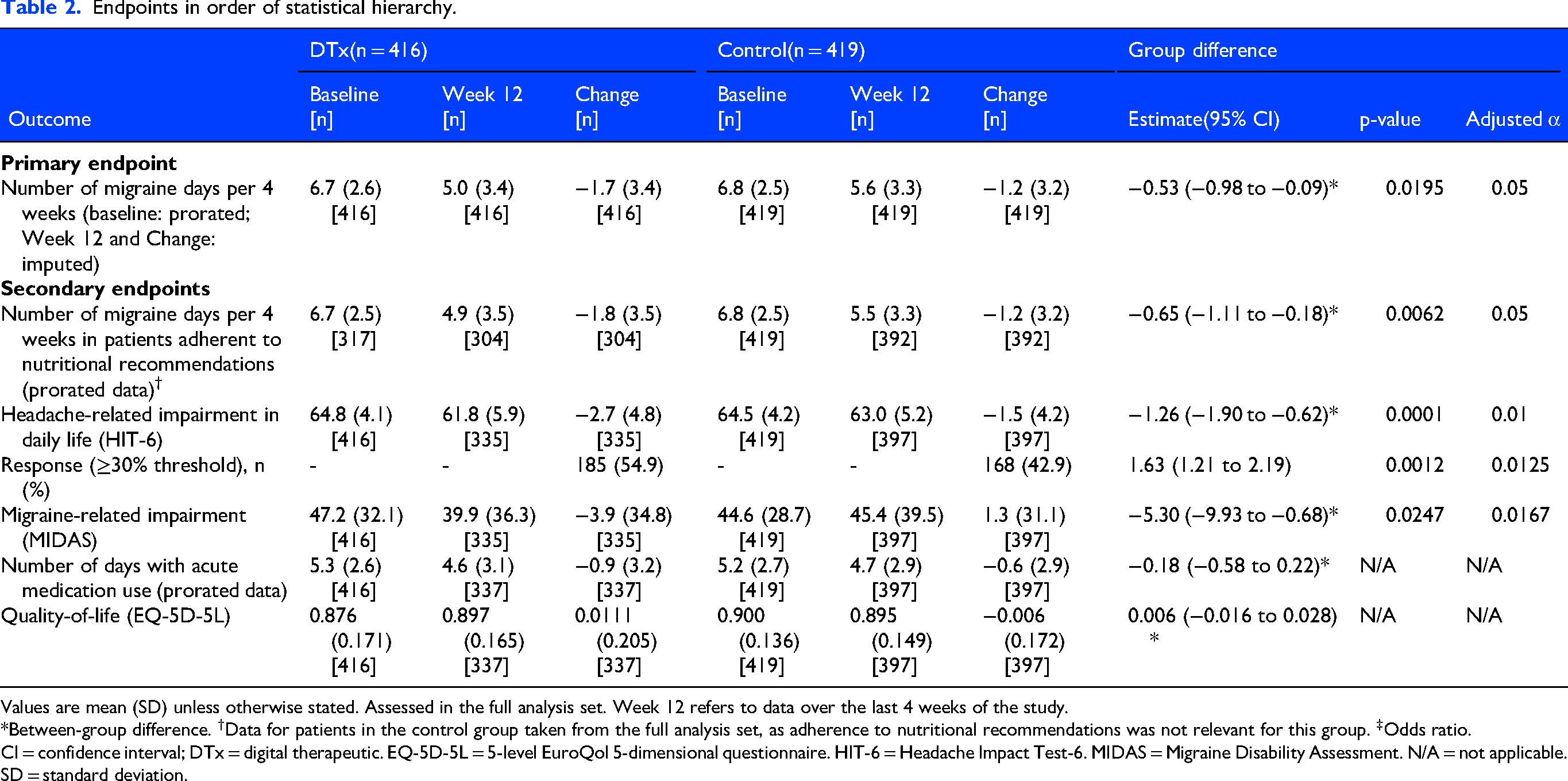
Values are mean (SD) unless otherwise stated. Assessed in the full analysis set. Week 12 refers to data over the last 4 weeks of the study.
*Between-group difference. †Data for patients in the control group taken from the full analysis set, as adherence to nutritional recommendations was not relevant for this group. ‡Odds ratio.
CI = confidence interval; DTx = digital therapeutic. EQ-5D-5L = 5-level EuroQol 5-dimensional questionnaire. HIT-6 = Headache Impact Test-6. MIDAS = Migraine Disability Assessment. N/A = not applicable. SD = standard deviation.
Baseline characteristics were well balanced between the two study arms, with no clinically meaningful differences observed for any demographic or clinical variable and are summarised in Table 1. The overall study population (N = 835; DTx n = 416, control n = 419) was predominantly female (95.0% in both arms), with a mean age of 39.1 years (SD 11.5). Mean body mass index was 24.3 kg/m2 (SD 4.6; n = 815). Participants had a long history of migraine, with a median of 18 years since diagnosis (IQR 10–28). Migraine with aura was present in 55.6% of participants. At baseline, participants experienced a mean of 6.8 migraine days of moderate-to-severe intensity per four weeks (SD 2.5). PRO scores reflected substantial disease burden: mean HIT-6 was 64.6 (SD 4.2), consistent with severe headache impact, and mean MIDAS was 45.9 (SD 30.5), indicating severe migraine-related disability. Mean EQ-5D-5L utility index was 0.888 (SD 0.155). Acute medication was widely used: 67.7% of participants used migraine-specific medication (triptans), 77.7% used non-migraine-specific medication, and 53.5% used both. A total of 190 participants (22.8%) were receiving concomitant preventive migraine medication at baseline, most commonly CGRP antibodies (27.9% of those on preventive treatment), antidepressants (24.2%), and beta blockers (15.3%). More than 61% of participants reported at least one comorbid condition, including psychiatric illness in 11.1%.
The trial met its primary endpoint; after 12 weeks, patients in the DTx group had a significantly greater reduction in the mean number of migraine days per 4 weeks compared with the control group (mean [SD]: 1.7 [3.4] versus 1.2 [3.2] days, respectively [Figure 3A]; imputed data, between-group difference estimate: −0.53 [95% CI −0.98 to −0.09], p = 0.0195 [Table 2]). Exploratory analysis showed that patients in the DTx group experienced a decreasing trend in the mean number of migraine days per 4 weeks through weeks 4, 8 and 12 (Supplemental figure 1). Post hoc analysis showed that the effect size for DTx versus control was similar for patients on migraine prevention medication compared with those who were not (between-group difference estimate: −0.52 [95% CI −1.57 to 0.54] versus −0.51 [-1.00 to −0.03], respectively). In keeping with the pre-specified analysis plan, additional subgroup analyses by class of preventive medication were not conducted, in order to preserve the inferential integrity of the trial and avoid the risk of spurious findings from multiple unplanned comparisons.

(A) Number of migraine days per 4 weeks in all patients (primary endpoint) and (B) in patients ≥50% adherent to nutritional recommendations (secondary endpoint) with (C) estimated treatment difference and (D) proportion of responders (patients achieving ≥30% relative reduction in the number of migraine days per 4 weeks based on use of a non-pharmacological intervention).
In the DTx group, 76.2% (317/416) of patients adhered to the nutritional recommendations; this subgroup of patients had a mean (SD) reduction of 1.8 (3.5) days in the number of migraine days per 4 weeks (figure 3B). While adherence to nutritional recommendations was not relevant for the control group, this was significantly greater than the reduction of 1.2 (3.2) days in the control group (prorated data; between-group difference estimate: −0.65 [95% CI −1.11 to −0.18], p = 0.0062, adjusted a = 0.05; Figure 3C, Table 2).
Patients reported a mean (SD) reduction from baseline in HIT-6 score of 2.7 (4.8) points and 1.5 (4.2) points in the DTx and control groups, respectively, indicating a greater improvement in headache-related impairment with DTx (between-group difference estimate: −1.26 points [95% CI −1.90 to −0.62], p = 0.0001, adjusted α = 0.01; Table 2).
There were greater proportions of responders (≥30% threshold) in the DTx group (54.9%; 185/337) compared with the control group (42.9% [168/392]; odds ratio: 1.63 [95% CI 1.21–2.19], p = 0.0012, adjusted α = 0.0125; Table 2). Exploratory analyses showed an increasing trend in the proportion of responders in the DTx group over time (≥30% threshold, Figure 3D; ≥50% threshold, Supplemental figure 2).
Patients reported a non-significant mean (SD) decrease (improvement) from baseline to Week 12 in the MIDAS scale of migraine-related impairment of 3.9 (34.8) points in the DTx group versus an increase of 1.3 (31.1) in the control group (between-group difference estimate: −5.30 points [95% CI −9.93 to −0.68], p = 0.0247, adjusted α = 0.0167; Table 2). Based on mean MIDAS score at baseline and Week 12, patients in the DTx group improved their MIDAS grade from very severe impairment to severe impairment, whereas there was no improvement in overall MIDAS grade in the control group (Table 2). Post hoc analysis showed that 37.6% of patients receiving DTx improved by at least one MIDAS grade compared with baseline; this increased with increasing baseline MIDAS grade severity, reaching 44.3% of patients with very severe impairment (MIDAS grade IV-B) at baseline (Supplemental figure 3).
There was no significant difference between the DTx and control groups in the number of days requiring acute medication or in change in quality-of-life (Table 2). Exploratory analysis suggested that PGIC score was higher at Week 12 for patients in the DTx group versus control (between-group difference estimate: −0.80 [95% CI −0.91 to −0.68]; Supplemental figure 4A). Overall, 77.3% of patients rated their overall health status as improved in the DTx group, compared with 30.7% in the control group (Supplemental figure 4B).
A total of 276 AEs (142 in the DTx group, 134 in the control group) and 22 SAEs (7 in the DTx group, 15 in the control group) were reported during the safety analysis. There were no AEs or SAEs causally related to the DTx (Table 3). Of the 205 infections reported during the study, 148 were due COVID-19 (81/102 in the DTx group; 67/103 in the control group).
Safety summary.

Data are number of AEs reported (not number of patients with the AE) in the safety analysis set.
*AEs during the study were coded according to the MedDRA version 27.0. †Includes cysts and polyps. ‡AE details: blood glucose derailment after food intake was initially linked to the DTx; medical monitoring later determined that it was a normal physiological response, ruling out the DTx as the cause. No SAEs were deemed related to the investigational product.
AE = adverse event. DTx = digital therapeutic. SAE = serious adverse event.
The PP sensitivity analysis included 259 patients in the DTx group and 346 in the control group (n = 605/835; 72.5% of the FAS). As expected, there was a greater reduction in the mean (SD) number of migraine days per 4 weeks (1.9 [3.4]) for the DTx group in the PP analysis than in the FAS (between-group difference: −0.85 [95% CI −1.34 to −0.37], p = 0.0006). In the ITT analysis (340 in the DTx group, 392 in the control group), the DTx group experienced a mean (SD) decrease of 1.8 (3.4) days in the number of migraine days per 4 weeks (between-group difference: −0.64 days [95% CI −1.09 to −0.2], p = 0.0048).
Discussion
The use of the sinCephalea, a non-pharmacological DTx which provides personalised nutritional and lifestyle recommendations via short-term use of CGM, on top of standard treatment, resulted in a significant reduction in the mean number of MMD per 4 weeks and associated disease-specific quality-of-life impairment (measured by HIT-6 and MIDAS), compared with use of a control app, all without DTx-related AEs. Furthermore, a large proportion of patients using the DTx improved their overall health status (assessed by PGIC) and reduced their migraine-related disease impairment (measured by MIDAS) by at least one grade. This study applied the same scientific rigor as is used for pharmacological interventions, 17 supporting the potential clinical utility of a DTx for migraine prevention as add-on therapy with standard treatment.
The DTx was assessed in patients with episodic migraine with severe disease impairment, indicated by high baseline HIT-6 and MIDAS scores (64.8 and 47.2, respectively). Furthermore, just under a quarter of patients were on migraine prevention pharmacological medications. This means that many patients had severe and persistent migraine despite receiving a high standard of care. It was therefore encouraging to see a large effect size with a non-pharmacological intervention, with or without concomitant pharmacological treatment. Currently, not universally accepted minimal clinically important difference (MCID) has been defined for the absolute reduction in monthly migraine days. Therefore, clinical relevance is usually assessed by responder rates, i.e., the proportion of patients achieving a ≥ 30% or ≥50% reduction in monthly migraine days. In the current study, 55% of patients achieved a clinically meaningful (≥30%) reduction in MMD, with 38% achieving a ≥ 50% reduction in MMD, alongside reductions in disease impairment; this compares favourably with pharmacological interventions, such as calcitonin gene-related peptide (CGRP) antibodies, where approximately 30–62% of patients achieve a ≥ 50% reduction in MMD after 3–6 months. 18 Furthermore, clinically relevant improvements in migraine-related impairment were even seen in 44% of patients with the most severe disease (MIDAS grade IV-B), and 77% of patients reported that their overall health status had improved (per PGIC). Consequently, DTx may be particularly beneficial for those with severe and persistent migraine or for those intolerant to other pharmacological treatments.
The observed between-group difference of −0.53 migraine days per 4 weeks is a modest absolute reduction in isolation; however, it should be interpreted in the context of the relatively low baseline migraine frequency in this population (mean 6.7 days per 4 weeks), in which a reduction of this magnitude represents a meaningful proportional decrease. Moreover, this estimate increased to −0.65 days in the adherent subgroup and −0.65 days in the per-protocol population, suggesting that the full clinical benefit is best captured in patients who engage with the intervention as intended. The within-group reduction in the DTx arm was substantially larger (1.7 days per 4 weeks), reflecting a combination of the true intervention effect and non-specific effects inherent to the open-label design which cannot be formally separated in the absence of blinding. It should be noted, however, that blinding is inherently not feasible in DTx trials as participants cannot be masked to a personalised digital intervention in the same way as to a pharmacological treatment. Furthermore, in behavioural and digital interventions, expectation effects are not merely a source of bias but may themselves constitute part of the therapeutic mechanism. Applying conventional MCID thresholds derived from pharmacological trials rigidly to the between-group difference in a multicomponent DTx study may therefore systematically underestimate its true clinical relevance.
The study population had a mean baseline frequency of 6.7 migraine days per 4 weeks; patients with chronic migraine were excluded per protocol. Whether the findings generalise to patients with higher-frequency episodic or chronic migraine remains to be established. Such patients may derive greater absolute benefit from the DTx, given the larger ceiling for migraine day reduction; however, they may also have more established migraine pathophysiology that is less amenable to dietary modification alone. Dedicated trials in higher-frequency migraine populations are warranted.
A Complier Average Causal Effect (CACE) estimate (ITT effect of −0.53 days divided by the compliance proportion of 317/416) yields −0.69 days, closely matching the −0.65 days observed in our per-protocol analysis. This convergence underscores the robustness of the intervention effect among compliers.
In addition to disease severity, our population demographics align with those in other studies assessing pharmacological interventions for migraine. 19 The greater proportion of women compared with men reflects the fact that migraine is more common and often more severe in women, leading to their overrepresentation in migraine studies.20,21 Additionally, studies have shown that women more frequently take part in DTx trials than men and may be more engaged with health digitalisation since they are more likely to have wearable devices.10,22,23
The absence of a between-group difference in acute medication use and EQ-5D-5L may be explained with several aspects. The absolute reduction in migraine days (0.53 days per four weeks) may have been insufficient to translate into detectable changes in acute medication behaviour within the 12-week observation period. The EQ-5D-5L measures broad health-related quality of life across five generic dimensions and may lack sensitivity to capture migraine-specific improvements, particularly given the near to normal baseline measure. However, the significant between-group differences in HIT-6 and MIDAS - migraine-specific instruments designed to capture functional and disability burden - support a genuine clinical benefit that is more appropriately reflected by disease-specific outcome measures.
The study shows that the DTx can be used for remote self-management, including behavioural modifications. In addition to providing personalised nutritional recommendations, the DTx provided educational content on sleep hygiene, relaxation exercises, and lifestyle factors, which have demonstrated efficacy in other disease areas 2 ; these components were not included in the control app. The application of these techniques with the DTx significantly reduced migraine days and improved response and disease-related quality-of-life. This compares favourably with other non-pharmaceutical therapies that are recommended by the current German treatment guidelines, such as cognitive behavioural therapy, relaxation techniques, or biofeedback. 18 These non-pharmacological therapies have been shown to reduce migraine frequency by 35‒50% in less rigorous studies than the current DTx study. 24
No DTx-related AEs or SAEs were reported in this trial. This contrasts favourably to traditional oral migraine preventative treatments, which commonly lead patients to discontinue treatment due to AEs.25,26 Pharmaceutical treatments therefore frequently involve a compromise between achieving therapeutic efficacy and managing AEs. The absence of such trade-offs in the DTx group underscores its potential as a viable non-pharmacological alternative for migraine management. Of interest, as patients were recruited between July 2021 and August 2023, the study took place during the COVID-19 pandemic. In total, 72% of the infections during the study were related to COVID-19.
The self-managed nature of sinCephalea warrants consideration in vulnerable patient groups. Patients with eating disorders were excluded from this trial, and nutritional self-management in such individuals would require careful clinical supervision. Conversely, the favourable safety profile and absence of DTx-related adverse events make sinCephalea particularly suitable for patient groups in whom pharmacological options are limited or contraindicated, such as women who are pregnant or planning to conceive. In routine clinical practice, prescription of sinCephalea should be accompanied by appropriate clinical oversight, especially in patients at nutritional risk.
Migraine severely impacts work productivity and professional life, primarily through presenteeism, leading to decreased effectiveness, job insecurity, and financial difficulties, 27 and the economic burden for the patient and healthcare system can be considerable. 28 The authors hypothesise that the global use of scalable DTx could alleviate these costs and improve access to effective care. Consequently, it is of interest that the DTx sinCephalea appeared to improve impairment, which could have positive economic implications. In the current study, daily impairment due to headache, measured by HIT-6, decreased by a mean of 2.7 points from baseline; notably, a mean reduction of ≥2.5 points in HIT-6 score is considered clinically meaningful for pharmacological interventions. 29
Reimbursement is a key issue as countries consider adopting DTx.30,31 The 2019 German Digital Healthcare Act, which allowed reimbursement for DTx, has significantly advanced the integration of DTx into the healthcare system; this led to approximately 374 000 DTx prescriptions over the first 3 years. 10 This legislative initiative underscores the growing acceptance and adoption of digital solutions in healthcare, reflecting their increasing role in patient care and insurance reimbursement processes. Concepts and frameworks for reimbursement of DTx have been explored based on the German experience and could be applied to other countries.26,27
This study's rigorous design and the high threshold for efficacy in the therapeutic area strengthen the reliability of the results, positioning the trial as a benchmark for future DTx intended for therapeutic use. The low dropout rate and good adherence further support the robustness of the findings. Furthermore, the sensitivity analysis in the PP population showed that efficacy is greater in patients who used the DTx as designed, highlighting the potential usefulness of this as an intervention for migraine. However, the open-label design of the study may have introduced self-assessment bias, a common issue in digital health research, potentially explaining the improvements seen in both groups (55% in the DTx group and 43% in the control group reported ≥30% reduction in MMD). To mitigate this effect, the control group used a design-matched control app as an electronic headache diary, improving comparability between groups.
The exploratory analysis revealed an early reduction in migraine days observed in both groups during the first four weeks of the intervention. Several non-specific mechanisms may have contributed to this pattern: regression to the mean, heightened self-monitoring associated with study participation, and expectation effects inherent to the open-label design. The progressive divergence between groups over subsequent weeks, however, suggests that the sustained treatment effect in the DTx group reflects a genuine intervention-specific benefit beyond these non-specific effects.
A key limitation is the use of PROs for primary and secondary endpoints, including changes in MMD and assessments from HIT-6 and MIDAS questionnaires. While PROs are vital for assessing the impact on quality-of-life and migraine burden, they are prone to subjective perception and recall bias. The daily electronic diary helped reduce subjective interpretation by recording symptoms according to IHS criteria, but self-assessment remains inherently subjective and must be considered when interpreting these findings. The open-label design strengthens this limitation, which comes with the nature of the tested intervention.
Glucose monitoring was restricted to the pre-intervention phase to derive personalized nutritional recommendations, and no longitudinal CGM data were collected during the 12-week intervention. Therefore, we cannot directly demonstrate changes in blood glucose variability over the study course, which represents a limitation of the present trial. It should be noted that the intervention included both personalized dietary advice and broader lifestyle recommendations, and these components were delivered simultaneously. As a result, we cannot disentangle the specific effects of the dietary intervention from those of the lifestyle guidance. Indeed, general improvements in diet quality, increased hydration, and potential reductions in body weight may each independently contribute to a reduction in migraine frequency through mechanisms unrelated to blood glucose, as discussed in the literature. 32 Furthermore, as BMI was assessed at baseline only and not re-measured at Week 12, formal adjustment for weight change was not possible. Future studies incorporating longitudinal anthropometric assessments and continuous glycaemic monitoring throughout the intervention period would allow more definitive mechanistic conclusions. However, the personalised, CGM-based diet was a core and novel element of the intervention, likely driving the observed efficacy.
Finally, the durability of the treatment effect beyond the 12-week study period remains an open question. Sustained engagement with DTx is a recognised challenge, and adherence to dietary modifications in routine clinical practice - without the structured support of a trial setting - may diminish over time. Future studies should incorporate longer follow-up periods and evaluate strategies to maintain product and dietary adherence. In summary, the DTx sinCephalea is the first non-pharmacological intervention powered by CGM to deliver personalised nutrition and lifestyle recommendations for migraine prevention. The DTx reduced migraine frequency and improved disease-specific quality-of-life impairment through remote nutritional management of migraine without any DTx-related AEs. While currently available only in Germany, future efforts will focus on expanding validation studies across different countries. Further research may explore any synergistic impacts of a low-glycaemic diet and digital health interventions on migraine treatment outcomes. As DTx continue to gain momentum, the findings of this trial highlight the potential for non-pharmacological DTx to transform the migraine treatment landscape. This will help address the significant burden of this condition using scalable, innovative, non-invasive, and convenient digital interventions.
Article highlights
A large open-label randomised trial evaluated a digital therapeutic (sinCephalea) delivering CGM-supported personalised nutrition for migraine prevention.
The digital intervention significantly reduced monthly migraine days compared with a design-matched control application.
Clinically relevant responder rates and migraine-related disability improved, particularly among adherent patients.
No digital therapeutic-related adverse events were observed.
Findings support digital therapeutics as a scalable non-pharmacological option in migraine care.
Supplemental Material
sj-png-1-cep-10.1177_03331024261459744 - Supplemental material for Efficacy of digital therapeutic sinCephalea for personalised nutrition versus control for migraine prevention: A 12-week open-label randomised clinical trial
Supplemental material, sj-png-1-cep-10.1177_03331024261459744 for Efficacy of digital therapeutic sinCephalea for personalised nutrition versus control for migraine prevention: A 12-week open-label randomised clinical trial by Stefan Evers, Hanna C.B. Grube, Astrid Gendolla, Charly Gaul, Kristian Ewald, Oliver Witt, Jenny Voggel, Matthias Nitschke, Christian Sina, Diamant Thaçi, Inke R. König and Torsten Schröder in Cephalalgia
Supplemental Material
sj-png-2-cep-10.1177_03331024261459744 - Supplemental material for Efficacy of digital therapeutic sinCephalea for personalised nutrition versus control for migraine prevention: A 12-week open-label randomised clinical trial
Supplemental material, sj-png-2-cep-10.1177_03331024261459744 for Efficacy of digital therapeutic sinCephalea for personalised nutrition versus control for migraine prevention: A 12-week open-label randomised clinical trial by Stefan Evers, Hanna C.B. Grube, Astrid Gendolla, Charly Gaul, Kristian Ewald, Oliver Witt, Jenny Voggel, Matthias Nitschke, Christian Sina, Diamant Thaçi, Inke R. König and Torsten Schröder in Cephalalgia
Supplemental Material
sj-png-3-cep-10.1177_03331024261459744 - Supplemental material for Efficacy of digital therapeutic sinCephalea for personalised nutrition versus control for migraine prevention: A 12-week open-label randomised clinical trial
Supplemental material, sj-png-3-cep-10.1177_03331024261459744 for Efficacy of digital therapeutic sinCephalea for personalised nutrition versus control for migraine prevention: A 12-week open-label randomised clinical trial by Stefan Evers, Hanna C.B. Grube, Astrid Gendolla, Charly Gaul, Kristian Ewald, Oliver Witt, Jenny Voggel, Matthias Nitschke, Christian Sina, Diamant Thaçi, Inke R. König and Torsten Schröder in Cephalalgia
Supplemental Material
sj-png-4-cep-10.1177_03331024261459744 - Supplemental material for Efficacy of digital therapeutic sinCephalea for personalised nutrition versus control for migraine prevention: A 12-week open-label randomised clinical trial
Supplemental material, sj-png-4-cep-10.1177_03331024261459744 for Efficacy of digital therapeutic sinCephalea for personalised nutrition versus control for migraine prevention: A 12-week open-label randomised clinical trial by Stefan Evers, Hanna C.B. Grube, Astrid Gendolla, Charly Gaul, Kristian Ewald, Oliver Witt, Jenny Voggel, Matthias Nitschke, Christian Sina, Diamant Thaçi, Inke R. König and Torsten Schröder in Cephalalgia
Footnotes
Acknowledgments
The authors would like to thank the participating patients and their families, clinicians, and study investigators. Special thanks are extended to Dominik Burziwoda-von Papen from Perfood for his unwavering support, which has been instrumental in the successful execution of this clinical trial, to Franziska Schulz from Perfood for her project management, trial management and support of clinical data management and Alicia Droste from Perfood for her trial management support. Additionally, we would like to acknowledge the study centre and the Center for Clinical Trials Lübeck Trial Centre (KKS), including the monitors, for their valuable contributions to the success of this study.
Medical writing support (in the form of writing assistance, including preparation of the draft manuscript under the direction and guidance of the authors, collating and incorporating authors’ comments for each draft, assembling tables and figures, grammatical editing, and referencing) was provided by Elena Garonna, PhD, CMPP, and Hayley Ellis, PhD, CMPP of Avalere Health, which was funded by Perfood.
ORCID iDs
Ethical considerations
The study was approved by the Ethics Committee of the University of Lübeck (January 19, 2021, file number 20–285) and was registered with the DRKS (March 8, 2021, DRKS-ID:DRKS00024657).
Consent to participate
Written informed consent was obtained from all patients prior to individual study onset.
Consent for publication
The authors agree to publish with Cephalalgia if accepted.
Author contributions
SE, IRK, CS, and TS conceived the study. DT was the chief investigator. OW, KE, and JV participated in patient data collection. IRK and HCBG were the study biostatisticians and responsible for the statistical analyses. SE, AG, CG, KE, and MN oversaw the study. SE, OW, IRK, and HCBG directly accessed and verified the data reported in the manuscript. SE, HCBG, AG, CG, KE, OW, JV, MN, CS, DT, IRK, and TS wrote and reviewed the manuscript. All authors had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Funding
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SE has received honoraria as advisory board member and as speaker from (past three years): Betapharm; Lilly; Lundbeck; Novartis; Perfood; Rehaler; Teva; research funding and consulting fees from Perfood; and has participated on advisory board for Perfood.
HCBG received funding support for statistical planning and analyses from Perfood, with payments made to the Institute of Medical Biometry and Statistics University of Lübeck.
CG has received consulting fees from Perfood, Vectura Fertin, Merz, Pfizer, and betapharm; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events for Lilly, Novartis, Lundbeck, Abbvie, Chordate, Hormosan, TEVA, Sanofi, betapharm, and Grünenthal; has participated on a Data Safety Monitoring Board or Advisory Board for Novartis, Lundbeck, Vectura, Merz, Abbvie, TEVA, and betapharm; and has acted as Scientific Advisor for migraine and cluster headache patient organisation.
KE and OW were employed at Perfood. JV was employed at Perfood; and has received speakers’ honoraria from Academy for Innovative Education and Management (AIM).
MN declares no competing interests.
CS was a co-founder and minority shareholder of Perfood. DT has received support for this manuscript from Perfood; has received grants or contracts from AbbVie, Novartis, and Leo; has received consulting fees from AbbVie, Almirall, Bristol-Myers Squib, Celltrion, Eli Lilly, Janssen-Cilag, Leo-Pharma, Novartis, Perfood, and UCB; has received payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from AbbVie, Almirall, Bristol-Myers Squib, Celltrion, Eli Lilly, Janssen-Cilag, Leo-Pharma, Novartis, and UCB; has participated on a Data Safety Monitoring Board or Advisory Board for AbbVie, Eli Lilly, Janssen, Novartis, and UCB; and has been member of the scientific board on the patient organisation “Psoriasis-Bund”.
IRK received funding support for statistical planning and analyses from Perfood, with payments made to the Institute of Medical Biometry and Statistics University of Lübeck.
TS was employed at Perfood; has a patent pending for Improved Method for Determining Blood Sugar Reactions; and was a co-founder and minority shareholder at Perfood.
AG declares no competing interests.
Data sharing statement
De-identified participant data that underlie the results will be made available on reasonable request to academic researchers. Requests to access the data can be made by sending an email together with a research plan to the study sponsor. Individual data are not publicly available owing to data protection regulations. Data will be available for 10 years after study completion.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.