
Abstract
Background
Evidence supporting calcitonin gene-related peptide monoclonal antibody (CGRP mAb) use in adolescents with migraine is limited. Rapid recovery for daily school functioning is particularly important during this stage of life. We aimed to evaluate early functional outcomes in daily and school activities, as well as headache-related outcomes after initiating CGRP mAb therapy in Japanese adolescents with migraine.
Methods
This single-center retrospective cohort study included patients aged 15–17 years who received CGRP mAb therapy (galcanezumab, fremanezumab or erenumab) for migraine between May 2021 and July 2025. The primary outcome was time to clinically meaningful improvement on the Headache Impact Test-6 (HIT-6) scores, comprising a reduction of ≥ 6 points from baseline, and was analyzed using the Kaplan–Meier method. Secondary outcomes included tracking longitudinal HIT-6 trajectories with mixed-effects models for repeated measures, exploratory univariable comparisons for early response (≥ 6-point reduction within 10–14 weeks), questionnaire-based daily functioning assessments, and safety evaluations.
Results
Of 34 adolescents who initiated CGRP mAb therapy, 33 participated in HIT-6 analyses. The cumulative response rate began increasing immediately after treatment initiation, reaching 68.3% (95% confidence interval = 44.6–81.8%) within the 10–14-week period; approximately half of the responders achieved meaningful improvement by weeks 4–6. Mixed-effects models for repeated measures analyses adjusted for baseline HIT-6 scores showed a least-squares mean change of −9.4 points at 12 weeks (95% confidence interval = −14.2 to −4.6; p < 0.001), with benefits sustained over follow-up. Among questionnaire respondents (n = 27), school attendance or concentration in the classroom was the most affected activity before treatment (70.4%) and 88.9% indicated that their primary treatment goals were mostly or partially achieved. Adverse events were reported by 40.7% of participants, primarily injection-site reactions (29.6%), none of which led to therapy discontinuations or modifications.
Conclusions
In this real-world adolescent cohort, CGRP mAb therapy was associated with early and clinically meaningful improvements in headache-related impact and self-reported functioning. Safety and tolerability findings are particularly notable given the limited evidence in this age group. Further prospective controlled studies are warranted to validate these findings and to identify predictors of early functional response.
This is a visual representation of the abstract.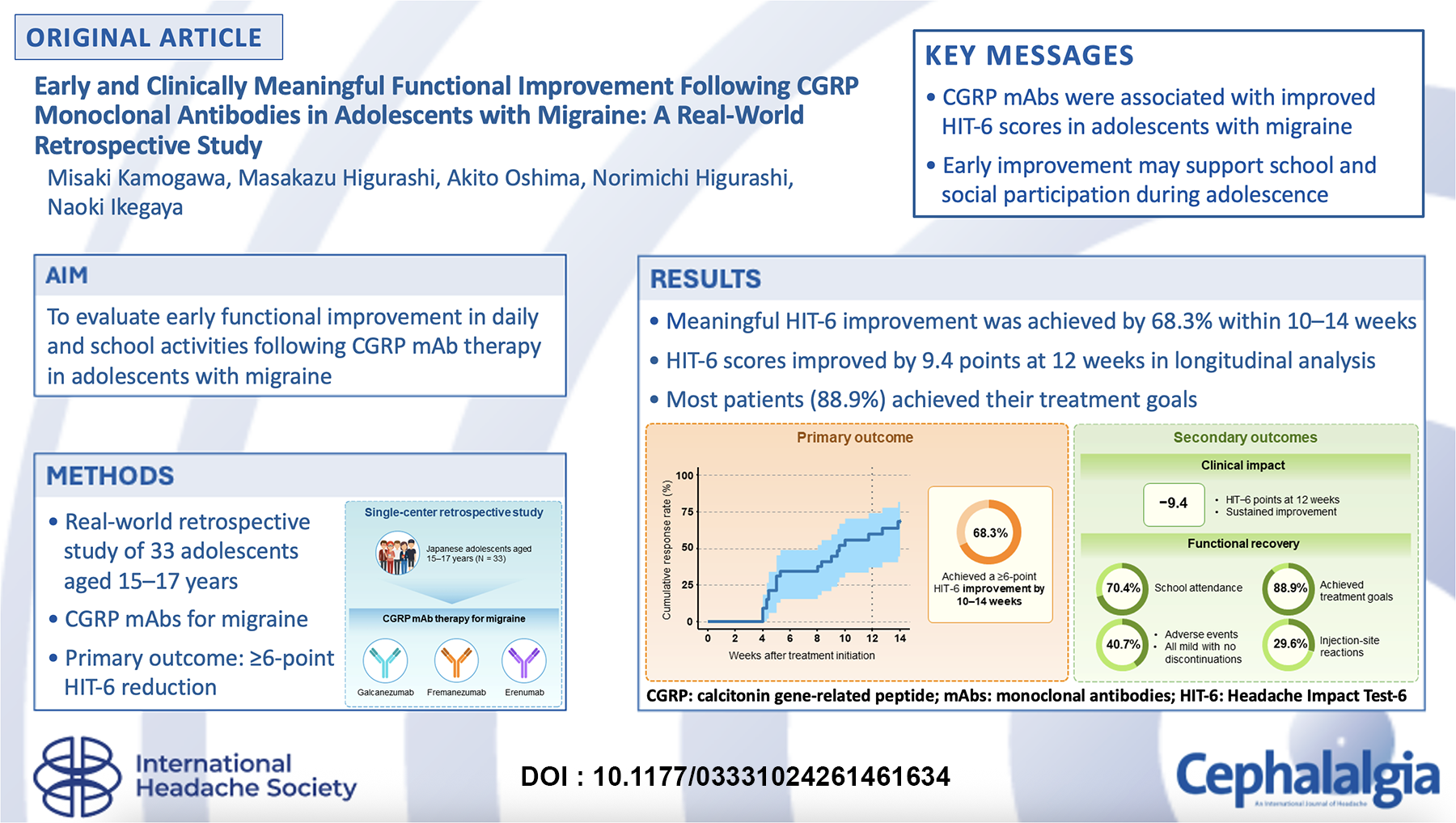
Introduction
Headache is a leading cause of disability throughout life, from childhood through adulthood, with migraine contributing substantially to the global health burden.1,2 Migraine attacks present with severe pain and are often accompanied by symptoms such as nausea, photophobia, and phonophobia, which can profoundly interfere with critical aspects of daily functioning, including academic performance, social engagement, and interpersonal relationships. 3 These effects are particularly salient during adolescence, a developmental stage characterized by increased academic pressures, variable daily routines, and heightened social complexity. In this context, headache-related functional impairment may accumulate and reinforce activity avoidance. 4 Accordingly, clinical management of adolescents with migraine should extend treatment objectives beyond only reducing headache frequency and intensity, emphasizing restoration of function in daily and school life.
Clinical trials and real-world studies in adults have established the efficacy of calcitonin gene-related peptide monoclonal antibodies (CGRP mAbs) for migraine prevention, with therapeutic benefits observed over 3–12 months.5–7 However, evidence regarding their use in adolescents is limited, with most data derived from small single-center studies and few real-world investigations.8,9 In addition, a previous study focused on patients with severe or treatment-refractory migraine. 10 Consequently, generalizable evidence regarding the effectiveness, safety, and longitudinal trajectories of treatment response to CGRP mAbs in adolescents with migraine is scarce. The American Headache Society recommends evaluating the effectiveness of monthly CGRP mAb therapy in adults at 3 months to guide continuation decisions, 11 with many studies designating 3 months as a key evaluation time point. However, adolescence often involves tightly scheduled examinations, school events, and extracurricular activities, where headache-related functional impairment directly influences treatment planning. It remains unclear whether the adult evaluation timeframe is sufficient for this age group, in whom delayed functional recovery may lead to difficulties keeping up with school and social activities. Thus, leveraging real-world data to longitudinally assess the temporal evolution of treatment effects alongside functional outcomes is a pragmatic approach to defining the clinical utility of CGRP mAb therapy in adolescents with migraine.
The present study was designed to assess whether CGRP mAb treatment in adolescents with migraine is associated with significant improvements in headache symptoms and functional outcomes, and to identify the magnitude and earliest occurrence of meaningful change in headache-related disability as measured using the Headache Impact Test-6 (HIT-6) scores. Using real-world data from a single center in Japan, we aimed to evaluate treatment-associated changes in daily functioning by integrating HIT-6 scores with additional patient-reported measures. Clarifying the temporal pattern and functional associations of treatment response in adolescents may inform preventive treatment selection in routine care and guide the establishment of clinically meaningful treatment objectives during this developmental stage.
Methods
Study design
This single-center, retrospective observational cohort study included adolescents aged 15–17 years receiving CGRP mAb therapy for migraine at the Hodogaya Neurosurgical Clinic in Kanagawa, Japan. The study protocol was reviewed and approved by the Ethics Committee of Yokohama City University Graduate School of Medicine (approval number: F260200006). Analyses of existing medical records, including HIT-6 data, were conducted on an opt-out basis for patients and guardians.
For the questionnaire survey, informed consent was obtained from patients and their guardians. The questionnaire was administered retrospectively after completion of follow-up via an electronic form. This study follows the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines.
Patients
Patients aged 15–17 years who received CGRP mAb therapy for migraine between May 2021 and July 2025 were included in this study. The observation period extended from May 2021 to November 2025. Brain magnetic resonance imaging was routinely performed at the initial visit to exclude secondary headache etiologies. Migraine diagnoses were established by board-certified headache specialists according to the International Classification of Headache Disorders, 3rd edition (ICHD-3). 13 In clinical practice in our center, CGRP mAb therapy was considered for patients with severe headache-related disability (HIT-6 scores ≥ 60), insufficient response or intolerance to at least one conventional preventive medication, poor adherence to oral preventive therapy, or a clinical need for prompt symptom relief due to time-sensitive circumstances such as upcoming academic examinations. The CGRP mAbs included galcanezumab (240 mg loading dose followed by 120 mg once monthly), fremanezumab (225 mg every 4 weeks), and erenumab (70 mg every 4 weeks). All three agents are covered under Japan's national health insurance system with a standard 30% co-payment, although costs exceed those of conventional oral preventive medications, and some patients declined treatment due to injection or cost concerns. In routine clinical practice, the choice among the three CGRP mAb agents and treatment regimen, including the galcanezumab loading dose, was determined through shared decision-making, considering tolerability profiles, patient or guardian preferences, and cost factors. Patients were counseled to continue CGRP mAb therapy for at least 3 months, and approximately 3 months of treatment served as a general guide for decisions regarding continuation or switching. Clinical data were collected from medical records and patient-reported outcome questionnaires. Patients with only a single available HIT-6 assessment during the observation period were excluded. Those who switched between CGRP mAbs during follow-up were not excluded from the study. Some patients qualified for multiple headache-related diagnoses during screening, either concurrently or across separate visits. Hence, a pre-established priority hierarchy was applied, assigning each individual to a single mutually exclusive category to ensure each patient was counted once.
Research items
The following data were collected retrospectively. Demographic characteristics (age, sex, height, and weight), medical history, migraine type (episodic or chronic, classified according to the ICHD-3), medication-overuse headache (MOH) status, longitudinal changes in HIT-6 scores, use of preventive migraine medications and triptans prior to CGRP mAb initiation, response to triptans before CGRP mAb therapy, preventive treatments administered after initiation, and concomitant use of triptans after treatment initiation were obtained from medical records. Patient-reported outcomes were assessed using questionnaires (see Supplementary material, Table S1) that evaluated daily-life disability, achievement of treatment goals, changes in headache status following treatment, Patient Global Impression of Change (PGIC) 12 score, presence of aura, adverse events associated with injectable treatments, and the severity of adverse events.
Adverse events and their severity were determined based on questionnaire responses and physician assessments at follow-up visits. Severity was classified as mild (no intervention required), moderate (requiring additional treatment) or severe (requiring treatment modification or discontinuation). Response to triptans prior to CGRP mAb initiation was assessed based on medical records; patients were classified as triptan responders if they were headache-free within 2 h of the specific triptan used by each patient, for at least three migraine attacks before CGRP mAb initiation.14,15 The presence of aura was primarily evaluated based on patient-reported questionnaires, with supplementary information drawn from medical records when questionnaire data were missing or insufficient.
Assessments
The primary outcome was time-to-response, defined as the interval from initiation of CGRP mAb therapy to the first clinically significant improvement in HIT-6 score, comprising a reduction of ≥ 6 points from baseline.16,17 Baseline HIT-6 was determined at the time of the initial CGRP mAb injection, with subsequent HIT-6 assessments conducted during routine monthly visits approximately every 4 weeks, consistent with the dosing interval of each CGRP mAb. Time-to-response was assessed within an observation window of 10–14 weeks after treatment initiation; due to variations in the timing of follow-up visits inherent in routine clinical practice, any visits within this window were considered representative of the 3-month assessment.
Secondary outcomes were evaluated using distinct analysis sets based on data availability. First, longitudinal changes in HIT-6 scores from baseline were analyzed among patients with repeated measurements. 18 Second, clinical factors associated with early response were examined within the same patient population. Early response was defined as a reduction of six or more points in the HIT-6 score within the specified 3-month assessment window (10–14 weeks) after treatment initiation. This “early” time frame aligns with the conventional week-12 efficacy assessment frequently used in pivotal CGRP mAb trials.19,20 Current evidence-based guidelines for adults recommend a minimum of 3–6 months before evaluating treatment effectiveness for anti-CGRP mAbs, 21 underscoring that meaningful improvement within the first 3 months may represent an earlier-than-expected clinical response. For daily life disability, respondents identified the single most impaired activity (single-choice), rather than multiple activities.
Given the small overall sample size, excluding switchers would have further reduced statistical power; therefore, switchers were retained in all analyses, including questionnaire-based assessments. Censoring was applied at discontinuation if CGRP mAb therapy was interrupted for 90 or more consecutive days. Follow-up time contributed to the analysis up to the point of discontinuation, and data after treatment resumption were not included.
Statistical analysis
Statistical analyses were performed using R, version 4.5.2 (R Foundation). Continuous variables are presented as the mean ± SD) or median (interquartile range (IQR)), as appropriate, while categorical variables are expressed as n (%). Comparisons between early and non-early responders were performed using Welch's t-test for continuous variables and Fisher's exact test for categorical variables. All statistical tests were two-sided, with p < 0.05 considered statistically significant. Time-to-response was evaluated using the Kaplan–Meier method. Because HIT-6 assessments were performed at scheduled clinic visits, event times are interval-censored rather than continuous. The Kaplan–Meier method was therefore applied for descriptive and exploratory purposes, and findings should be interpreted accordingly. To assess the robustness of the primary analysis against potential bias related to treatment switching and incomplete follow-up, two sensitivity analyses were conducted. First, patients who switched CGRP mAbs were censored at the time of switching. Second, in a conservative worst-case analysis, all patients without a confirmed response within 14 weeks were treated as non-responders (simple proportion). Longitudinal HIT-6 trajectories were analyzed using a mixed-effects model for repeated measures (MMRM), in which time was treated as a categorical factor (0, 4, 8, 12, and 16 weeks). Follow-up visits occurred at variable intervals in routine clinical practice, and visit times were grouped into 4-week categories based on the nearest scheduled interval. Baseline HIT-6 served as a covariate. A participant-level random intercept accounted for the within-subject correlation across repeated measurements. Model assumptions included normally distributed residuals and missing at random for incomplete observations. Baseline characteristics and treatment-related factors potentially associated with early response were explored through univariable comparisons. Due to the limited sample size, multivariable analyses were not conducted to avoid overfitting, and all analyses should be regarded as exploratory and interpreted accordingly. Questionnaire-based outcomes were summarized descriptively.
Missing data
All available data were included in the analyses. Patients with less than 3 months of follow-up contributed data up to their last visit. For Kaplan–Meier analyses, patients were retained if treatment continuation was confirmed despite intermittent missing assessments. Missing values were not imputed for longitudinal analyses; instead, data from subsequent visits were used.
Results
Patient characteristics
Between May 2021 and July 2025, 342 adolescents aged 15–17 years presented with headache at the Hodogaya Neurosurgical Clinic. Following clinical evaluation, 217 individuals received a diagnosis of migraine. Of these, 183 were managed without CGRP mAbs, and 34 received CGRP mAb therapy (Figure 1). One patient was excluded due to insufficient longitudinal HIT-6 follow-up scores, resulting in 33 patients included in HIT-6–based analyses.
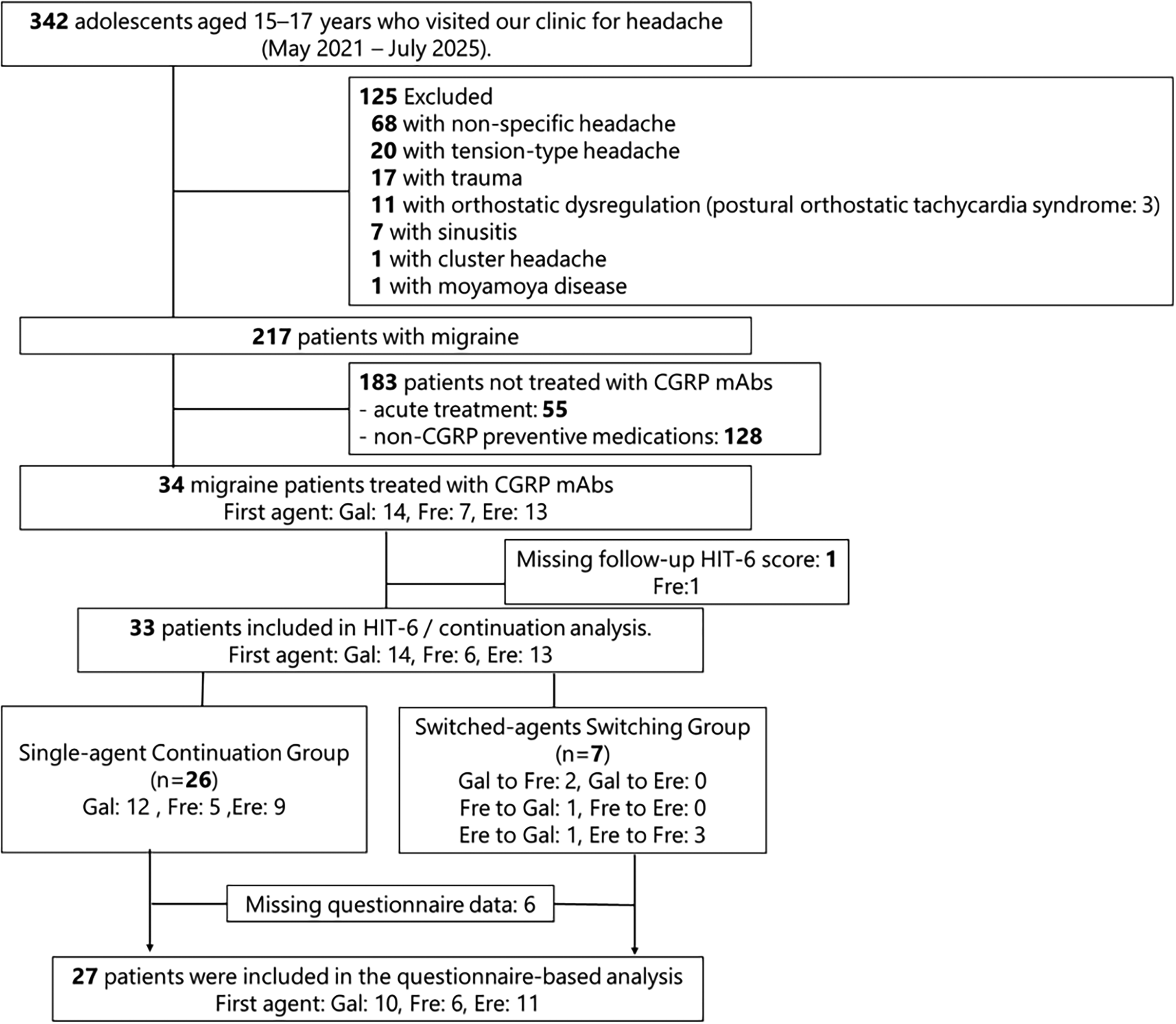
Study design and patient flow. Of the 34 patients included, 33 were eligible for the HIT-6 and continuation analysis, and 27 were included in the questionnaire-based analysis. Among 308 excluded adolescents screened, 17 met criteria for ≥ 2 diagnoses; in the flowchart, each patient was assigned to a single mutually exclusive category according to a prespecified priority order (migraine > cluster headache > tension-type headache > orthostatic dysregulation/postural orthostatic tachycardia syndrome > trauma > sinusitis > non-specific headache). Gal, galcanezumab; Fre, fremanezumab; Ere, erenumab; CGRP mAb, calcitonin gene-related peptide monoclonal antibody
Most patients were 17 years old (21/33; 63.6%) and 20/33 (60.6%) of patients were female (Table 1). Nineteen patients (57.6%) presented with at least one comorbid condition. Before initiating CGRP mAb therapy, the median number of preventive medications used was 2 (IQR = 0–2). In total, 24/33 (72.7%) of patients had a history of preventive medications and triptan use, while 13/24 (54.2%) were classified as triptan responders. The median follow-up duration for the cohort was 153 days (IQR = 65–219 days), with a median of 5 CGRP mAb administrations (IQR = 3–7). Seven patients (21.2%) switched between CGRP mAbs during the follow-up period, primarily due to insufficient efficacy. Only one patient switched prior to the 10–14-week primary assessment window. Of the 33 patients, 20 (60.6%) had follow-up extending beyond 3 months (≥ 84 days). Among the remaining 13 patients (39.4%) with follow-up less than 3 months, eight (61.5%) had already achieved a clinically meaningful HIT-6 improvement (≥ 6-point reduction) prior to their last visit.
Baseline characteristics of the study population.
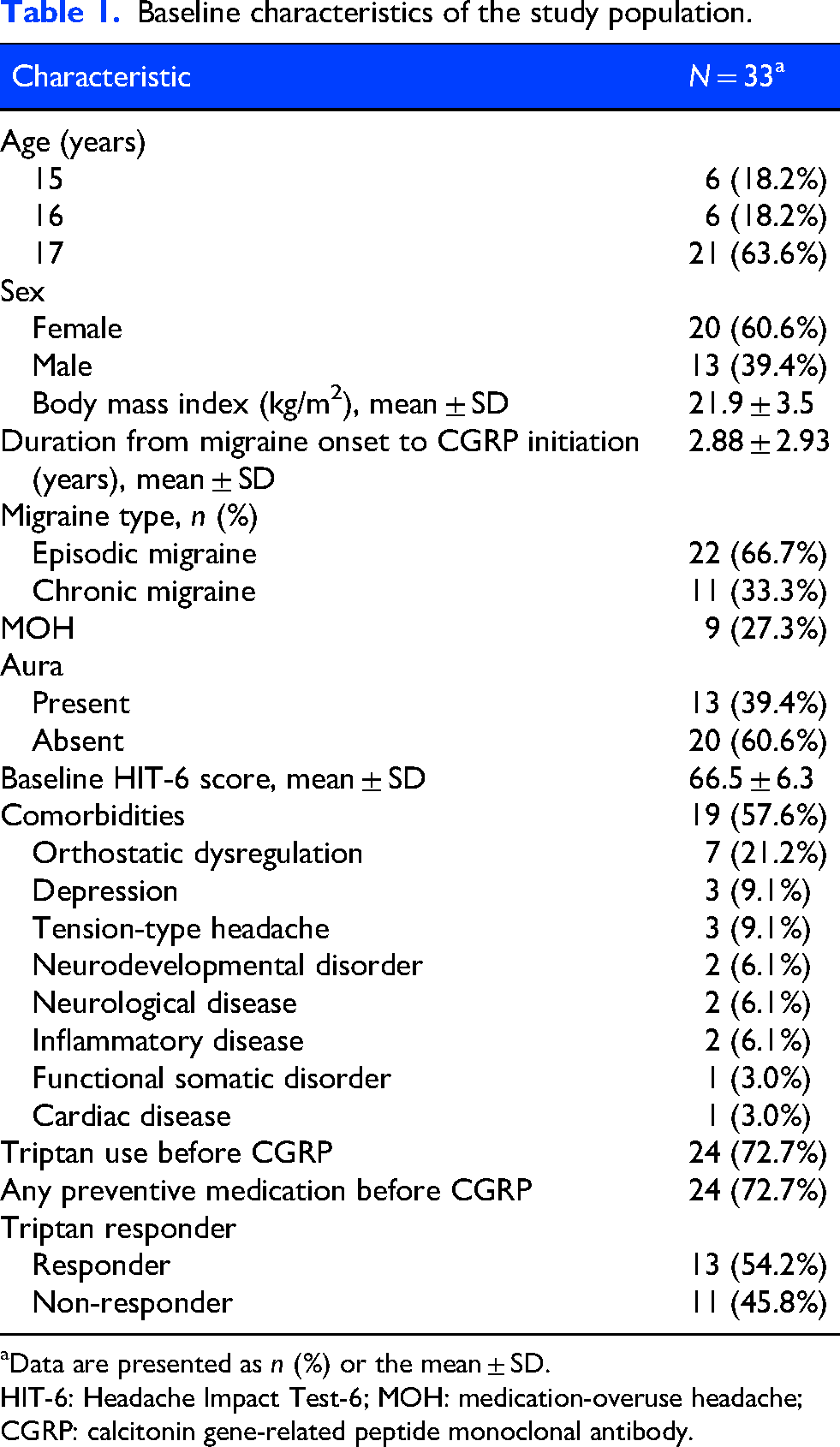
Data are presented as n (%) or the mean ± SD.
HIT-6: Headache Impact Test-6; MOH: medication-overuse headache; CGRP: calcitonin gene-related peptide monoclonal antibody.
During the 14 weeks following CGRP mAb initiation, 24 (72.7%) patients received concomitant preventive medications; some patients received more than one agent, including antidepressants (15; 45.5%), antiepileptic drugs (11; 33.3%), calcium channel blockers (10; 30.3%), and β-blockers (3; 9.1%).
Primary outcome
The time-to-first response, defined as a decrease of at least 6 points in HIT-6 scores from baseline, was analyzed using the Kaplan–Meier method. The cumulative response rate began increasing immediately after treatment, reaching 68.3% (95% CI = 44.6–81.8%) within 3 months (10–14 weeks) (Figure 2). Notably, approximately half of the responders achieved a clinically meaningful improvement as early as 4–6 weeks after the first dose. Among patients who achieved an early response (a ≥ 6-point reduction within 3 months), one (5.0%) experienced a transient drop in response, where the HIT-6 reduction fell below 6 points at certain visits. However, this patient regained meaningful improvement with continued treatment, and no patient returned to their baseline HIT-6 levels by the final follow-up. In sensitivity analyses, censoring patients at the time of CGRP mAb switching yielded a 14-week cumulative response rate of 68.2% (95% CI = 43.1–82.3%). In the conservative worst-case analysis, the response rate was 57.6% (19/33; 95% CI = 39.2–74.5%). Although the latter yielded a lower estimate, both analyses were consistent in direction with the primary analysis.
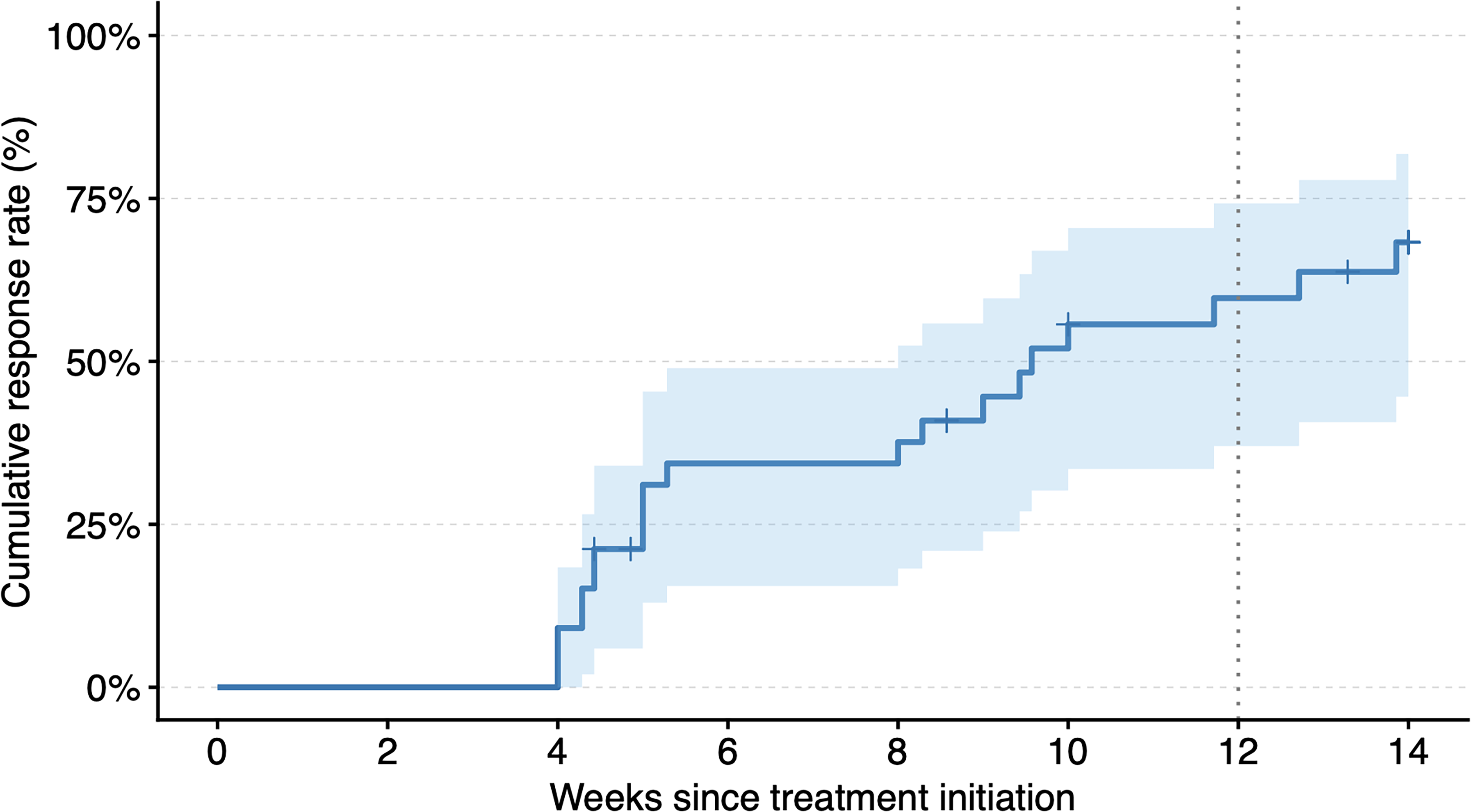
Time-to-first response to calcitonin gene-related peptide monoclonal antibodies (CGRP mAbs). Kaplan–Meier curve of the cumulative probability of first response, defined as a ≥ 6-point reduction in Headache Impact Test-6 score from baseline, among adolescents treated with CGRP mAbs).
Secondary outcomes
HIT-6-based outcomes (n = 33)
Longitudinal changes in HIT-6 scores
Among the 33 patients with longitudinal HIT-6 data, the MMRM, incorporating baseline HIT-6 scores as a covariate, showed a statistically significant reduction in HIT-6 scores following treatment initiation (Figure 3). At 12 weeks, the least-squares mean (LS mean) change from baseline was −9.4 points (95% CI = −14.2 to −4.6; p < 0.001), representing a significant change relative to baseline. This reduction persisted throughout the observation period.
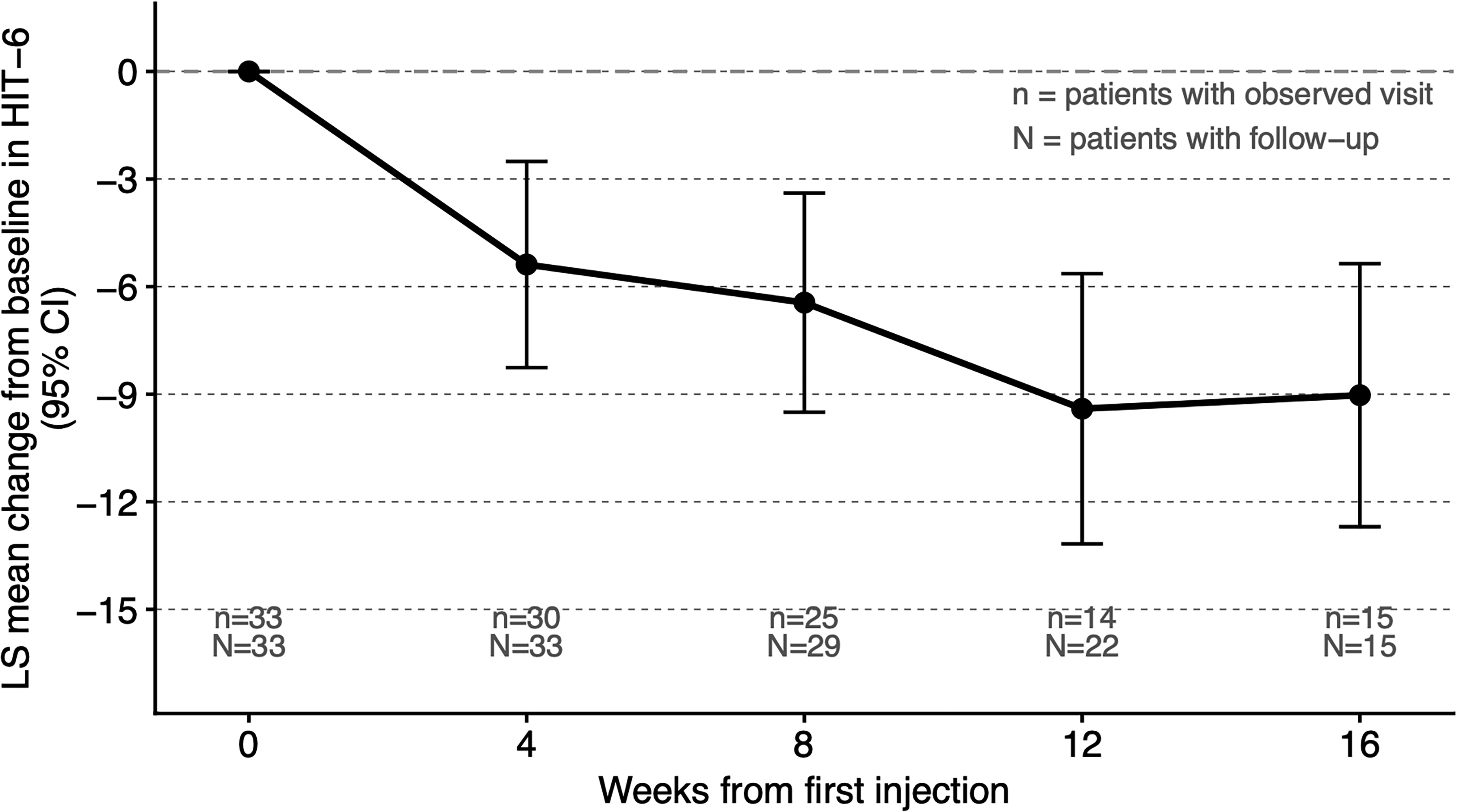
Estimated change in Headache Impact Test-6 (HIT-6) score over time by a mixed-effects model for repeated measures (MMRM). Estimated changes in HIT-6 score from baseline over time derived from a MMRM. Points represent the least-squares mean (LS mean) with 95% confidence intervals (CI). Numbers below the x-axis indicate the number of patients with an observed visit at each time point (n) and the number of patients with follow-up at or beyond each time point (N).
Factors associated with early response
In the same cohort of 33 patients, univariable comparisons were conducted to identify factors associated with early response (≥ 6-point reduction in HIT-6 score within 3 months) (Table 2). No clinical characteristic, such as age, sex, migraine subtype, baseline HIT-6 score or prior medication history, showed statistically significant differences between early responders and non-early responders; exact p-values for all comparisons are presented in Table 2.
Univariate analysis of factors associated with early response to CGRP mAbs.
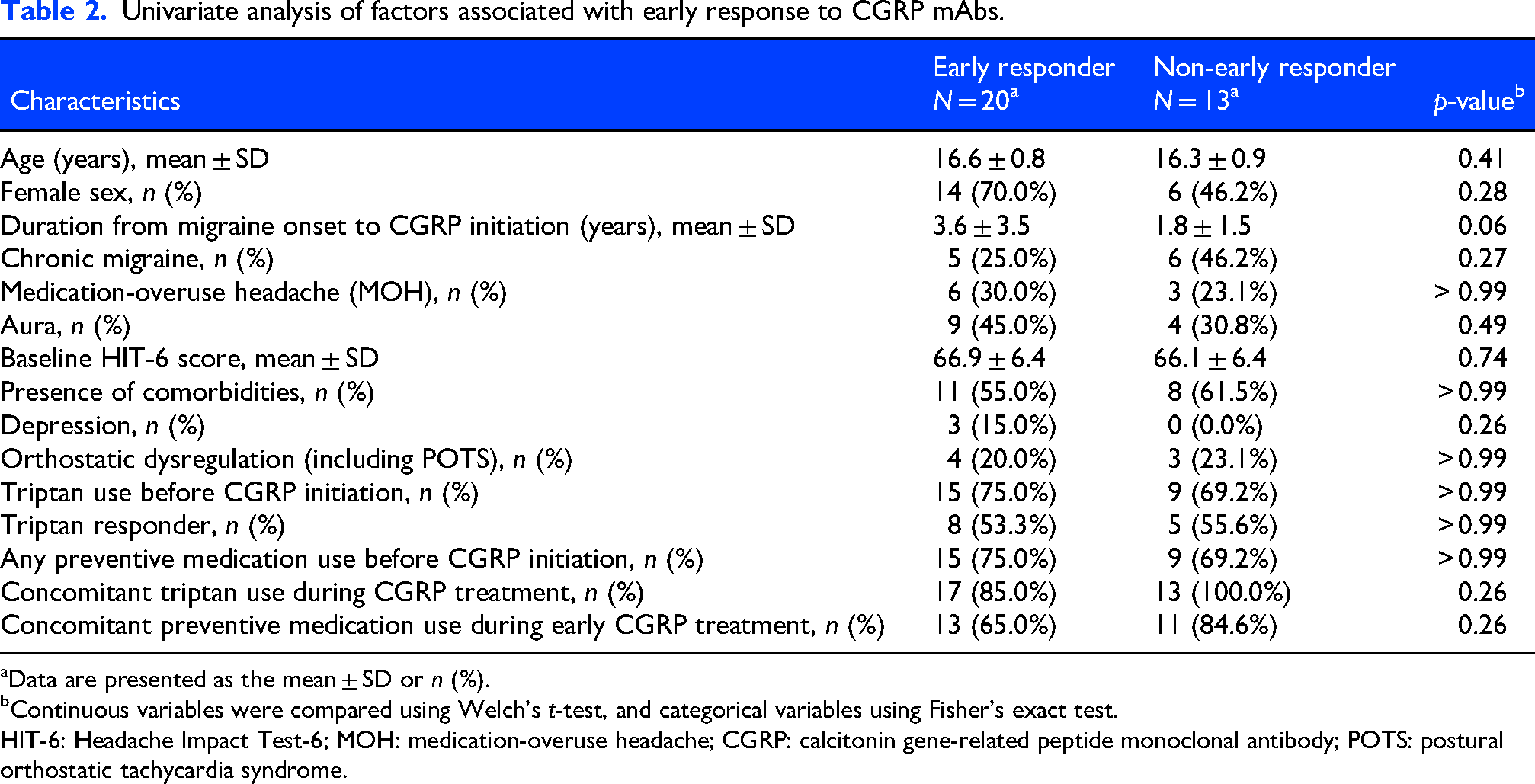
Data are presented as the mean ± SD or n (%).
Continuous variables were compared using Welch's t-test, and categorical variables using Fisher's exact test.
HIT-6: Headache Impact Test-6; MOH: medication-overuse headache; CGRP: calcitonin gene-related peptide monoclonal antibody; POTS: postural orthostatic tachycardia syndrome.
Additionally, early response rates were compared among the three CGRP mAb agents. Early responders accounted for 50.0% (7/14) in the galcanezumab group, 83.3% (5/6) in the fremanezumab group, and 61.5% (8/13) in the erenumab group, with no significant differences among groups (p = 0.50). Among those treated with galcanezumab, early response was analyzed based on whether a loading dose was administered at treatment initiation. None of the patients receiving a single initial injection achieved early response (0/3; 0%), whereas 60% (6/11) of those who received the recommended two-injection loading dose responded early; however, this difference did not reach statistical significance (p = 0.20).
Questionnaire-based outcomes (n = 27)
Daily life disability and goal attainment
Of the 33 eligible patients, 28 were successfully contacted. One patient declined participation, and 27 patients completed the questionnaire (response rate 81.8%). The most frequently reported daily life activity impaired by migraine prior to treatment was “school attendance or concentration in class,” noted by 19 patients (70.4%). This was followed by “tardiness or early departure from school” in five patients (18.5%), and impairment related to preparation for entrance examinations in one patient (3.7%) (Table 3).
Daily activities impaired by migraine before CGRP mAb initiation.
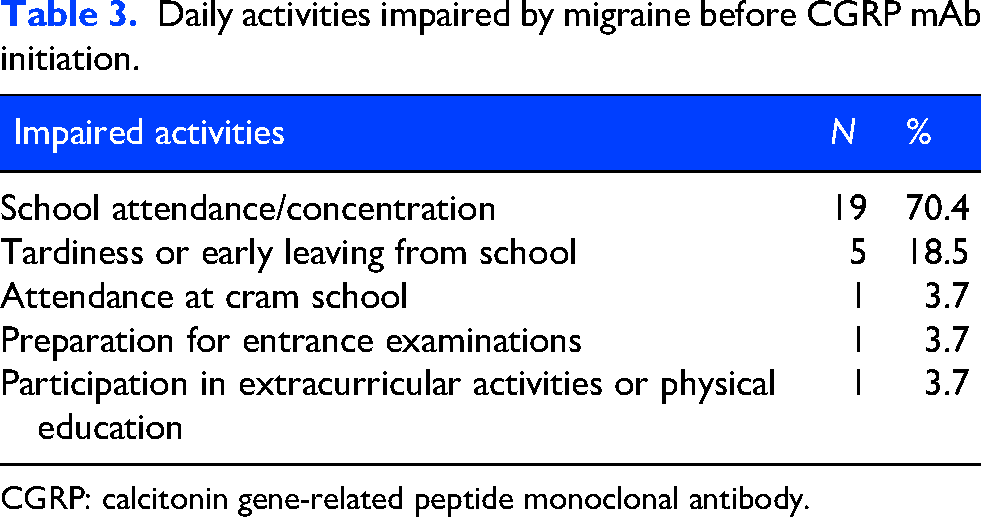
CGRP: calcitonin gene-related peptide monoclonal antibody.
Regarding the attainment of primary treatment goals, 18 patients (66.7%) reported their goals were “almost achieved,” while six patients (22.2%) reported “partially achieved,” yielding an overall goal attainment rate of 88.9% (24/27). In contrast, three patients (11.1%) reported that their goals were not achieved (Table 4). Patient-reported headache improvement categories and PGIC responses are shown in the Supplementary material (Figures S1 and S2, respectively).
Achievement of the primary goal after CGRP mAb treatment.
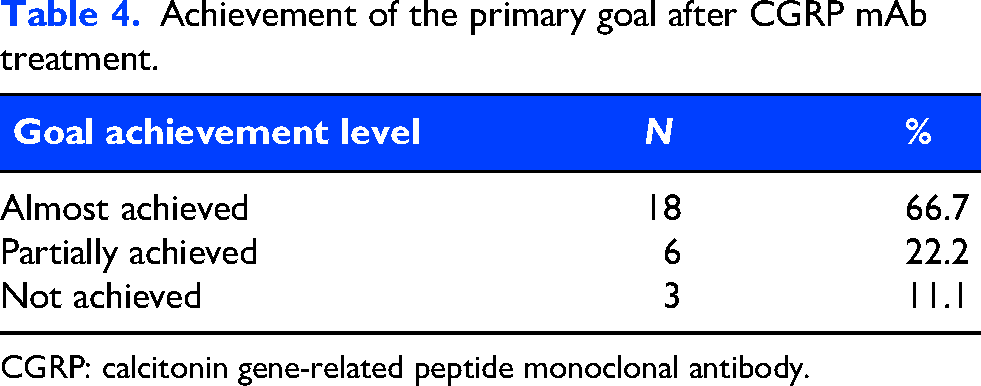
CGRP: calcitonin gene-related peptide monoclonal antibody.
Safety
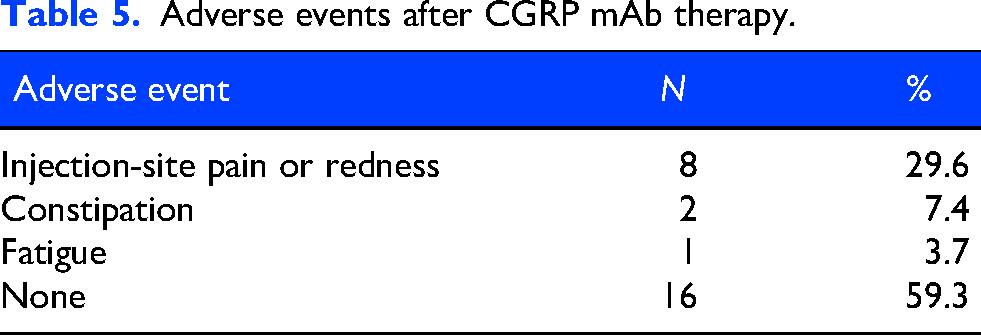
Adverse events were observed in 11/27 (40.7%) of patients (Table 5), whereas 16/27 (59.3%) reported none during CGRP mAb therapy. The most common adverse event was injection-site reactions (pain or redness), reported in eight patients (29.6%), followed by constipation in two patients (7.4%). According to patient-reported questionnaires and physician assessments documented in the medical records, all adverse events were mild and did not substantially impact daily activities. No patients discontinued CGRP mAb therapy or switched CGRP mAbs due to adverse events throughout the observation period.
Adverse events after CGRP mAb therapy.
Discussion
This single-center retrospective study evaluated the real-world effectiveness of CGRP mAb therapy in Japanese adolescents aged 15–17 years with migraine. Clinically meaningful improvement in the HIT-6 scores was observed within the 10–14 weeks assessment window, with benefits sustained over follow-up. Adverse events were mild and did not require treatment discontinuation, supporting the tolerability of CGRP mAbs in this age group. However, because this was an uncontrolled study with a small sample size, causal inference is not possible, and the findings should be interpreted cautiously. Within these constraints, meaningful functional improvement appeared achievable earlier than the 3–6 months recommended in adult guidelines. These results may be informative for clinicians considering CGRP mAb therapy in adolescents, a population for which controlled evidence remains limited.
A plausible mechanism for the observed improvement in HIT-6 scores may involve age-related migraine biology, such as heightened dependence on CGRP and increased neuroplasticity in central sensitization. CGRP mAbs are considered to exert their effects by inhibiting CGRP signaling within the trigeminovascular system, thereby attenuating peripheral and central sensitization. 3 Adolescents may exhibit less well-established maladaptive neuroplastic changes (“pain memory”) and fewer cumulative comorbidities or age-associated vascular alterations than adults,3,22 potentially contributing to the earlier functional improvements observed in this cohort. Additionally, non-biological factors, including care-seeking patterns, concurrent educational support, and expectation-driven responses at treatment initiation, may have contributed to observed outcomes.
Randomized controlled evidence in pediatric populations has recently demonstrated that CGRP mAbs significantly reduce migraine frequency compared with placebo in children and adolescents. 23 However, these trials primarily evaluated migraine days rather than functional outcomes. Evidence regarding the time course of functional improvement has been more extensively characterized in adult populations. In adults, clinically meaningful improvements in HIT-6 tend to occur gradually, often requiring at least 12 weeks to approach maximal benefit: phase III fremanezumab trials showed 6–7 point improvement at week 12, 19 while LIBERTY reported −3.7 points at week 12 and −6.4 points at week 16, with further incremental gains.5,7 Real-world open-label data in adults suggest sustained benefit contingent upon ongoing therapy rather than short induction courses. 6 Hence, direct comparisons between our findings and adult studies are constrained by differences in study populations, follow-up schedules, missing-data patterns, and analytic approaches. Therefore, variations observed between different age groups should be interpreted as hypothesis-generating rather than confirmatory. Within these limitations, the LS mean HIT-6 change at 12 weeks (–9.4 points) in our adolescent cohort represented a statistically significant change from baseline. Meta-regression analyses have reported larger treatment effects in younger individuals. 20 Pediatric real-world data reveal a substantial or moderate response in 70% at initial follow-up (mean 2.7 months), with functional improvement in 62%. 10 However, elevated placebo responses in pediatric migraine populations 24 warrant prospective controlled studies to distinguish pharmacologic efficacy from non-specific influences. Age-related variations in interictal CGRP activity may also underlie response heterogeneity.25,26
We further explored whether an early clinically meaningful HIT-6 response was associated with previous triptan responsiveness; however, univariable analyses did not identify a significant association. Most pediatric triptan trials have focused on acute efficacy as their primary outcome, leaving the relationship between acute triptan response and longer-term functional outcomes unclear.27–29 Similarly, no significant difference in early response rates was observed between those with and without concomitant preventive medication use during CGRP treatment (Table 2). However, as with other explored clinical characteristics, these findings should be considered inconclusive given the limited sample size.
A key strength of the present study lies in its focus on functional improvement, rather than solely on headache-frequency metrics. We estimated the time required to achieve a clinically meaningful HIT-6 improvement using longitudinal data from routine clinical records. These findings were supplemented by adolescent-relevant patient-reported outcomes that addressed school-life impairment, treatment-goal attainment, and adverse events.5,30 This approach may be particularly relevant in adolescence, when migraine-related impairment can disrupt academic and social activities regardless of monthly migraine or headache days.4,31 However, these questionnaire-based outcomes were collected retrospectively after follow-up completion and may be subject to recall bias, warranting cautious interpretation. Given this concern, the Pediatric Migraine Disability Assessment (PedMIDAS), which requires detailed retrospective recall of specific activity-loss days and is therefore more susceptible to this bias, was not administered in the present study.
Persistent migraine symptoms in adolescents can lead to school absences and activity avoidance, potentially resulting in persistent limitation of social participation and future opportunities.32,33 The unpredictability of migraine attacks may also impose psychological burdens, including loneliness and irritability. 34 In this cohort, the impact on school life was frequently reported as a major burden, while treatment-goal attainment was high, suggesting that CGRP mAbs may be relevant to addressing issues particularly salient in adolescence. Early functional improvement, if confirmed in controlled studies, may imply an opportunity to intervene before functional impairment becomes entrenched, with potential implications for preventing further chronicity and refractoriness.
Adverse events were reported in 40.7% of patients, all mild and not precluding continued treatment, consistent with prior pediatric findings. 10 Higher rates reported in some adult studies19,35–37 may reflect differences in data collection methods because systematically solicited reporting tends to produce higher event rates than routine documentation. Notably, even with questionnaire-based assessments, approximately 60% of participants reported no adverse events, supporting the tolerability of CGRP mAbs during adolescence.
Strengths and limitations
Despite its single-center design, this study was conducted in a specialized clinical setting where adolescents with migraine were systematically evaluated and treated, likely supporting consistency in treatment initiation, follow-up decisions, and assessment procedures. Given the limited evidence available for adolescent populations, we prioritized functional recovery beyond reductions in headache frequency by integrating longitudinal HIT-6 assessments with patient-reported outcomes, thus yielding real-world descriptive data on treatment-associated outcomes and tolerability.
Several limitations warrant consideration. First, as a retrospective observational study with a small sample size and without a comparator group, distinguishing treatment effects from the natural course of illness or placebo-related effects was not possible, limiting causal inference. Second, the HIT-6 was developed and validated primarily in adult populations, and its psychometric properties in adolescents remain insufficiently established. Third, variations in visit intervals and assessment timing within routine practice may have contributed to measurement bias in HIT-6 trajectories. In particular, discrepancies between the number of patients with follow-up beyond 12 weeks (n = 22; 66.7%) and those with an observed visit at the 12-week time point (n = 14; 42.4%) reflect the impact of visit timing variability on longitudinal analyses such as MMRM. Although the MMRM incorporated all available data under a missing-at-random assumption, findings at this key time point should be interpreted with caution. Fourth, although monthly migraine day data were collected as part of routine practice, reliable documentation was difficult to obtain due to inconsistent diary completion, precluding its inclusion as an outcome measure. This limits direct comparison with existing CGRP mAb trials that predominantly report headache frequency as a primary endpoint. Fifth, detailed patient-reported outcomes and adverse event data were only accessible for questionnaire respondents, introducing potential selection bias; additionally, retrospective collection of these outcomes may be affected by recall bias, warranting cautious interpretation. Sixth, because CGRP mAb therapy was initiated based on clinical judgement rather than a standardized protocol, indication bias is an inherent limitation of this real-world observational study. Patients who received CGRP mAbs may represent a more severely affected subgroup, which could influence the generalizability of the findings. Furthermore, because some patients declined treatment due to financial or injection-related concerns, those who initiated therapy may differ systematically from those who did not, potentially contributing to selection bias. Seventh, analyses of associated factors were exploratory and limited to univariable models due to sample-size constraints. Given the limited sample size and potential for residual confounding, all findings from these analyses should be considered inconclusive and require validation in larger prospective studies.
Conclusions
CGRP mAb therapy in adolescents with migraine was associated with clinically meaningful functional improvement before the conventional 3-month evaluation period and was generally well tolerated. Considering the substantial impact of migraine on school performance and social participation during adolescence, treatment outcomes should be assessed not only by headache-frequency metrics but also by functional recovery. These findings warrant validation through prospective controlled studies. When early functional recovery is prioritized, CGRP mAb therapy may facilitate shared decision-making for adolescents with migraine.
Clinical implications
CGRP monoclonal antibodies were associated with improvement in HIT-6 scores in adolescents with migraine.
Early clinically meaningful improvement was observed within about 3 months.
CGRP mAbs in adolescents with migraine may support participation in school and social activities during adolescence.
Supplemental Material
sj-docx-1-cep-10.1177_03331024261461634 - Supplemental material for Early and clinically meaningful functional improvement following CGRP monoclonal antibodies in adolescents with migraine: A real-world retrospective study
Supplemental material, sj-docx-1-cep-10.1177_03331024261461634 for Early and clinically meaningful functional improvement following CGRP monoclonal antibodies in adolescents with migraine: A real-world retrospective study by Misaki Kamogawa, Masakazu Higurashi, Akito Oshima, Norimichi Higurashi and Naoki Ikegaya in Cephalalgia
Supplemental Material
sj-docx-2-cep-10.1177_03331024261461634 - Supplemental material for Early and clinically meaningful functional improvement following CGRP monoclonal antibodies in adolescents with migraine: A real-world retrospective study
Supplemental material, sj-docx-2-cep-10.1177_03331024261461634 for Early and clinically meaningful functional improvement following CGRP monoclonal antibodies in adolescents with migraine: A real-world retrospective study by Misaki Kamogawa, Masakazu Higurashi, Akito Oshima, Norimichi Higurashi and Naoki Ikegaya in Cephalalgia
Footnotes
Ethical considerations
This study was approved by the Ethics Committee of Yokohama City University Graduate School of Medicine (approval number: F260200006). For analyses of existing medical record data, patients and their guardians were provided the opportunity to opt out.
Author contributions
MK, MH, and AO designed and conceptualized the study. MK and MH acquired the data. All authors contributed to data analysis and interpretation. MK, NI, and AO drafted the manuscript. All authors critically revised the manuscript and approved the final version submitted for publication.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Consent to participate
Informed consent was obtained from patients and their guardians for the questionnaire survey.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets analyzed during the current study are not publicly available due to ethical and privacy restrictions but are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.