
Abstract
Aim
In view of limited evidence-based acute treatments for spontaneous vertigo in vestibular migraine, this real-world cohort study assessed the effectiveness of rimegepant for acute vestibular migraine-related vertigo and factors associated with treatment response.
Methods
Clinical data were retrospectively collected from 86 patients with documented vestibular migraine treated with rimegepant 75 mg orally disintegrating tablets for acute attacks at a tertiary referral hospital between March and November 2025. Predictors of 2-h vertigo relief, defined as improvement from moderate or severe baseline vertigo to mild or no vertigo on an 11-point numeric rating scale, and 2-h numeric rating scale scores were analyzed using regression models accounting for within-patient clustering of attacks.
Results
Among 86 patients, 192 of 252 treated vertigo episodes (76.2%) achieved vertigo relief. At 2 h after dosing, the mean change in vertigo numeric rating scale score was −4.44 (95% CI, −4.65 to −4.23). In adjusted models, age younger than 60 years (OR, 3.45 [95% CI, 1.15 to 10.31]; P = 0.027) and lower baseline numeric rating scale (OR per 1-point increase, 0.56 [95% CI, 0.36 to 0.86]; P = 0.008) were associated with higher odds of vertigo relief. Younger age, lower baseline numeric rating scale score, and better hearing (β, −1.14 [95% CI, −2.02 to −0.26]; P = 0.013) were also associated with lower 2-h numeric rating scale scores.
Conclusion
Rimegepant was effective for vertigo episodes in patients with vestibular migraine, and treatment responsiveness was closely associated with age, baseline vertigo severity, and auditory function. These findings support the early initiation of rimegepant for acute treatment of vestibular migraine, rather than delaying treatment until vertigo exacerbation.
This is a visual representation of the abstract.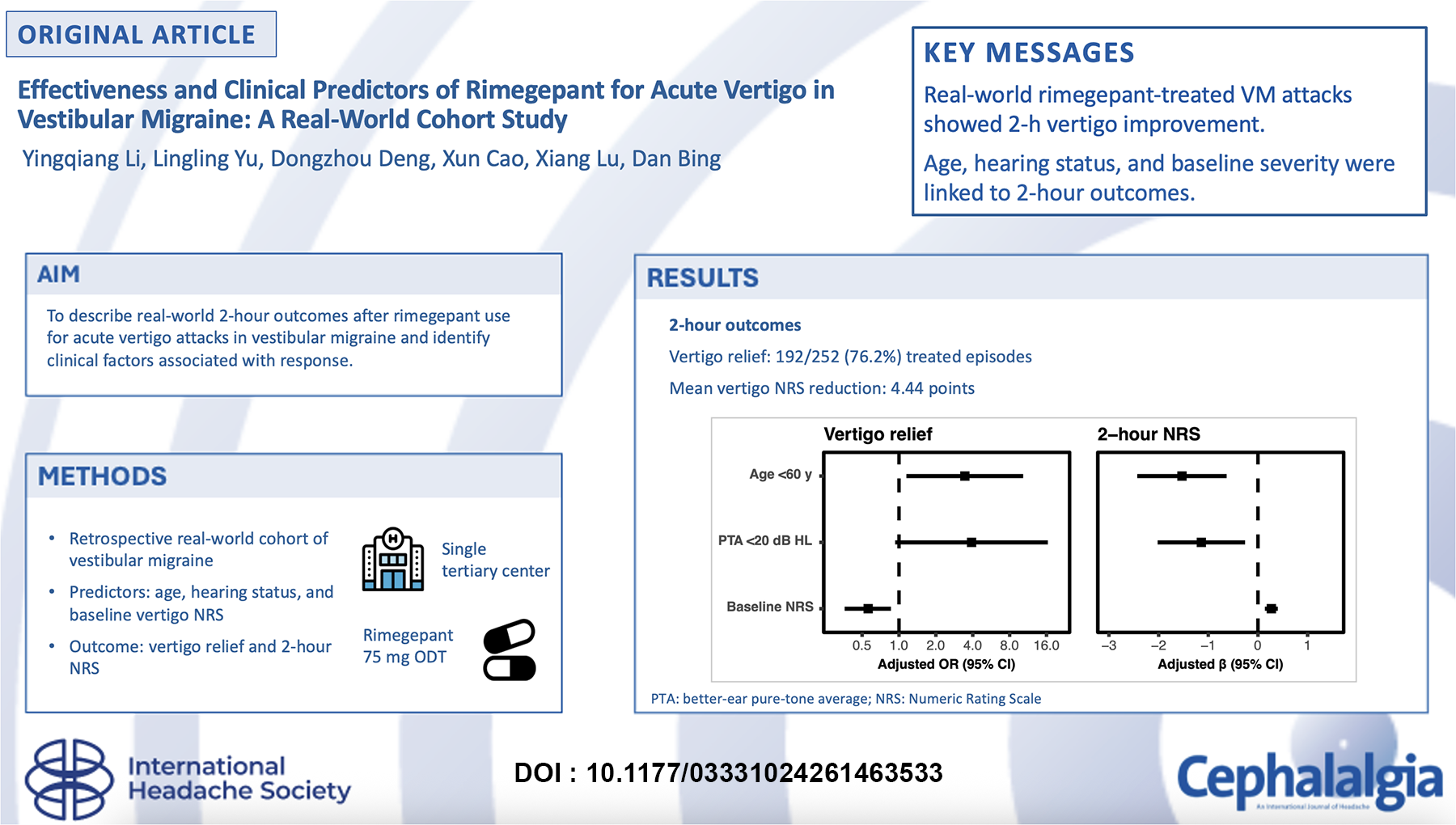
Introduction
Vestibular migraine (VM) is a prevalent episodic vestibular disorder, characterized by recurrent attacks of spontaneous or provoked vertigo or dizziness of at least moderate intensity, frequently accompanied by migrainous features and not better accounted for by alternative diagnoses. 1 As a leading cause of recurrent episodic vertigo, VM affects 1% to 2.7% of the general population annually,2,3 accounting for approximately 11% of cases in specialized dizziness clinics and 13% in headache clinics.4,5
Vestibular migraine presents substantial clinical challenges. Acute attacks are often highly disabling and patients frequently seek emergency care for rapid symptom relief. The unpredictable nature of these acute episodes often causes profound fear and anxiety among patients. Routine acute management heavily relies on symptomatic therapies used for acute peripheral vertigo, including vestibular suppressants, which have notable limitations due to adverse effects. 6 Alternative emergency medication is largely derived from experience in migraine management. A Cochrane review identified only two placebo-controlled randomized clinical trials (RCTs) evaluating triptans (rizatriptan and zolmitriptan) for acute VM, concluding with very low-certainty evidence that they provide little to no difference in vertigo improvement within two hours. 7 A recent robust RCT of oral rizatriptan (10 mg) similarly demonstrated no significant benefit over placebo in relieving acute vertigo, unsteadiness, or headache at the 1-h primary endpoint. 8 Preclinical murine models further support these clinical findings, revealing that triptans are ineffective in blocking calcitonin gene-related peptide (CGRP)-induced motion sensitivity and nausea surrogates. 9 Collectively, current evidence does not support triptans as a reliably effective therapy for acute vestibular symptoms in VM. This reinforces the need to evaluate alternative mechanism-based options.
CGRP plays a central role in the pathophysiology of migraine and vestibular disorders, and is a well-established therapeutic target for migraine. Rimegepant, an oral CGRP receptor antagonist, has demonstrated efficacy and favorable tolerability in the acute treatment of migraine. 10 It has also shown benefit in improving vertigo symptoms in preventive treatment of VM. 11 Emerging evidence further supports the important role of CGRP in the vestibular pathways, with CGRP-immunoreactive terminals present in the human vestibular periphery,12,13 and CGRP-associated sensitization observed within the vestibular nucleus in a chronic migraine model. 14 These findings provide the biological plausibility for CGRP antagonism as a rational strategy for managing vestibular symptoms in VM. Notably, the recently released Chinese clinical practice guideline 15 for VM suggests gepants as a promising option while emphasizing the lack of VM-specific clinical evidence.
VM exhibits significant clinical heterogeneity. Patients often present with variable attack severities and prevalent comorbidities, such as anxiety, depression, and sleep disturbances, which may influence treatment response. Conventional RCTs often underrepresent such complexity. Real-world studies are therefore particularly informative for acute VM research, as they better capture clinical variability, comorbidities, and attack severity. As such, we conducted a real-world cohort study to evaluate the effectiveness of rimegepant 75 mg ODT in the acute treatment of vertigo attacks in Chinese patients with VM and to identify prognostic factors associated with treatment response. By addressing this evidence gap, this study seeks to inform and optimize acute-phase management strategies for VM.
Methods
Study design, participants and treatment
Clinical data were extracted from the Hospital Information System (HIS) of the study hospital (Figure 1). The study was approved by the Institutional Review Board of Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology (Approval No. TJ-IRB202602006). The requirement for informed consent was waived because of the retrospective nature of the study and the use of de-identified clinical data. This study is reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement.
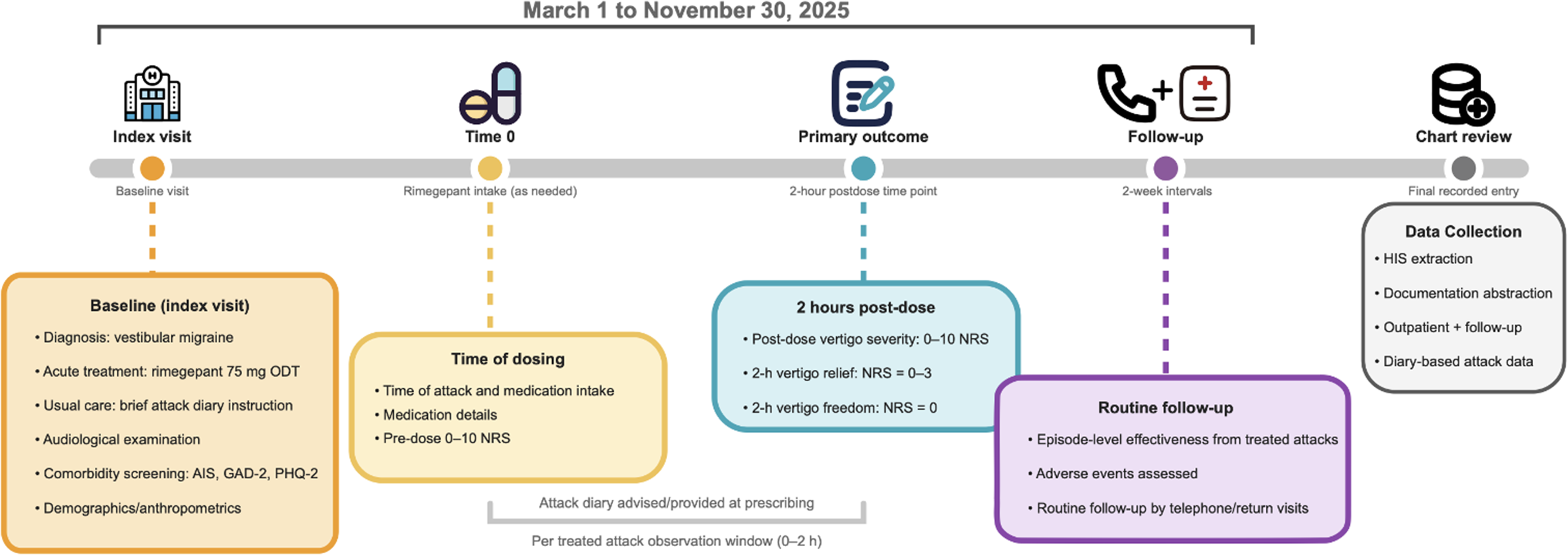
Study design and data-collection time points.
Inclusion criteria were: i) individuals aged 18 years or older, ii) diagnosis of VM based on the consensus criteria of the Bárány Society and the International Headache Society (IHS)1,16; iii) had treatment-response follow-up data available; iv) no prior use of anti-CGRP drugs; v) with untreated vertigo attacks exceeding 2 h; vi) receipt of rimegepant, 75 mg orally disintegrating tablet, prescribed as needed for the acute treatment of vestibular vertigo attacks.
Exclusion criteria were: (i) concomitant diagnosis of other episodic vestibular syndromes (e.g., Ménière disease, benign paroxysmal positional vertigo, acute vestibular neuritis, vestibular paroxysmia); (ii) missing baseline audiogram or questionnaire data. For episode-level analyses, treated attacks were additionally excluded if baseline or 2-h NRS was missing or if baseline NRS was <4; participants were excluded if they had no eligible treated attacks.
In routine clinical practice, patients prescribed rimegepant were instructed to self-administer one 75 mg orally disintegrating tablet when vertigo was moderate or severe, without taking more than one tablet within 24 h. 17 Because rimegepant had only recently been introduced in clinical practice, clinicians explained the rationale for its use in vertigo episodes and asked patients to keep a diary for treated episodes. Trained clinic staff provided guidance on diary completion when needed. The diary captured the timing of vertigo onset and medication intake, vertigo intensity at dosing and 2 h after dosing, accompanying symptoms, perceived symptom change, recurrence of vertigo attacks, medication adherence, and potential adverse events. Diary information was obtained during routine follow-up outpatient visits or telephone contacts by clinic staff, usually at approximately two-week intervals when clinically feasible. These activities were part of usual clinical care to evaluate effectiveness and safety and guide treatment decisions.
Outcomes
Vertigo intensity was self-reported using an 11-point numeric rating scale (NRS), ranging from 0 for no vertigo to 10 for the worst imaginable vertigo. 18 NRS scores were categorized as none (0), mild (1–3), moderate (4–6), or severe (7–10).19,20 Based on this NRS categorization, the primary outcome was 2-h vertigo relief, defined as improvement from moderate or severe vertigo at dosing to mild or no vertigo 2 h post-dose. 7 Vertigo freedom was evaluated as a secondary outcome and was defined as complete absence of vertigo at 2 h, corresponding to an NRS score of 0.
Baseline measures
Baseline demographic and anthropometric characteristics were obtained at the index visit using standardized clinical measurements and documentation. Age was recorded in years and additionally classified into two groups (<60 and ≥60 years). Sex was recorded as male or female. BMI was calculated from height and weight measured at the first visit and categorized as <25 and ≥25 kg/m2. 21 Sleep disturbance and symptoms of anxiety and depression are common in patients with vestibular migraine and have been associated with greater dizziness-related burden and reduced treatment response, making them potential confounders when estimating treatment effectiveness.22–24 At the study institution, patients routinely completed brief screening questionnaires in validated Chinese versions to assess these comorbidities, including the Athens Insomnia Scale (AIS),25,26 the 2-item Generalized Anxiety Disorder scale (GAD-2),27,28 and the 2-item Patient Health Questionnaire (PHQ-2).29,30 For analysis, scores were categorized as AIS less than 8 vs 8 or greater, 25 GAD-2 less than 3 vs 3 or greater, 27 and PHQ-2 less than 3 vs 3 or greater, 29 consistent with established screening thresholds. These variables were included as covariates in adjusted models.
Audiology assessment
As part of routine clinical evaluation for vestibular migraine at the study institution, patients underwent audiologic assessment before treatment. Pure-tone audiometry was performed in sound-treated booths using a MADSEN Conera clinical audiometer (Otometrics, Taastrup, Denmark) with TDH-39 supra-aural earphones for air-conduction testing and a B-71 bone vibrator for bone-conduction testing. A brief otoscopic examination and a screening tympanogram (MADSEN Zodiac 901, Otometrics) were obtained to identify obstructing cerumen and middle-ear disease. Hearing thresholds were measured using pure-tone air-conduction (0.5, 1, 2, 3, 4, 6, and 8 kHz) and bone-conduction (0.5, 2, and 4 kHz) audiometry, following a modified Hughson–Westlake procedure. 31 All technicians underwent centralized training and certification at the study institution/site. Ambient sound levels were monitored daily at each test site and were required to meet the permissible ambient-noise limits specified in GB/T 16296.1-2018. 32 Hearing loss was defined by the World Health Organization better-ear criterion as a better-ear 4-frequency pure-tone average (PTA; 0.5, 1, 2, and 4 kHz) of ≥20 dB HL. 33 Hearing was analyzed both categorically using this threshold and continuously as the better-ear PTA (dB HL).
Statistical analysis
Baseline characteristics were summarized overall and by first-episode vertigo relief status. Categorical variables are presented as number (percentage) and continuous variables as median (IQR). Between-group comparisons used the Mann-Whitney U test for continuous variables and the Pearson χ2 test or Fisher exact test for categorical variables, as appropriate. Change in vertigo NRS from the pre-dose baseline to 2 h was estimated using a linear mixed-effects model with time as a fixed effect and random intercepts for participant and for episode nested within participant to account for repeated treated episodes and paired measurements within episodes. Model-based estimated marginal means at baseline and 2 h and the mean difference (2 h minus baseline) with 95% confidence intervals (CIs) were obtained from model contrasts.
Associations between clinical characteristics and episode-level outcomes were evaluated using models that accounted for clustering of treatment episodes within participants. Vertigo relief and vertigo freedom were analyzed using population-averaged generalized estimating equation (GEE) logistic regression with an exchangeable working correlation structure and robust standard errors, with results reported as odds ratios (ORs) and 95% CIs. 34 Two-hour NRS was analyzed using a linear mixed-effects model (LMM) with a participant-level random intercept, with results reported as mean differences and 95% CIs. 35 Multivariable models were adjusted for prespecified covariates (age, sex, insomnia, depression, and anxiety). Potential nonlinear associations of age and better-ear PTA with vertigo relief and 2-h NRS were evaluated using restricted cubic splines (RCS), and Wald tests were used to assess the nonlinear component.
Analyses were conducted using R, version 4.3.3 (R Foundation for Statistical Computing). Sensitivity analyses restricted the analytic sample to the first treated episode per participant and additionally evaluated vertigo remission (2-h NRS score of 0–1) as an additional outcome (Supplementary eMethods). Complete-case analysis was used for model covariates and outcomes because missing data were limited after eligibility screening, and imputation was not performed. All tests were 2-sided, and P < 0.05 was considered statistically significant.
Results
Baseline characteristics of included patients
Among 301 VM patients prescribed rimegepant, 115 adults were eligible for acute-use screening. According to the inclusion and exclusion criteria, the final study population comprised 86 patients (Figure 2, Supplementary Table S1) with a median age of 48.0 years (IQR, 35.2 to 59.0 years) (Table 1).
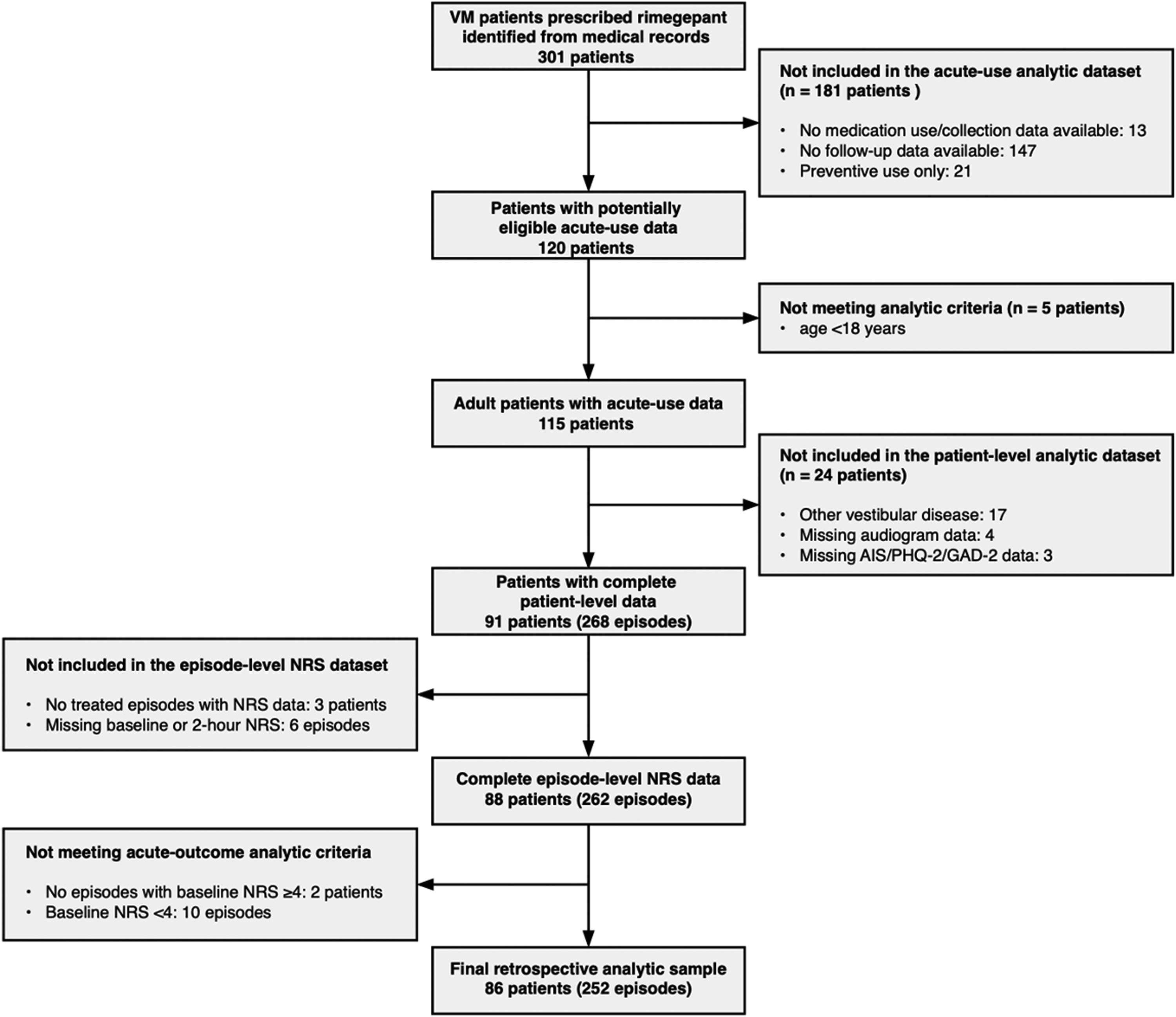
Flowchart of patient selection, exclusions, and final analytic sample.
Baseline characteristics of patients according to occurrence of 2-h vertigo relief in first treated episode
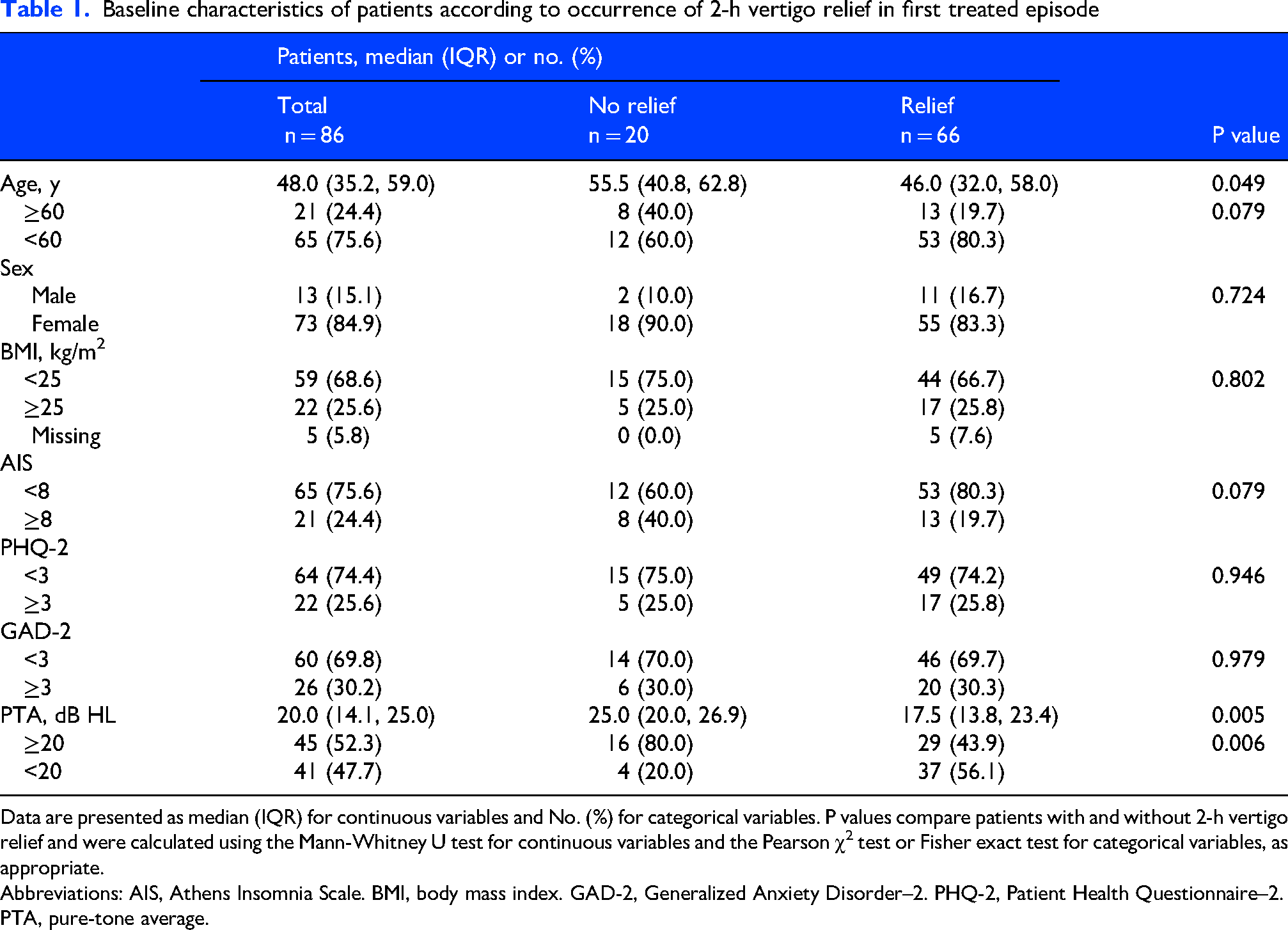
Data are presented as median (IQR) for continuous variables and No. (%) for categorical variables. P values compare patients with and without 2-h vertigo relief and were calculated using the Mann-Whitney U test for continuous variables and the Pearson χ2 test or Fisher exact test for categorical variables, as appropriate.
Abbreviations: AIS, Athens Insomnia Scale. BMI, body mass index. GAD-2, Generalized Anxiety Disorder–2. PHQ-2, Patient Health Questionnaire–2. PTA, pure-tone average.
Table 1 summarizes baseline characteristics according to the occurrence of 2-h vertigo relief in the first treated episode. Overall, 66 patients achieved vertigo relief, whereas 20 did not. Patients with vertigo relief were younger than those without relief, with a median age difference of 9.5 years (46.0 vs 55.5 years). The proportion of patients aged ≥60 years was also lower in the relief group than in the non-relief group (19.7% vs 40.0%), suggesting less favorable response among older patients. Hearing status also differed between groups. Patients with vertigo relief had a lower better-ear PTA than those without relief, with a median difference of 7.5 dB HL (17.5 vs 25.0 dB HL). Consistently, PTA ≥20 dB HL was less common among patients with vertigo relief than among those without relief (43.9% vs 80.0%). Sex, BMI, insomnia symptoms, depressive symptoms, and anxiety symptoms were broadly similar between the two groups.
NRS scores of vertigo improved post-dose
Among 252 acute vertigo episodes in 86 patients with VM (Figure 3), model-estimated mean vertigo NRS scores were 6.70 pre-dose and 2.26 at 2 h after rimegepant 75 mg ODT, corresponding to a mean change of −4.44 points (95% CI, −4.65 to −4.23). Pain intensity showed a similar reduction in pain-associated episodes, with a mean change of −4.25 points (Supplementary Figure S1). No adverse events related to rimegepant were documented.
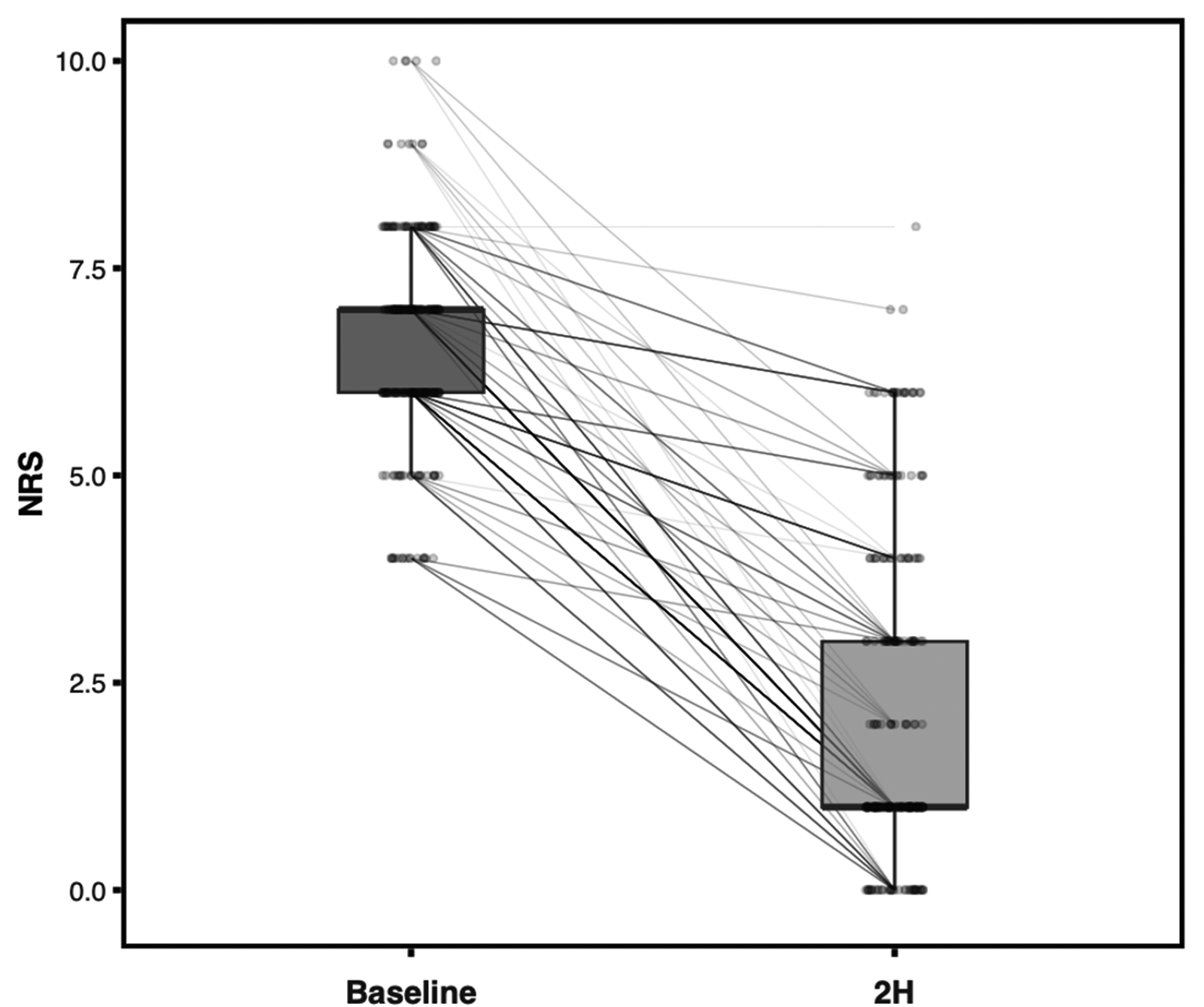
Change in vertigo intensity from baseline to 2 h after rimegepant treatment.
Clinical factors associated with treatment outcomes
Table 2 presents results from univariable and multivariable models, including GEE logistic regression for 2-h vertigo relief and a linear mixed-effects model for 2-h NRS. Overall, 2-h vertigo relief occurred in 192 of 252 treated episodes (76.2%). Across treated episodes, younger age and lower baseline vertigo severity were associated with more favorable outcomes after rimegepant treatment. After adjustment for sex, insomnia, anxiety, and depression, patients aged <60 years had more than threefold higher odds of vertigo relief than those aged ≥60 years (OR, 3.45 [95% CI, 1.15 to 10.31]). In contrast, greater baseline vertigo severity was associated with a lower likelihood of relief. Each 1-point increase in baseline NRS corresponded to 44% lower odds of vertigo relief (OR, 0.56 [95% CI, 0.36 to 0.86]). Similar patterns were observed for residual vertigo intensity at 2 h. Patients aged <60 years had lower 2-h NRS scores than those aged ≥60 years, whereas higher baseline NRS was associated with greater residual symptom burden at 2 h. Better-ear PTA <20 dB HL was also associated with lower residual vertigo intensity after adjustment, corresponding to an estimated 1.14-point lower 2-h NRS score compared with PTA ≥20 dB HL (β, −1.14 [95% CI, −2.02 to −0.26]). Results were similar in analyses restricted to the first episode per patient (Supplementary Table S2). Restricted cubic spline analyses suggested nonlinear associations for better-ear PTA with both vertigo relief and 2-h NRS, with the lowest odds of relief and the highest 2-h NRS observed at intermediate PTA values (Figure 4).
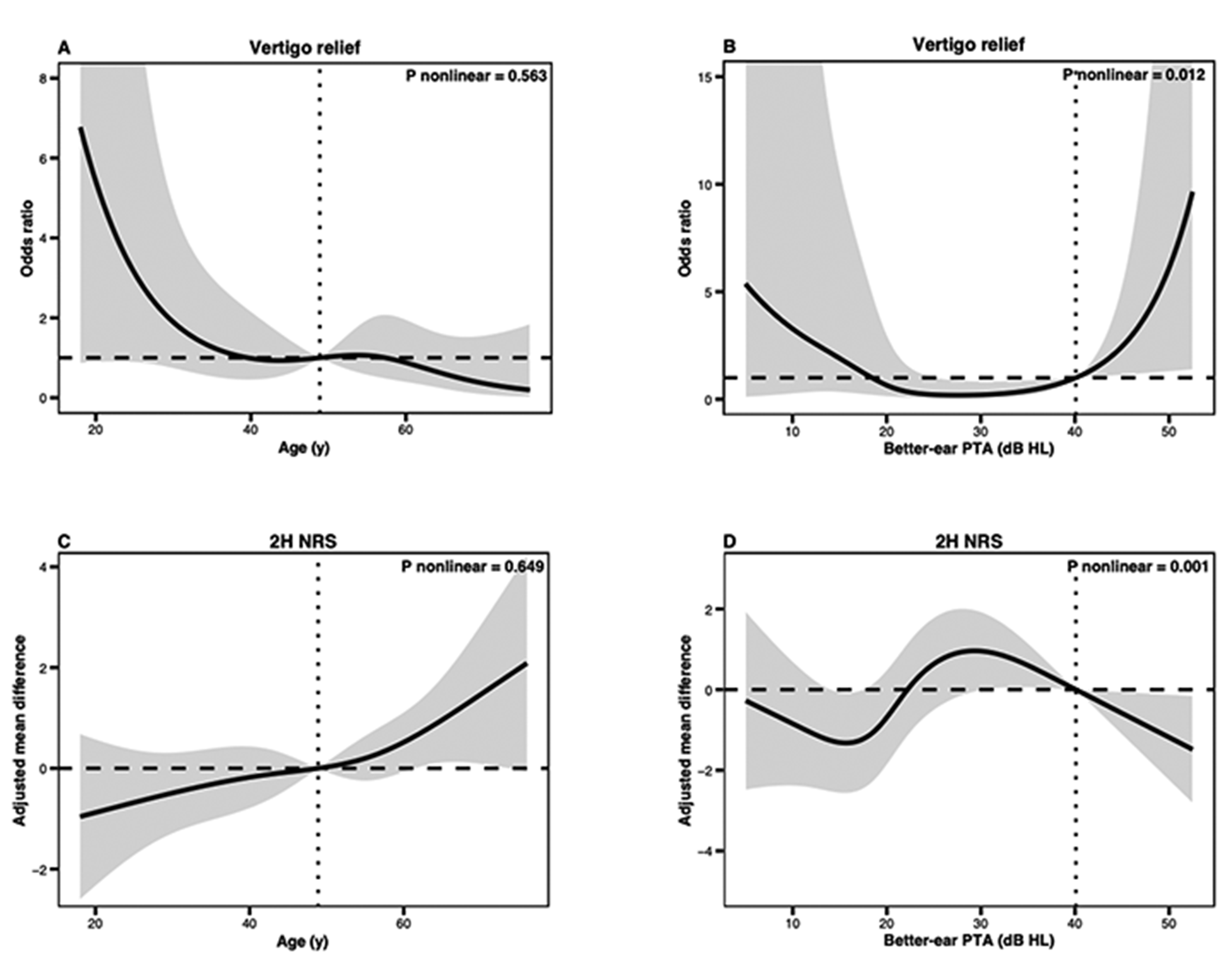
Restricted cubic spline associations of age and better-ear pure-tone average with vertigo outcomes.
Associations between clinical characteristics and treatment response outcomes. (252 episodes from 86 patients)
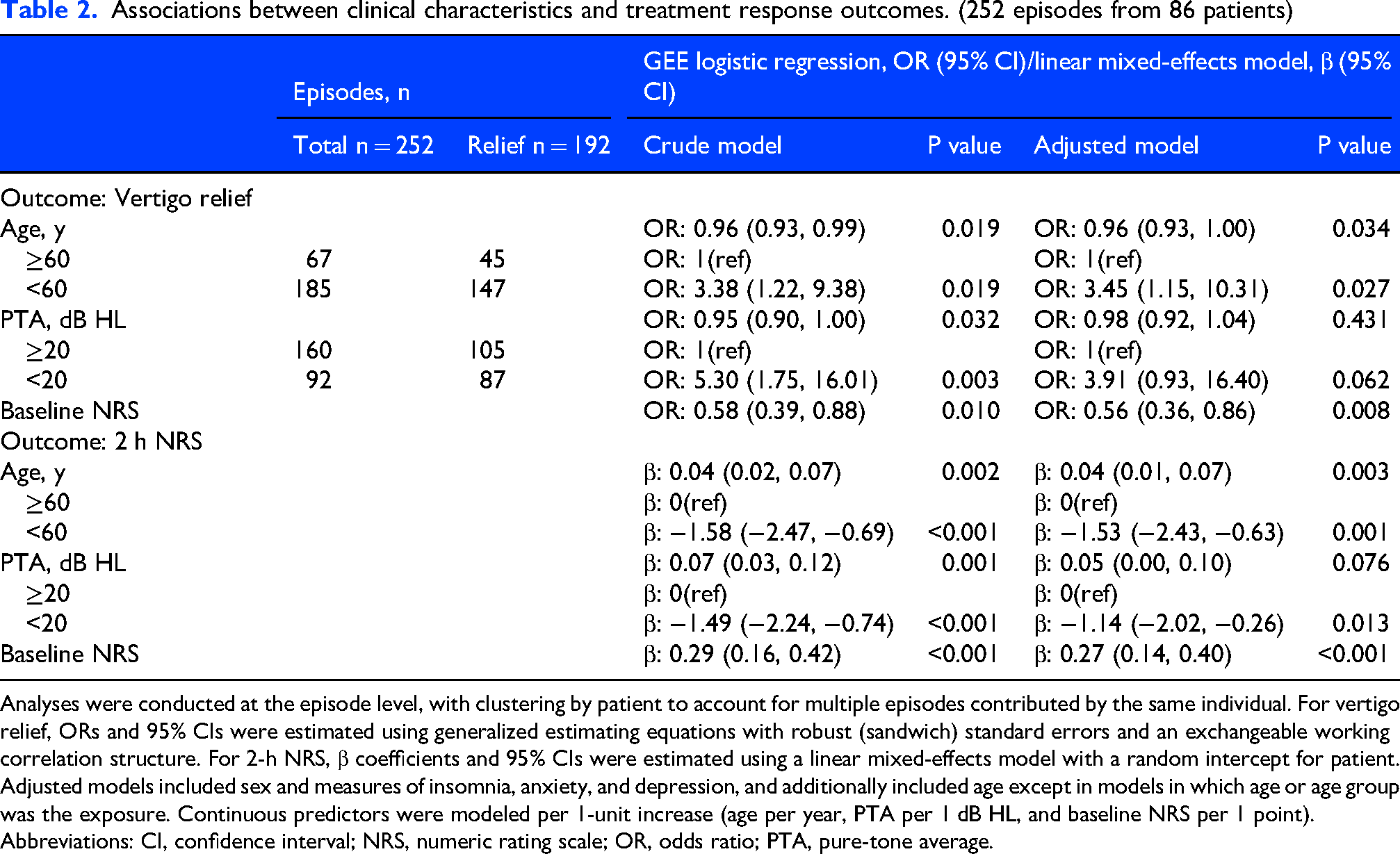
Analyses were conducted at the episode level, with clustering by patient to account for multiple episodes contributed by the same individual. For vertigo relief, ORs and 95% CIs were estimated using generalized estimating equations with robust (sandwich) standard errors and an exchangeable working correlation structure. For 2-h NRS, β coefficients and 95% CIs were estimated using a linear mixed-effects model with a random intercept for patient.
Adjusted models included sex and measures of insomnia, anxiety, and depression, and additionally included age except in models in which age or age group was the exposure. Continuous predictors were modeled per 1-unit increase (age per year, PTA per 1 dB HL, and baseline NRS per 1 point).
Abbreviations: CI, confidence interval; NRS, numeric rating scale; OR, odds ratio; PTA, pure-tone average.
Additional analyses of secondary 2-h outcomes were generally consistent with the primary vertigo relief analysis. Complete vertigo freedom occurred in 39 of 252 treated episodes (15.5%). In adjusted models, younger age and lower baseline vertigo severity remained the main factors associated with complete vertigo freedom, whereas better-ear PTA showed the same direction of association but with a wide confidence interval after adjustment (Table 3). Remission of vertigo occurred in 146 of 252 episodes (57.9%). For remission of vertigo, younger age and better hearing remained associated with higher odds of remission (Supplementary Table S3).
Associations between clinical characteristics and vertigo freedom at 2 h. (252 episodes from 86 patients)
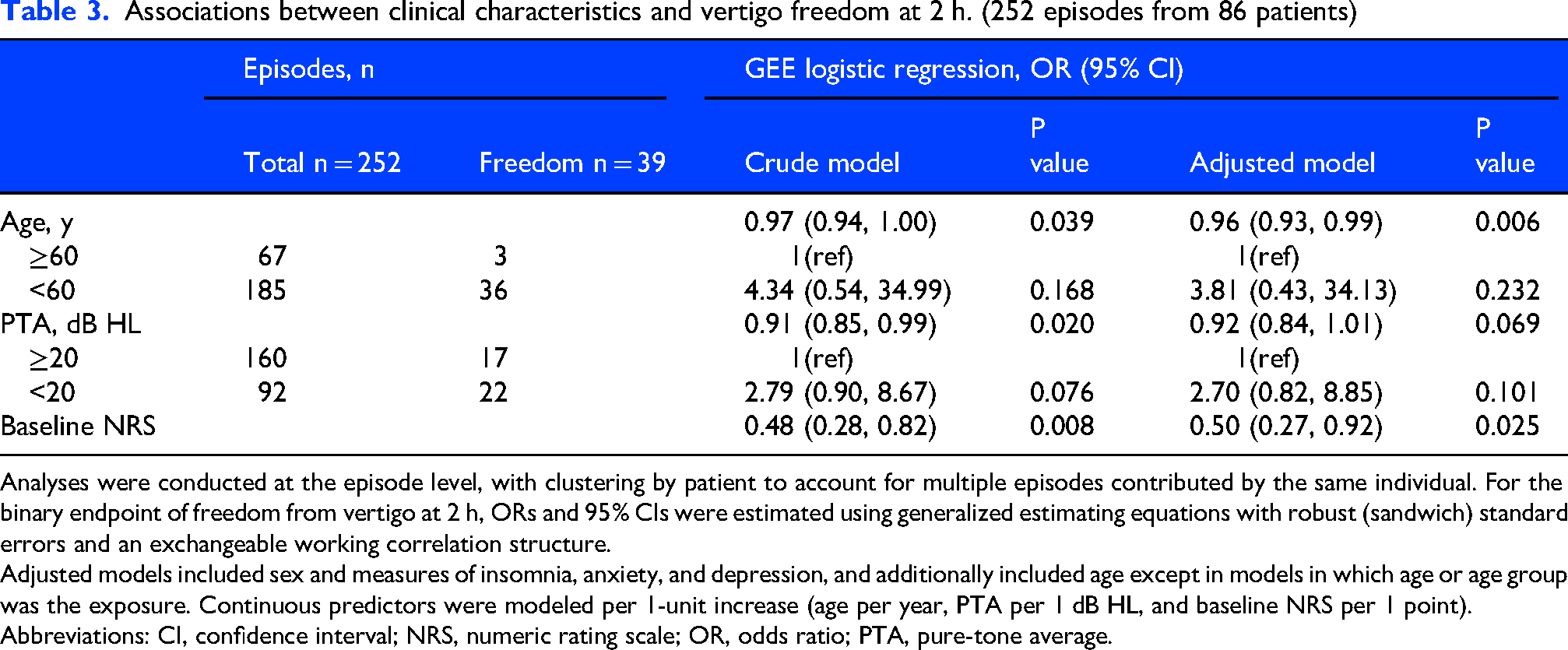
Analyses were conducted at the episode level, with clustering by patient to account for multiple episodes contributed by the same individual. For the binary endpoint of freedom from vertigo at 2 h, ORs and 95% CIs were estimated using generalized estimating equations with robust (sandwich) standard errors and an exchangeable working correlation structure.
Adjusted models included sex and measures of insomnia, anxiety, and depression, and additionally included age except in models in which age or age group was the exposure. Continuous predictors were modeled per 1-unit increase (age per year, PTA per 1 dB HL, and baseline NRS per 1 point).
Abbreviations: CI, confidence interval; NRS, numeric rating scale; OR, odds ratio; PTA, pure-tone average.
Discussion
In this real-world cohort of 86 patients with VM, rimegepant as acute treatment was associated with a significant reduction in vertigo intensity from baseline to 2 h post-dose. Across 252 episodes, vertigo intensity decreased by a mean of 4.44 NRS points at 2 h, and 76.2% of episodes met criteria for vertigo relief. Younger age and better-preserved hearing were associated with more favorable outcomes across several episode-level vertigo outcomes.
Clinical and mechanistic context for CGRP antagonism in vestibular migraine
The available randomized evidence for acute pharmacological treatment of vestibular migraine remains limited. In the 2023 Cochrane review, 7 only two placebo-controlled randomized trials, including 133 participants, evaluated triptans for acute vestibular migraine attacks: one compared 10 mg rizatriptan with placebo, and the other compared 2.5 mg zolmitriptan with placebo.8,36 Across these trials, vertigo relief occurred in 76 of 161 triptan-treated attacks (47.2%) and 55 of 101 placebo-treated attacks (54.5%). In the present real-world cohort, 192 of 252 rimegepant-treated episodes (76.2%) achieved 2-h vertigo relief, a rate numerically higher than those reported in the prior randomized triptan evidence. This observation provides clinically relevant context for the potential acute use of rimegepant in vestibular migraine. Nevertheless, because comparisons are indirect across heterogeneous studies, these findings should not be interpreted as evidence of comparative efficacy.
CGRP signaling is present in the human vestibular periphery and inner ear, providing an anatomical substrate through which CGRP antagonism could influence vestibular processing or peripheral sensory gain. 12 Moreover, preclinical work indicates that chronic migraine modeling induces vestibular dysfunction accompanied by CGRP upregulation and sensitization within vestibular nuclei, and that targeting CGRP-related mechanisms can attenuate vestibular abnormalities. 14 Clinically, preventive studies of CGRP-targeted monoclonal antibodies, including randomized data with galcanezumab, have shown improvement in vestibular symptoms in VM. Together, these observations support the concept that CGRP participates in migraine-related vestibular symptom generation rather than acting solely as a mediator of headache.37,38
Factors associated with treatment response
Age emerged as the most consistent predictor of acute effectiveness across analytic approaches. Older patients (≥60 years) had lower odds of vertigo relief and greater residual symptom burden at 2 h. Several non–mutually exclusive mechanisms may account for this association. First, the clinical phenotype of vestibular migraine may become more heterogeneous with age, increasing the likelihood of overlapping vestibular symptoms. 39 A higher prevalence of non-migraine vestibular mechanisms, including degenerative vestibulopathy, vascular comorbidity, or concomitant mood and sleep disorders, could attenuate the apparent effectiveness of a migraine-specific therapy. Second, aging is associated with a global decline in vestibular system reserve, encompassing reduced central compensation capacity, impaired multisensory integration, and progressive peripheral sensory degeneration, including hearing and vestibular dysfunction. These changes may limit rapid reversibility of acute symptoms. Third, the biological process of aging involves a progressive decline in calcitonin gene-related peptide synthesis and a reduction in receptor density within sensory neurons, 40 which could theoretically attenuate pharmacologic effects of CGRP receptor antagonism.
Our analysis also revealed a crucial non-linear relationship between pure-tone audiometry thresholds and acute treatment response. Patients with preserved hearing (better-ear PTA <20 dB HL) showed the most favorable outcomes. In contrast, intermediate degrees of hearing loss were associated with the lowest odds of relief and the highest residual vertigo scores. Notably, efficacy did not continue to decline with more advanced hearing loss but appeared to plateau. Although confidence intervals were wide and estimates should be interpreted cautiously, this pattern suggests that treatment response does not follow a simple linear gradient across auditory impairment. One possible explanation is that preserved cochlear function reflects a predominantly functional, migraine-driven network disturbance that remains biologically reversible. Intermediate hearing loss may indicate a mixed phenotype characterized by partial peripheral labyrinthine injury superimposed on central sensitization, thereby reducing responsiveness to CGRP receptor antagonism. While these interpretations remain speculative, the consistency of directional effects across models supports the relevance of auditory phenotype as a potential modifier of acute response. Additionally, among participants with vestibular testing, normal caloric results were associated with greater vertigo relief in crude analyses and remained marginal after adjustment (Supplementary Table S4), and prior studies similarly indicate that peripheral vestibular abnormalities on caloric testing are associated with poorer treatment response in vestibular migraine.41,42
Baseline vertigo severity at dosing was among the strongest predictors of acute outcomes. While baseline severity is not a perfect surrogate for time-to-dose, it plausibly reflects one of two clinically meaningful constructs: delayed treatment after symptom escalation, and/or inherently more severe attacks that are more refractory. In migraine headache, the importance of early treatment—particularly prior to cutaneous allodynia—has been well described for triptans. 43 Similarly, gepant data in migraine indicate improved 2-h outcomes when treatment is administered at mild rather than moderate or severe baseline pain. 44 These converging lines of evidence support a biologically plausible interpretation: early intervention may prevent or dampen progressive sensitization within relevant sensory networks, whereas once escalation occurs, symptom relief becomes less achievable within a short time window. Applied to VM, this suggests a pragmatic clinical strategy: rather than waiting until vertigo becomes intolerable, patients may benefit from taking migraine-specific therapy at the earliest recognizable onset of vestibular symptoms, before the attack reaches peak intensity.
Strengths and limitations of study
The advantage of this study is the real-world setting, evaluation across repeated treatment episodes with analytic methods accounting for within-patient correlation, and a coherent set of sensitivity analyses. To our knowledge, this study is among the first to evaluate rimegepant for the acute treatment of vertigo in vestibular migraine, is the first to systematically examine prognostic factors associated with treatment response, and includes the largest sample reported to date. The study has several limitations. First, the observational design without a comparator group limits causal interpretation. Second, although measured baseline characteristics were generally similar between included and excluded patients, unmeasured differences related to follow-up availability, treatment response, tolerability, satisfaction, or adverse events cannot be excluded. Third, outcomes were based on patient-reported vertigo NRS at 2 h, which is clinically interpretable but has not been specifically validated. Fourth, exploratory vestibular testing analyses were limited by missing data. Finally, the single-center tertiary-care setting may limit generalizability, and validation in broader clinical populations is warranted.
Conclusion and clinical relevance
In this real-world clinical study, rimegepant was associated with substantial improvement in the acute treatment of VM-related vertigo. Age was a consistent predictor of acute effectiveness, and better hearing and preserved vestibular function showed directionally favorable associations that, while sometimes only marginally statistically significant, are mechanistically plausible and clinically relevant for hypothesis generation. Baseline symptom severity at dosing strongly predicted response, aligning with the broader migraine literature emphasizing early treatment. Clinically, these findings suggest that rimegepant may be most useful in younger patients with VM and better-preserved audiovestibular function, particularly when administered earlier during an attack. Future randomized, adequately powered trials should evaluate rimegepant and other gepants for acute vestibular symptoms in VM, with pre-specified stratification by age, auditory/vestibular phenotype, and treatment timing, and with outcomes spanning both acute relief and longer-term disability.
Article highlights
This real-world cohort provides early clinical evidence for rimegepant in acute vertigo attacks in vestibular migraine.
Vertigo relief occurred in 76.2% of treated episodes, with a mean 2-h NRS reduction of 4.44 points.
Younger age, lower baseline severity, and better hearing were associated with better response.
Findings support earlier mechanism-based treatment and future stratified trials.
Supplemental Material
sj-docx-1-cep-10.1177_03331024261463533 - Supplemental material for Effectiveness and clinical predictors of rimegepant for acute vertigo in vestibular migraine: A real-world cohort study
Supplemental material, sj-docx-1-cep-10.1177_03331024261463533 for Effectiveness and clinical predictors of rimegepant for acute vertigo in vestibular migraine: A real-world cohort study by Yingqiang Li, Lingling Yu, Dongzhou Deng, Xun Cao, Xiang Lu and Dan Bing in Cephalalgia
Supplemental Material
sj-docx-2-cep-10.1177_03331024261463533 - Supplemental material for Effectiveness and clinical predictors of rimegepant for acute vertigo in vestibular migraine: A real-world cohort study
Supplemental material, sj-docx-2-cep-10.1177_03331024261463533 for Effectiveness and clinical predictors of rimegepant for acute vertigo in vestibular migraine: A real-world cohort study by Yingqiang Li, Lingling Yu, Dongzhou Deng, Xun Cao, Xiang Lu and Dan Bing in Cephalalgia
Supplemental Material
sj-png-3-cep-10.1177_03331024261463533 - Supplemental material for Effectiveness and clinical predictors of rimegepant for acute vertigo in vestibular migraine: A real-world cohort study
Supplemental material, sj-png-3-cep-10.1177_03331024261463533 for Effectiveness and clinical predictors of rimegepant for acute vertigo in vestibular migraine: A real-world cohort study by Yingqiang Li, Lingling Yu, Dongzhou Deng, Xun Cao, Xiang Lu and Dan Bing in Cephalalgia
Footnotes
Acknowledgements
None.
Ethical considerations
The study was approved by the Institutional Review Board of Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology (Approval No. TJ-IRB202602006).
Consent to participate
The requirement for informed consent was waived because of the retrospective nature of the study and the use of de-identified clinical data.
Consent for publishing
The authors agree that if accepted, the article publishes with Cephalalgia.
Author contributions
YL performed the data analysis and drafted the manuscript. LY and DB contributed to study design, data interpretation, and manuscript revision. DD and XC acquired data and revised the manuscript. XL and DB conceived and supervised the study, interpreted the data, and critically revised the manuscript. YL and LY contributed equally and share first authorship. XL and DB are co–corresponding authors. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (82571336), the National Key R&D Program of China (2023YFC2508400), and the Hubei Provincial Key Research and Development Program (2022BCA006).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated and/or analyzed during the current study are derived from an institutional hospital information system and include patient-level clinical information. In accordance with institutional policy and applicable data protection regulations, these data are not publicly available. De-identified data may be made available from the corresponding author on reasonable request and subject to institutional approval.
Open practices
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.