
Abstract
Aim
To evaluate whether initiation of calcitonin gene-related peptide (CGRP) monoclonal antibodies (mAbs) was non-inferior to initiation of onabotulinumtoxinA with respect to the hazard of ischemic stroke or transient ischemic attack (IS + TIA) in a real-world cohort of adults with migraine.
Methods
We conducted a retrospective, active-comparator, new-user pharmacoepidemiology study using the NIH All of Us Research Program Registered Tier Dataset (v8). Adults with migraine initiating CGRP mAbs (erenumab, fremanezumab, galcanezumab, eptinezumab) were compared with initiators of onabotulinumtoxinA from January 2018 through September 2023. The primary outcome was IS + TIA occurring more than 90 days after treatment initiation. Inverse probability of treatment weighting (IPTW) with stabilized propensity scores was used to adjust for 23 baseline covariates. Non-inferiority was assessed on the hazard ratio (HR) scale using a prespecified margin of 1.5, with non-inferiority concluded if the upper bound of the 95% confidence interval (CI) was less than 1.5. Prespecified subgroup analyses included migraine with aura and without aura. Prespecified sensitivity analyses included a per-protocol analysis, a crossover-excluded analysis, and an IS-only analysis. Fracture was used as a negative control outcome.
Results
Among 16,147 patients with migraine in the cohort, the primary comparison included 1,581 CGRP mAb initiators and 947 onabotulinumtoxinA initiators. IPTW achieved a good covariate balance for the primary comparison (maximum standardized mean difference 0.016). For the primary outcome, 14 IS + TIA events occurred among CGRP mAb initiators and 22 among onabotulinumtoxinA initiators. The hazard ratio for IS + TIA was 0.524 (95% CI 0.263–1.046), which met the prespecified statistical criterion for non-inferiority because the upper confidence bound was below 1.5; however, the estimate was imprecise because of the small number of events. In the migraine with aura subgroup, the estimate also met the non-inferiority criterion (HR 0.419, 95% CI 0.163–1.080), whereas the migraine without aura subgroup, per-protocol analysis, and major adverse cardiovascular events analysis were inconclusive for non-inferiority. For major adverse cardiovascular events the HR was 1.068 (95% CI 0.589–1.935). The fracture negative control was also not significantly different (HR, 1.175; 95% CI, 0.692–1.993; p = 0.551), arguing against systematic healthy-user confounding. A formal adjusted comparison with untreated patients was not feasible due to structural confounding inherent to the stepped-care treatment pathway.
Conclusions
In this real-world diverse cohort, initiation of CGRP mAbs met the prespecified statistical criterion for non-inferiority relative to onabotulinumtoxinA for the primary IS + TIA outcome. However, this finding was based on few events and wide CIs and should be interpreted cautiously as limited evidence against a large relative increase in incident IS + TIA risk, rather than as definitive evidence of equivalent safety, absence of modest harm, or a protective effect. Several secondary, subgroup, and supportive analyses remained inconclusive for non-inferiority. Larger adequately powered comparative safety studies are needed.
This is a visual representation of the abstract.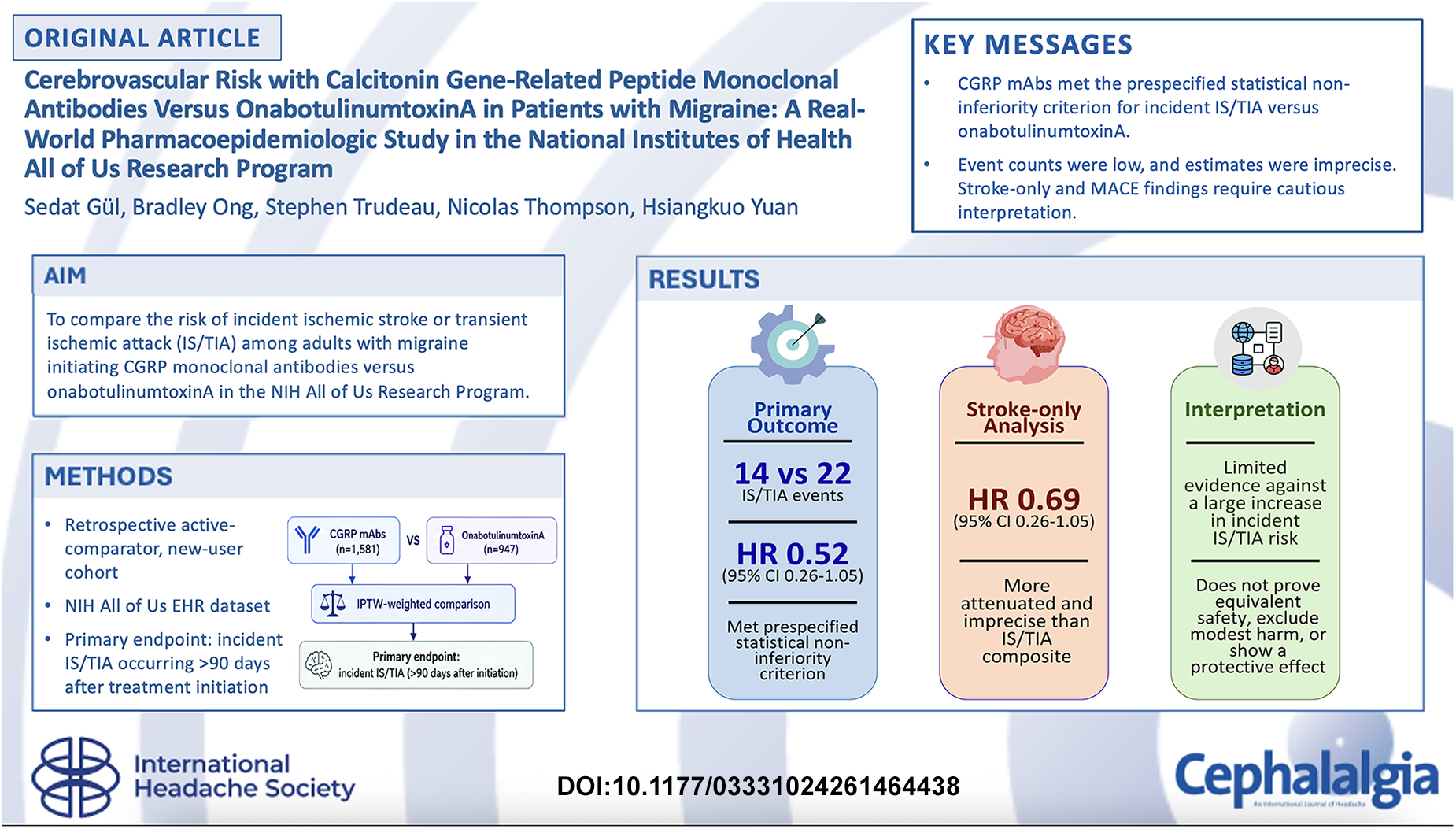
Introduction
Migraine with aura is a well-established risk factor for ischemic stroke, with prior studies reporting an approximately 2.0 to 2.5-fold higher relative risk overall and substantially higher risks in younger women who use combined oral contraceptives. 1 More broadly, headache is a common and clinically important manifestation across multiple stroke subtypes, underscoring the close relationship between headache disorders and cerebrovascular disease.2,3
Calcitonin gene-related peptide (CGRP)-targeted therapies have transformed preventive treatment for migraine. Four monoclonal antibodies (mAbs), erenumab, fremanezumab, galcanezumab, and eptinezumab, are approved by the United States (US) Food and Drug Administration (FDA) for migraine prevention, and small-molecule CGRP receptor antagonists (gepants) are also now available for acute treatment.4–8
However, despite widespread clinical use, the cerebrovascular safety of CGRP mAbs remains incompletely characterized in real-world populations. Mechanistically, this question is relevant because CGRP is a potent vasodilatory neuropeptide that may contribute to cerebral ischemic preconditioning, raising concern that pathway blockade could have the unintended risk of worsening cerebrovascular outcomes. 9 At the same time, pivotal phase III trials systematically excluded patients with recent stroke, recent major cardiovascular events, or substantial cerebrovascular risk, limiting the applicability of trial-based safety data to patients commonly encountered in clinical practice. The largest prior real-world comparative safety study, 10 which used Medicare claims data, did not identify an increased risk of composite cardiovascular events among CGRP mAb users relative to onabotulinumtoxinA users, although rare cardiovascular events may be difficult to detect in population-average analyses. In addition, that analysis excluded patients with prior myocardial infarction or stroke and enrolled predominantly older White adults. 10 Whether these findings generalize to younger, more diverse populations with varying vascular risk profiles remains unknown.
To address this gap, we conducted a pharmacoepidemiologic study using the National Institutes of Health (NIH) All of Us Research Program, a large US research cohort with substantial racial, ethnic, and socio-economic diversity. We evaluated the comparative cerebrovascular safety of CGRP mAbs versus onabotulinumtoxinA in a real-world population with broader demographic representation than prior claims-based studies and with inclusion of patients who had vascular comorbidities commonly excluded from clinical trials. We sought to determine whether initiation of CGRP mAbs was non-inferior to initiation of onabotulinumtoxinA with respect to ischemic cerebrovascular events.
Methods
Study design and data source
We conducted a retrospective active-comparator, new-user pharmacoepidemiologic study using the NIH All of Us Research Program Registered Tier Dataset, version 8 (Curated Data Repository [CDR] v8; release C2024Q3R9). 11 The All of Us Research Program is a prospective US cohort of more than 804,000 participants with longitudinal electronic health record (EHR) data from over 35 contributing health systems, mapped to the Observational Medical Outcomes Partnership (OMOP) Common Data Model. All analyses were conducted within the secure All of Us Researcher Workbench on Google Cloud Platform. The study adhered to the All of Us Data User Code of Conduct and was registered in the All of Us Research Hub (Identifier: aou-rw-a119f16e). 11 The Cleveland Clinic Institutional Review Board (IRB) determined that the project did not constitute human subject research; therefore, no IRB approval was required. This study is reported in accordance with Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for observational studies. 12
Study population
We identified adults aged 18 to 75 years with migraine using International Classification of Diseases, Tenth Revision (ICD-10) codes (G43.0x, G43.1x, G43.7x, G43.8x, and G43.9x). Migraine was defined by at least two qualifying diagnoses recorded at least 30 days apart. Patients were also required to have at least six months between the first qualifying migraine diagnosis and treatment initiation. These criteria were intended to establish baseline clinical history and did not impose a minimum duration of post-index follow-up. All patients contributed person-time from the index date regardless of subsequent follow-up duration.
The study period included 1 January 2018 to 1 September 2023. Patients with cluster headache (G44.0x) and migraine with cerebral infarction codes (G43.6x) were excluded to reduce outcome misclassification and to avoid including patients with a pre-existing cerebrovascular migraine subtype directly related to the study endpoint. Aura status was classified conservatively: patients with any G43.1x code were classified as having migraine with aura, irrespective of co-occurring codes for migraine without aura. Study size was determined by the number of patients in the Registered Tier dataset who met prespecified eligibility criteria during the study period; no a priori sample size calculation was performed.
Exposure definition
Using a new-user active-comparator design, we assigned each patient to the highest-priority preventive treatment class they initiated on or after 1 January 2018: (1) CGRP mAbs (erenumab, fremanezumab, galcanezumab, or eptinezumab); (2) onabotulinumtoxinA; (3) older preventive therapies (topiramate, amitriptyline, nortriptyline, propranolol, metoprolol, valproate, venlafaxine, and candesartan); or (4) no preventive therapy. Triptans were classified as acute therapies and were not considered preventive exposures; patients receiving triptans without a preventive drug were included in the no-preventive group. Patients receiving gepants were retained as a separate exploratory cohort because of mixed acute and preventive indications and were not included in the primary causal comparison.
For the primary comparative analysis, we compared initiators of CGRP mAbs with initiators of onabotulinumtoxinA, an active comparator selected to reduce confounding by indication relative to untreated comparators, while recognizing that onabotulinumtoxinA is often used in a more chronic or treatment-refractory migraine population. Patients who initiated both CGRP mAbs and onabotulinumtoxinA within 30 days were excluded (n = 10). The index date was defined as the date of first qualifying prescription or administration for the assigned treatment class. To preserve a new-user design, patients were required to have no use of the assigned treatment class during the preceding 12 months. If more than one eligible treatment class was initiated on the same date, treatment assignment was determined using a prespecified hierarchy, with CGRP mAbs prioritized over onabotulinumtoxinA, followed by older preventive therapies. The priority hierarchy served only as a tie-breaker in the rare case of simultaneous initiation of multiple drug classes on the same date; no future prescription information was used in group assignment.
Outcomes
The primary outcome was the first incident composite of ischemic stroke or transient ischemic attack (IS + TIA), defined using ICD-10 codes I63.x and G45.x, respectively, when associated with an inpatient or emergency department encounter (visit_concept_id 9201, 262, 8717, or 9203). All patients contributed person-time from the index date (day 0). In the primary analysis, events occurring within 90 days after treatment initiation were not counted toward the primary endpoint in order to reduce reverse causation bias from pre-existing or evolving cerebrovascular disease at the time of treatment initiation. Patients were not required to remain event-free during the 90-day window to be included in the analysis.
Secondary outcomes included IS alone, TIA alone, hemorrhagic stroke (I60-I62), myocardial infarction (I21.x), and major adverse cardiovascular events (MACE). MACE was defined as a composite of IS, myocardial infarction, and intracerebral hemorrhage, consistent with commonly used definitions of major adverse cardiovascular events in observational cardiovascular safety analyses. 13 Subarachnoid hemorrhage (I60.x) and other nontraumatic hemorrhagic stroke (I62.x) were excluded from MACE definition because of distinct pathophysiology and low event counts that precluded meaningful analysis. All-cause mortality was not formally analyzed due to limitations in death ascertainment, and death was therefore not modeled as a competing risk in the primary Cox analyses.
Fracture (S42.x, S52.x, S72.x, M80.x) and urinary tract infection (UTI; N39.0) were used as negative control outcomes to assess residual unmeasured confounding.
Covariates and propensity score modeling
Baseline covariates were ascertained from EHR data before the index date and included age, sex, self-reported race and ethnicity, aura status, prior stroke, hypertension, diabetes, chronic kidney disease (CKD), heart failure, coronary artery disease, atrial fibrillation, statin use, aspirin use, anticoagulant use, antiplatelet use, combined oral contraceptive use, prior triptan use, and prior preventive use. Episodic versus chronic migraine status and monthly headache days were not available as standardized structured variables in the analytic dataset and therefore could not be included in the baseline table or propensity score model. Prior triptan use and prior preventive use were modeled as binary variables defined as any documented use before the index date. Prior preventive use referred to any use of older preventive therapies included in the study medication framework before cohort entry.
Separate binary logistic regression propensity score models with L2 (ridge) regularization were fit for each comparison after standardization of model features using Python (version 3.10) with scikit-learn's Logistic Regression function. L2 regularization was used to reduce overfitting and stabilize propensity score estimation. Stabilized inverse probability of treatment weighting (IPTW) were estimated and truncated at the 1st and 99th percentiles to create weighted pseudo-populations with improved comparability on measured baseline covariates. These weights were constructed to estimate the average treatment effect (ATE) in the weighted population. Covariate balance was assessed using standardized mean differences (SMD) and visualized with a Love plot; an SMD less than 0.1 was required for all covariates before proceeding with formal causal analysis. Missing data were not imputed; analyses were based on available structured EHR data in the Registered Tier dataset. Episodic versus chronic migraine status and monthly headache days were not available as standardized structured variables in the analytic dataset, precluding adjustment or restriction based on migraine frequency status.
Statistical analysis
IPTW-weighted Cox proportional hazards models with robust standard errors were fitted using Python (version 3.10) and the lifelines package (version 0.30.0) within the All of Us Researcher Workbench. In the primary weighted Cox models, treatment group was the predictor of interest, with IPTW used to balance measured baseline covariates between groups prior to outcome modeling; additional covariate adjustment was not applied in the outcome model. A Cox time-to-event framework was selected because follow-up time varied across patients and the primary objective was to compare the hazard of first incident IS + TIA between treatment groups over time.
Because the primary clinical question was whether CGRP mAbs were not meaningfully worse than onabotulinumtoxinA with respect to ischemic cerebrovascular safety, the primary analysis was framed as a non-inferiority comparison rather than a superiority test. Non-inferiority was evaluated on the hazard ratio (HR) scale using a prespecified margin of 1.5. This margin was selected as a pragmatic upper safety boundary for a rare but clinically important outcome in an active-comparator observational study. Because IS + TIA events are uncommon in migraine prevention cohorts, a narrower margin would require substantially larger event counts than were available in the All of Us dataset and would be poorly suited to the precision expected from this real-world analysis. Clinically, the margin was chosen to test whether CGRP mAbs could exclude a large relative excess risk compared with onabotulinumtoxinA, an established preventive treatment often used in chronic or treatment-refractory migraine. The margin should not be interpreted to mean that a 50% increase in IS + TIA hazard would be acceptable for all patients. Rather, it was intended as a boundary for ruling out a large safety signal while recognizing that smaller increases in risk could still be clinically relevant, particularly for patients with high baseline vascular risk. Under this framework, the null hypothesis was that the hazard ratio was greater than or equal to 1.5, and the alternative hypothesis was that the hazard ratio was less than 1.5. Non-inferiority was concluded when the upper bound of the 95% confidence interval (CI) was below 1.5. Two-sided p values are reported as descriptive measures of superiority testing where applicable but were not the primary basis for inference.
The primary intention-to-treat (ITT) analysis followed patients from the index date (day 0) regardless of subsequent treatment changes. Patients who did not experience the outcome were censored at the date of last available follow-up in the dataset. Follow-up began at day 0 for all patients; the 90-day outcome latency window affected the definition of the primary endpoint rather than the timing of cohort entry. Three sensitivity analyses were prespecified: (1) per-protocol, with censoring at treatment discontinuation, defined as a gap of more than 90 days between successive observed CGRP mAb prescriptions or administrations and a gap of more than 150 days between successive onabotulinumtoxinA administrations; (2) crossover-excluded, with exclusion of patients who switched between groups during follow-up (all 327 crossover patients switched from onabotulinumtoxinA to CGRP mAbs, representing treatment escalation; no reverse switching was observed); and (3) IS only, defined by exclusion of TIA from the composite outcome. Subgroup analyses were conducted in migraine with aura and without aura. A formal interaction test (treatment-by-aura status) was performed. Post hoc power calculations were performed using the Schoenfeld method. In an additional sensitivity analysis, the 90-day latency window was removed and all IS + TIA events from day 0 onward were counted to assess whether the latency definition introduced survivor bias.
We attempted to formally compare CGRP mAbs with an untreated reference group using multiple progressive restriction strategies (prior triptan use, prior preventive use, and ≥2 prior preventive therapy class failures). Despite these restrictions, prior triptan use remained severely imbalanced (minimum post-weighting SMD, 0.449), reflecting structural confounding inherent to the stepped-care treatment pathway. This comparison was therefore reported descriptively only.
Results
Study population
Of 26,763 patients with migraine identified in the All of Us Registered Tier Dataset, 19,025 had at least two qualifying codes recorded ≥30 days apart, and 16,147 met all eligibility criteria, including the requirement for at least six months between the first qualifying migraine diagnosis and the index date. Exclusions occurred primarily because patients did not meet the requirement for at least two qualifying migraine diagnoses recorded 30 days apart or did not meet the minimum six-month interval between first qualifying migraine diagnosis and treatment initiation; additional exclusions included cluster headache and migraine with cerebral infarction codes.
The final cohort comprised 1,581 CGRP mAb initiators, 947 onabotulinumtoxinA initiators, 3,845 older preventive initiators, and 9,385 patients with no preventive therapy. The no-preventive group was included for descriptive analyses only and was not part of the primary causal comparison. An additional 389 gepant users were retained as an exploratory cohort. Given the mixed indication profile of gepants in this cohort, with ubrogepant indicated only for acute treatment and rimegepant indicated for both acute and preventive treatment, and the low event count (n = 4 IS + TIA events), gepant users were retained for descriptive analyses only and were not included in formal causal inference.
The cohort was predominantly female (85.3%), with a mean age of 51.2 years (standard deviation [SD] 13.3). Non-White participants comprised 38.7% of the cohort, including 15.4% Hispanic and 13.2% Black/African American participants.
Baseline characteristics
Baseline characteristics by treatment group are shown in Table 1. Compared with onabotulinumtoxinA initiators, patients initiating CGRP mAbs were younger (mean age, 49.0 years), more likely to have migraine with aura (47.2%), and more likely to have prior triptan use (75.1%) and prior preventive use (87.1%). Episodic versus chronic migraine status and monthly headache days were not reliably available as standardized structured variables in the analytic dataset. In contrast, onabotulinumtoxinA initiators had higher prevalences of vascular comorbidities, including hypertension (44.2%) and atrial fibrillation (5.4%). These baseline differences were consistent with treatment selection along a stepped-care pathway and supported the need for propensity score adjustment.
Baseline characteristics of primary analytic treatment groups.a

Exploratory gepant users were excluded from this table.
Values are n (%) unless otherwise stated. Abbreviations: CAD = coronary artery disease; CKD = chronic kidney disease; IS + TIA = ischemic stroke or transient ischemic attack; MACE = major adverse cardiovascular events; SD = standard deviation. Combined oral contraceptive use refers to estrogen-containing oral contraceptive therapy.
Propensity score balance
IPTW achieved good covariate balance for the primary comparison (CGRP mAbs versus onabotulinumtoxinA): maximum SMD 0.016, mean SMD 0.006, with all 23 covariates below the 0.1 threshold (Figure 1). The largest baseline imbalances before weighting were prior triptan use (SMD 0.418 before versus 0.010 after) and prior preventive use (SMD 0.313 versus 0.013), both of which were attenuated substantially after weighting. Propensity scores showed substantial overlap between groups (CGRP mAbs: mean 0.654, SD 0.115; onabotulinumtoxinA: mean 0.577, SD 0.150). Stabilized inverse probability weights were not extreme, with a mean of 1.00 and a maximum of 3.354 before truncation.
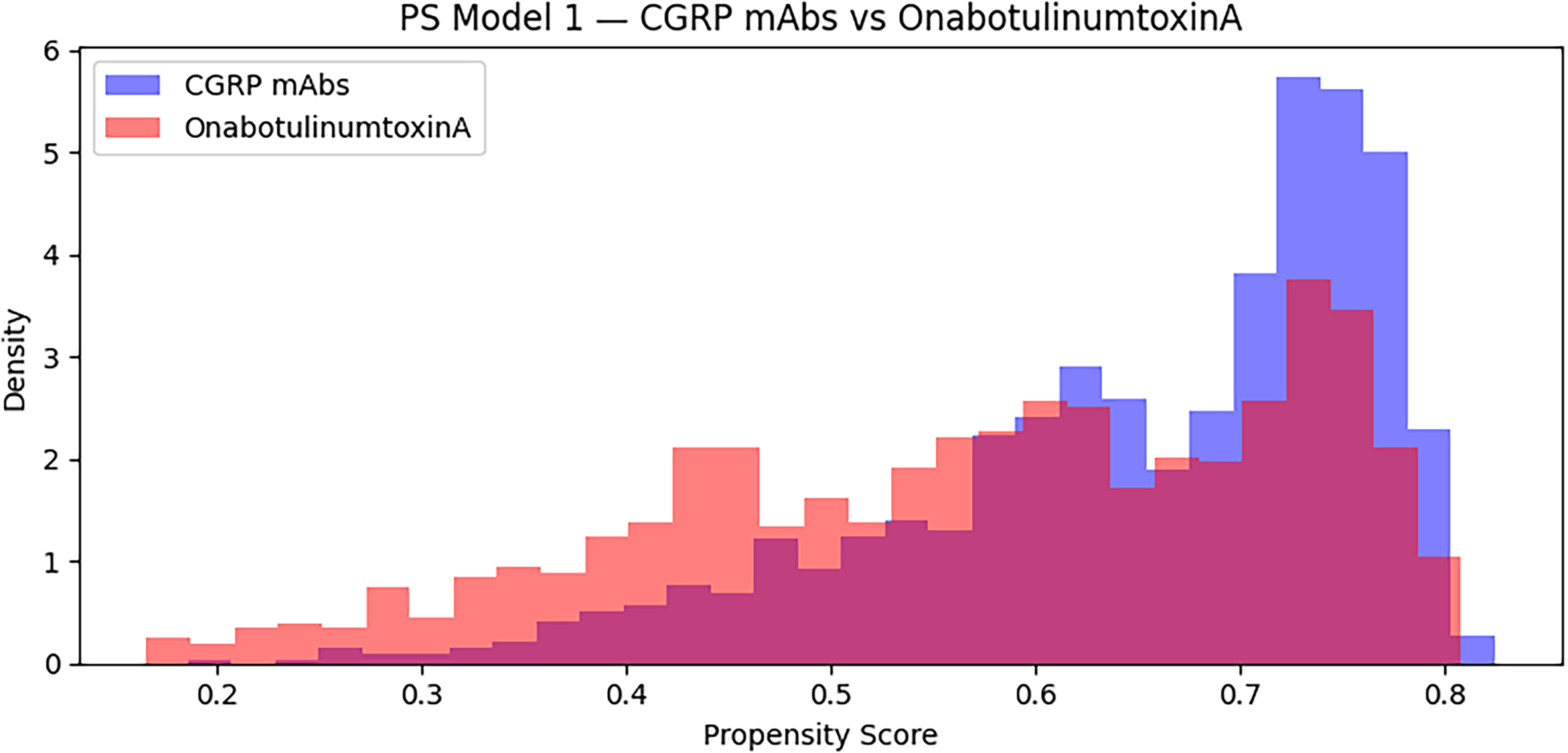
Distribution of propensity scores before weighting for initiators of CGRP monoclonal antibodies and onabotulinumtoxinA.
Primary outcome: IS + TIA
Over a median follow-up of 2.8 years in the CGRP mAb group and 2.9 years in the onabotulinumtoxinA group, 14 IS + TIA events occurred in the CGRP mAb group (0.33 per 100 person-years) and 22 events occurred in the onabotulinumtoxinA group (0.78 per 100 person-years). After IPTW adjustment, the hazard ratio for IS + TIA comparing CGRP mAbs with onabotulinumtoxinA was 0.524 (95% CI 0.263–1.046) (Table 2). Because the upper bound of the 95% CI was below the prespecified non-inferiority margin of 1.5, this met the criterion for non-inferiority. Given the low number of outcome events, the estimate remained imprecise with respect to the exact magnitude of effect (Figure 2).

Covariate balance before and after inverse probability of treatment weighting for initiators of CGRP monoclonal antibodies and onabotulinumtoxinA. Standardized mean differences (SMDs) for 23 baseline covariates comparing initiators of CGRP monoclonal antibodies and onabotulinumtoxinA before and after inverse probability of treatment weighting (IPTW). Each point represents a covariate; values <0.1 indicate adequate balance. IPTW achieved near-complete covariate balance, with all variables below the prespecified threshold (maximum SMD, 0.016).
IPTW-weighted Cox models for primary, secondary, and subgroup outcomes.
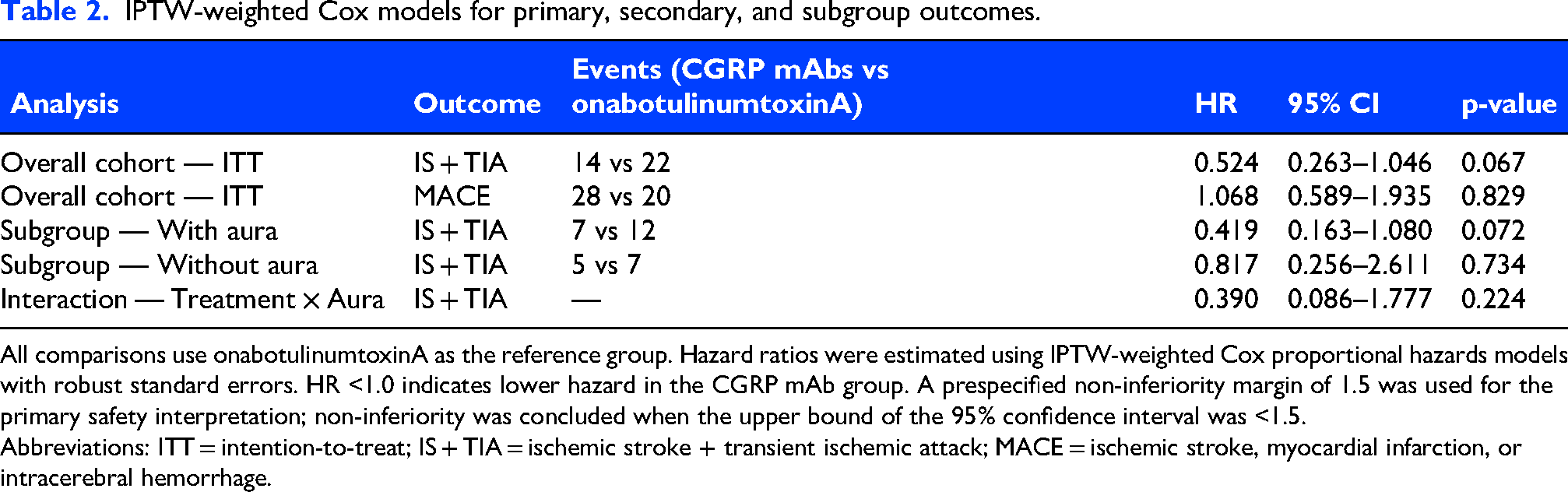
All comparisons use onabotulinumtoxinA as the reference group. Hazard ratios were estimated using IPTW-weighted Cox proportional hazards models with robust standard errors. HR <1.0 indicates lower hazard in the CGRP mAb group. A prespecified non-inferiority margin of 1.5 was used for the primary safety interpretation; non-inferiority was concluded when the upper bound of the 95% confidence interval was <1.5.
Abbreviations: ITT = intention-to-treat; IS + TIA = ischemic stroke + transient ischemic attack; MACE = ischemic stroke, myocardial infarction, or intracerebral hemorrhage.
Sensitivity analyses
All three prespecified sensitivity analyses produced HRs directionally consistent with the primary analysis (Table 3). The crossover-excluded analysis met the prespecified non-inferiority criterion (HR 0.496, 95% CI 0.230–1.069). The IS-only analysis, which represents the harder and more clinically specific cerebrovascular endpoint, also met the prespecified non-inferiority criterion but showed a more attenuated and imprecise estimate than the IS + TIA composite (HR 0.694, 95% CI 0.327–1.475). In contrast, the per-protocol analysis was inconclusive for non-inferiority because the upper confidence bound was 1.505, slightly exceeding the prespecified margin (HR 0.317, 95% CI 0.067–1.505).
Sensitivity and negative-control analyses for CGRP mAbs vs onabotulinumtoxinA. Analyses 1 to 4 showed directionally consistent findings. The primary, crossover-excluded, and ischemic stroke-only analyses met the prespecified non-inferiority criterion, whereas the per-protocol analysis was inconclusive because the upper confidence bound slightly exceeded the margin of 1.5.
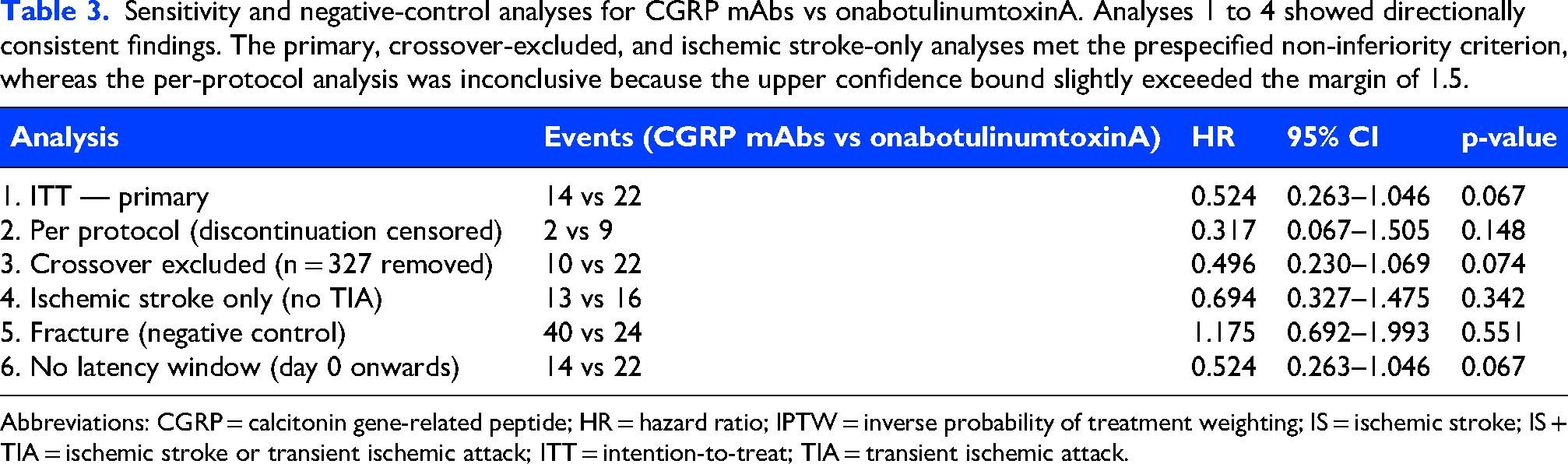
Abbreviations: CGRP = calcitonin gene-related peptide; HR = hazard ratio; IPTW = inverse probability of treatment weighting; IS = ischemic stroke; IS + TIA = ischemic stroke or transient ischemic attack; ITT = intention-to-treat; TIA = transient ischemic attack.
In an additional sensitivity analysis, removal of the 90-day latency window (day 0 onward) produced an identical estimate to the primary analysis (HR 0.524, 95% CI 0.263–1.046, p = 0.067), confirming that no IS + TIA events occurred within the first 90 days in either group. Overall, the direction of effect was similar across sensitivity analyses (HR range, 0.317–0.694).
Subgroup analyses
In the migraine with aura subgroup (CGRP mAbs n = 746, onabotulinumtoxinA n = 382), IPTW achieved covariate balance (maximum SMD 0.026). The HR for IS + TIA was 0.419 (95% CI 0.163–1.080), meeting the prespecified criterion for non-inferiority, with descriptive incidence rates of 0.34 and 1.05 per 100 person-years in the CGRP mAb and onabotulinumtoxinA groups, respectively. In the migraine without aura subgroup, the HR was 0.817 (95% CI 0.256–2.611), which was inconclusive for non-inferiority because the upper confidence bound exceeded 1.5.
Secondary and negative control outcomes
For MACE, the HR was 1.068 (95% CI 0.589–1.935), which was inconclusive for non-inferiority because the upper confidence bound exceeded 1.5. The numbers of events for individual secondary outcomes, including hemorrhagic stroke, intracerebral hemorrhage, and subarachnoid hemorrhage, were too low to support meaningful analysis in the primary comparison. For fracture, the HR was 1.175 (95% CI 0.692–1.993, p = 0.551). For UTI, the HR was 0.688 (95% CI 0.550–0.862, p = 0.001).
CGRP mAbs vs untreated patients
Despite progressive restriction of the untreated comparator to a more treatment-refractory subgroup, defined by prior triptan use and at least two prior preventive therapy class failures (n = 1206), severe imbalance in prior triptan use persisted (minimum SMD, 0.449), precluding formal causal inference. In the restricted comparison, unadjusted IS + TIA rates were 0.41 per 100 person-years in the CGRP mAb group and 0.49 per 100 person-years in the untreated group (unadjusted HR 0.764, 95% CI 0.382–1.531, p = 0.449). These results are therefore reported descriptively only.
Descriptive incidence rates across all groups
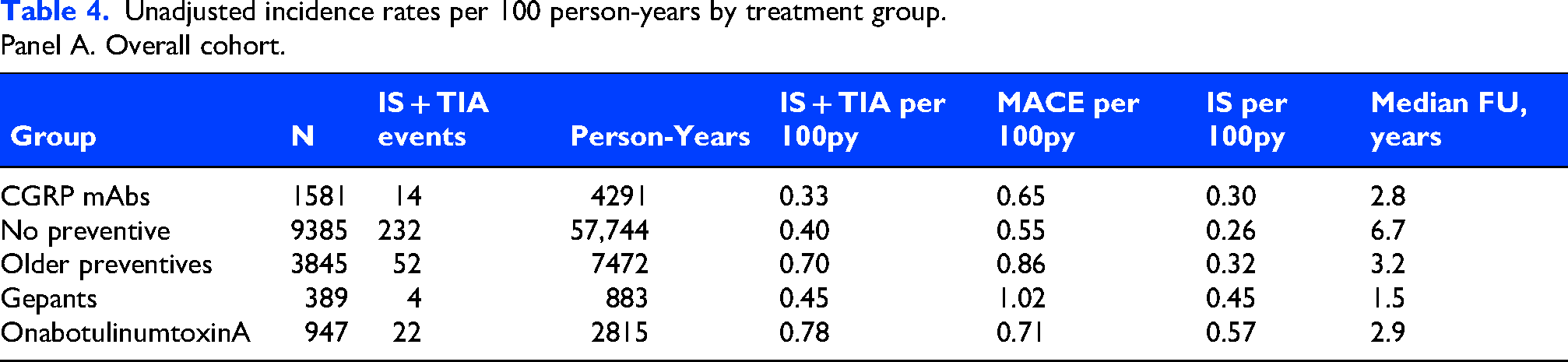
Table 4 presents unadjusted IS + TIA incidence rates per 100 person-years across all treatment groups. CGRP mAbs had the lowest rate overall (0.33 per 100 person-years) and in the migraine with aura subgroup (0.34 per 100 person-years). OnabotulinumtoxinA had the highest rate (0.78 per 100 person-years overall and 1.05 per 100 person-years in the aura subgroup).
Unadjusted incidence rates per 100 person-years by treatment group.
Panel A. Overall cohort.
Panel B. Migraine with aura subgroup.
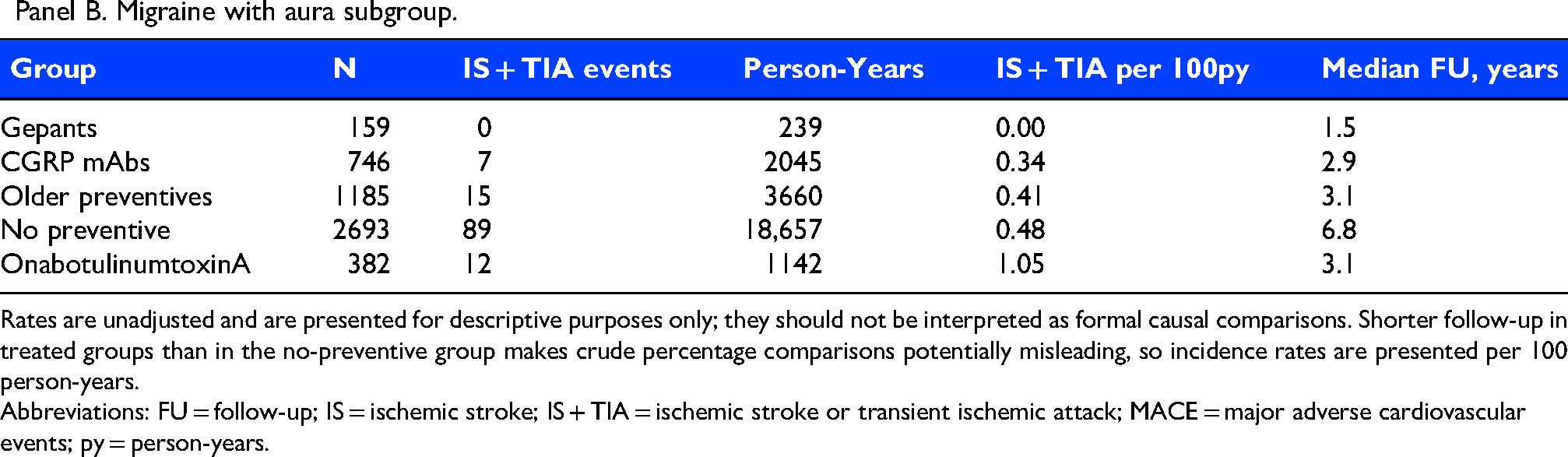
Rates are unadjusted and are presented for descriptive purposes only; they should not be interpreted as formal causal comparisons. Shorter follow-up in treated groups than in the no-preventive group makes crude percentage comparisons potentially misleading, so incidence rates are presented per 100 person-years.
Abbreviations: FU = follow-up; IS = ischemic stroke; IS + TIA = ischemic stroke or transient ischemic attack; MACE = major adverse cardiovascular events; py = person-years.
Discussion
In this real-world cohort from the NIH All of Us Research Program, CGRP mAbs met the prespecified statistical criterion for non-inferiority relative to onabotulinumtoxinA for the primary IS + TIA outcome. However, this finding was based on 36 primary outcome events and should be interpreted with caution. The primary analysis is best understood as evidence against a large relative increase in incident IS + TIA risk compared with onabotulinumtoxinA, rather than as definitive evidence of equivalent safety, absence of modest harm, or a protective effect. Not all analyses met the non-inferiority threshold. The subgroup without aura, the per-protocol analysis, and the MACE analysis were inconclusive for non-inferiority because their CIs crossed the prespecified margin of 1.5. Although several point estimates were below 1.0, these estimates were imprecise and should not be interpreted as evidence that CGRP mAbs reduce ischemic cerebrovascular risk.
Our primary finding was directionally consistent with the largest prior real-world study, which also found no increased cardiovascular risk with CGRP mAbs compared with onabotulinumtoxinA in Medicare beneficiaries. 10 However, the present study extends that literature in several ways. First, the All of Us cohort includes substantially greater racial and ethnic diversity than prior claims-based studies. 14 Second, our cohort included patients with vascular comorbidities who were commonly excluded from clinical trials and prior observational studies. Third, we examined the migraine with aura subgroup, which is clinically relevant given its higher baseline IS risk. At the same time, the baseline differences between treatment groups are clinically important. OnabotulinumtoxinA initiators had a higher burden of vascular comorbidity, consistent with real-world treatment selection along a stepped-care pathway. Although IPTW achieved excellent balance across measured covariates, residual differences in vascular risk, migraine severity, prior treatment failure, or referral patterns may not have been fully captured in structured EHR data. If present, this residual confounding would most likely bias estimates toward a lower observed risk among CGRP mAb users. This possibility is an important reason not to interpret HRs below 1.0 as evidence of a protective effect.
The theoretical concern that CGRP-pathway blockade could worsen cerebrovascular outcomes by attenuating protective vasodilatory responses was not supported by the primary analysis, which met the prespecified criterion for non-inferiority for IS + TIA. However, these results should not be overinterpreted as definitive evidence of vascular safety across all outcomes, because several CIs remained wide and some analyses, including MACE, were inconclusive for non-inferiority. Importantly, our analysis addressed incident event risk only. It did not evaluate stroke severity, infarct characteristics, disability, recovery, recurrence, or outcomes after an ischemic event. In addition, because preventive migraine treatment is preference-sensitive and generally long-term, this finding should be applied in the context of baseline vascular risk, prior treatment response, tolerability of competing therapies, and patient preferences.
The point estimate for IS + TIA in the aura subgroup was lower than that in the subgroup without aura, and the aura subgroup met the prespecified non-inferiority criterion, whereas the subgroup without aura was inconclusive for non-inferiority. Nonetheless, this subgroup remains clinically important because treatment decisions in patients with migraine with aura are often influenced by concerns about cerebrovascular risk.1,15 The increasing clinical and public visibility of CGRP-targeting therapies further underscores the need for post-marketing safety studies that evaluate rare cerebrovascular outcomes in diverse real-world populations. 16 Additional study in larger cohorts with greater event accrual will be needed to determine whether the observed difference in point estimates reflects chance or true heterogeneity.
The IS-only sensitivity showed a more attenuated and non-significant estimate than the prespecified IS + TIA composite outcome, suggesting that the primary composite finding may be partly driven by TIA events. This distinction is important because TIA diagnoses in structured EHR data are more susceptible to misclassification than ischemic stroke and may differ in clinical severity. The IS + TIA composite is the prespecified primary outcome because TIA and IS share the same pathophysiology and clinical urgency, and because TIA is relevant in cerebrovascular safety surveillance. However, TIA is less specific than IS in structured EHR data, is more susceptible to diagnostic misclassification, and may differ in clinical severity. Therefore, the primary composite endpoint should not be interpreted as equivalent to a hard IS endpoint. The stroke-only analysis remained directionally similar but was less precise and did not provide definitive evidence for or against a difference in ischemic stroke risk alone.
Our study has several limitations. First, the primary comparison was underpowered, and the number of IS + TIA events was small (14 events among CGRP mAb initiators and 22 events among onabotulinumtoxinA initiators). As a result, CIs were wide and included both potentially meaningful risk reduction and little to no difference between groups. Although the upper confidence bound fell below the non-inferiority margin, the study cannot exclude smaller increases in risk that may still be clinically relevant for preventive therapy. Similarly, the lower point estimate should not be interpreted as evidence that CGRP mAbs reduce ischemic cerebrovascular risk. Second, interpretation of non-inferiority depends on the selected margin. We used a prespecified HR margin of 1.5 to reflect the rarity of events and the practical limits of precision in this real-world safety analysis, but we recognize that this is a clinically permissive margin for preventive migraine therapy. The rationale for this margin was not that a 50% increase in IS + TIA hazard would be broadly acceptable. Rather, the margin was intended to evaluate whether CGRP mAbs could exclude a large relative increase in incident ischemic cerebrovascular risk compared with an active preventive comparator. This distinction is important because patients considered for CGRP mAbs may have substantial migraine-related disability, may have failed or not tolerated older preventives, and may be choosing among treatments with different efficacy, tolerability, contraindications, and access profiles. For patients with migraine with aura or other vascular risk factors, even a smaller increase in IS + TIA risk may be clinically meaningful and should be weighed against expected benefit and patient preferences. Third, residual confounding remains possible, particularly for factors that are incompletely captured in structured EHR data, such as migraine chronicity, headache-day burden, prior treatment failures, disease severity, subspecialty neurologic care, and insurance authorization patterns. This limitation is particularly important for the active-comparator design because onabotulinumtoxinA is approved and typically used for chronic migraine, whereas CGRP mAbs are used in both episodic and chronic migraine. Episodic versus chronic migraine status and monthly headache days were not reliably available as standardized structured variables in the analytic dataset and could not be included in Table 1 or the propensity score model. We considered a sensitivity analysis restricted to patients with coding compatible with chronic migraine, but a valid chronic migraine-restricted analysis could not be performed without returning to source-level data. Residual confounding by migraine frequency or treatment indication may therefore remain despite excellent measured covariate balance, and the lower point estimates for CGRP mAbs should be interpreted cautiously. Fourth, outcome ascertainment relied on ICD-10 coding linked to inpatient or emergency department encounters rather than direct adjudication or imaging confirmation. As such, outcome misclassification cannot be excluded. This concern is particularly relevant for TIA, which may be coded variably in routine care and lacks the same imaging-based confirmation as many ischemic stroke diagnoses. Because the primary endpoint combined IS and TIA, and because TIA is a less specific endpoint for the mechanistic concern around CGRP blockade and hard ischemic events, the composite should not be interpreted as equivalent to a hard ischemic stroke endpoint. We therefore present ischemic stroke alone as a key secondary analysis and interpret it alongside the primary composite endpoint. Fifth, we did not model death as a competing risk. This was partly because all-cause mortality was not formally analyzed given limitations in death ascertainment within the dataset. If death differed by treatment group, standard Cox models may have incompletely accounted for informative censoring, although the low number of cerebrovascular events and expected low short-term mortality in this migraine cohort may lessen the magnitude of this bias. Sixth, follow-up CGRP mAb exposure remained limited relative to the drug class's availability, reducing the ability to assess longer-term effects. Finally, because the All of Us cohort is volunteer-based, the study population may not fully reflect the broader population of patients with migraine in routine clinical practice.
Conclusions
In this real-world cohort from the NIH All of Us Research Program, CGRP mAbs met the prespecified statistical criterion for non-inferiority relative to onabotulinumtoxinA for incident ischemic stroke or transient ischemic attack. Because this finding was based on fewer than 40 primary events, it should be interpreted cautiously as evidence against a large relative increase in incident IS + TIA risk, rather than as definitive evidence of equivalent safety or a protective effect. The IS-only analysis was directionally similar but more attenuated and imprecise, and the IS + TIA composite should not be interpreted as equivalent to a hard ischemic stroke endpoint. Larger comparative safety studies with longer follow-up and more detailed outcome characterization will be important to more precisely define the cerebrovascular safety of CGRP mAbs.
Article highlights
Calcitonin gene-related peptide monoclonal antibodies met the prespecified statistical criterion for non-inferiority versus onabotulinumtoxinA for incident IS + TIA.
The primary analysis should be interpreted as evidence against a large relative increase in incident IS + TIA risk, not as proof of equivalent safety or vascular protection.
Low event counts limited precision, and the lack of stroke severity and post-event outcome data supports the need for larger comparative safety studies.
Footnotes
Ethical considerations
The Cleveland Clinic Institutional Review Board (IRB) determined that the project did not constitute human subject research; therefore, no IRB approval was required.
Author contributions
SG: Conceptualization, methodology, data curation, formal analysis, investigation, writing – original draft, and writing – review & editing.
BO: Formal analysis, investigation, writing – original draft, writing – review & editing, and manuscript revisions.
ST: Writing – review & editing.
NT: Methodology, formal analysis, software, validation, and writing – review & editing.
HY: Methodology, supervision, project administration, and writing – review & editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
BO serves as an editorial board member of the Neurology Resident & Fellow Section Editorial Board and as Assistant Editor of Headache: The Journal of Head and Face Pain. BO has participated as an uncompensated host for the Neurology Minute podcast of the American Academy of Neurology. BO has also received research funding from American Academy of Neurology and American Headache Society. BO has also been selected to participate in the 2026/2027 Cephalalgia Reviewer Academy.
HY serves as an associate editor of Cephalalgia. HY has received funding from AHS Early-Stage Investigator Research Award, Pfizer-Jefferson Collaborative Research; institutional support for serving as an investigator from Teva, AbbVie, Ipsen, Rehaler, Pfizer, Shiratronics, Lundbeck, Johnson & Johnson; consultant/advisory fees from Salvia, AbbVie, Pfizer, Cerenovus; and royalties from Cambridge University Press and MedLink Neurology.
The other authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Data availability statement
Analyses were conducted within the NIH All of Us Researcher Workbench. Code is available upon reasonable request.